

Abstract
The aim of this retrospective study was to assess the differences between standard R-CHOP and other Rituximab-associated chemotherapy (R-miniCHOP and R-CHOEP) regimens in terms of survival and potential adverse effects. The six-month survival outcomes of 94 diffuse large B-cell lymphomas (DLBCL) patients indicated no statistical difference between overall survival and disease-free survival in the two subgroups. The biological response to therapy (blood count, LDH levels) was similar in both subgroups. Despite having different clinical indications, R-miniCHOP and R-CHOEP provide viable therapeutic alternatives to the standard R-CHOP regimen.
Keywords: diffuse large B-cell lymphoma, prognosis, CHOP, rituximab
Introduction
Despite being considered the most frequent type of non-Hodgkin lymphoma, diffuse large B-cell lymphoma (DLBCL) is in fact a heterogenous group of lymphoproliferative disorders, with different clinical, morphological, immunohistochemical and genetic features [1]. The importance of these particularities lies in their potential role in the selection of the optimal therapeutic algorithm, as well as individualized predictors for the efficiency of the selected regimen. The treatment protocol, on the other hand, did not change much during the last twenty years. One notable exception was the introduction of Rituximab as an important addition to standard chemotherapy protocol in CD20+ cases, providing significant improvement in complete remission rate, disease-free survival and overall survival, with minimal added toxicity [2].
Nevertheless, up to 15% of patients diagnosed with DLBCL exhibit primary refractory disease and 20-25% relapse after the initial response to R-CHOP (Rituximab, Cyclophosphamide, Doxorubicin, Vincristine and Prednisone) regimen [2]. Therefore, other therapeutic solutions were to be tested, such as R-miniCHOP (consisting of adjusted short-term R-CHOP regimen), and R-CHOEP (Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, Etoposide and Prednisone), which adds Etoposide to the conventional regimen. The indication for each of these therapies usually depends on a series of factors, such as age, stage of the disease and biological status, but no precise recommendation has been made so far, as there is only a limited number of studies addressing this issue [3,4,5].
The aim of this study was to evaluate three Rituximab-based treatment regimens in DLBCL according to their short-term biological impact, overall and disease-free survival rate, as well as to perform a detailed literature review of the current therapeutic options in DLBCL according to the Ann Arbor classification and the 2015 ESMO Clinical Practice guidelines.
Methods
We performed a ten-year retrospective analysis of all de novo patients with DLBCL admitted and treated in the Clinical Department of Hematology, at Filantropia City Hospital of Craiova. One hundred and twenty-eight DLBCL cases were diagnosed and classified according to the 2008 World Health Organization classification of tumors of hematopoietic and lymphoid tissues [6]. We selected all DLBCL-confirmed patients that followed Rituximab-based chemotherapy. Only those cases undergoing the complete therapeutic protocol were included. The protocol of our study was approved by the Ethics Committee of the University of Medicine and Pharmacy of Craiova.
Data analysis was performed with GraphPad Prism v7.0 (GraphPad Software Inc. San Diego, USA). Data was analyzed by descriptive statistics and survival estimates using the Kaplan-Meier method. The comparative analysis of the survival endpoints was performed by the Mantel-Cox and Wilcoxon regression tests. Statistically significant results entailed the p value inferior to 0.05 limit in both tests.
Results
Ninety-four patients were selected according to the inclusion criteria. The following regimens were used: R-CHOP, R-CHOEP, and R-miniCHOP. Mean age in the R-CHOP group was 53.2 years, while in the alternative rituximab-based regimen (R-CHOEP and R-miniCHOP) was 66.5 years.
The patients were divided in two groups, both including Rituximab as an indispensable therapeutic agent. The first group of 78 cases was treated with R-CHOP regimen, while the second group, consisting of 16 cases, included all patients with other Rituximab-associated regimen, such as R-miniCHOP and R-CHOEP.
Relevant blood test analysis indicated variations of their mean values at different timeframes (T0-the beginning of therapy, T1-end of therapy/6 months). However, no statistical difference was observed between the groups.
Figure 1.
