

Abstract
Objectives:
To examine whether (a) childhood neighborhood context predicts alcohol use disorder, nicotine dependence, and cannabis use disorder symptoms at age 39 and (b) socioeconomic status during young adulthood mediates these relationships. Gender differences were also examined.
Study design:
Seattle Social Development Project, a prospective longitudinal study of 808 individuals followed from ages 10 to 39 in Seattle, Washington, United States. The sample was gender balanced (51% male).
Methods:
Alcohol, nicotine, and cannabis use disorder symptoms were assessed using the DSM-IV-based Diagnostic Interview Schedule. Childhood neighborhood data consisted of 10 neighborhood-level variables from the 1990 national census, which were consolidated using principal component analyses. Two components with eigenvalues greater than 1 were extracted—neighborhood disadvantage and neighborhood stability. Educational attainment and employment status represented socioeconomic status during young adulthood. Covariates included baseline symptoms of psychopathology, baseline substance use, gender, ethnicity, and childhood socioeconomic status at the family level. Negative binomial regression was used as the primary modeling strategy. Six models for each outcome measure were estimated. The first three models examined associations between two neighborhood components and each substance use outcome measure. Next, we tested the second research question by adding unemployment and college graduate indicators at age 30 as potential mediators underlying the link between childhood neighborhood context and three substance use measures.
Results:
Study findings revealed that childhood neighborhood stability significantly reduced alcohol and cannabis use disorder symptoms nearly 3 decades later. Path analyses suggested that socioeconomic status during the transition to adulthood did not influence these relationships, but rather had independent effects on problematic nicotine and cannabis use. Furthermore, the effects of childhood neighborhood factors on problematic nicotine use were stronger for men.
Conclusions:
Neighborhood characteristics during childhood may be important factors for alcohol and cannabis use disorder symptoms among adults and nicotine dependence disorder symptoms among men. Prevention efforts that address community stability and disadvantage can and should start in childhood, with a focus on intervention targets that might gain salience later in life to discourage the development and persistence of problematic substance use in adulthood.
Keywords: problematic substance use, neighborhood characteristics in childhood, socioeconomic status, young adulthood
Introduction
More than 20 million Americans experience substance dependence or abuse in 2013,1 costing U.S. taxpayers more than $700 billion annually.1–4 Substance use is an inherently developmental phenomenon that often begins during adolescence and evolves across the life course,5 highlighting the need to identify factors contributing to the emergence and persistence of substance use problems across the life course.
Childhood neighborhood characteristics and adulthood problematic substance use
Socioecological frameworks posit that neighborhood context may function as an important factor shaping adult substance use.6,7 Emerging evidence has corroborated this perspective, although results have varied across studies.8–10 Importantly, the life course perspective suggests that factors contributing to adulthood substance use can originate in earlier developmental periods.11–13 By extension, childhood neighborhood factors, such as neighborhood-level poverty, may play a role in adulthood substance use either indirectly via their influence on adolescent substance use14,15 or directly, as found in other adulthood developmental outcomes.16–18 However, existing relevant studies have often relied on cross-sectional data,19,20 with very few notable exceptions,21,22 and thus the impact of childhood neighborhood on adulthood substance use is largely unknown. Further, the few existing longitudinal studies linking childhood neighborhood context to adulthood substance use have either focused on truncated periods that extend only to participants’ early 20s—the normative peak age 21—or targeted individual perceptions about a neighborhood rather than neighborhood context objectively assessed at a neighborhood level.22 As such, a prospective investigation of the impact of childhood neighborhood context on adulthood problematic substance use that persists beyond the normative peak age is lacking. This represents an important gap in the knowledge base for locating effective intervention targets that are implicated in earlier developmental periods.
Role of socioeconomic status during the transition to adulthood
The impact of childhood neighborhood context on adulthood problematic substance use remains understudied, and thus even fewer longitudinal tests have examined mechanisms underlying the link between childhood neighborhood context and adulthood problematic substance use. The life course perspective provides a conceptual anchoring point for this inquiry. Elder (1998) defined the life course as “a sequence of socially defined, age-graded events and roles that the individual enacts over time” (p. 941 ). During the life course, individuals establish foundations for socioeconomic status (SES), such as completing school and moving into paid employment.23,24
Two strands of existing research have provided evidence that a person’s attained SES—i.e., SES as an adult—might play a role in the link between childhood neighborhood context and adulthood substance use. First, childhood neighborhood context, such as neighborhood-level poverty, can influence educational attainment,25–27 an SES indicator, because institutional resources critical to academic achievement and educational attainment, such as quality schools, are lacking in impoverished neighborhoods.28,29 Similarly, childhood neighborhood-level poverty can also shape labor force participation in adulthood,30 another SES indicator, because social capital that often functions as an important means of securing a job might be limited in impoverished neighborhoods, which likely affect an individual’s likelihood of finding a job. 26,31
Further, adults’ SES may influence their substance use. Role compatibility theory32 and age-graded social control theory,33 for example, hypothesize that substance use is expected to decrease as individuals assume more adult roles. This is because achieving and then maintaining success in life course markers, such as finding and keeping a paid job, are incompatible with problematic substance use. Supporting such contentions, the risk of alcohol abuse and dependence, for example, is elevated among individuals who did not go to college.34,35 Similarly, unemployment predicts increased heavy drinking36 and alcohol use and nicotine dependence disorder symptoms.22
Taken together, it is feasible that adults’ SES may mediate the association of childhood neighborhood context with adulthood problematic substance use. To our knowledge, no existing longitudinal study has examined this possibility. Such gaps in our knowledge base limit the public health system’s ability to locate effective intervention targets for adulthood substance use across the life course.
