

Abstract
Aim
This study aimed to develop a concise tool with acceptable predictive properties to identify young children with specific language impairment (SLI).
Methods
In this nested case–control study children with SLI attending two special needs schools for severe speech and language difficulties in the Netherlands were matched by date of birth and sex with control children attending mainstream education. This study analysed the predictive validity for having SLI at a mean age of eight years and three months (range 4–11 years) using combinations of six language milestones that were registered at 24, 36 and 45 months and retrieved from the children's healthcare files in 2012.
Results
We included 253 pairs of children with and without SLI. During a single visit, combinations of two milestones at one age achieved a specificity of at least 97% and sensitivities ranged from 32% to 64%. However, the concise tool, which combined five milestones at three different ages – 24, 36 and 45 months – had a specificity of 96% (95% confidence interval 94–99%) and a sensitivity of 71% (95% confidence interval 66–77%).
Conclusion
Combining milestones at different ages provided a concise tool that could help to detect children with SLI at a young age.
Keywords: Developmental language disorder, Language milestones, Sensitivity, Specific language impairment, Specificity
Abbreviations
- CI
Confidence interval
- DLD
Developmental language disorder
- SD
Standard deviation
- SLI
Specific language impairment
Key notes.
This study of 253 children with specific language impairment (SLI) and 253 matched controls was carried out to develop a concise tool that identified young children with SLI.
Combining two milestones at a single visit had high specificity rates, but low sensitivity rates, for predicting SLI.
However, combining five milestones registered at three different ages enabled us to provide a concise tool to facilitate identifying young children with SLI.
Introduction
Specific language impairment (SLI) is diagnosed in children who exhibit a significant deficit in language ability that cannot be attributed to hearing loss, low nonverbal intelligence or neurological damage 1. The reported prevalence of SLI varies from 2% to 12%, due to differences in definitions or study methods 2. The most cited prevalence is 7%, as reported in a study by Tomblin et al. 3.
Specific language impairment has been associated with social, emotional, personality and learning problems 4, 5, 6. When SLI is identified early this can improve long‐term outcomes and provide early parental insights into their child's problems 7, 8. There have been some indications that early interventions may have a positive effect on a child's development and give them a better chance to develop their potential skills 9.
In 2015, the US Preventive Services Task Force reviewed the evidence on screening for speech and language delays and disorders 10 and found inadequate evidence on the accuracy of screening instruments for use in primary care settings. The Task Force also stated that the accuracy of surveillance by primary care clinicians was inadequate to identify children needing further evaluation for speech and language delays and disorders 11. It also considered that the benefits of early detection and intervention were not yet sufficiently proven 11. However, the American Academy of Pediatrics has stated that early identification of developmental disorders is an important task for paediatric healthcare professionals and it has recommended incorporating developmental surveillance at every well‐child visit 12.
The fact that we do not currently have an adequate screening instrument for speech and language delay should not deter us from attempting to develop and refine what is already available to try and identify children with SLI as early as possible.
In a previous study on data collected in 2012, we investigated whether children with and without SLI had reached language milestones at a specific age 13. A special feature of the study was that we used having SLI from the age of four years as the gold standard. The conclusion of that study was that single language milestones between two and four years of age were moderately predictive for SLI 13. Our hypothesis for the present study was that the predictive validity could be increased by using combinations of milestones.
The present study aimed to construct a concise tool to facilitate identifying young children with SLI by using combinations of language milestones that could be administered between the ages of 24 and 45 months. We felt it was necessary that the tool should have acceptable predictive properties for detecting children with SLI in well‐child clinics and paediatrics settings and should be quick and easy to administer.
Methods
Design and study population
This was a nested case–control study and the cases were 253 children (77% boys) with SLI who attended two special needs schools for severe speech and language difficulties in the eastern part of the Netherlands. They were matched by date of birth and sex with 253 control children who attended mainstream education. The current study analysed the predictive validity for having SLI, using combinations of six language milestones registered at 24, 36 and 45 months that were retrieved from the children's healthcare files in 2012. At the time of the data collection the ages of the subjects in this study ranged from 4 to 11 years, with a mean age of eight years and three months. A previous study on achieving language milestones at a specific age, published in 2016, was also based on data that the authors retrieved in 2012 and that study also covered the children who were included in the current study 13.