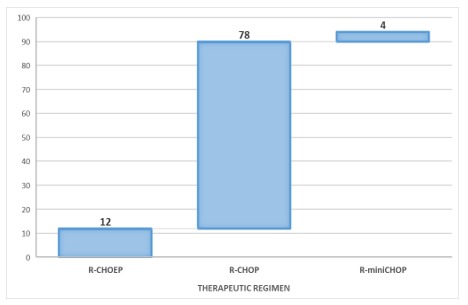
Patients distribution according to DLBCL treatment regimen
Table 1.
Variation of statistical parameters of hemoglobin, lymphocytes and LDH values at the beginning of therapy (T0) and at 6 months/end of therapy (T1)
| Mean | Std. dev. | Median | Var. | Min/Max | SEM | 95% CI | p value: t-test, Welch correction | |
| Hb (T0) | 11.8 | 2.164 | 12.2 | 18.34 | 7.8/16.9 | 0.48 | 10.78-12.81 | 0.66 |
| Hb (T1) | 12.08 | 2.106 | 12.1 | 17.44 | 6.8/17.52 | 0.52 | 10.95-13.2 | |
| Lymphocytes (T0) | 1842 | 942.5 | 1620 | 51.16 | 389/3750 | 228.6 | 1358-2327 | 0.356 |
| Lymphocytes (T1) | 1563 | 686.2 | 1300 | 43.9 | 590/3150 | 190.3 | 1148-1978 | |
| LDH (T0) | 420.4 | 153.6 | 359 | 36.53 | 273/733 | 51.19 | 302.4-538.5 | 0.3375 |
| LDH (T1) | 343.9 | 227.9 | 240 | 66.28 | 124/827 | 58.86 | 217.7-470.2 |
The comparative analysis of the Kaplan-Meier curves in the two groups indicated no statistical difference regarding the 5-year overall survival (Mantel-Cox test: p=0.47; Gehan-Wilcoxon test: p=0.44), with an average survival rate of 43.36% in the R-CHOP group, and 35.15% in the second group. (Fig.2)
Figure 2.
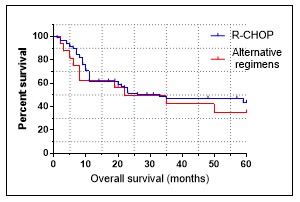
Overall survival for R-CHOP vs. alternative Rituximab-based regimens in DLBCL patients
When disease-free survival was analyzed similar results were observed. There was no statistical difference between the R-CHOP and the alternative Rituximab-based regimens (Mantel-Cox: p=0.79; Gehan-Wilcoxon: p=0.94). The mean survival rate in the first group was 53.18%, and 60.26% in the second group. (Fig.3)
Figure 3.
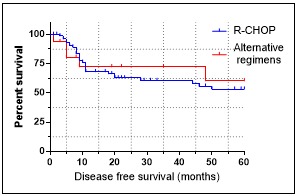
Disease-free survival for R-CHOP vs. alternative Rituximab-based regimens in DLBCL patients
Discussion
The therapeutic options in diffuse large B-cell lymphoma witnessed minimal changes during the last two decades. Immunotherapy, along with anti-CD 20 monoclonal antibody Rituximab, provided the most significant therapeutic breakthrough of the last few years. Due to the progress made over the last decades in terms of pathogenic and molecular heterogeneity of this disease, new regimens and therapeutic agents are being developed in order to improve the results normally achieved with conventional treatments. The treatment of lymphomas evolves towards targeted therapies, by understanding tumor biology and discovering new signaling pathways. Moreover, several biological therapies are available today, ranging from the already known interferon therapy, to rituximab or radiolabeled antibodies, to name just a few of the recent acquisitions in the DLBCL therapeutic armamentarium [7].
The management of DLBCL is distributed into several categories according to the stage of the disease, organ involvement, age and relapse after initial remission [8]. The 2015 ESMO guidelines provided a further patients’ distribution according to the International Prognostic Index (IPI) score.
