

INTRODUCTION
Sexual minority youth are more likely to report higher levels of substance use compared to their heterosexual peers (Marshal et al., 2008). According to Minority Stress Theory, anti-gay victimization, discrimination, and internalized stigma place sexual minority youth at risk for adverse health outcomes, such as substance use (Meyer, 2003). However, there are significant gender differences among sexual minority youth. The disparity in reported substance use between sexual minority girls (SMGs) and heterosexual girls are much larger than the disparities seen between sexual minority and heterosexual boys (Marshal et al., 2008). Despite these differences, few studies have focused on substance use disparities between SMGs and heterosexual girls (please see Hipwell et al., 2013, Marshal, King et al., 2012; Marshal, Sucato et al., 2012, Montano, McCauley, Miller, Chisolm, & Marshal, 2016). Identifying risk and protective factors for substance use among SMGs may provide needed information about potentially modifiable factors as targets for reducing these disparities.
Previous research has suggested that parent-child communication can be protective against substance use throughout adolescence (Hawkins, Catalano, & Miller, 1992; Kingon & O’Sullivan, 2001). Parent-child communication refers to the degree to which adolescents feel they can talk freely with their parents. This could involve factual information, such as what the adolescent is doing, or emotional topics, such as how the adolescent responds to a stressful event. This construct has been measured by the frequency of, the quality of, or the adolescents’ satisfaction with the communication with their parents (Ryan, Jorm, & Lubman, 2010). The frequency of parent-child communication has been a target for substance use prevention (Beatty, Cross, & Shaw, 2008); however, the evidence for impact of the frequency of parent-child communication on adolescent substance use has been mixed. In one study, more frequent parent-child communication was associated with lower onset rates of alcohol and nicotine use among adolescents (Cohen, Richardson, & LaBree, 1994); whereas, Otten et al. (2007) found that more frequent parent-child communication had no impact on nicotine use onset .
Parental knowledge of their child’s behaviors and whereabouts (Marceau, Abar, & Jackson, 2015) may be another key factor in reducing the risk for adolescent substance use, and evidence for parental knowledge’s protectiveness against adolescent substance use is more robust (Racz & McMahon, 2011). Although the mechanism by which parental knowledge may be protective against substance use is poorly understood, it has been suggested that parents who are highly knowledgeable of their child’s activities and whereabouts are less likely to allow their child to associate with substance-using peers (Laird, Criss, Pettit, Dodge, & Bates, 2008). Parental knowledge has been measured by both parents’ and adolescents’ perceptions of parental knowledge. Previous research have suggested that adolescents’ report of parental knowledge are similar to parents’ report of parental knowledge (Kerr and Stattin 2000; Kerr et al., 2010; Soenens et al. 2006), and both parental report and adolescent report of parental knowledge are associated with lower levels of substance use (Barnes, Reifman, Farrell, & Dintcheff, 2000; Dishion & Kavanagh, 2003).
Youth normally seek autonomy from their parents during adolescence according to the meta-monitoring theory of autonomy (Kobak & Cole, 1994). Youth can claim more autonomy from their parents by spending less time with them (Larson, Richards, Moneta, Holmbeck, & Duckett, 1996). Corresponding to this decrease in spending time with parents is the decrease in the frequency of parent-child communication (Branje, Brett, & Collins, 2012). However, there is variability in how parent-child communication and parental knowledge change over time. For example, trajectories representing high, medium, decreasing, and inconsistent communication throughout adolescence have been identified in the literature (Tobler & Komro, 2010). Other researchers have identified trajectories representing low and decreasing levels of parental knowledge, as well as stable moderate or high levels of parental knowledge during adolescence (Laird, Criss, Pettit, Bates, & Dodge, 2009). Thus, the first goal of this study is to examine variability in trajectories of parent-child communication frequency and adolescent perceptions of parental knowledge of their activities across ages 12 to 17 in a sample of adolescent girls.