Present study
The present study addressed two central research questions. First, is childhood neighborhood context, objectively measured at age 10, associated with alcohol use disorder, nicotine dependence, and cannabis use disorder symptoms at age 39? Second, does participants’ SES during the transition to adulthood (age 30) mediate the link between childhood neighborhood context and disorder symptoms almost 3 decades later? From the life course perspective, the 30s represent an important transition period because shifts in the life course markedly decelerate during this period and an individual’s position in life course markers, such as educational attainment and employment status, stabilize.37,38
Further, we examined potential gender differences in the link between childhood neighborhood factors and adulthood substance use, considering empirical evidence suggesting such differences and a lack of consensus regarding for which gender the impact is more amplified. The negative impact of contemporaneous neighborhood poverty (i.e., adulthood neighborhood poverty) on adulthood problematic drinking was exacerbated among women in some studies39,40 and among men in other studies.41 It remains unknown whether such gender differences exist in the link between childhood neighborhood characteristics and adulthood problematic substance use, particularly for substances other than alcohol.
Methods
Sample
Data were from the Seattle Social Development Project (SSDP), a longitudinal panel study that followed participants from ages 10 to 39 with consistently high retention rates (88% of the still-living sample included in the age 39 survey). Seventy-seven percent of fifth graders and their parents from 18 elementary schools serving high-crime neighborhoods in Seattle, Washington, consented to be part of the study in 1985, resulting in a panel of 808 participants.
Data collection was conducted yearly in childhood and adolescence (ages 10–16) and at eight points in adulthood (ages 18–39), for a total of 15 waves. Initially, students completed group-administered questionnaires in their classrooms. Beginning in 1988 (the age 13 interview), trained interviewers conducted interviews in person using paper and pencil. Starting at the age 21 wave, interviews were completed in person with the use of a laptop. Survey questions changed year to year to correspond to developmental characteristics and research questions.
Retention rates averaged 90% across study years, ranging from 87% in the first wave of Grade 6 students to 88% of the still-living sample included in the age 39 survey (n = 677). The sample was racially diverse (47% European American, 26% African American, 22% Asian American, and 5% Native American) and gender balanced (51% male), and 19% of participants were from families with low SES. Further details of the sampling strategy and data collection procedures are described elsewhere.42 The study was approved by the human subjects review committee at the affiliated university.
Measures
Substance use disorder symptoms: Diagnostic Interview Schedule (age 39)
Substance use disorder symptoms were assessed using an abbreviated version of the Diagnostic Interview Schedule43 based on the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV).44 Three disorder symptom indexes were created by summing the number of DSM-IV criteria met for alcohol abuse and dependence (range = 0–11), nicotine dependence (range = 0–7), and cannabis abu se and dependence (range = 0–11) disorder symptoms. A symptom count was chosen rather than diagnoses, considering an ongoing and unresolved debate regarding whether DSM-IV abuse and dependence diagnoses accurately represent severity.45 Relatedly, the diagnosis threshold might not reflect a natural cutoff.46–48
Childhood neighborhood context at age 10
Neighborhood data consisted of variables from the 1990 national census. Participant addresses in 1985 (at age 10) were geocoded and linked to their census block groups. Following suggestions in prior studies,49,50 census block groups in the SSDP data, the finest spatial unit available, were used to represent boundaries of neighborhoods. The average of 2.8 participants per block group at age 10 (ICC < .01) indicated that spatial clustering would not be significant. Consistent with other studies using SSDP data at age 15,51 the present analysis focused on 10 neighborhood-level characteristics that were consolidated using principal components analyses with promax rotation. Of note, we decided to use participant addresses at age 10—the SSDP assessment point that best represents childhood52—rather than adolescence. Two components with eigenvalues greater than 1 were extracted and factor loadings were evaluated to define their nature. The number and nature of these two components are in line with prior studies.51,53 The first component of neighborhood disadvantage was represented by the first eight neighborhood items, such as percentage of adults without a high school diploma and percentage of families living in poverty (see Appendix A for a list of items and factor loadings), primarily capturing the overall economic deprivation of the neighborhood. Higher scores indicated more neighborhood-level disadvantage. In comparison, the second component was mainly represented by the last two neighborhood items, the percentage of individuals living in a neighborhood for 5 years or more and the percentage of owner-occupied homes, primarily capturing neighborhood stability (see Appendix A for a list of items and factor loadings). Higher scores indicated more neighborhood-level stability.
Socioeconomic status at age 30
SES indicators included educational attainment (1 = college graduate, 0 = otherwise) and employment status (1 = unemployed, 0 = otherwise) at age 30. The employment status variable was constructed using data from a life-history calendar.54,55 If participants were unemployed and not out of the labor force for voluntary reasons (e.g., full-time student or homemaker) at age 30, they were considered unemployed. Of note, we focused on educational attainment and employment status, which are developmentally appropriate and important indicators of SES in young adulthood, considering that many young adults experience frequent changes in income.56
Covariates
Covariates included average substance use at ages 13 and 14, measured prospectively using self-reported measures of past-month alcohol, tobacco, and cannabis use. Prior symptoms of psychopathology were also included in the model as covariates, measured by internalizing (affective disorder and anxiety problems) and externalizing (attention deficit and hyperactivity, oppositional defiant, and conduct problems) scales reported by teachers on the Child Behavior Checklist (CBCL) when participants were age 10 to 12.57,58 Scales were created by standardizing the average score on the internalizing and externalizing subscales, following CBCL guidelines. Previous analyses of our data have found these scales to be reliable and valid.59 In addition, sociodemographic covariates included race and ethnicity, represented by binary indicator variables for three ethnic minority groups (African American, Asian American, and Native American, with Caucasian American as the referent); gender (1 = male, 0 = female); and low childhood SES at the family level (1 = lowest 25% of household income and lived with parents with less than 12 years of education, 0 = otherwise).