Therefore, in young low-risk patients without a bulky mass six cycles of CHOP, combined with 6 cycles of Rituximab every 21 days are recommended as the standard treatment in stage I and II CD20+ DLBCL. For young low-intermediary risk patients with bulky disease, the treatment regimen consists of six R-CHOP cycles every 21 days along with localized radiotherapy, or the more intensive R-ACVBP (Rituximab, Doxorubicin, Vindesine, Cyclophosphamide, Bleomycin and Prednisone) regimen every 14 days, without radiotherapy. For young high or intermediary-high risk patients either 6-8 CHOP and Rituximab chemotherapy cycles every 21 days, or more intensive regimens such as R-ACVBP, R-CHOEP can be used [9,10].
For older patients (between 60 and 80 years old) the ESMO guidelines recommend 6 to 8 cycles of R-CHOP every 21 days. Local radiation therapy in older patients with bulky disease seems to be efficient. For patients aged over 80 years R-miniCHOP is advised. In case of cardiac involvement or other co-morbidities, Doxorubicin can be withdrawn from the regimen or it can be substituted by Gemcitabine, Etoposide or liposomal Doxorubicin [9,10].
Apart from the risk stratification, another important landmark in DLBCL treatment is the extension of the disease. Stage I and II lymphoma without bulky disease is found in some 30% of DLBCL. Initially, patients have been treated by localized radiotherapy with good short-term results, but remission could not be maintained in the long term for most of the cases [11]. Nowadays, patients with localized disease but without bulky mass are good candidates for chemotherapy, with standard treatment for these cases consisting of 6 R-CHOP cycles every 21 days [11].
Several studies compared the advantages of associated chemo- and radiation therapy over chemotherapy alone, with conflicting results. While some authors plead for the associated therapy, most papers did not observe any substantial benefit for localized disease without bulky mass [12,13]. Armitage suggested four R-CHOP cycles and, if complete remission is achieved, two more chemotherapy cycles or local radiation therapy can be delivered. In case of bulky disease, radiotherapy is mandatory after six R-CHOP cycles [8]. Same treatment was also proposed in the MINT study for localized bulky disease [11].
For localized disease with specific organ involvement, the therapeutic attitude is different. In case of primary DLBCL of the testis there is a significant risk of central nervous system (CNS) involvement, therefore R-CHOP associated to radiotherapy and Methotrexate or intrathecal (i.t.) Cytarabine is advised [14]. For patients displaying CNS involvement during their first presentation high dose i.v. and i.t. Methotrexate or Cytarabine-in case of lymphomatous meningitis-is recommended [15,16]. In case of altered cardiac function, R-CEOP can be advised [17].
Treatment of advanced stage DLBCL also witnessed several changes during the last 30 years. In the 80s, when IIIrd generation treatments, such as M-BACOD (Methotrexate, Bleomycin, Doxorubicin, Cyclophosphamide, Vincristine and Dexamethasone), ProMACE/CytaBOM (Cyclophosphamide, Doxorubicin, Etoposid, Cytozar, Bleomycin, Vincristine, Methotrexate, Prednison) were developed, it was commonly believed that these regimens were more efficient than CHOP for advanced stage DLBCL patients [18,19]. Further studies comparing these regimens to CHOP on large number of patients proved no significant differences in complete remission or disease-free survival, but lower toxicity for CHOP [20].
GELA study analyzed R-ACVBP on 379 patients aged under 60 years, proving its superiority over the R-CHOP-21, but with higher toxicity. R-ACVBP includes Rituximab, Doxorubicin, Cyclophosphamide, Vindesine, Bleomycin, and Prednisone, for induction of remission, and consolidation with Methotrexate, Doxorubicin, and Cyclophosphamide [21].
For stage III-IV, low performance status, high serum LDH levels patients of younger age (<60 years), autologous stem cell transplantation can be advised as adjuvant therapy [8].