Sociodemographic and contextual factors may influence variability of parent-child communication and parental knowledge over time. For example, frequency of parent-child communication among boys tends to decrease and stay low throughout adolescence, whereas frequency of parent-child communication among girls tends to decrease initially, only to increase in later adolescence (Keijsers & Poulin, 2013). Additionally, White girls living in a low-risk neighborhood were more likely to report high levels of parental knowledge over time (Laird et al., 2009). In contrast, African American girls living in single-parent households were more likely to report low levels of parental knowledge over time (Latendresse, Ye, Chung, Hipwell, & Sartor, 2017).
In addition, levels of parent-child connectedness may influence how frequent adolescents communicate with their parents (Lezin, Rolleri, Bean, & Taylor, 2004). Sexual minority youth often report low levels of parent-child connectedness (Conover & Meredith, 2014). Thus, sexual orientation might be a personal risk factor associated with decreased parent-child communication and parental knowledge. Additionally, emerging research also suggests that SMGs are less likely to communicate with their parents and to report lower levels of parental knowledge (Montano et al., 2016; Montano, McCauley, Miller, Chisolm, & Marshal, 2017).
Low frequency of parent-child communication and low levels of parental knowledge may put SMGs at additional risk for substance use. Studies have established links, often using crosssectional data, between a girl’s sexual orientation and substance use (Dermody et al., 2016), a girl’s sexual orientation and low parental knowledge (Montano et al., 2016), and lower parental knowledge and adolescent substance use (Svensson, 2003). Little is known regarding how trajectories of SMGs communicating with their parents and their perceptions of parental knowledge of their activities during adolescence explain (i.e., mediate) the association between sexual orientation and substance use. Determining how SMGs communicating with their parents and parental knowledge of their activities serve as mechanisms underlying the relationship between sexual orientation and substance use could inform targets for intervention. Thus, the second goal of this study is to determine the associations between sexual orientation, trajectories of parent-child communication frequency and perceived parental knowledge over time, and substance use.
In this paper, we aim to identify distinct trajectories of parent-child communication of and adolescent’s perceptions of parental knowledge of their activities and to examine the associations of sexual orientation with trajectories of parent-child communication and parental knowledge and substance use at age 18. We hypothesize that sexual orientation will predict membership in trajectories representing low levels of parent-child communication and parental knowledge. We also hypothesize that stable low trajectories of parent-child communication and parental knowledge compared to stable high trajectories of parent-child communication and parental knowledge (as protective factors against substance use) will be associated with higher levels of substance use at age 18 (Dillon, Pantin, Robbins, & Szapocznik, 2008; Manuel Barrera, Biglan, Ary, & Li, 2001). Finally, we test the hypothesis that low levels of parent-child communication of activities and perceptions of parental knowledge of activities over time will mediate the association between sexual orientation and substance use at age 18.
Methods
Sample
The analyses used data from the Pittsburgh Girls Study (PGS, N=2450), a prospective study of girls who were first assessed at ages 5–8. In the first wave, 53% of girls were identified by their caretaker as African American, 41% as White, and 6% as other race or multi-racial (see Keenan et al., 2010 and Hipwell et al., 2002 for details of sampling and study design). The current analyses focused on the adolescent period, a time when substance use first develops, using data spanning 12–17 years of age (Table 1). Caregiver informed consent and youth assent were obtained from all participants prior to data collection. The study was approved by the University of Pittsburgh Human Subjects Protection Office.
Table 1.
Demographics of the sample at age 17
| Sociodemographic Factor | % (n) | % (n) |
|---|---|---|
| Race | White 41.2 (1010) |
African American 58.7 (1439) |
| Sexual Orientation | Heterosexual Girl 83.3 (2041) |
Sexual Minority Girl 16.6 (407) |
| SES | Higher SES 60.4 (1237) |
Lower SES 39.6 (811) |
| Household Status | Cohabitating Parents 50.5 (1032) |
Single-Parent 49.5 (1012) |
| Neighborhood Problems | Low Neighborhood Problems 46.9 (1148) |
High Neighborhood Problems 53.1 (1302) |
| Cigarette use in last year | No Use in the Last Year 79.1 (2049) |
Use in the last year 20.9 (429) |
| Marijuana use in the last year | No Use in the Last Year 75.3 (2051) |
Use in the last year 24.7 (507) |
| Alcohol use in the last year | No Use in the Last Year 60.1 (2051) |
Use in the last year 39.8 (818) |
Note: SES = socioeconomic status
Measures
Sexual orientation.
