

Abstract
Introduction:
Ardhavabhedaka described under Shiroroga (disease of the head in Ayurveda) occurs due to vitiation of Tridosha (all of three biological humors). The signs and symptoms of migraine can be correlated with Ardhavabhedaka. Looking to the agony caused during acute episode of migraine and unavailability of specific management and only symptomatic management in conventional medicine this study was conducted. Agnikarma is indicated in severe pain and Pathyadi decoction is indicated in the management of Shiroroga.
Aim and Objective:
The aim of this study was to evaluate the efficacy of Agnikarma and Pathyadi decoction in the management of Ardhavabhedaka (migraine).
Materials and Methods:
A total of 15 patients were selected from outpatient department of Ayurveda College. Agnikarma was done on affected temporal side of face, dot type for 1 time, once in a week followed by application of honey–Ghee. Along with this, Pathyadi decoction 40 ml twice a day for 30 days was also given.
Results:
Statistically highly significant relief (P < 0.001) was noted in headache, photophobia and phonophobia and statistically significant (P < 0.05) relief was noted in vomiting, nausea and vertigo.
Conclusion:
Agnikarma along with Pathyadi decoction can be considered as an effective line of treatment to manage Ardhavabhedaka (migraine).
Keywords: Agnikarma, Ardhavabhedaka (migraine), Pathyadi decoction
Introduction
Ardhavabhedaka is one of the Shiroroga (disorder of head) which can be correlated with migraine having symptoms like paroxysmal unilateral (half cranial) headache sometime associated with vertigo, nausea, photophobia and phonophobia. As per Acharya Sushruta Ardhavabhedaka occur due to vitiation of Tridosha (Vata – Pitta – Kapha).[1] While Acharya Charaka had mentioned that vitiated Vata/Vata - Kapha are involved in manifestation of Ardhavabhedaka,[2] while Acharya Vagbhatta believed that Ardhavabhedaka occurs due to vitiated Vata.[3]
According to International headache society, migraine is the most common neurovascular headache and is a common disabling primary headache disorder. It is now recognized as a chronic illness, not simply as headache. Migraine headache often limited the degree to which headache sufferers could engage in regular activities.[4] In the global burden of disease survey 2010, it was ranked as the third most prevalent disorder and 7th highest specific cause of disability worldwide.[5] The world health organization (WHO) ranks migraine among the world’s most disabling medical illness. It is three times more common in women than men.
As per Ayurveda, ‘pain can not occur without involvement of Vata Dosha’.[6] Agnikarma (local cauterization) having Ushna (hot), Tikshna (penetrating) property may pacify the aggravated Vata Dosha and thus, Agnikarma can be beneficial in Ardhavabhedaka. Furthermore, Agnikarma is easy and quick procedure to perform and also effective. Thus, Agnikarma has been selected as the choice of treatment procedure in this trial.
Pathyadi deccoction[7] is mentioned in Sharangdhara Samhita, especially in the management of Shiroroga. This decotion has ingredients having Ushna Virya (hot potency) and Vata Shamaka (Vata subsiding) property which can be beneficial in Ardhavabhedaka as this disease has dominancy of vitiation of Vata and Kapha Dosha, dominancy. Further it is also being widely practiced to manage Shiroroga.
Aim and objectives
The aim of this study is to evaluate the efficacy of Agnikarma and Pathyadi decoction in the management of Ardhavabhedaka (migraine).
Materials and Methods
Patients
In the present study, 15 patients fulfilling the criteria for diagnosis of Ardhavabhedaka (migraine) were selected from the outpatient department of Shalakyatantra Govt. Akhandanand Ayurveda college, Ahmedabad, Gujarat, India.
Drug
Pathyadi decoction was procured from Government Ayurved Pharmacy, Rajpipala, Gujarat, India.
The research protocol was approved by the Institutional ethics committee (Certi. No. 28; date: 25/06/2016) and registered in clinical trial registry of India vide CTRI/2017/01/007845. Informed consent from each enrolled patient was obtained before commencement of the treatment.
Diagnostic criteria
-
The diagnosis was made on following criteria of migraine.
- At least 5 episode of headache, in past history fortnightly or at 10 days interval or random occurrence (Pakshahat (madrosis)– Dashahat– Aksmatprvartate)
- Headache episode lasting for 4–72 h
-
Headache has at least 2 or 3 of the following four characteristics.
- Unilateral location
- Pulsating quality
- Moderate or severe pain intensity
- Aggravation by or leading to avoidance of routine physical activity (e.g., walking or climbing stairs).
-
During headache at least one of the following:
- Nausea or vomiting
- Photophobia and or phonophobia.
Inclusion criteria
Patients fulling the diagnostic criteria of either sex having age between 16 to 70 years and willing to participate and provide consent were included.