In case of relapsed and refractory DLBCL, prior to establishing salvage chemotherapy, a thorough patient assessment, with a personalized treatment based on age, co-morbidities and other patient-related factors being considered mandatory [22]. For late relapse, in patients with a good prognostic index, the initial regimen may be repeated [17]. In case of early relapse or refractory disease, several second line regimens may be followed in eligible patients by stem cell autotransplantation. None of the second line regimens, such as R-DHAP (Rituximab, Cisplatin, Cytarabine, Dexamethasone), R-ICE (Rituximab, Ifosfamide, Carboplatin, Etoposide), R-GDP (Rituximab, Gemcitabine, Dexamethasone, Cisplatin), ESHAP, BEAM (Carmustyne, Etoposid, Cytarabine, Melphalan) has been shown to be superior to the others [23]. However, a study carried out in 2014 by Crump et al. revealed that R-GDP (Rituximab, Cisplatin, Gemcitabine, Dexamethasone) has the same efficacy as R-DHAP but is less toxic [24].
A beacon of hope comes from the new therapies which are currently tested in non-Hodgkin lymphomas. Bortezomib, lenalidomide, mTOR inhibitors and new anti-CD20 monoclonal antibodies are recent therapies, which are being increasingly used in DLBCL treatment. Bortezomib is a proteasome inhibitor that inhibits NF-κB activity and in combination with chemotherapy has a better therapeutic response than single chemotherapy [25]. Lenalidomide is an analog of Thalidomide, an immunomodulatory and antiangiogenic agent that inhibits the secretion of proinflammatory cytokines. It demonstrated greater efficacy in the response rate for patients with non-germinal center DLBCL than those with lymphoma of the germinal center [26]. In a Phase 1 study, the efficacy of associating Ibrutinib, a new oral bruton tyrosine kinase inhibitor, together with R-CHOP was investigated, demonstrating good tolerability and possible improvement in response rate, but additional studies are needed to establish the exact role of this drug in DLBCL [27].
In hematological neoplasia, due to the graft-versus-host, the therapeutic potential of the immune system has been proven therefore its manipulation has become a very important treatment alternative. CARs (Chimeric antigen receptors) are artificial bio-constructs that recognize a tumor cell antigen and a molecule in the effector cell due to the T-activating domains of the composition, thus redirecting the T lymphocytes against neoplastic cells. T cells are collected from a patient by apheresis and then genetically modified to express CARs for redirection against the target neoplastic cells. Later they are multiplied in the laboratory, frozen and returned to the patient. They will recognize the neoplastic cells that have the target antigen on the surface and can remain in the body for a long time, resulting in complete lasting remissions. Results of clinical trials and distinct generations of CARs may result in a change in the therapeutic strategy in DLBCL [10,28].
Conclusions
Our study provided the scientific framework for the assessment of the efficacy of R-CHOP versus other Rituximab-associated regimens in patients with de novo DLBCL. The data indicated that there are no significant differences in treatment endpoints between the two groups, supporting the hypothesis that all three Rituximab-based regimens provide good therapeutic alternatives for DLBCL patients with dose-dependent adaptation based on age and comorbidities.
Acknowledgments