The study schools were located in Nijmegen and Arnhem, which is a mixed rural and urban healthcare area. The selection criteria for admission to these special needs schools are very strictly formulated by the Dutch Department of Education and include having a score of more than 1.5 standard deviations (SD) below the mean on two or more language tests covering the following areas: auditory processing, speech production problems, grammatical problems and lexical‐semantic problems 14, 15.
In addition, the disorder should not be due to hearing impairment or limited cognitive skills, as established with a validated test. The tested nonverbal intelligence quotient should be at least 80. A special committee selects the tests used 16. Autism spectrum disorder should be excluded as a cause of the language disorder. These criteria correspond with the internationally generally used criteria for SLI 1. The children in our study were diagnosed by a multidisciplinary team of specialists, including an audiologist, a psychologist, a didactic specialist and a speech therapist. Their report was then examined by an independent, Government‐controlled committee. Children were very occasionally admitted to these schools even though they did not fully meet all the admission criteria. We therefore examined the test scores of all cases and only included children who met all the inclusion criteria.
The controls were children attending mainstream education in the same region. Each case was matched with a control child of the same sex and the same date of birth give or take two days.
A total of 330 children, aged between 4 and 11 years, attended the two special needs schools for children with severe speech and language problems in the studied region. Of these, 306 fully met the criteria for admission to these special needs schools. We excluded 18 children due to a cleft palate or because they had been adopted. Adoption was an exclusion criterion, because data on their earlier milestones were not always available or reliable. The parents of four children did not want their child to take part. Fully documented child healthcare files were found for 259 of the remaining 284 children. We were able to include 253 children attending mainstream education who had fully documented child healthcare files and the study therefore comprised 253 matched pairs (Fig. S1).
Informed consent
In the Netherlands, all parents of children who attend Municipal Health Services are informed at the start of their care that their child's anonymous data may be used for scientific research. The Dutch Central Committee on Research Involving Human Subjects assessed the research project and concluded that individual parental approval was not needed, because the anonymity of the filed data was guaranteed. Despite this, we still decided to inform the parents of the cases about the study and ask for their consent.
Dutch well‐child care
In the Netherlands, all children are invited to attend 11 visits to well‐child care facilities from birth to the age of four years and the attendance rate is almost 95% 17. Child development data are collected at each visit in a uniform way using a Dutch instrument 18 that is a modification of the Gesell test. It consists of a set of age‐appropriate items, also called milestones, which cover five developmental fields. A total of 23 milestones cover language development and communication and are called language milestones. All child health professionals are trained to administer and register the milestones in the well‐child care system according to a uniform protocol. When a child passes or fails an item at a visit this is registered in the child healthcare file as a plus or minus, respectively. Our previous study in 2016 reported on the predictive properties of all 23 language milestones. In that study, which used the same study population as the current study, we also established that the mean age of the cases and controls were not significantly different for most of the well‐child care visits 13.
In the present study, we used the six language milestones that are registered between the ages of 24 and 45 months in the child healthcare files.
The concise tool
The Dutch developmental instrument that we used includes the following six language milestones between the ages of 24 and 45 months: says two‐word sentences and points at six parts of a doll's body at 24 months, says sentences of three or more words and speech is understood by acquaintances at 36 months and talks spontaneously about events at home or in the playground and asks questions about who, what, where and how at 45 months of age. Our aim was to construct a tool based on these six language milestones between the ages of 24–45 months to facilitate identifying children with SLI.
Statistical analyses and calculation
Multiple imputations were applied to adjust for missing values for the milestones. This simulation‐based approach creates a number of imputed (completed) data sets by filling in plausible values for the missing data. The imputations were based on a model that uses information from other language milestones to achieve optimal estimates. Uncertainty about the model estimates is reflected in differences between imputations in the various completed data sets. We used multivariate imputation by chained equations to create 20 imputed data sets based on all language milestones between 24 and 45 months of age and the group variable, which was the case or control group 19. The averages of the outcomes of the language milestones over all 20 completed data sets are presented. All statistical analyses were performed in R Version 3.1.3 (The R Foundation, Vienna, Austria) and SPSS version 20.0 for Windows (IBM Corp, Armonk, NY, USA).
To construct the concise tool with the milestones, we calculated the proportion of children with a referral at one or more age visits. All possible combinations of outcomes, pass or fail, of the two milestones administered at each of the three ages were tested on their predictive validity in terms of specificity and sensitivity. To keep the number of false positives low, we preferred a specificity of at least 95%. We calculated 95% confidence intervals (95% CI) according to the method devised by Rubin 20 or the exact confidence interval from the binomial distribution.
