

Dear Editor,
Epiploic appendagitis mimics acute abdomen or is a condition associated with acute abdomen, although it is usually not treated by emergent surgical intervention and has characteristic findings on computed tomography (1). Mechanical intestinal obstruction is not a real manifestation of the disease because those small appendages (inflamed or not) cannot easily obstruct the small or large intestines because of their small sizes. Epiploic or omental appendages are in fact visceral peritoneal pouches that arise from the serosal and antimesenteric surface of the large intestine. They may act as defending mechanisms, similar to the omentum (2). They can even be helpful in spontaneous healing of small perforations in the hollow viscera, and they can also be used as a patch during surgical interventions, such as in appendectomy, by the surgeon. Because of their roles in defending mechanisms, they can also be speculatively interpreted as dwarf omental structures. Consisting of fat tissue and vessels, they have a length of 0.5–5 cm. While epiploic appendages located near the sigmoid colon are the biggest, >100 such appendages may also occur. None of them are found at the rectal wall. Unfortunately, epiploic appendages are detected on computed tomography only when they are inflamed or surrounded by fluid accumulation. Torsion of epiploic appendages results in vascular occlusion that might lead to ischemia (3). Although there are rare reports about acute epiploic appendagitis, a condition resulting in mechanical obstruction of the ileum elongated like a horse by inflamed and fused epiploic appendagitis has not been reported previously.
An 87-year-old female and obese patient with hypertension, diabetes mellitus, and Alzheimer disease was admitted to emergency service because of abdominal distention, nausea, vomiting, and subfebrile fever lasting for 3 days. She had abdominal tenderness and guarding in all quadrants of the abdomen. Computed tomography revealed widely distended small intestines, but epiploic appendagitis was not indicated (Figure 1, 2). The white blood cell count and CRP levels were 18000/mm3 and 31 mg/L, respectively. She was operated on because of mechanical intestinal obstruction and acute abdomen. Midline laparotomy revealed that elongated and inflamed horseshoe shaped epiploic appendagitis formed by the inflammatory fusion of two epiploic appendages of the splenic flexura, which elongated and obstructed the ileal loop located 30 cm proximal to the ileocecal valve (Figure 3). Adhesiolysis was enough to treat the condition, and the patient was discharged from the hospital on the 3rd postoperative day uneventfully.
Figure 1.

Coronal view of dilated loops of the small intestine on computed tomography
Figure 2.