Exclusion criteria
Patients not eligible for Agnikarma as per Ayurvedic texts
Referred pain in one half of the head due to disorder of eye, ear, nose, throat, teeth etc.
Patients having migraine other than Migraine without Aura
PatientsZ suffering from diabetes, tuberculosis, hypertension, malignancy, any other general debilitating health condition, needing surgical intervention (polyp etc.) or patients who were on any other medications which may interfer with trial treatment.
Examinations
Vitals examination – Pulse, temperature, blood pressure, respiration and general examination of eye, ear, nose, throat, head and oral cavity was done before initiating the treatment.
Investigations were carried out before treatment like routine hematological tests complete blood count (CBC), bleeding time (BT), clotting time (CT).
Treatment trial
All the patients (n = 15) were administered treatment trial as follow.
Agnikarma.[8]
Equipment: Panchdhatu Shalaka [made up of Tamra (copper), Loha (iron), Yashada (zinc), Rajata (silver), Vanga (lead)] [Figure 1]
Figure 1.

Agnikarma Shalaka (instrument used for Agnikarma)
Schedule: 4 schedules at the interval of 7 days
Type: Bindu (Dot type) (1 time) (dimension – 2–3 mm) [Figure 2]
Time: Morning (after breakfast)
Site:[9] Bhru–Lalat–Shankha Pradesha (Temporal area of the face of affected side) [Figure 2]
Precautions: Patients were asked to have light meal before Agnikarma.
Pre–procedure: Before Agnikarma, site was cleaned with warm water swab to avoid any possibility of infection. Agnikarma Shalaka was heated on gas stove till red hot. Mixture of Honey – Ghrita in unequal quantity was kept ready.
Procedure: Patient was asked to lie in lateral side, affected side facing upward. Most tender point was elicited and marked on temporal side of face. With red hot Shalaka, a small dot type burn (diameter 2 – 3 mm), till Twaka Dagdha (superficial burn) was done
Post-Procedure: immediately after burn, mixture of honey (1 ml)– Ghrita (2 ml) (unequal quantity) was applied to that site
Instructions: After Agnikarma, patients were instructed to avoid washing that part for 24 hours to avoid any infection. After Agnikarma, all the patients were asked to apply mixture of honey – Ghrita 2 times a day for next 7 days for better wound healing effect.
Pathyadi decoction[6] was given in the dose[10] of 40 ml, [Table 1]. Time of intake was 2 times/day, morning and evening (empty stomach) for 30days (along with Agnikarma).
Figure 2.

Agnikarma: Site of performing of Agnikarma
Table 1.
Ingredient of Pathyadi deccoction
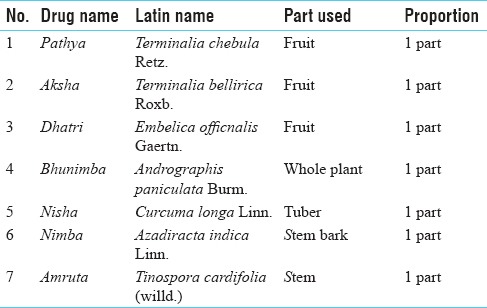
Preparation[11] for Pathyadi decoction to this patient was given 20 gms of coarse powder of Pathyadi decoction and instructed to soak that powder overnight in 320 ml of water. Next morning, patient was instructed to boil that mixture till quantity was reduced to 40ml. then it should be filtered and drink while it is luke warm.
Assessment criteria
Symptoms of Ardhavabhedaka were given gradations as per the severity
Headache was graded according to HIT-6 [Headache impact test– 6] (annexure 1)
Results were assessed before and after the treatment on the basis of change in the grade.
Assessment of overall effect of therapy
Overall effect of therapy was assessed in terms of complete remission if 100% improvement in symptoms and no recurrences during the follow-up period was observed. When improvement in symptoms was between 75% and 100%, it was considered as marked improvement and as moderate improvement when the improvement in symptoms was between 50% and 75%. Mild improvement when the improvement in the symptoms was between 25% and 50%. Changes up to 25% were taken as no change.
Statistical analysis
Obtained data of before and after treatment was analyzed statistically with Wilcoxon signed rank test by using Sigma Stat, Ver-3.5 (2007), by Systat Software Inc., San Jose, California.
Observation
In the present study, one patient dropped out due to migration to other state. In present clinical trial, maximum number of patients, i.e. 66.67% patients belonged to age group of 31–40. 60% of patients were female, 46.67% were homemakers, 80% were Hindu, 93.33% were married, 20% of patients had education till graduation, 60% of patients were from middle class, 40% of patients were having moderate appetite, 66.67% patients were having regular defecation, 53% of patients having Vata-Pitta Sharirika Prakriti (physical constituation) and 53% of patients were having Tamasika Manasa Prakriti (psycololgical status).