Analysis
Considering that the distributional nature of substance use outcome measures (i.e., nonnegative integers showing positive skewness with evidence of overdispersion), negative binomial regression was used as the main modeling strategy.60 Coefficients from regression models were exponentiated to generate rate ratios that described the proportional change in the number of symptoms associated with a 1-unit change in a predictor.61
Six models for each outcome measure were estimated. The first three models examined associations between childhood neighborhood disadvantage and childhood neighborhood stability and each substance use outcome measure (i.e., alcohol, nicotine, and cannabis abuse or dependence disorder symptoms). Next, we tested the second research question by adding age 30 unemployment and college graduate indicators as potential mediators underlying the focal association. Of note, fit indexes for a path analysis are less relevant in the present paper, because all possible paths were estimated (i.e., a fully saturated model). Finally, interaction terms between gender and childhood neighborhood disadvantage and childhood neighborhood stability were tested to examine possible gender differences in the association of childhood neighborhood factors with adulthood problematic substance use. All models adjusted for gender, race, substance use at ages 13 or 14, internalizing and externalizing at ages 10–12, and low childhood SES.
All analyses were conducted in Mplus (version 7.3). Missing data were handled with full-information maximum likelihood, a recommended method to handle missingness62 that is available in Mplus.
Results
Childhood neighborhood factors at age 10 and substance use at age 39
Table 1 reports descriptive statistics for main analysis variables (n=808). Of note, a specific sample size for each variable differed, as missingness varied across waves. On average, participants reported less than one abuse or dependence symptoms for all three substances. Regarding SES at age 30, 26% of the study participants were college graduates and 16% were unemployed. Correlations among model variables are reported in Table 2, all of which were in the expected direction except that childhood neighborhood disadvantage was not significantly correlated with substance use symptoms.
Table 1.
Descriptive statistics of all analysis variables
| Variable | n | M or % | SD |
|---|---|---|---|
| Alcohol use disorder symptoms age 39 (range 0–11) | 599 | .48 | 1.36 |
| Nicotine use disorder symptoms age 39 (range 0–7) | 604 | .56 | 1.20 |
| Cannabis use disorder symptoms age 39 (range 0–11) | 608 | .28 | 1.00 |
| Neighborhood disadvantage age 10 | 792 | .00 | 1.00 |
| Neighborhood stability age 10 | 792 | .00 | 1.00 |
| College graduate by age 30 | 718 | 26% | |
| Unemployment at age 30 | 688 | 16% | |
| Drug use age 10–12 | 787 | 0.00 | 0.31 |
| Internalizing age 10–12 | 759 | 0.01 | 0.12 |
| Externalizing age 10–12 | 760 | 0.01 | 0.20 |
| Gender (male=1) | 808 | 51% | |
| Childhood socioeconomic status age 10–16 | 804 | 19% | |
| Race (white=1) | 808 | 47% |
Table 2.
Correlations among model variables
| 1 | 2 | 3 | 4 | 5 | 6 | |
|---|---|---|---|---|---|---|
| 1. Alcohol use disorder symptoms | ||||||
| 2. Nicotine use disorder symptoms | .19** | |||||
| 3. Cannabis use disorder symptoms | .29** | .33** | ||||
| 4. Neighborhood disadvantage | .04 | .01 | .00 | |||
| 5. Neighborhood stability | −.09* | −.04 | −.08* | −.34** | ||
| 6. College graduate (by age 30) | −.06 | −.23** | −.13** | −.14** | .09* | |
| 7. Unemployment (at age 30) | .04 | .11** | .10* | .09* | −.07 | −.14** |
p < .05.
p < .01.
First, we estimated models predicting each of the three substance use disorder symptom measures (Table 3, Models 1–3). Results from the mo del with both childhood neighborhood factors (Model 3) showed that neighborhood stability at age 10 was associated with a reduced number of alcohol use disorder symptoms at age 39 (rate ratio [RR] = 0.73; 95% CI = 0.59, 0.92). For every standard deviation increase in residential stability, there was a 27% decrease in risk of alcohol use disorder symptoms at age 39. Neighborhood stability was also marginally associated with a reduced number of cannabis use disorder symptoms (RR = 0.76; 95% CI = 0.57, 1.01; p < .10). Neither of the two neighborhood factors was associated with nicotine dependence disorder symptoms.
Table 3.