Results
At the time of the data collection, the mean ages of the 253 children in the SLI group and the 253 in the control group were eight years and three months with a standard deviation of one year and 10 months and 77% were boys. In another previous study, published in 2017 with the same study population, we established that the pregnancy characteristics and Apgar scores did not differ significantly between both groups 21. The numbers of cases and controls with available data on achieving language milestones between the ages of 24 and 45 months are documented in Table 1. Missing values were imputed and the available and imputed data were used in the analyses. Table 1 also shows the predictive validity per age visit using combinations of the two milestones. The outcomes showed specificities ranging from 85% to 100% and sensitivities ranging from 32% to 78%. High sensitivity rates were always combined with specificity rates below 90%.
Table 1.
Validity of combinations of failure on one or two milestones at each age visit based on the imputed data (n = 253 controls, n = 253 cases)
| Age in months | Milestone | Number of children | Outcomes on milestones | Sensitivity % (95% CI) | Specificity % (95% CI) | |
|---|---|---|---|---|---|---|
| Cases | Controls | |||||
| n | n | |||||
| 24 | A | 226 | 244 | A− | 72 (67–78) | 88 (84–92) |
| B | 204 | 220 | B− | 38 (32–44) | 94 (91–97) | |
| A and B | 203 | 219 | A− or B− | 78 (73–83) | 85 (81–90) | |
| A− and B− | 32 (26–38) | 97 (95–99) | ||||
| 36 | C | 200 | 226 | C− | 49 (43–56) | 100 (99–100) |
| D | 203 | 238 | D− | 56 (50–62) | 97 (95–99) | |
| C and D | 194 | 220 | C− or D− | 64 (58–70) | 97 (94–99) | |
| C− and D− | 41 (35–47) | 100 (98–100) | ||||
| 45 | E | 88 | 130 | E− | 52 (45–58) | 98 (96–100) |
| F | 101 | 122 | F− | 56 (50–63) | 97 (95–99) | |
| E and F | 76 | 115 | E− or F− | 64 (58–70) | 95 (92–98) | |
| E− and F− | 44 (38–50) | 99 (99–100) | ||||
A = Says two‐word ‘sentences’; B = Points at six parts of a doll's body; C = Says ‘sentences’ of three or more words; D = Speech is understood by acquaintances; E = Talks spontaneously about events at home/playground; F = Asks questions about ‘who’, ‘what’, ‘where’ and ‘how’; A− = failure on milestone A.
The predictive validity of the combinations of all six milestones was calculated (Table S1). At the age of 36 months the milestone of speech is understood by acquaintances did not contribute much to the detection of more children with SLI, but decreased the specificity rate and this milestone was therefore excluded from the tool. The final version of the concise tool consisted of the following combination: two milestones at the age of 24 months, says two‐word sentences and points at six parts of a doll's body, one milestone at the age of 36 months, says sentences of three or more words and two at the age of 45 months, namely talks spontaneously about events at home or in the playground and asks questions about who, what, where and how. This combination, which had the optimal predictive value, with a sensitivity of 71% and a specificity of 96%, is shown in Figure 1.
Figure 1.
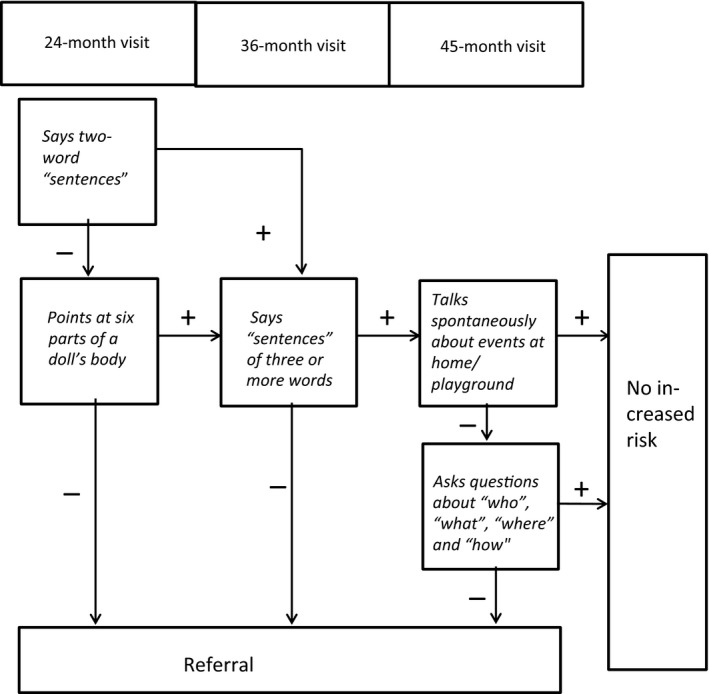
Flow chart with optimal combination using five milestones referred to as concise tool.