In the present study, upon observing the etiological factors of Ardhavabhedaka, it was found that maximum number of patients were having Vishamashana (taking food irrespective of time/hunger) that is, 47%; while 33% of patients were doing Adhyashana (having food before digestion of previous meal) and 20% of patients had dominancy of Lavana Rasa (salty) in the regular food.
By further analysis, it was observed that 100% of patients had headache, 60% of patients had nausea, 46.67% of patients had vomiting, 20% had vertigo, 86.67% of the patients complained of photophobia and 93.33% of patients had phonophobia.
Results
The present trial drugs provided highly significant (P < 0.001) result in headache, nausea, vomiting, vertigo and photophobia [Table 2]. No any complication of the procedure or adverse drug reaction was found during this trial.
Table 2.
Effect of therapy
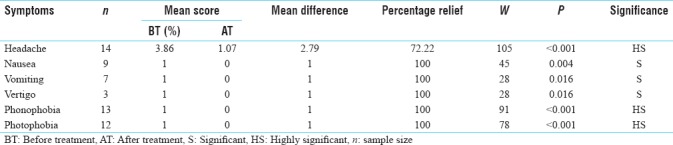
Effect of therapy on sign and symptoms
In headache, 72.22% relief was found which was statistically highly significant at the level of P < 0.001. In Hrillasa (nausea), 100% relief was found and the result was statistically significant at the level of P = 0.004. In Chhardi (vomiting), 100% relief was found, the result was statistically significant at the level of P 0.016. In Bhrama (vertigo), 100% relief was found, which was statistically significant at the level of P 0.016. In Shabda Asahishnuta (phonophobia), 100% relief was found, which was statistically highly significant at the level of P < 0.01. In Prakasha Asahishnuta (photophobia), 100% relief was found, which was statistically highly significant at the level of P < 0.01.
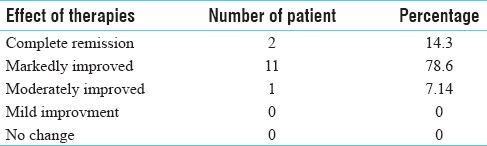
Overall effect of therapy
On analyzing overall effect of therapy; maximum number of patients had marked improvement, that is, 11 (78.6%); 2 (14.3%) patient had complete remission while 1 (7.14%) patient had moderate improvement [Table 3].
Table 3.
Overall effect of therapy
Discussion
In present study Shirah-Shoola (headache) was taken as chief complaint and 100% patients had headache. Along with headache there were associated complaints like nausea, vomiting, vertigo, phonophobia and photophobia.
Among these nausea and vomiting indicated vitation of Rasavaha Srotasa in manifestation of Ardhavabhedaka. While Bhrama is one of the features of vititated Vata and Pitta Dosha. photophobia and phonophobia is not specified as symptoms in Ardhavabhedaka, but is the progressive stage of disease, loss of vision and hearing impairment (Nayana and Shravana Vinashyet) may be present as complication. Hence, photophobia and phonophobia may be considered as systemic manifestations of the disease.
In the present study, in Headache, 72.22% (P < 0.001) relief and 100% relief in nausea, vomiting, vertigo, phonophobia and photophobia was found. Three patients (21.43%) had the recurrence of headache at the end of the course but severity, duration and frequency were decreased significantly. All these patients had to take analgesic medicine before treatment but after treatment none of the patients had to take analgesics for the same.
Probable mode of action of Agni Karma
Heat is often used to relieve pain in many diseases, however, the exact mode of its action and mechanism is not clearly understood.
According to Ayurveda, Agni has Ushna Guna. This Ushna Guna gets transferred to Twaka (skin) by Agnikarama. This Guna normalises Vata and Kapha. This might have helped to reduce Shira – Shoola in Ardhavabhedaka.
The local thermos therapy may increase tissue metabolism and toxins. Heat may stimulate lateral spinothalamic tract which leads stimulation of descending pain inhibitory fibers which release endogenous opioid peptide which binds with opiod receptors at substantia gelatinosa rolandi which inhibit release of P-substance (Presynaptic inhibition) and blockage of transmission of pain sensation occur.[12]
Heat has also been claimed to act as a counter irritant. It has been suggested that such responses might be explained on the basis of the pain gate control theory. In this theory, it is believed that nociceptor fibers residing in the superficial skin get stimulated by heat. These fast-acting fibers after activating, close the gate for slow-acting fibers for chronic pain.[13]
Probable mode of action of Pathyadi decoction
This formulation is a multidrug combination and is indicated specially in Shiroroga in Shrangdhara Samhita.[6] It contains 67% Dravya with Ushna Virya (hot potency) and Madhura Vipaka (sweet post digestion effect) 43% drugs are Tridoshaghna (all three Dosha pacification). So by all virtues cited above, it normalizes the vitiated Vata-Kapha Dosha. In addition, Pathyadi decoction contains drugs such as Guduchi [Tinospora cordifolia (willd.)], Nimba [Azadiracta indica Linn.], and Haridra [Curcuma longa Linn.] possessing Raktaprasadaka (blood purifier) property that may normalize vitiated Rakta Dhatu (oxygen carrying capacity of blood). Drugs such as Guduchi [Tinospora cordifolia (willd.)] and Amalaki [Embelica officinalis Gaertn.] have Dipana (appetizing) property. These drugs will normalize Ama (by product toxins after digestion), as Ama get decreased it may subside Ajirna (Indigestion).