Sexual orientation was assessed with three questions that asked about attraction, dating behaviors, and identity. Attraction was measured with the item: “Which best describes your feelings? Are you: “only attracted to females,” “mostly attracted to females,” “equally attracted to females and males,” “mostly attracted to males,” and “only attracted to males.” For behaviors, we asked participants the sex of their current dating partner. For identity, each participant was asked if she considered herself to be: “heterosexual or straight,” “gay or lesbian,” or “bisexual”. For these analyses, participants were categorized as SMGs if they chose any of the following: any attraction to females, or currently dating a girl, or identifying as lesbian or bisexual as in prior work (Badgett & Goldberg, 2009; Saewyc et al., 2004). We used sexual orientation as a predictor variable at age 17 because preliminary analyses showed that only 14% of those who endorsed a same-sex sexual identity at age 17 endorsed same-sex attraction at age 14 and that 10% of those who endorsed same-sex attraction at age 17 endorsed same-sex attraction at age 14. Thus, if we were to use same sex attraction or orientation measured at age 14, many SMGs in the data set would have been inappropriately classified as heterosexual or having only opposite sex attraction.
Parent-child communication and parental knowledge.
We used self-report on the 13item Supervision and Involvement Scale (Loeber, Farrington, Stouthamer-Loeber, & Van Kammen, 1998), administered annually from age 12 to 17. Parent-child communication comprised five items regarding the last time the participants discussed with their parents what they had done or will do during the day or how they are doing at school (responses were:1 = yesterday/today, 2 = a couple of days ago, 3 = a couple of weeks ago, and 4 = more than a couple of weeks ago) and how often they spoke with their parents about what they are going to do for the day (responses were 1 = often, 2 = sometimes, 3 = almost never, and 4 = never). Cronbach’s α ranged from .77 at age 12, to .78 at age 17. Parental Knowledge consisted of two items asking adolescents how often they perceived that their parents knew about their activities. Responses were 1 = Almost Never, 2 = Sometimes, and 3 = Almost Always. Cronbach’s α ranged from .54 at age 12, to .71 at age 17. We used the mean scores for each component as the outcome variables in our analyses (Table 1).
Substance use.
Substance use was measured using the Nicotine, Alcohol, Drug, and Substance Use (NADU) scale (Pandina, Labouvie, & White, 1984). Five NADU questions asked participants how often they had used tobacco, marijuana, or engaged in binge-drinking (defined as having 4 or more drinks in one sitting in the past year; National Institute on Alcohol Abuse and Alcoholism) . We chose to analyze binge drinking instead of any alcohol use because binge drinking is a risky form of alcohol use (Courtney & Polich, 2009). Because the distributions of the responses were highly skewed, the variables were dichotomized to reflect ‘none’ vs. ‘any use’ in the past year, as in prior work (Chung, Kim, Hipwell & Stepp, 2013; Chung, Pedersen, Kim, Hipwell & Stepp, 2014; Marshal et al., 2013).
Covariates
Sociodemographic characteristics.
Caregivers provided data on the adolescents’ age and race, household structure (single or dual parent), and whether the household received public assistance (e.g. WIC, food stamps, welfare), which was used as an index of poverty status.
Neighborhood.
Caregivers completed the 17-item Your Neighborhood Scale (Loeber & Farrington, 1998), which assessed the severity of perceived neighborhood problems (e.g. unemployment, burglaries and thefts, and abandoned houses) scored on 3-point Likert scales of “not a problem” (1) to “big problem” (3). Responses were summed (sum scores ranged between 3 and 51). The score was then dichotomized using the mean sum score as a cut-off for high neighborhood problems. Internal consistency was high (Cronbach’s α = .94).