Discussion
The main finding of our study was that a combination of language milestones may provide a useful instrument that can be used in well‐child care and paediatrics to detect children with a high risk of SLI. Our latest study showed that the concise tool was quick and easy to administer and helpful in facilitating the early identification of children with SLI. However, this tool will need to be validated in a new study in the community.
As described in our previous study 13, important factors when choosing satisfactory values for sensitivity and specificity of a screening instrument include the prevalence and severity of the disease, the consequences of not detecting the disease, the importance of early detection and avoiding needless parental concern. Furthermore, we do not currently have irrefutable evidence of the benefits of early treatment 11. When we had to choose between high values of specificity or sensitivity we preferred a low percentage of false positives (high specificity) rather than the chance of missing a child with SLI (lower sensitivity). Accordingly, we concluded that optimal predictive values for a suitable instrument for screening for SLI were a specificity of at least 90%, while a sensitivity of at least 70% was acceptable.
A review on screening for speech and language delay published in 2015 reported on the accuracy of screening instruments 11 and it stated that sensitivity and specificity rates of at least 70% were considered acceptable. Screening instruments used by parents had sensitivity rates ranging from 50% to 94% and specificity rates ranging from 45% to 96%. For screening instruments used by trained examiners, the sensitivity rates were 17–100% and specificity rates were 46–100% 22. The gold standard used in these studies was another language test carried out at the same time or, in exceptional cases, a language test one year later. In our study, we used the diagnosis of SLI at school age that is after the age of four years, as the gold standard. This means that slow starters were excluded from the study population. Therefore, we consider our gold standard to be superior to the gold standards in the studies mentioned by Wallace et al. 22.
In the Netherlands, there is a well‐organised well‐child care system, where 95% of all children are seen at regular age‐points, making it easy to implement this screening tool. With the present system, many children with SLI are not detected or are detected later than desired 23. Implementation of this concise tool in the Netherlands would improve this. Our study shows that using a combination of two milestones at 24, 36 or 45 months of age will detect some children with SLI at a young age. Based on the outcomes shown in Table 1, we can conclude that children who fail on both milestones at a specific age have a very high risk of having SLI. When this is the case, we recommend that the professional takes a medical history, performs a physical examination and gains the opinion of the parents before the child is referred for further diagnostic investigations. Children who fail on only one of the two milestones at a specific age should be followed up, because they have an increased risk for having SLI. This way the specificity rate of the test will remain high and the sensitivity rate will increase.
Several of the milestones used in this study are also used as language milestones by the National Institute on Deafness and Other Communication Disorders. These include knows a few parts of the body and can point to them when asked and puts two words together, such as more cookie or no juice, at the age of 24 months of age 24. The American Family Physician Website considers it a red flag when the child does not use unique two word phrases, including noun‐verb combinations at the age of 30 months 25. Milestones in the Dutch language were used in our study and the healthcare system in the Netherlands is different to that in many countries. However, we believe that the combinations in our concise tool can be useful in other countries, as it uses language milestones used by the National Institute or as red flags by other investigators. Further investigations in other countries with different healthcare systems and different languages will be necessary before our concise tool can be implemented there.
A limitation of the study was the number of missing values for two milestones at the age of 45 months. This was caused by a change in Government policy for economic reasons during the period of data registration. This meant that the child was no longer seen by a physician but by a well‐child care nurse at 45 months. The nurses were not trained to administer the Dutch developmental instrument and this meant that it was not used by them. Because of this, the percentage of missing values in the language milestones at 45 months ranged from 56% to 57%, which was much higher than usual. Missing data at this age are therefore not likely to be related to the outcome and can be considered as missing at random. Multiple imputations were applied to take the missing structure of the data into account.
We expect that when this concise tool is used that some children with other developmental problems will be included in the false‐positive children. Even though they will not be diagnosed as having SLI, referrals for investigation may be useful for many of these children.