Negative binomial models of alcohol, nicotine, and cannabis use disorder symptoms at age 39, predicted by childhood neighborhood factors
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| RR | 95% CI | RR | 95% CI | RR | 95% CI | RR | 95% CI | RR | 95% CI | |
| Alcohol | ||||||||||
| ND | 1.03 | 0.80, 1.32 | 0.94 | 0.72, 1.21 | 0.95 | 0.69, 1.30 | 0.90 | 0.70,1.15 | ||
| NS | 0.74** | 0.60, 0.93 | 0.73** | 0.59, 0.92 | 0.73** | 0.58, 0.92 | 0.58** | 0.41,0.82 | ||
| ND × gender | 0.96 | 0.62, 1.49 | ||||||||
| NS × gender | 1.49 | 0.95,2.34 | ||||||||
| Nicotine | ||||||||||
| ND | 1.05 | 0.86, 1.28 | 1.01 | 0.82, 1.25 | 0.70 | 0.53, 0.93 | 0.99 | 0.81,1.21 | ||
| NS | 0.91 | 0.77, 1.09 | 0.92 | 0.76, 1.11 | 0.93 | 0.77, 1.13 | 1.23 | 0.92,1.65 | ||
| ND × gender | 1.71** | 1.26, 2.34 | ||||||||
| NS × gender | 0.59** | 0.42,0.83 | ||||||||
| Cannabis | ||||||||||
| ND | 0.90 | 0.65, 1.25 | 0.86 | 0.62, 1.20 | 0.94 | 0.63, 1.40 | 0.88 | 0.63,1.24 | ||
| NS | 0.77 | 0.59, 1.02 | 0.76* | 0.57, 1.01 | 0.77* | 0.58, 1.02 | 0.94 | 0.61,1.46 | ||
| ND × gender | 0.79 | 0.47, 1.32 | ||||||||
| NS × gender | 0.66 | 0.39,1.13 | ||||||||
Note. Sample sizes: alcohol (n = 599); nicotine (n = 604); cannabis (n = 608). Neighborhood disadvantage and stability measured at age 10. All models adjusted for earlier symptoms of psychopathology; earlier use of alcohol, tobacco, and cannabis; race; socioeconomic status at individual level; and gender. ND = neighborhood disadvantage; NS = neighborhood stability; RR = rate ratio; CI= confidence interval.
p < .10.
p < .05.
Role of socioeconomic status at age 30
Next, SES indicators at age 30 were added to Model 3 as potential mechanisms underlying the focal linkage. As shown in Figure 1, the effects of neighborhood stability remained significantly associated with adulthood alcohol (RR = 0.73; 95% CI = 0.58, 0.91) and cannabis (RR = 0.75; 95% CI = 0.57, 0.97) use disorder symptoms, even after accounting for SES indicators.
Figure 1.
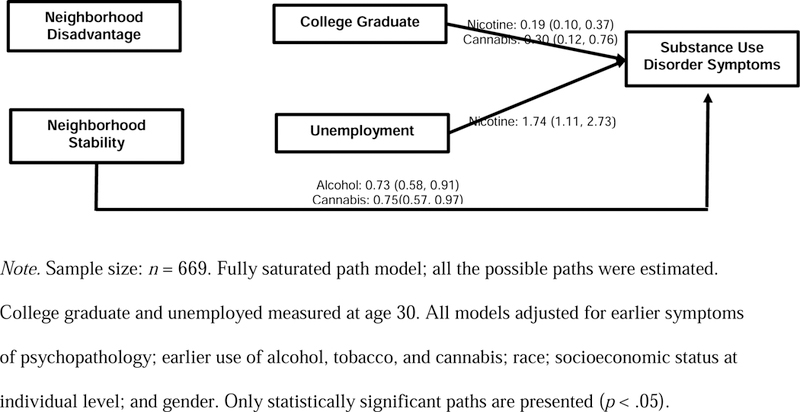
Association of childhood neighborhood factors with alcohol, nicotine, and cannabis use disorder symptoms at age 39 and mediation by SES markers at age 30.
In addition, results suggest that an individual’s educational attainment and employment status are particularly important predictors of nicotine dependence disorder symptoms. Having a college degree was associated with a reduced number of nicotine dependence disorder symptoms (RR = 0.19; 95% CI = 0.10, 0.37). Unemployment increased the number of nicotine dependence disorder symptoms (RR = 1.74; 95% CI = 1.11, 2.73). Having a college degree was associated with fewer cannabis use disorder symptoms (RR = 0.30; 95% CI = 0.12, 0.76).
Gender differences
Analyses with gender interaction terms (Table 3, Models 4 and 5) revealed that the effect of childhood neighborhood disadvantage and neighborhood stability on nicotine dependence symptoms was stronger for men. There was no evidence of gender differences in the effect of childhood neighborhood disadvantage or neighborhood stability on alcohol or cannabis use disorder symptoms.
Discussion
The present study prospectively assessed the potential impact of childhood neighborhood factors on adulthood alcohol, nicotine, and cannabis use disorder symptoms and the possible role of participants’ SES during the transition to adulthood (age 30) in the focal link. Possible sex differences were also evaluated. The present study aimed to strengthen the public health system’s ability to locate effective intervention targets in earlier developmental periods and across the life course.
As suggested by socioecological frameworks5–7 and the life course perspective,11–13 our findings suggest that childhood neighborhood context, particularly neighborhood stability, lessens problematic alcohol and cannabis use for both genders and nicotine use for men at age 39, beyond the normative peak age of substance use. Our findings extend prior studies reporting that residential stability at a neighborhood level might decrease substance use problems during the normative peak age—early 20s. 21 A long-lasting impact of neighborhood stability on adulthood substance use might be attributable to earlier neighborhood-based social capital and social networks, which tend to be positively associated with neighborhood stability.63,64 Earlier neighborhood-based social capital and networks have been linked to lower levels of substance use in adolescents, such as fewer alcohol problems in adolescence.65,66 Our findings suggest that these effects may carry over to adulthood.