Statistical Analysis
Two often used longitudinal modeling procedures that identify subgroups of trajectories in a sample are latent growth mixture modeling (LGMM) and group-based trajectory modeling (GBTM). Both approaches have been used to identify normal and pathological development throughout adolescence and identify predictors of such trajectories (Nagin & Odgers, 2010). One fundamental difference between the two approaches is that LGMM assumes that individuals within a group trajectory will have variations in trajectories within that identified group; in contrast, GBTM assumes that individuals within a group trajectory will follow the same trajectory (Nagin & Odgers, 2010). Stated differently, LGMM models variability within and between groups whereas GBTM models differences between groups (Nagin & Odgers, 2010). Consequently, LGMM requires a priori hypotheses of the characteristics that differentiate subpopulations within a trajectory whereas GBTM does not require such hypotheses. The purpose of this study was not to identify subpopulations of SMGs who follow distinct trajectories of parent-child communication and parental knowledge, rather, this study seeks to describe the relationships between sexual orientation, trajectories of parent-child communication and parental knowledge over time, and subsequent substance use at age 18; therefore, GBTM is an acceptable approach for analyzing trajectory data for this study.
This study used a two-step procedure to generate semi-parametric group-based trajectory models using traj, a STATA procedure developed by Jones et al. (STATA v.14 plugin, Pittsburgh, PA). The overall approach of group-based trajectory modeling is to find the iteration of group trajectories with the most parsimonious solution. The procedure calculated the Bayesian information criterion (BIC) for each iteration, with higher BIC scores indicating the most parsimonious model.
To determine the optimal number of trajectories, we considered BIC, and prior relevant research (e.g., Laird et al., 2009), as recommended by Nagin (2005). This study used a two-step approach to identifying the trajectories, similar to a study on group trajectories of distal parental supervision by Laird et al. (2009). In the first step, we calculated the BIC for one to four groups with linear trajectories. The second step was to determine the appropriate trajectory shape (e.g., linear, quadratic) for each group. Previous studies on the trajectories of parent-child communication and parental knowledge show that this behavior tends to decrease on average in a quadratic fashion over time (Laird et al., 2009; Tobler & Komro, 2010). Thus, the study calculated BIC for quadratic, linear, and stable (i.e. intercept only) trajectories for each group. We first designated all trajectories as intercept-only. BIC was computed for each iteration of the model. At the next iteration, the first group was specified as a linear trajectory, while the other two were intercept-only. The iteration that had the highest BIC was then compared to the BIC of the next iteration (e.g., the first group was promoted to a quadratic trajectory, and the other two groups remained at intercept-only, as shown in Table 2). To provide further evidence for model adequacy, we used the following criteria as recommended by Nagin (2005): (a) all group trajectories have statistically significant β coefficients (i.e., p-values <.05); (b) estimated group membership is close to percentages of those assigned to the group trajectory; (c) average posterior probability >.70; and (d) the odds of correct classification > 5.0.
Table 2.
Parameters used to select group trajectories and determine model adequacy
| Model | Comparison | BIC |
|---|---|---|
| Parent-Child Communication |
||
| a. All intercept-only | N/A | −10151.47 |
| b. One linear, two intercept-only | a | −10151.04 |
| c. One quadratic, two intercept-only | b | −10143.94 |
| d. Quadratic, linear, and intercept-onlya | c | −10087.71 |
| e. Two quadratic, one intercept-only | d | −10089.50 |
| f. One quadratic, two linear | d | −10091.47 |
| g. Two quadratic, one linear | d | −10093.29 |
| Parental Knowledge |
||
| a. All intercept-only | N/A | −9679.07 |
| b. One linear, two intercept-only | a | −9765.00 |
| c. One quadratic, two intercept-only | a | −9611.03 |
| d. Quadratic, linear, and intercept-only | c | −9588.57 |
| e. Two quadratic, one intercept-only | d | −9618.77 |
| f. Two quadratic, one linear | d | −9596.26 |
| g. All quadratica | f | −9593.54 |
Note. Each letter represents an iteration of the 3-group trajectories of various shapes (intercept-only, linear, or quadratic). The iteration with the highest BIC (Bayesian Information Criterion) was the model used for mediation analysis.
