

Abstract
ABSTRACT: Purpose: The present study proposes the comprehensive ultrasound evaluation of a consecutive batch of patients with acute cardiogenic pulmonary edema. Method: The registry included all patients with acute pulmonary edema from 2 emergency hospitals between February and May 2016. During the first 3 days of admission, a transthoracic ultrasound was performed which included the parameters of systolic and diastolic function of the left ventricle, right ventricular systolic function, heart cavity dimensions, estimated pulmonary pressure, and the presence and severity of valvular disease. Results: A total of 70 patients were enrolled in the registry. The mean ejection fraction of the left ventricle was 39.5±11.4% and the average indexed end-diastolic volume was 77.7±29.5ml/m⊃2, above the upper limit of normal. All patients in whom diastolic function could be evaluated had a degree of diastolic dysfunction. Functional parameters of the right ventricle were normalized as average, and the mean pulmonary artery pressure was increased: 40.9±16.7mmHg. The most common valvular heart disease were mitral and tricuspid insufficiency, with moderate or severe impairment in 82.8%, respectively 65.7% of the patients.
Keywords: acute pulmonary edema, echocardiography, sistolic function
Introduction
Acute pulmonary edema (APE) is part of the acute heart failure syndromes (AHF) and is characterized by severe dyspnea, pulmonary congestion and decreased oxygen saturation.
In most cases, the cause is cardiogenic (cardiogenic APE) and is the sudden increase in filling pressures in the left cavities, which results in increased pulmonary capillary pressure resulting in pulmonary stasis.
Although acute diagnosis and management is primarily based on clinical picture and symptom relief, prognosis and long-term management depend especially on primary cardiac disease. This requires a comprehensive assessment of the heart, both structural and functional, an assessment in which echocardiography plays the most important role.
According to the European Society of Cardiology (ESC) guidelines, all patients with APE should be evaluated by echocardiography (Class I indication). This assessment should include the calculation of the left ventricular ejection fraction (LVEF), the identification of segmental kinetic disorders (e.g in case of an ischemic etiology), assessment of right ventricular function (VD), including estimation of pulmonary artery pressure, evaluation of diastolic function of left ventricle and the identification of possible valvular disease. According to different echocardiographic data, patients can be classified into several categories. The most widely used classification refers to LVEF and divides patients into the following categories:
- Reduced LVEF (<40%)
- Mid-range LVEF (40-49%)
- Preserved LVEF (>50%)
The role of echocardiography is more than observational, because patient management is directly dependent on echocardiographic parameters. For example, certain drug therapies (beta blockers, angiotensin converting enzyme inhibitors, antialdosteronics) have shown effectiveness in decreasing mortality, but only in patients with low LVEF. Other non-medical therapies, such as implantable defibrillator or resynchronization therapy, are only indicated for patients with LV systolic dysfunction.
Likewise, patients with heart failure of valvular etiology can benefit from cardiovascular surgery or interventional techniques for correction of valvular disease. Prognostic importance of LVEF has also been demonstrated, so patients with low ejection fraction have increased mortality compared to those with normal or mid-range LVEF [2,3].
Data from registries and studies on echocardiographic parameters in AHF syndromes are plenty, but information on the specific case of are scarce and limited to the most common indicators (systolic VS function and valvular disease) [4].
This study aims to analyze all the echocardiographic parameters of interest in patients with APE, with particular emphasis on the least investigated in registries, such as diastolic function and LV filling pressures, systolic function of right ventricle (RV), as well as data provided by tissue doppler.
Material and methods
The present article represents the detailed analysis of the ecographic parameters from a prospective observational study that enrolled consecutive patients with cardiogenic pulmonary edema between February 2016 and May 2016 at two emergency clinical hospitals: the "Bagdasar-Arseni" Emergency Clinical Hospital Bucharest and the Clinical Hospital County Emergency Craiova.
This study was approved by the Local Institutional Ethics Committee and patients had signed an informed consent before being included. All patients enrolled signed their agreement concerning data processing and publication. Inclusion criteria was diagnosis of cardiogenic pulmonary edema at admission. The diagnosis of APE was established on the basis of history and reasons for presentation (acute dyspnea with orthopnea), clinical examination (pulmonary rales in at least 1/2 of the lung area), pulmonary radiography (alveolar stasis) and the presence of hypoxemia (SaO⊂2<90%).