The childhood neighborhood disadvantage factor, which primarily captured the overall economic deprivation of a given neighborhood, was associated with the number of nicotine dependence disorder symptoms only for men. These findings appear to contradict some prior studies reporting either the statistically significant impact of neighborhood economic deprivation on adulthood binge drinking41 or nonsignificant gender interaction terms in the context of smoking.20 However, these prior studies focused on a more concurrent impact of neighborhood (i.e., neighborhood poverty during adulthood). The impact of the socioeconomic aspects of a neighborhood might be more temporally proximal for adulthood substance use. Alternatively, childhood neighborhood poverty might interact with adulthood neighborhood poverty rather than exerting an independent impact on adulthood substance problems, as suggested by the resource substitution hypothesis.67 Investigating unique and joint impacts of childhood and adulthood neighborhood contexts could contribute to a deeper understanding of the association between neighborhood context and substance use across the life course.
The current findings did not support our hypothesis that SES during the critical transition period from young adulthood to adulthood37,38,68 might mediate the link between childhood neighborhood context and adulthood problematic substance use. Rather, an individual’s SES at age 30 tended to exert independent effects on adulthood problematic substance use, particularly nicotine dependence symptoms at age 39. In addition, having a college degree was associated with fewer cannabis use disorder symptoms. A similar association did not emerge regarding alcohol use disorder symptoms. Potentially, the effects of role incompatibility32 and social control33 of adulthood SES on substance use might be more potent for highly stigmatized substances, such as cigarettes,69 or illegal substances, such as cannabis.
The current findings should be interpreted in the context of a few methodological limitations. First, all measures except for childhood neighborhood measures were reported by participants, potentially raising concerns about response bias. Second, we relied on point-in-time measures of childhood neighborhood characteristics. Although bounded by data coverage of the SSDP and our intentional focus on childhood, our dependence on these point-in-time measures might have limited our statistical power to detect differences in substance abuse based on the childhood neighborhood disadvantage factor. However, a prior study reported that point-in-time measures of neighborhood context are not likely to produce bias in estimation due to limited variation in childhood neighborhood characteristics over time.70 Also, neighborhood stability, also using point-in-time measures, had predictive capacity for outcome measures, lending more confidence to our neighborhood measures. Nevertheless, replicating the present study with data that cover multiple childhood data points, particularly early childhood, might be fruitful for the aforementioned analytic reason and considering the importance of early childhood family poverty reported in the context of other adulthood developmental outcomes.71 Third, except for medical purposes, cannabis use was illegal in the state of Washington during all waves of SSDP data collection except for the last wave (age 39), which may have influenced the study results. Future research should investigate whether such change in legal restrictions on cannabis use might affect the associations examined in the current study, particularly those between adulthood SES indicators and cannabis use. Finally, the SSDP sample, a community sample from a regional area, overrepresented high-crime neighborhoods at the initial assessment. As such, variation in economic deprivation of the neighborhood might be limited, possibly leading to the statistically nonsignificant results related to the neighborhood disadvantage factor. Replication of study findings with other datasets conducted in other regional areas will be a fruitful future direction.
The current study made three significant contributions to the existing literature. First, by capitalizing on prospective longitudinal data from a 29-year period, we investigated the potential impact of childhood neighborhood factors, objectively assessed at a neighborhood level, on adulthood problematic substance use that persisted beyond the normative peak age. This approach enabled us to assess whether childhood neighborhood context might cast long-lasting effects on adulthood substance use problems. Second, we examined potential mechanisms that might clarify how childhood neighborhood context influences adulthood substance use. Third, gender differences were tested to elucidate childhood neighborhood factors that are unique to each gender. To our knowledge, no other existing studies have incorporated these unique strengths.
In conclusion, our findings suggest that neighborhood characteristics during childhood may be an important factor for alcohol and cannabis use disorder symptoms among adults and nicotine dependence disorder symptoms among men. Community-based prevention efforts such as Communities That Care72 or environmental strategies such as the Community Trials Project73,74 might provide effective guidance for addressing community stability. The current study also suggests that individuals’ attained SES should be considered in policy and prevention efforts seeking to discourage the development and persistence of substance use problems in adulthood. Taken together, our study findings support the argument that prevention efforts can and should start in childhood and should identify additional intervention targets later in life.
Highlights.
Childhood neighborhood stability significantly reduced problematic alcohol and cannabis use nearly 3 decades later.
An individual’s socioeconomic status during young adulthood tended to exert independent effects on adulthood problematic substance use, particularly nicotine dependence and cannabis use symptoms.
The effects of childhood neighborhood factors on problematic nicotine use were stronger for men.
Acknowledgements
We would like to extend our gratitude to the SSDP study participants for their continued contribution to the study.
Funding
This research was supported by grants 1R01DA033956-01, and 1R01DA024411-05-07 from the National Institute on Drug Abuse. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies. The funding agencies played no role in the study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit this article for publication.
Appendix A.