It is reported that most of the drugs of Pathyadi decoction also possess analgesic, anti-inflammatory, a nervine tonic property which might have helped to reduce pain.
Conclusion
Agnikarma and Pathyadi decoction provided significant relief in the symptoms of Ardhavabhedaka (migraine). Agnikarma has provided significant relief in pain, whereas, Pathyadi decoction may have acted on systemic symptoms such as nausea, vomiting and vertigo.
Thus Agnikarma and Pathyadi decoction therapy are effective in the management of Ardhavebhedaka (migraine). Further research work on Agnikarma as pain management should be done on large sample size.
Financial support and sponsorship
This study was financially supported by Gujarat Ayurved University, Jamnagar.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Acharya YT, editor. Ch. 25., Ver. 15. Varanasi: Chaukhambha Surbharti Publication; 2014. Sushruta Samhita of Acharya Sushruta. Uttartantra. Reprint Edition; p. 655. [Google Scholar]
- 2.Acharya YT, editor. Reprint Edition. Ch. 9., Ver. 75. New Delhi: Chaukhambha Publication; 2014. Charaka Samhita of Agnivesha, Siddhi Sthana; p. 721. [Google Scholar]
- 3.Tripathi B, editor. Ashtang Hridayam of Vagbhatta, Uttara Sthana. Reprint Edition. Ch. 23., Ver. 7. New Delhi: Chaukhambha Sanskrit Pratishthan; 2011. p. 1051. [Google Scholar]
- 4.International Headache Society. Reprints and permissions. [Last retrieve on 2015 Apr 14];Cephalalgia, July-2013. 33(9):644. [Doi: 10.1177/0333102413485658] Available from: http://www.sagepub.co.uk/journalsPermissions.nav, cep.sagepub.com . [Google Scholar]
- 5.Tripathi B, editor. Reprint Edition. Ch. 2., Ver. 143. Varanasi: Chaukhambha Surbharti Prakashana; 2011. Sharangdhara Samhita of Acharya Sharangdhar, Madhyam Khanda; p. 154. [Google Scholar]
- 6.Singhal GD, editor. Sushruta Samhita of Acharya Sushruta with English translation, Sutra Sthan, Reprint Edition. Ch. 17, Ver. 7. Delhi: Chaukhambha Sanskrit Pratishthan; 2015. p. 160. [Google Scholar]
- 7.Acharya YT, editor. Charaka Samhita of Agnivesha, Siddhi Sthana. Reprint Edition. Ch. 9., Ver. 78. New Delhi: Chaukhambha Publication; 2014. p. 721. [Google Scholar]
- 8.Acharya YT, editor. Sushruta Samhita of Acharya Sushruta. Sutrasthana. Reprint Edition. Ch. 12., Ver. 9. Varanasi: Chaukhambha Surbharti Publication; 2014. p. 52. [Google Scholar]
- 9.Tripathi B, editor. Sharangdhara Samhita of Acharya Sharangdhar, Madhyam Khanda. Reprint Edition. Ch. 2., Ver. 3. Varanasi: Chaukhambha Surbharti Prakashana; 2011. p. 133. [Google Scholar]
- 10.Shrivastav S, editor. Sharangdhara Samhita of Acharya Sharangdhara with “Jivanprada” commentary, Madhyam Khanda. Reprint Edition. Ch. 2, Ver. 1. Varanasi: Chaukhambha Orienetalia; 2013. p. 134. [Google Scholar]
- 11. [Last retrieve on 2017 Apr 21]. Available from: https://www.cambridge.org/core/services/aopcambridge-core/content/view/S0317167100047697 .
- 12.Umesh S, Manjusha R, Dwivedi RR, Narayan B. Role of Agnikarma and Ajmodadivati in the management of Sandhigata Vata W.S.R. cervical spondylosis. AYU. 2009;30:345–9. [Google Scholar]
- 13.Sangoli KS, Venkatesh BA. [Last retrieved on 2016 Dec 18];The role of Agnikarma in the management of Ardhavabhedaka. Indian J Anc Med Yoga. 2015 Jan-Mar;8(1):15–24. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.