The authors declare no financial or nonfinancial conflict of interest.
References
- 1.Carbone A, Gloghini A, Kwong YL, Younes A. Diffuse large B cell Lymphoma: using pathologic and molecular biomarkers to define subgroups for novel therapy. Ann Hematol. 2014;93:1263–1277. doi: 10.1007/s00277-014-2116-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Coiffier B, Lepage E, Briere J, Herbrecht R, Tilly H, Bouabdallah R, Morel P, Van Den Neste E, Salles G, Gaulard P, Reyes F, Lederlin P, Gisselbrecht C. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med. 2002;346(4):235–242. doi: 10.1056/NEJMoa011795. [DOI] [PubMed] [Google Scholar]
- 3.Gang AO, Strøm C, Pedersen M, d'Amore F, Pedersen LM, Bukh A, Pedersen BB, Moeller MB, Mortensen LS, Gadeberg OV, Ingeberg S, Mourits-Andersen T, Pulczynski S, d Nully Brown P. R-CHOEP-14 improves overall survival in young high-risk patients with diffuse large B-cell lymphoma compared with R-CHOP-14. A population-based investigation from the Danish Lymphoma Group. Ann Oncol. 2012;23(1):147–153. doi: 10.1093/annonc/mdr058. [DOI] [PubMed] [Google Scholar]
- 4.Wästerlid T, Szekely E, Werner Hartman L, Jerkeman M. R-CHOEP-14 is associated with superior overall survival compared to R-CHOP-21 and R-CHOP-14 in patients with DLBCL ≤70 Years-a Swedish lymphoma registry population based study. Blood. 2014;124(21):4427–4427. [Google Scholar]
- 5.Peyrade F, Jardin F, Thieblemont C, Thyss A, Emile JF, Castaigne S, Coiffier B, Haioun C, Bologna S, Fitoussi O, Lepeu G, Fruchart C, Bordessoule D, Blanc M, Delarue R, Janvier M, Salles B, André M, Fournier M, Gaulard P, Tilly H; Groupe d'Etude des Lymphomes de l'Adulte (GELA) investigators. Attenuated immunochemotherapy regimen (R-miniCHOP) in elderly patients older than 80 years with diffuse large B-cell lymphoma: a multicentre, single-arm, phase 2 trial. Lancet Oncol. 2011;12(5):460–468. doi: 10.1016/S1470-2045(11)70069-9. [DOI] [PubMed] [Google Scholar]
- 6.Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H. WHO classification of tumours of haematopoietic and lymphoid tissues. 4. Lyon: IARC Press; 2008. [Google Scholar]
- 7.Molina TJ, Canioni D, Copie-Bergman C, Recher C, Brière J, Haioun C, Berger F, Fermé C, Copin MC, Casasnovas O, Thieblemont C, Petrella T, Leroy K, Salles G, Fabiani B, Morschauser F, Mounier N, Coiffier B, Jardin F, Gaulard P, Jais JP, Tilly H. Young patients with non-germinal center B-cell-like diffuse large B-cell lymphoma benefit from intensified chemotherapy with ACVBP plus rituximab compared with CHOP plus rituximab: analysis of data from the Groupe d'Etudes des Lymphomes de l'Adulte/lymphoma study association phase III trial LNH 03-2B. J Clin Oncol. 2014;32(35):3996–4003. doi: 10.1200/JCO.2013.54.9493. [DOI] [PubMed] [Google Scholar]
- 8.Armitage JO. How I treat patients with diffuse large B-cell lymphoma. Blood. 2007;110(1):29–36. doi: 10.1182/blood-2007-01-041871. [DOI] [PubMed] [Google Scholar]
- 9.Ghielmini M, Vitolo U, Kimby E, Montoto S, Walewski J, Pfreundschuh M, Federico M, Hoskin P, McNamara C, Caligaris-Cappio F, Stilgenbauer S, Marcus R, Trneny M, Dreger P, Montserrat E, Dreyling M. Panel Members of the 1st ESMO Consensus Conference on Malignant Lymphoma. ESMO Guidelines consensus conference on malignant lymphoma 2011 part 1: diffuse large B-cell lymphoma (DLBCL), follicular lymphoma (FL) and chronic lymphocytic leukemia (CLL) Ann Oncol. 2013;24(3):561–576. doi: 10.1093/annonc/mds517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tilly H, Gomes da Silva M, Vitolo U, Jack A, Meignan M, Lopez-Guillermo A6, Walewski J, André M, Johnson PW, Pfreundschuh M, Ladetto M. ESMO Guidelines Committee.Diffuse large B-cell lymphoma (DLBCL): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015;26(suppl 5):v116–v125. doi: 10.1093/annonc/mdv304. [DOI] [PubMed] [Google Scholar]