Factor loadings for census measures of neighborhood variables at age 10.
| Census Variable by Block Group | Neighborhood Disadvantage | Neighborhood Stability |
|---|---|---|
| Percentage of adults without high school diploma | .84 | −.03 |
| No. of racial groups more than 10% of population | .83 | .24 |
| Proportion of households receiving public assistance income | .84 | −.20 |
| Percentage of youth aged 10–17 | .95 | .32 |
| Percentage of families living in poverty | .80 | −.24 |
| Percentage of men in labor force and unemployed | .69 | −.14 |
| Percentage of women in labor force and unemployed | .73 | −.10 |
| Percentage of single-parent, female-headed households | .94 | −.01 |
| Percentage of owner-occupied homes | .24 | .83 |
| Percentage of families in same house from 1985–1990 | .20 | .96 |
| Eigenvalue | 5.64 | 1.92 |
| Percentage of variance | 56% | 19% |
Footnotes
Statement of Ethical Approval
All study procedures were approved by the Human Subjects Review Committee at the affiliated university.
Competing Interests
None declared.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Substance Abuse and Mental Health Services Administration (SAMHSA). Results from the 2013 National Survey on Drug Use and Health: Summary of National Findings Rockville, MD: Substance Abuse and Mental Health Services Administration; 2014. [Google Scholar]
- 2.Centers for Disease Control and Prevention. Excessive Drinking Costs U.S. $223.5 Billion 2014; www.cdc.gov/features/alcoholconsumption/.
- 3.National Drug Intelligence Center. National Drug Threat Assessment Washington, DC: United States Department of Justice; 2011. [Google Scholar]
- 4.U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress. A Report of the Surge on General Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2014. [Google Scholar]
- 5.Zucker RA. Alcohol use and the alcohol use disorders: A developmental-biopsychosocial systems formulation covering the life course. In: Cicchetti D, Cohen DJ, editors. Developmental psychopathology 2nd ed. New York: Wiley; 2006. p. 620–56. [Google Scholar]
- 6.Bronfrenbrenner U Making human beings human: Bioecological perspectives on human development Thousand Oaks, CA: Sage; 2005. [Google Scholar]
- 7.Bronfrenbrenner U, Morris PA. The ecology of developmental processes. In: Lerner R, editor. Handbook of child psychology: 1 Theoretical models of human development 5th ed. New York: Wiley; 1998. p. 992–1028. [Google Scholar]
- 8.Bryden A, Roberts B, Petticrew M, McKee M. A systematic review of the influence of community level social factors on alcohol use. Health & Place 2013;21:70–85. [DOI] [PubMed] [Google Scholar]
- 9.Jackson N, Denny S, Ameratunga S. Social and socio-demographic neighborhood effects on adolescent alcohol use: A systematic review of multi-level studies. Social Science & Medicine 2014;115:10–20. [DOI] [PubMed] [Google Scholar]
- 10.Karriker-Jaffe KJ. Areas of disadvantage: A systematic review of effects of area‐level socioeconomic status on substance use outcomes. Drug and alcohol review 2011;30:84–95. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Elder GH Jr., Time, human agency, and social change: Perspectives on the life course. Social Psychology Quarterly 1994;57:4–15. [Google Scholar]
- 12.McLeod JD, Almazan EP. Connections between childhood and adulthood. In: Mortimer J, Shanahan MJ, editors. Handbook of the life course New York: Kluwer Academic/Plenum; 2003. p. 391–411. [Google Scholar]
- 13.Shanahan MJ. Pathways to adulthood in changing societies: Variability and mechanisms in life course perspective. Annu Rev Sociol 2000;26:667–92. [Google Scholar]
- 14.Breslin FC, Adlaf EM. Part-time work and adolescent heavy episodic drinking: The influence of family and community context. Journal of Studies on Alcohol 2005;66:784–94. [DOI] [PubMed] [Google Scholar]
- 15.Tucker JS, Pollard MS, De La Haye K, Kennedy DP, Green HD. Neighborhood characteristics and the initiation of marijuana use and binge drinking. Drug Alcohol Depend 2013;128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Duncan GJ, Magnuson K. The Long Reach of Early Childhood Poverty. Stanford University: Stanford Center for the Study of Poverty and Inequality; 2011.
- 17.Leventhal T, Brooks-Gunn J. Moving to Opportunity: an Experimental Study of Neighborhood Effects on Mental Health. Am J Public Health 2003;93:1576–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ludwig J, Duncan GJ, Gennetian LA, Katz LF, Kessler RC, Kling JR, et al. Neighborhood Effects on the Long-Term Well-Being of Low-Income Adults. Science 2012;337:1505–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Galea S, Ahern J, Tracy M, Vlahov D. Neighborhood Income and Income Distribution and the Use of Cigarettes, Alcohol, and Marijuana. American Journal of Preventive Medicine 2007;32:S195–S202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Karriker-Jaffe KJ. Neighborhood socioeconomic status and substance use by U.S. adults. Drug and Alcohol Dependence 2013;133:212–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Buu A, Dipiazza C, Wang J, Puttler LI, Fitzgerald HE, Zucker RA. Parent, family, and neighborhood effects on the development of child substance use and other psychopathology from preschool to the start of adulthood. J Stud Alcohol Drugs 2009;70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lee JO, Jones T, Rhew IC, Kosterman R, Lovasi G, Catalano RF, et al. The association of unemployment from age 21 to 33 with substance use disorder symptoms at age 39: The role of childhood neighborhood characteristics. Drug and Alcohol Dependence 2017;174:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Macmillan R The structure of the life course: Classic issues and current controversies. Advances in Life Course Research 2005;9:3–24. [Google Scholar]
- 24.Schulenberg JE, Maggs JL. A developmental perspective on alcohol and other drug use during adolescence and the transition to young adulthood. Journal of Studies on Alcohol, Suppl 2002;14:54–70. [DOI] [PubMed] [Google Scholar]
- 25.Jencks C, Mayer S. The social consequences of growing up in a poor neighborhood. In: Lynn. LE, McGeary. MFH, editors. Inner-city poverty in the United States Washington, DC: National Academy Press; 1990. p. 111–86. [Google Scholar]
- 26.Pebley AR, Sastry N. Neighborhoods, poverty and children’s well-being: A review; 2003.