Transthoracic echocardiography, following a standardized protocol, was performed on all patients within the first 3 days of admission. Echocardiograms were performed by only one operator in each of the two centers, and the echocardiographs used were Aloka ProSound Alpha 10® and General Electric Vivid 7®. Among the parameters analyzed, we mention: LVEF, LV indexed end-diastolic volume, septal LV S', mitral E / A ratio, E / e' ratio, tricuspid annular systolic excursion, Fractional area change (FAC) of RV, S' on RV wall, RV-right atrium (RA) gradient, inferior vena cava (IVC) diameter, indexed atrial volume, presence and severity of valvular disease. The cut-off for normal values regarding dimensions, volumes and other echocardiographic parameters were established according to the guidelines of the American Society of Echocardiography (ASE) and the European Society (EACVI) [5]. The LV ejection fraction was calculated according to ESC recommendations by the Simpson biplane method. Another important parameter, less emphasized in HF studies, is diastolic dysfunction of the LV. This may be the major pathophysiological factor in patients with HF and preserved LVEF. Diastolic dysfunction was classified based on the mitral valve E / A ratio.
The LV filling pressure was calculated using the E / e 'ratio, where e' is the mean between the septal and lateral LV wall peak early velocity. Another LV function parameter is the maximum systolic velocity of the mitral annulus calculated by tissue Doppler at the basal level of interventricular septum(S')-normal value >6.5cm/s. According to ESC recommendations, calculating tissue velocities should be considered in all patients with heart failure (Class IIa indication) [1].
The systolic function of RV was evaluated using several parameters: TAPSE, FAC and S 'of the lateral wall of the RV. The TAPSE calculation was performed by M mode echocardiography in the apical incidence (TAPSE=17mm is the cut-off below which the parameter is abnormally low). Fractional area change (FAC) of RV is calculated similarly to EF of LV, but instead of volumes, the end-diastolic and end-systolic areas of RV are used (1). RV fractional area chance <35% indicates systolic dysfunction [5]. Systolic pulmonary artery pressure (PAPs) was estimated according to ESC recommendations [6].
Figure 1.
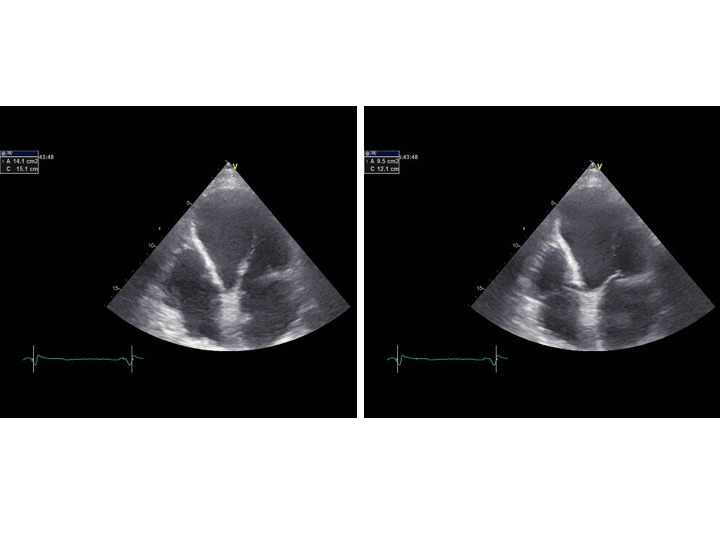
End-diastolic area (EDA) and end-systolic (ESA) area of the right ventricle. The fractional area change (FAC) is calculated as follows: FAC=(EDA-ESA)/EDA x 100
The data obtained were recorded in Microsoft Excel files, then processed statistically in order to analyze the relationships between study variables and to compare different paraclinical data to normal range data. We used Student’s t test, either for one-sample compared to a known mean value, or for two-samples, and Chi⊃2 test for independence.
Results
We enrolled 70 consecutive patients of which 36 at the Bagdasar-Arseni Emergency Clinical Hospital and 34 at the County Emergency Clinical Hospital, Craiova. The mean age was 72.1 years, exactly half of the patients being male.
The LV ejection fraction was calculated according to ESC recommendations by the Simpson biplane method, its mean value being 39.5±11.4%(1).
Table 1.