- 11.Pfreundschuh M, Kuhnt E, Trümper L, Osterborg A, Trneny M, Shepherd L, Gill DS, Walewski J, Pettengell R, Jaeger U, Zinzani PL, Shpilberg O, Kvaloy S, de Nully Brown P, Stahel R, Milpied N, López-Guillermo A, Poeschel V, Grass S, Loeffler M, Murawski N. MabThera International Trial (MInT) Group.CHOP-like chemotherapy with or without rituximab in young patients with good-prognosis diffuse large-B-cell lymphoma: 6-year results of an open-label randomised study of the MabThera International Trial (MInT) Group. Lancet Oncol. 2011;12(11):1013–1022. doi: 10.1016/S1470-2045(11)70235-2. [DOI] [PubMed] [Google Scholar]
- 12.Miller TP1, Dahlberg S, Cassady JR, Adelstein DJ, Spier CM, Grogan TM, LeBlanc M, Carlin S, Chase E, Fisher RI. Chemotherapy alone compared with chemotherapy plus radiotherapy for localized intermediate- and high-grade non-Hodgkin’s lymphoma [see comments] N Engl J Med. 1998;339(1):21–26. doi: 10.1056/NEJM199807023390104. [DOI] [PubMed] [Google Scholar]
- 13.Fillet G, Bonnet C, Mounier N, et al. No role for chemoradiotherapy when compared with chemotherapy alone in elderly patients with localized low risk aggressive lymhoma: final results of the LNH93-4 GELA study [abstract] Blood. 2005;106(9a):Abstract 15–Abstract 15. [Google Scholar]
- 14.Zucca E1, Conconi A, Mughal TI, Sarris AH, Seymour JF, Vitolo U, Klasa R, Ozsahin M, Mead GM, Gianni MA, Cortelazzo S, Ferreri AJ, Ambrosetti A, Martelli M, Thiéblemont C, Moreno HG, Pinotti G, Martinelli G, Mozzana R, Grisanti S, Provencio M, Balzarotti M, Laveder F, Oltean G, Callea V, Roy P, Cavalli F, Gospodarowicz MK. International Extranodal Lymphoma Study Group.Patterns of outcome and prognostic factors in primary large-cell lymphoma of the testis in a survey by the International Extranodal Lymphoma Study Group. J Clin Oncol. 2003;21:20–27. doi: 10.1200/JCO.2003.11.141. [DOI] [PubMed] [Google Scholar]
- 15.Benevolo G1, Stacchini A, Spina M, Ferreri AJ, Arras M, Bellio L, Botto B, Bulian P, Cantonetti M, Depaoli L, Di Renzo N, Di Rocco A, Evangelista A, Franceschetti S, Godio L, Mannelli F, Pavone V, Pioltelli P, Vitolo U, Pogliani EM. Fondazione Italiana Linfomi.Final results of a multicenter trial addressing role of CSF flow cytometric analysis in NHL patients at high risk for CNS dissemination. Blood. 2012;120(16):3222–3228. doi: 10.1182/blood-2012-04-423095. [DOI] [PubMed] [Google Scholar]
- 16.Fletcher CD, Kahl BS. Central nervous system involvement in diffuse large B-cell lymphoma: an analysis of risks and prevention strategies in the post-rituximab era. Leuk Lymphoma. 2014;55(10):2228–2240. doi: 10.3109/10428194.2013.869326. [DOI] [PubMed] [Google Scholar]
- 17.Petrov L. Limfoamele maligne. In: Bojan A, Cucuianu A, Urian L, editors. Hematologie Clinica. Cluj-Napoca: Casa Cartii de Stiinta; 2009. pp. 199–255. [Google Scholar]
- 18.Shipp MA, Yeap BY, Harrington DP, Klatt MM, Pinkus GS, Jochelson MS, Rosenthal DS, Skarin AT, Canellos GP. The m-BACOD combination chemotherapy regimen in large-cell lymphoma: analysis of the completed trial and comparison with the M-BACOD regimen. J Clin Oncol. 1990;8(1):84–93. doi: 10.1200/JCO.1990.8.1.84. [DOI] [PubMed] [Google Scholar]