- 27.Wodtke GT, Harding DJ, Elwert F. Neighborhood Effects in Temporal Perspective: The Impact of Long-Term Exposure to Concentrated Disadvantage on High School Graduation. American Sociological Review 2011;76:713–36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Brooks-Gunn J, Duncan GJ, Aber L. Neighborhood poverty New York: Russell Sage; 1997. [Google Scholar]
- 29.Small ML, Newman K. Urban poverty after The Truly Disadvantaged: The rediscovery of the family, the neighborhood, and culture. Annu Rev Sociol 2001;27:23–45. [Google Scholar]
- 30.Galster G, Santiago A, Lucero J, Cutsinger J. Adolescent neighborhood context and young adult economic outcomes for low-income African Americans and Latinos. Journal of Economic Geography 2016;16:471–503. [Google Scholar]
- 31.Haveman R, Wolfe B. Succeeding Generations: On the Effects of Investments in Children New York: Russell Sage; 1994. [Google Scholar]
- 32.Yamaguchi K, Kandel DB. On the resolution of role incompatibility: A life event history analysis of family roles and marijuana use. American Journal of Sociology 1985;90:1284–325. [Google Scholar]
- 33.Laub JH, Sampson RJ. Shared Beginnings, Divergent Lives: Delinquent Boys to Age 70 Cambridge, MA: Harvard University Press; 2003. [Google Scholar]
- 34.Oesterle S, Hawkins JD, Hill KG. Men’s and Women’s Pathways to Adulthood and Associated Substance Misuse. Journal of Studies on Alcohol and Drugs 2011;72:763–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Harford TC, Yi HY, Hilton ME. Alcohol abuse and dependence in college and noncollege samples: A ten-year prospective follow-up in a national survey. Journal of Studies on Alcohol 2006;67:803–9. [DOI] [PubMed] [Google Scholar]
- 36.Mossakowski KN. Is the duration of poverty and unemployment a risk factor for heavy drinking? Social Science & Medicine 2008;67:947–55. [DOI] [PubMed] [Google Scholar]
- 37.Arnett JJ. Emerging adulthood. A theory of development from the late teens through the twenties. Am Psychol 2000;55:469–80. [PubMed] [Google Scholar]
- 38.Rindfuss RR. The young adult years: Diversity, structural change, and fertility. Demography 1991;28:493–512. [PubMed] [Google Scholar]
- 39.Kuipers MAG, van Poppel MNM, van den Brink W, Wingen M, Kunst AE. The association between neighborhood disorder, social cohesion and hazardous alcohol use: A national multilevel study. Drug and Alcohol Dependence 2012;126:27–34. [DOI] [PubMed] [Google Scholar]
- 40.Matheson FI, White HL, Moineddin R, Dunn JR, Glazier RH. Drinking in context: the influence of gender and neighbourhood deprivation on alcohol consumption. Journal of Epidemiology and Community Health 2012;66:e4–e. [DOI] [PubMed] [Google Scholar]
- 41.Fone DL, Farewell DM, White J, Lyons RA, Dunstan FD. Socioeconomic patterning of excess alcohol consumption and binge drinking: a cross-sectional study of multilevel associations with neighbourhood deprivation. BMJ Open 2013;3:e002337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Hawkins JD, Smith BH, Hill KG, Kosterman R, Catalano RF, Abbott RD. Understanding and preventing crime and violence. In: Thornberry TP, Krohn MD, editors. Taking Stock of Delinquency: An Overview of Findings from Contemporary Longitudinal Studies New York: Springer; 2003. p. 255–312. [Google Scholar]
- 43.Robins L, Helzer JE, Croghan J, Williams JBW, & Spitzer RL NIMH Diagnostic Interview Schedule. Version III Rockville, MD: National Institute of Mental Health; 1981. [Google Scholar]
- 44.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-IV) 4th ed. Washington DC: American Psychiatric Association; 1994. [Google Scholar]
- 45.Langenbucher JW, Labouvie E, Martin CS, Sanjuan PM, Bavly L, Kirisci L, et al. An application of item response theory analysis to alcohol, cannabis, and cocaine criteria in DSM-IV. Journal of Abnormal Psychology 2004;113:72–80. [DOI] [PubMed] [Google Scholar]
- 46.Beseler CL, Hasin DS. Cannabis dimensionality: Dependence, abuse and consumption. Addictive Behaviors 2010;35:961–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Hasin DS, Liu XH, Alderson D, Grant BF. DSM-IV alcohol dependence: a categorical or dimensional phenotype? Psychological Medicine 2006;36:1695–705. [DOI] [PubMed] [Google Scholar]
- 48.Saha TD, Compton WM, Pulay AJ, Stinson FS, Ruan WJ, Smith SM, et al. Dimensionality of DSM-IV nicotine dependence in a national sample: An item response theory application. Drug and Alcohol Dependence 2010;108:21–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Duncan DT, Kawachi I, Subramanian SV, Aldstadt J, Melly SJ, Williams DR. Examination of How Neighborhood Definition Influences Measurements of Youths Access to Tobacco Retailers: A Methodological Note on Spatial Misclassification. American Journal of Epidemiology 2014;179:373–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Spielman SE, Yoo EH. The spatial dimensions of neighborhood effects. Social Science & Medicine 2009;68:1098–105. [DOI] [PubMed] [Google Scholar]