Transverse view of dilated loops of the small intestine on computed tomography
Figure 3.
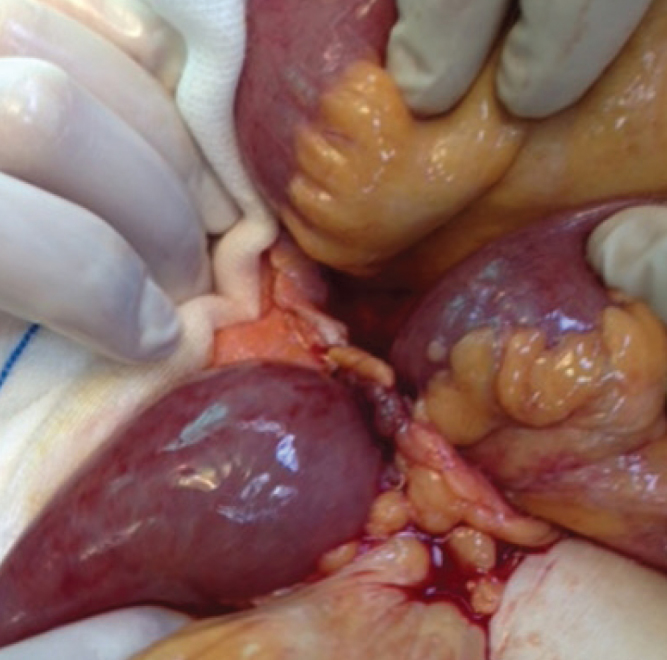
Laparotomy view of the elongated ileum by acute appendagitis before adhesiolysis
Acute epiploic appendagitis is a self-limited condition caused by torsion of larger appendages, in particular, because smaller ones cannot easily rotate around their own axis. Their vascular stalk tends to rotate with their growing size. Adhesion, intestinal obstruction, invagination, intraperitoneal loose bodies, peritonitis, or abscess formation are awaited as complications. It is usually a disease occurring during the 4th–5th decades of life. Acute appendagitis is rare but can result in ischemia presenting as an acute clinical condition which can mimic acute appendicitis, cholecystitis, diverticulitis, or other more serious causes of acute abdominal pain (4). Surgical treatment can be avoided if diagnosis has been established by computed tomography despite the presence of the sign and symptoms of acute abdomen. The typical and pathognomonic sign on computed tomography is usually an oval-shaped fat density of 2–3 cm (3). However; the untypical structure described in the present case resulted in a misdiagnosis on tomographic images because the characteristic high attenuated central dot within the inflamed appendages that normally corresponds to a thrombosed draining vein was not visualized because of fused and inflamed appendages which formed a longe around ileum (1). Epiploic appendagitis can be primary or secondary. While primary disease is a benign and localized infection which is caused by thrombosis of the vein of the stalk of the structure, secondary epiploic appendagitis is associated with inflammation of the neighboring organs, such as diverticulitis, appendicitis, and cholecystitis. Sigmoid colon and cecum are mostly involved areas of the colon (5).
Both intestinal obstruction and acute abdomen may hide epiploic appendagitis and should be kept in mind for differential diagnosis. In conclusion; ileum was elongated like a horse by epiploic appendagitis of the splenic flexura of the colon. In the present case, whether inflamed and fused epiploic appendages or mechanical intestinal obstruction caused acute abdomen is similar to the chicken and egg situation.
Footnotes
Peer-review: Externally peer-reviewed.
Author Contributions: Consept - D.Y., A.K.; Design - D.Y., A.K.; Supervision - A.K.; Resources - A.H., M.Ç.; Materials - A.H.; Data Collection and/or Processing - D.Y., A.K.; Analysis and/or Interpretation - A.H.; Literature Search - A.H., D.Y.; Writing Manuscript - D.Y.; Critical Review - M.Ç.
Conflict of Interest: The authors have no conflict of interest to declare.
Financial Disclosure: The authors declared that this study has received no financial support.
REFERENCES
- 1.Uslu Tutar N, Ozgul E, Oguz D, Cakir B, Tarhan NÇ, Coskun M. An uncommon cause of acute abdomen-epiploic appendagitis: CT findings. Turk J Gastroenterol. 2007;18:107–10. [PubMed] [Google Scholar]
- 2.Leclercq P, Dorthu L. Epiploic appendagitis. CMAJ: Canadian Medical Association Journal. 2010;182:939. doi: 10.1503/cmaj.090791. https://doi.org/10.1503/cmaj.090791 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Singh AK, Gervais DA, Hahn PF, Sagar P, Mueller PR, Novelline RA. Acute epiploic appendagitis and its mimics. Radiographics. 2005;25:1521–34. doi: 10.1148/rg.256055030. https://doi.org/10.1148/rg.256055030 [DOI] [PubMed] [Google Scholar]
- 4.Pogorelić Z, Stipić R, Druzijanić N, et al. Torsion of epiploic appendage mimic acute appendicitis. Coll Antropol. 2011;35:1299–302. [PubMed] [Google Scholar]
- 5.Legome EL, Belton AL, Murray RE, Rao PM, Novelline RA. Epiploic appendagitis: the emergency department presentation. J Emerg Med. 2002;22:9–13. doi: 10.1016/s0736-4679(01)00430-9. https://doi.org/10.1016/S0736-4679(01)00430-9 [DOI] [PubMed] [Google Scholar]