Mean and normal values of the echocardiographic parameters analyzed in the study. M=male; F=female gender; LVEF=left ventricular ejection fraction; EDV=tend-diastolic volume; ESV=end-systolic volume; IVS=interventricular septum; FAC=fractional area change; RV=right ventricle; RA=right atrium; LA=left atrium; ICV=inferior vena cava; sPAP=systolic pressure in the pulmonary artery. The established normal values were recorded from: [5,6]
Echographic parameter |
Mean study value |
Normal value |
LVEF (%) |
39.5±11.4 |
52-72 (M), 54-74 (F) |
Indexed EDV LV (ml/m2) |
77.7±29.5; 82.3 (M), 73.1 (F) |
34-74 (M), 29-61 (F) |
IVS diameter (mm) |
12.9±2.6; 12.7 (M), 13.2 (F) |
6-10 (M), 6-9 (F) |
LV septal S' (cm/s) |
4.9±1.2 |
>6.5 |
E/e' |
18.4±8.1 |
<14 |
TAPSE (mm) |
18.4±4.3 |
>17 |
FAC RV (%) |
40.3±7.8 |
>35 |
RV wall S' (cm/s) |
10.7±2.5 |
>9.5 |
IVC (mm) |
17.7±3.3 |
<21 |
estimated sPAP (mmHg) |
40.9±16.7 |
<37 |
Indexed LA end-diastolic volume (ml/m⊃2) |
53.7±22 |
16-34 |
Indexed LA end-systolic volume(ml/m⊃2) |
33.6±12.1; 34.6 (M), 32.6 (F) |
25±7 (M), 21±6 (F) |
There were 44.2% of patients with low LVEF (<40%), 34.3% with mid-range LVEF (40-49%) and 21.5% with preserved ejection fraction (≥50%). Of note is the important difference between the mean EF between males and females, which was 35%, respectively 44%. In fact, 57.1%of male patients had reduced EF and only 31.4% of women (p Chi⊃2=0.03). The mean S’ value in our study was 4.9±1.2cm/s.
The mean value of indexed end-diastolic volume of left ventricle was 77.7±29.5ml/m2, above the upper limit of the cut-off for normal values (61 ml/m2 for women and 74ml/m⊃2 for men). Also, the mean interventricular septum thickness (IVS), calculated from the longitudinal axis incidence, was 12.9±2.6mm (equivalent to a diagnosis of mild-moderate ventricular hypertrophy). Particularly, the mean diameter was higher among women (13.2mm) compared to men (12.7mm).
According to the study protocol, diastolic dysfunction was classified based on the mitral valve E/A ratio. A total of 22 patients (31.5%) had atrial fibrillation, which was the reason for which the diastolic function could not be appreciated using this parameter.
Of the other patients, all had a degree of diastolic dysfunction as follows: grade I-47.9% (23 patients), grade 2-22.9% (11 patients), grade 3-29.2% (14 patients).
The mean value of E/e’ ratio was 18.4±8.1, 70% of the patients had E /e ’≥14, representing elevated LV filling pressures.
The difference between males and females in the study was not statistically significant 19.2 vs. 17.7 (p Student >0.05).
The systolic function of RV was evaluated using several parameters: TAPSE, FAC and S 'of the lateral wall of the RV. The mean value of TAPSE was 18.4±4.3mm. 32.8%of the patients studied had TAPSE <17mm (12 males and 11 women) which is the lowest value of normal range. The mean FAC in this study was 40.3±7.8%, 15 patients (21.4%) had FAC <35%. The mean value of the RV wall S 'was 10.7±2.5cm/s, with 27 of the patients (37.1%) having an S' of <9.5cm/s. There were no significant differences between the male and female groups in the analysis of any of the RV function parameters (p Student >0.05). The mean estimated sPAP was 40.9±16.7mmHg (Table 1).
The mean left atrial (LA) indexed volume was 53.7±22ml/m2, corresponding to a severe LA dilation (>48ml/m2). Average right atrial (RA) indexed volume was 33.6±12.1ml/m2, equivalent to a slight RA dilation. On the concern of valvular disease, 82.8% of the patients had moderate or severe mitral regurgitation, 18.5% had mean or severe aortic stenosis and 65.7% had moderate or severe tricuspid regurgitation. The full prevalence values of valvular diseases values are found in Table 2.
Table 2.
Patients with valvular heart disease classified according to severity
Valvular heart disease |
Valvular disease severity (number of patients) |
|||
Without valvular disease |
Mild |
Moderate |
Severe |
|
Mitral regurgitation |
2 |
10 |
39 |
19 |
Mitral stenosis |
66 |
2 |
0 |
2 |
Inaortic regurgitation |
36 |
17 |
13 |
4 |
Aortic stenosis |
49 |
8 |
5 |
8 |
Triscuspid regurgitation |
5 |
19 |
38 |
8 |
Discussions
Echocardiography is not only an important exploration for establishing the diagnosis and etiology of heart failure, but it also provides prognostic data [1], even though there are relatively few studies on AHF patients [7,8].