Most adequate iteration
After establishing the group trajectories, we then added the following factors to the model simultaneously: (a) sexual orientation, (b) race, (c) single-parent household, (d) SES, and (e) high versus low neighborhood problems to test if these sociodemographic characteristics were risk factors for following less protective trajectories of parent-child communication and parental knowledge. To test if the group trajectories of parent-child communication and parental knowledge were significant mediators in the relationship between sexual orientation and substance use, we first ran a logistic regression model testing the association between sexual orientation and substance use at age 18. We then ran another logistic regression model testing the relationship between group trajectories of parent-child communication and parental knowledge and substance use at age 18. We then ran a logistic regression model testing the association between sexual orientation and substance use adjusted for group trajectories of parent-child communication and parental knowledge. We conducted a Sobel Test to test if group trajectories of parent-child communication and parental knowledge were statistically significant mediators between sexual orientation and substance use. For the mediation analysis, we treated the group trajectories as categorical variables instead of ordinal variables because we wanted to test the relationships between the group trajectories and subsequent substance use at age 18 as opposed to the relationships between increases or decreases in parent-child communication or parental knowledge and subsequent substance use at age 18. Finally, we re-ran the models adjusting for race, single-parent household, SES, and high neighborhood problems measured at age 17.
Missing Data.
Analysis of the panel data showed that they were strongly balanced. Seventy-nine percent (n = 1815) and 77% (n = 1770) of the participants completed all 6 parentchild communication and parental knowledge yearly assessments, respectively. Eighty-one percent (n = 1860) completed all 6 yearly assessments for cigarette, marijuana, and binge drinking. Older adolescents (OR = 1.60 95% CI [1.41, 1.82], p < .001) and SMGs (OR = 3.01, [1.71, 5.3], p < .001) were more likely to have missing data for the parent-child communication assessments; additionally, both groups were also more likely to have missing data for the parental knowledge assessments (OR = 1.42 [1.29, 1.57], p < .001) and OR = 3.17, [2.00, 5.03], p < .00, respectively). Participants receiving public assistance (OR: 4.01, [CI: 1.14, 14.1], p = .03) or who identified as African American (OR = 0.19, [0.05, 0.72], p = .02) were more likely to have missing data for the cigarette use measurement; older adolescents (OR = 0.61 [0.43, 0.86], p = .004), participants receiving public assistance (OR = 4.23, [1.41, 12.73], p = .01), and participants who identified as African American (OR = 0.30, [0.10, 0.87], p = .03) were more likely to have missing data for the marijuana use measurement. Finally, older participants (OR = 0.71, [0.52, 0.95], p = .02), participants receiving public assistance (OR = 3.00, [1.09, 8.24], p = .03), and participants who identify as African American (OR = 0.34, [0.12, 0.93], p = .04) were more likely to have missing data for the alcohol measurements. The above analyses were adjusted for age. Although there is no standard test to determine the mechanism for missing data, these analyses suggest that the missingness of our outcomes was associated with observed data, and therefore, were missing at random (Dong & Peng, 2013; Rubin, 1976). Based on that assumption, we used maximum likelihood estimates for the group-based trajectory models (Nagin & Odgers, 2010) and multiple imputation for the mediation analysis to minimize the risk for biased estimates (Karahalios, Baglietto, Carlin, English, & Simpson, 2012).
Results
Group Based Trajectories of Parent-child communication and Parental Knowledge
Parent-child communication.