Since 2014, several experts have recommended that the term SLI should no longer be used for children with language disorders that are not associated with a known biomedical aetiology 26. The expression of developmental language disorder (DLD) is now recommended instead of SLI 27. DLD has a broader reach than SLI and the criteria for meeting the definition of DLD have become less stringent than for the definition of SLI. A new development is that low intellectual capacity or no significant difference between verbal and nonverbal abilities are no longer exclusion criteria. The cases in our study were not assessed with these new criteria, as we used the criteria that schools for children with severe speech and language difficulties in the Netherlands used for their selection procedure. Therefore, our cases were more strictly selected and did not fit with the new criteria of DLD. For this reason, we used the old name SLI. We assume that our concise tool will also be able to detect many children diagnosed with DLD, even though DLD includes children with a broader range of problems than SLI. However, this should be tested in a new study.
A strength of our study was the prospective design. Data on language milestones were registered before the diagnosis of SLI was made. This means that recall bias can be excluded. Furthermore, the language milestones were collected in a uniform manner by trained professionals. Another strength was that all cases were thoroughly investigated and diagnosed. As the diagnosis of SLI was made after the age of four years, this meant that the impairment was likely to have been persistent and we considered it unlikely that slow starters were included in our case group. In the Netherlands, the majority of children attend well‐child care services and practically all children in our study region with SLI would have been referred to the two special needs schools.
Conclusion
We concluded that our concise tool, which was based on combinations of language milestones at specific ages, could be helpful in detecting children with SLI. The tool was quick and easy to administer. A major advantage was that it could enable the majority of children with SLI to be identified before the age of four years and before starting primary school. This makes it possible for adequate educational support to be in place when these children start school, thus giving them the best possible start in their education.
Funding
This research was supported by ZonMW, Netherlands Organization for Health Research and Development (grant number 200320016 and 73200.095001), who played no role in the study or paper.
Conflict of interest
The authors have no conflict of interests to declare.
Supporting information
Figure S1 Study population.
Table S1 Validity of combinations of all milestones at all age visits based on the imputed data (n = 253 controls, n = 253 cases).
References
- 1. Leonard LB. Children with specific language impairment. 2nd ed Cambridge, MA: MIT Press, 2014. [Google Scholar]
- 2. Law J, Boyle J, Harris F, Harkness A, Nye C. Prevalence and natural history of primary speech and language delay: findings from a systematic review of the literature. Int J Lang Commun Disord 2000; 35: 165–88. [DOI] [PubMed] [Google Scholar]
- 3. Tomblin JB, Records NL, Buckwalter P, Zhang X, Smith E, O'Brien M. Prevalence of specific language impairment in kindergarten children. J Speech Lang Hear Res 1997; 40: 1245–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Clegg J, Hollis C, Mawhood L, Rutter M. Developmental language disorders–a follow‐up in later adult life. Cognitive, language and psychosocial outcomes. J Child Psychol Psychiatry 2005; 46: 128–49. [DOI] [PubMed] [Google Scholar]
- 5. Conti‐Ramsden G, Mok PLH, Pickles A, Durkin K. Adolescents with a history of specific language impairment (SLI): strengths and difficulties in social, emotional and behavioral functioning. Res Dev Disabil 2013; 34: 4161–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. St Clair MC, Pickles A, Durkin K, Conti‐Ramsden G. A longitudinal study of behavioral, emotional and social difficulties in individuals with a history of specific language impairment (SLI). J Commun Disord 2011; 44: 186–99. [DOI] [PubMed] [Google Scholar]
- 7. Conti‐Ramsden G, Durkin K. Language development and assessment in the preschool period. Neuropsychol Rev 2012; 22: 384–401. [DOI] [PubMed] [Google Scholar]
- 8. Reilly S, McKean C, Morgan A, Wake M. Identifying and managing common childhood language and speech impairments. BMJ 2015; 350: h2318. [DOI] [PubMed] [Google Scholar]
- 9. Law J. The efficacy of treatment for children with developmental speech and language delay/disorder: a meta‐analysis. J Speech Lang Hear Res 2004; 47: 924–43. [DOI] [PubMed] [Google Scholar]
- 10. Berkman ND, Wallace I, Watson L, Coyne‐Beasley T, Cullen K, Wood C, et al. Screening for speech and language delays and disorders in children age 5 years or younger: a systematic evidence review for the U.S. Preventive Services Task Force. Evidence Synthesis No. 120. AHRQ Publication No. 13‐05197‐EF‐1, 2015. [PubMed]
- 11. Siu AL. Screening for speech and language delay and disorders in children aged 5 years or younger: US Preventive Services Task Force recommendation statement. Pediatrics 2015; 136: e474–81. [DOI] [PubMed] [Google Scholar]
- 12. Council on Children With Disabilities, Section on Developmental Behavioral Pediatrics, Bright Futures Steering Committee MHI for CWSNPAC . Identifying infants and young children with developmental disorders in the medical home: an algorithm for developmental surveillance and screening. Pediatrics 2006; 118: 405–20. [DOI] [PubMed] [Google Scholar]
- 13. Diepeveen FB, Dusseldorp E, Bol GW, Oudesluys‐Murphy AM, Verkerk PH. Failure to meet language milestones at two years of age is predictive of specific language impairment. Acta Paediatr 2016; 105: 304–10. [DOI] [PubMed] [Google Scholar]
- 14. wetten.nl – Wet op de expertisecentra – BWBR0003549 (Internet). Available at: http://wetten.overheid.nl/BWBR0003549/2015-03-04 (accessed on March 19, 2018).