The left ventricular systolic function, expressed by the ejection fraction (LVEF), is both a management orientation factor and an important prognostic factor [1,8]. In our study, the mean LVEF was 39.5%±11.4, which denotes an average mild to moderate systolic dysfunction. The LVEF had a quite balanced distribution:
• 15 patients with severe systolic dysfunction (LVEF≤30%)
• 16 patients with moderate systolic dysfunction (30%<LVEF<40%)
• 10 patients with mild-moderate systolic dysfunction (LVEF=40%)
• 14 patients with mild systolic dysfunction (40%<LVEF<50%)
• 15 patients without systolic dysfunction (LVEF≥50%)
Of note is the important difference between the mean LVEF among men (35%) and women (44%). Basically, 57.1% of male patients had reduced LVEF (<40%), and only 31.4% of women. The difference was statistically significant (p Chi⊃2=0.03).
The data collected from the current study are similar to those of the largest AHF registry in Romania, RO-AHFS. In a subgroup analysis of this register, Chioncel et al. showed mean LVEF among patients with APE was 39.2±13.2% [4]. Another international registry, OPTIMIZE-HF, demonstrated that patients with low LVEF had a higher risk of in-hospital mortality compared to those with preserved EF [9]. Accordingly, in our study, a high percentage of patients had significant systolic dysfunction which places them at a high risk of major cardiovascular events; consequently, they have entered a careful follow-up program.
With regard to diastolic function, all patients included in this study (in whom the diastolic function could be evaluated by E / A ratio) had a degree of impairment (grade I, II or III diastolic dysfunction). Considering these data and literature on the subject, we consider diastolic dysfunction and increased VS (E/e ') filling pressures as specific and common features of patients with APE. In some cases, it may precede systolic dysfunction and may even be the major pathophysiological factor of cardiac damage in patients with preserved LVEF [10].
The increase in filling pressures results in an increase in LA dimensions, expressed by the indexed volume. The primary role of the LA is to modulate the filling of the VS, both by its reservoir and conduct function and by its contraction. Although LA has structural and mechanical adaptive possibilities, increased pressures cause its expansion and remodeling [11]. The fact that the average LA indexed volume was not only above the upper limit of normal, but it was in the category of severe dilation, shows the importance of diastolic function and the important implications of its impairment. Dilatation of LA, as claimed by literature data, is a subtle expression of diastolic dysfunction, therefore an important prognostic indicator of the evolution of HF patients [12].
The function of the right ventricle (RV) is a prognostic indicator whose importance is extensively emphasized in recent years, including the recommendations of American and European echocardiography associations [1,5]. RV dysfunction has a negative prognostic role, correlating with the risk of death and worsening HF [13, 14, 15]. Although in this study the mean values of the RV function parameters were within the normal range, we consider that patients with RV dysfunction require careful follow-up, with a closer follow-up and adjustment of the therapy based on clinical and paraclinical data.
Study limitations
One of the study limitations is the observational character of this study, with the aim of having a background analysis of the echocardiographic assessment in patients with APE. Another limitation is the relatively small number of patients, which may question the generalization of data. Finally, another potential source of error is that examinations were conducted by two operators. We attempted to overcome this limitation by making an exact protocol for the echocardiographic examination.
Study limitations
Conclusion
Echocardiography is a useful method, both in explaining the etiology of acute pulmonary edema, and also in assessing complications and prognosis. The group of patients studied showed a relatively balanced distribution of LV systolic function, from severe systolic dysfunction to normal LVEF with a mean value in the range of mild to moderate dysfunction. Diastolic dysfunction was present in all patients, as confirmed by increased filling pressures and significant LA dilation. The systolic function of the RV was within the normal range for all the echocardiographic parameters assessed. The most common valvular diseases with significant impairment were mitral and tricuspid regurgitation.
Acknowledgments
The study was conducted in the Emergency County Hospital of Craiova (Tabaci Street, 1, 200642, Craiova) and in the Bagdasar-Arseni Emergency Clinical Hospital (12 Berceni Road, 4th District, 041915, Bucharest).