For all girls, specifying the three trajectory groups as quadratic decreasing, linear increasing, and high-intercept only was the most adequate model with the highest BIC (Table 2 and Appendix A). A frequent stable trajectory characterized group 1 (72.4% of the sample), an infrequent increasing trajectory characterized group 2 (20.1% of the sample), and an infrequent decreasing trajectory characterized group 3 (7.5% of the sample). Figure 1A represents these three trajectory groups. Appendix A shows that the identified group trajectories fulfilled all indicators of model adequacy, with statistically significant β coefficients for all three groups, group membership estimates were close to percentages of those assigned to the group trajectory (differences by 0.1 to 0.4 percentage points); average posterior probability >.70 for all three groups; and the odds of correct classification > 5.0.
Figure 1.
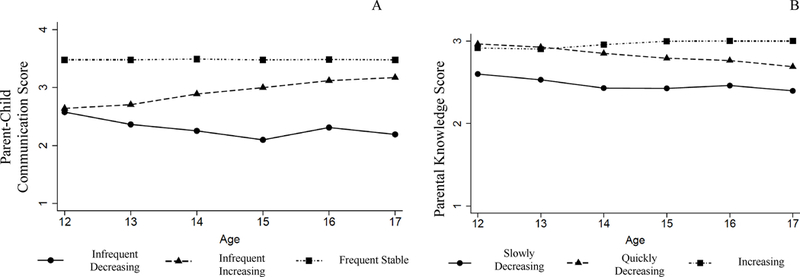
Group trajectories and percentage of participants in each group by parental monitoring components: (A) Parent-Child Communication, (B) Parental Knowledge
Parental Knowledge.
For all adolescents, specifying the trajectory shapes as low and increasing quadratic, decreasing quadratic, and high quadratic was the most adequate model with the highest BIC (Table 2 and Appendix A). An increasing trajectory characterized group 1 (30.1% of the sample), a quickly decreasing trajectory characterized group 2 (36.8% of the sample), and a slowly decreasing trajectory characterized group 3 (33.0%). Figure 1B visualizes these three group trajectories. Appendix A shows that the identified group trajectories fulfilled all indicators of model adequacy, with statistically significant β coefficients for all three groups, group membership percentages were close to percentages of those assigned to the group trajectory (differences by 0.1 to 0.4 percentage points); average posterior probability >.70 for all three groups; and the odds of correct classification > 5.0 for all three groups, except for the quickly decreasing group, which had an odds of correct classification of 4.53.
Sexual Orientation as a Predictor of Group Trajectory
Table 3 summarizes the results of the analysis testing the association between the five sociodemographic characteristics (sexual orientation, race, single-parent household, SES, and high versus low neighborhood problems) and trajectory group membership. We used the frequent stable group and the increasing group for parent-child communication and parental knowledge, respectively, as the reference groups because we were interested in how low levels of parent-child communication and parental knowledge over time can be risk factors for substance use. SMGs were more likely to follow the infrequent decreasing trajectory than the frequent stable trajectory of parent-child communication over time. African American youth and youth with lower SES at age 12 were more likely to follow both the infrequent increasing and infrequent decreasing trajectories rather than frequent stable trajectory of parent-child communication over time. Living in a single-parent household or in a high-problem neighborhood at age 12 was not predictive of any parent-child communication group trajectory. To explore the possibility that race might moderate the association between sexual orientation and group trajectories, given the high proportions of African American and White girls in PGS, we ran an analysis that included the interaction term race x sexual orientation for the parentchild communication trajectories, but no interaction between race and sexual orientation was found for the infrequent increasing group (β = − 0.17, S.E. = 0.57, t = − 0.29, p = 0.77) or the infrequent decreasing group (β = − 0.06, S.E. = 0.62, t = − 0.10, p = 0.92).
Table 3.