- 15. wetten.nl – Besluit leerlinggebonden financiering – BWBR0014753 (Internet). Available at: http://wetten.overheid.nl/BWBR0014753/2010-10-01 (accessed on March 19, 2018).
- 16. Psychological testing (COTAN) – NIP English (Internet). Available at: https://www.psynip.nl/en/dutch-association-psychologists/activities-nip/psychological-testing-cotan/ (accessed on March 19, 2018).
- 17. CBS – Ouders geven consultatiebureau gemiddeld een ruime 7 – Webmagazine (Internet). Available at: https://www.cbs.nl/en-gb/news/2014/44/parents-give-child-health-centres-a-7-out-of-10 (accessed on March 19, 2018).
- 18. Laurent de Angulo M, Brouwers‐de Jong E, Blijsma‐Schlosser J, Bulk‐Bunschoten A, Pauwels J, Steinbuch‐Linstra I. Ontwikkelingsonderzoek in de jeugdgezondheidszorg. Assen: van Gorkum, 2008. [Google Scholar]
- 19. van Buuren S. Flexible imputation of missing data. Boca Raton, FL: Chapman & Hall/CRC Press, 2012. [Google Scholar]
- 20. Rubin DB. Frontmatter. Multiple imputation for nonresponse in surveys. Hobroken, NJ: John Wiley & Sons, Inc., 2008. [Google Scholar]
- 21. Diepeveen FB, van Dommelen P, Oudesluys‐Murphy AM, Verkerk PH. Specific language impairment is associated with maternal and family factors. Child Care Health Dev 2017; 43: 401–5. [DOI] [PubMed] [Google Scholar]
- 22. Wallace IF, Berkman ND, Watson LR, Coyne‐Beasley T, Wood CT, Cullen K, et al. Screening for speech and language delay in children 5 years old and younger: a systematic review. Pediatrics 2015; 136: e448–62. [DOI] [PubMed] [Google Scholar]
- 23. Uilenburg N, Wiefferink K, Verkerk P, van Denderen M, van Schie C, Oudesluys‐Murphy AM. Accuracy of a screening tool for early identification of language impairment. J Speech Lang Hear Res 2018; 61: 104. [DOI] [PubMed] [Google Scholar]
- 24. Speech and Language Developmental Milestones [NIDCD Health Information] (Internet). Available at: https://www.nidcd.nih.gov/health/speech-and-language (accessed on March 19, 2018).
- 25. McLaughlin MR. Speech and language delay in children. Am Fam Physician 2011; 83: 1183–8. [PubMed] [Google Scholar]
- 26. Ebbels S. Introducing the SLI debate. Int J Lang Commun Disord 2014; 49: 377–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Bishop DVM, Snowling MJ, Thompson PA, Greenhalgh T, and the CATALISE‐2 consortium . Phase 2 of CATALISE: a multinational and multidisciplinary Delphi consensus study of problems with language development: terminology. J Child Psychol Psychiatry 2017; 58: 1068–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Figure S1 Study population.
Table S1 Validity of combinations of all milestones at all age visits based on the imputed data (n = 253 controls, n = 253 cases).