References
- 1.Ponikowski P, Voors AA, Anker SD. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–2200. doi: 10.1093/eurheartj/ehw128. [DOI] [PubMed] [Google Scholar]
- 2.Maggioni AP, Dahlström U, Filippatos G. EURObservational Research Programme: the Heart Failure Pilot Survey (ESC-HF Pilot) Eur J Heart Fail. 2010;12(10):1076–1084. doi: 10.1093/eurjhf/hfq154. [DOI] [PubMed] [Google Scholar]
- 3.Pocock SJ, Ariti CA, McMurray JJV. Predicting survival in heart failure: a risk score based on 39 372 patients from 30 studies. Eur Heart J. 2013;34(19):1404–1413. doi: 10.1093/eurheartj/ehs337. [DOI] [PubMed] [Google Scholar]
- 4.Chioncel O, Ambrosy AP, Bubenek S. Epidemiology, pathophysiology, and in-hospital management of pulmonary edema. J Cardiovasc Med. 2016;17(2):92–104. doi: 10.2459/JCM.0000000000000192. [DOI] [PubMed] [Google Scholar]
- 5.Lang RM, Badano LP, Mor-Avi V. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur Hear J-Cardiovasc Imaging. 2015;16(3):233–271. doi: 10.1093/ehjci/jev014. [DOI] [PubMed] [Google Scholar]
- 6.Galiè N, Humbert M, Vachiery J-L. ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. 2016;37(1):67–119. doi: 10.1093/eurheartj/ehv317. [DOI] [PubMed] [Google Scholar]
- 7.Zannad F, Garcia AA, Anker SD. Clinical outcome endpoints in heart failure trials: a European Society of Cardiology Heart Failure Association consensus document. Eur J Heart Fail. 2013;15(10):1082–1094. doi: 10.1093/eurjhf/hft095. [DOI] [PubMed] [Google Scholar]
- 8.Parissis JT, Nikolaou M, Mebazaa A, Ikonomidis I, Delgado J, Vilas-Boas F, Paraskevaidis I, Mc Lean A, Kremastinos D, Follath F. Acute pulmonary oedema: clinical characteristics, prognostic factors, and in-hospital management. Eur J Heart Fail. 2010;12(11):1193–1202. doi: 10.1093/eurjhf/hfq138. [DOI] [PubMed] [Google Scholar]
- 9.Abraham WT, Fonarow GC, Albert NM. Predictors of In-Hospital Mortality in Patients Hospitalized for Heart Failure. J Am Coll Cardiol. 2008;52(5):347–356. doi: 10.1016/j.jacc.2008.04.028. [DOI] [PubMed] [Google Scholar]
- 10.Smart N, Haluska B, Leano R, Case C, Mottram PM, Marwick TH. Determinants of functional capacity in patients with chronic heart failure: Role of filling pressure and systolic and diastolic function. Am Heart J. 2005;149(1):152–158. doi: 10.1016/j.ahj.2004.06.017. [DOI] [PubMed] [Google Scholar]
- 11.Wong M, Staszewsky L, Latini R, Barlera S, Glazer R, Aknay N, Hester A, Anand I, Cohn JN. Severity of left ventricular remodeling defines outcomes and response to therapy in heart failure. J Am Coll Cardiol. 2004;43(11):2022–2027. doi: 10.1016/j.jacc.2003.12.053. [DOI] [PubMed] [Google Scholar]
- 12.Grayburn PA, Appleton CP, DeMaria AN. Echocardiographic predictors of morbidity and mortality in patients with advanced heart failure. J Am Coll Cardiol. 2005;45(7):1064–1071. doi: 10.1016/j.jacc.2004.12.069. [DOI] [PubMed] [Google Scholar]
- 13.Frea S, Pidello S, Bovolo V, Iacovino C, Franco E, Pinneri F, Galluzzo A, Volpe A, Visconti M, Peirone A, Morello M, Bergerone S, Gaita F. Prognostic incremental role of right ventricular function in acute decompensation of advanced chronic heart failure. Eur J Heart Fail. 2016;18(5):564–572. doi: 10.1002/ejhf.504. [DOI] [PubMed] [Google Scholar]
- 14.Kjaergaard J, Akkan D, Iversen KK, Køber L, Torp-Pedersen C, Hassager C. Right ventricular dysfunction as an independent predictor of short- and long-term mortality in patients with heart failure. Eur J Heart Fail. 2007;9((6-7)):610–616. doi: 10.1016/j.ejheart.2007.03.001. [DOI] [PubMed] [Google Scholar]
- 15.Papaioannou VE, Stakos DA, Dragoumanis CK, Pneumatikos IA. Relation of tricuspid annular displacement and tissue Doppler imaging velocities with duration of weaning in mechanically ventilated patients with acute pulmonary edema. BMC Cardiovasc Disord. 2010;10(Lv):20–20. doi: 10.1186/1471-2261-10-20. [DOI] [PMC free article] [PubMed] [Google Scholar]