- 19.Longo DL, DeVita VT Jr, Duffey PL, Wesley MN, Ihde DC, Hubbard SM, Gilliom M, Jaffe ES, Cossman J, Fisher RI, Young RC. Superiority of ProMACE-CytaBOM over ProMACEMOPP in the treatment of advanced diffuse aggressive lymphoma: results of a prospective randomized trial [published erratum in J Clin Oncol; 1991; 9:710] J Clin Oncol. 1991;9(1):25–38. doi: 10.1200/JCO.1991.9.1.25. [DOI] [PubMed] [Google Scholar]
- 20.Fisher RI, Gaynor ER, Dahlberg S, Oken MM, Grogan TM, Mize EM, Glick JH, Coltman CA Jr, Miller TP. Comparison of a standard regimen (CHOP) with three intensive chemotherapy regimens for advanced non-Hodgkin's lymphoma. N Engl J Med. 1993;328(14):1002–1006. doi: 10.1056/NEJM199304083281404. [DOI] [PubMed] [Google Scholar]
- 21.Recher C, Coiffier B, Haioun C Molina TJ, Fermé C, Casasnovas O, Thiéblemont C, Bosly A, Laurent G, Morschhauser F, Ghesquières H, Jardin F, Bologna S, Fruchart C, Corront B, Gabarre J, Bonnet C, Janvier M, Canioni D, Jais JP, Salles G, Tilly H. Groupe d'Etude des Lymphomes de l'Adulte. Intensified chemotherapy with ACVBP plus rituximab versus standard CHOP plus rituximab for the treatment of diffuse large B-cell lymphoma (LNH03-2B): an open-label randomised phase 3 trial. Lancet. 2011;378(9806):1858–1867. doi: 10.1016/S0140-6736(11)61040-4. [DOI] [PubMed] [Google Scholar]
- 22.Stephen DS, Oliver W. Diffuse large B-cell Lymphoma and related diseases. In: Kaushansky K, Lichtman M, Prchal J, editors. Williams hematology. 9. Mc Graw Hill Education; 2016. pp. 1625–1639. [Google Scholar]
- 23.Sanz MA, Carreras E. Limfoma difuso de celulas B grandes. In: Rovira M, Sanz j, editors. Manual Practico de Hematologia Clinica. Antares; pp. 349–335. [Google Scholar]
- 24.Crump M, Kuruvilla J, Couban S MacDonald DA, Kukreti V, Kouroukis CT, Rubinger M, Buckstein R, Imrie KR, Federico M, Di Renzo N, Howson-Jan K, Baetz T, Kaizer L, Voralia M, Olney HJ, Turner AR, Sussman J, Hay AE, Djurfeldt MS, Meyer RM, Chen BE, Shepherd LE. Randomized comparison of gemcitabine, dexamethasone, and cisplatin versus dexamethasone, cytarabine, and cisplatin chemotherapy before autologous stem-cell transplantation for relapsed and refractory aggressive lymphomas: NCIC-CTG LY.12. J Clin Oncol. 2014;32:3490–3496. doi: 10.1200/JCO.2013.53.9593. [DOI] [PubMed] [Google Scholar]
- 25.Wilson WH. Treatment strategies for aggressive lymphomas: what works? Hematology Am Soc Hematol Educ Program. 2013;2013:584–590. doi: 10.1182/asheducation-2013.1.584. [DOI] [PubMed] [Google Scholar]
- 26.Hernandez-Ilizaliturri FJ, Deeb G, Zinzani PL, Pileri SA, Malik F, Macon WR, Goy A, Witzig TE, Czuczman MS. Higher response to lenalidomide in relapsed/refractory diffuse large B-cell lymphoma in nongerminal center B-cell-like than in germinal center B-cell-like phenotype. Cancer. 2011;117(22):5058–5066. doi: 10.1002/cncr.26135. [DOI] [PubMed] [Google Scholar]
- 27.Younes A, Thieblemont C, Morschhauser F Flinn I, Friedberg JW, Amorim S, Hivert B, Westin J, Vermeulen J, Bandyopadhyay N, de Vries R, Balasubramanian S, Hellemans P, Smit JW, Fourneau N, Oki Y. Combination of ibrutinib with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) for treatment-naive patients with CD20-positive B-cell non-Hodgkin lymphoma: non-randomised, phase 1b study. Lancet Oncol. 2014;15:1019–1026. doi: 10.1016/S1470-2045(14)70311-0. [DOI] [PubMed] [Google Scholar]
- 28.Pule M, Finney H, Lawson A. Artificial T-cell receptors. Cytotherapy. 2003;5(3):211–226. doi: 10.1080/14653240310001488. [DOI] [PubMed] [Google Scholar]