- 51.Herrenkohl TI, Hawkins JD, Abbott RD, Guo J. Correspondence between youth report and census measures of neighborhood context. Journal of Community Psychology 2002;30:225–33. [Google Scholar]
- 52.Centers for Disease Control and Prevention. Middle childhood (9–11). 2018. [Google Scholar]
- 53.Sampson RJ. Great American city: Chicago and the enduring neighborhood effect Chicago, IL: University of Chicago Press; 2012. [Google Scholar]
- 54.Axinn WG, Pearce LD, Ghimire D. Innovations in life history calendar applications. Social Science Research 1999;28:243–64. [Google Scholar]
- 55.Caspi A, Moffitt TE, Thornton A, Freedman D, Amell JW, Harrington H, et al. The life history calendar: A research and clinical assessment method for collecting retrospective event-history data. International Journal of Methods in Psychiatric Research 1996;6:101–14. [Google Scholar]
- 56.Adler NE, Stewart J. Health disparities across the lifespan: Meaning, methods, and mechanisms. In: Stewart J, Adler N, editors. Biology of disadvantage: Socioeconomic status and health Oxford: Blackwell Publishing; 2010. p. 5–23. [DOI] [PubMed] [Google Scholar]
- 57.Achenbach TM. CBCL 4–18: YSR and TRF Profiles Burlington, VT: University of Vermont Press; 1991. [Google Scholar]
- 58.Achenbach TM, Edelbrock C. Manual for the Child Behavior Checklist and Revised Child Behavior Profile Burlington, VT: University of Vermont Press; 1983. [Google Scholar]
- 59.Kosterman R, Hawkins JD, Mason WA, Herrenkohl TI, Lengua LJ, McCauley E. Assessment of Behavior Problems in Childhood and Adolescence as Predictors of Early Adult Depression. Journal of Psychopathology and Behavioral Assessment 2010;32:118–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Coxe S, West SG, Aiken LS. The Analysis of Count Data: A Gentle Introduction to Poisson Regression and Its Alternatives. Journal of Personality Assessment 2009;91:121–36. [DOI] [PubMed] [Google Scholar]
- 61.Atkins DC, Gallop RJ. Rethinking how family researchers model infrequent outcomes: A tutorial on count regression and zero-inflated models. Journal of Family Psychology 2007;21:726–35. [DOI] [PubMed] [Google Scholar]
- 62.Schlomer GL, Bauman S, Card NA. Best Practices for Missing Data Management in Counseling Psychology. Journal of Counseling Psychology 2010;57:1–10. [DOI] [PubMed] [Google Scholar]
- 63.Brisson DS, Usher CL. Bonding social capital in low-income neighborhoods. Family Relations 2005;54:644–53. [Google Scholar]
- 64.Drukker M, Kaplan C, Feron F, van Os J. Children’s health-related quality of life, neighbourhood socio-economic deprivation and social capital. A contextual analysis. Social Science & Medicine 2003;57:825–41. [DOI] [PubMed] [Google Scholar]
- 65.Duncan SC, Duncan TE, Strycker LA. A multilevel analysis of neighborhood context and youth alcohol and drug problems. Prevention Science 2002;3:125–33. [DOI] [PubMed] [Google Scholar]
- 66.Winstanley EL, Steinwachs DM, Ensminger ME, Latkin CA, Stitzer ML, Olsen Y. The association of self-reported neighborhood disorganization and social capital with adolescent alcohol and drug use, dependence, and access to treatment. Drug and Alcohol Dependence 2008;92:173–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Ross CE, Mirowsky J. The interaction of personal and parental education on health. Social Science & Medicine 2011;72:591–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Oesterle S Background paper: Pathways to young adulthood and preventive interventions targeting young adults. Institute of Medicine and National Research Council, Improving the health, safety, and well-being of young adults: Workshop summary Washington, DC: National Academies Press; 2013. p. 147–76. [PubMed] [Google Scholar]
- 69.Stuber J, Galea S, Link BG. Smoking and the emergence of a stigmatized social status. Social Science & Medicine 2008;67:420–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Kunz J, Page ME, Solon G. Are point-in-time measures of neighborhood characteristics useful proxies for children’s long-run neighborhood environment? Economics Letters 2003;79:231–7. [Google Scholar]
- 71.Duncan GJ, Ziol-Guest KM, Kalil A. Early-Childhood Poverty and Adult Attainment, Behavior, and Health. Child Development 2010;81:306–25. [DOI] [PubMed] [Google Scholar]
- 72.Hawkins JD, Oesterle S, Brown EC, Abbott RD, Catalano RF. Youth Problem Behaviors 8 Years After Implementing the Communities That Care Prevention System: A Community-Randomized Trial. JAMA Pediatrics 2014;168:122–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Grube JW. Preventing sales of alcohol to minors: Results from a community trial. Addiction 1997;92:S251–S60. [PubMed] [Google Scholar]
- 74.Holder HD, Gruenewald PJ, Ponicki WR, Treno AJ, Grube JW, Saltz RF, et al. Effect of community-based interventions on high-risk drinking and alcohol-related injuries. Journal of the American Medical Association 2000;284:2341–7. [DOI] [PubMed] [Google Scholar]