Sociodemographic Characteristics Predictive of Group Membership
| Predictor Sociodemographic Characteristics | |||||
|---|---|---|---|---|---|
| Sexual Orientationa β (S.E.) |
African Americanb β (S.E.) |
Low SES (age 12)c β (S.E.) |
Single Parent Household (age 12)d β (S.E.) |
High Neighborhood Problems (age 12)e β (S.E.) |
|
| Parent-Child Communication | |||||
| Frequent Stable | Ref | Ref | Ref | Ref | Ref |
| Infrequent increasing | 0.33(0.17) | 0.83***(0.16) | 0.50*** (0.14) | −0.28 (0.15) | 0.29 (0.14) |
| Infrequent decreasing | 0.51*(0.23) | 0.94***(0.26) | 0.57** (0.21) | −0.06 (0.21) | 0.13 (0.20) |
| Parental knowledge | |||||
| Increasing | Ref | Ref | Ref | Ref | Ref |
| Quickly Decreasing | 0.48 (0.25) | −0.20 (0.16) | 0.45* (0.18) | 0.53** (0.17) | 0.07 (0.15) |
| Slowly Decreasing | 1.04***(0.24) | 0.50** (0.19) | 0.68*** (0.18) | 0.55** (0.18) | 0.50 (0.12) |
Note. S.E. = Standard error, SES = socioeconomic status, Ref = reference group
Heterosexual girls were used as reference
White girls were used as reference
Cohabitating parents were used as reference
Higher SES was used as reference
Low Neighborhood Problems was used a reference
p < .05
p < .01
p < .001
Both SMGs and African American girls were more likely to follow the slowly decreasing trajectory of parental knowledge over time. Youth with lower SES and youth living in a singleparent household at age 12 were more likely to report both the slowly decreasing and quickly decreasing trajectories rather than the increasing trajectory of parental knowledge over time. Living in a high-problem neighborhood at age 12 was not predictive of any parental knowledge group trajectory. To examine race as a moderator of the association between sexual orientation and group trajectories, we ran an interaction analysis using the term race x sexual orientation for the parental knowledge trajectories, but no interaction between race and sexual orientation was found for the slowly decreasing group (β = − 0.27, S.E. = 0.52, t = − 0.53, p = 0.60) or the quickly decreasing group (β = − 0.37, S.E. = 0.53, t = − 0.70, p = 0.48).
We then conducted the analysis using sexual identity (bisexual and lesbian versus heterosexual) and sexual attraction (mostly attracted to the opposite sex, equally attracted to both sexes, and mostly/completely attracted to the same sex versus completely attracted to the opposite sex) as predictor variables. Only bisexual girls (n = 150) and girls who were mostly/completely attracted to the same sex (n = 54) were more likely to follow to the slowly decreasing parent-child communication group relative to the frequent stable group (Appendix B) whereas girls who were mostly attracted to the opposite sex (n = 169) and girls who were mostly/completely attracted to the same sex were more likely to belong to the slowly decreasing group of parental knowledge relative to the increasing group (Appendix B). However, when we used sexual identity and sexual attraction as predictor variables, the sample size for each group were small (e.g, lesbians n = 39) compared to the sexual orientation variable that combined identity, attraction, and behavior.
Associations between Sexual Orientation, Trajectory Groups and Substance Use
Parent-child communication.
Table 4 summarizes the associations between sexual orientation, parent-child communication group trajectories, and substance use at age 18. We used frequent stable group as the reference group because we were interested in how low levels of parent-child communication over time mediate the relationship between sexual orientation and substance use. Model 1 showed that sexual orientation was a statistically significant predictor for all three substance use outcomes at age 18. Model 2 showed that the addition of the parent-child communication trajectories to model 1 reduced the β coefficient for sexual orientation on all substance use outcomes, except for binge drinking. The Sobel Test indicated that the mediated effect of the parent-child communication trajectories was statistically significant for cigarette use and marijuana use, but not for binge drinking. Model 3 showed the association between sexual orientation and substance use adjusted for race, single-parent household, SES, and neighborhood problems. Model 4 showed that even when adjusted for race, single-parent household, SES, and neighborhood problems, the Sobel Test indicated that the mediated effect of the parent-child communication trajectories was statistically significant for cigarette use and marijuana use, but not for binge drinking.
Table 4.
Associations between sexual orientation, parent-child communication group trajectories, and substance use at age 18
| Simple Models | Adjusted Models | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Model 1 | Model 2 | Model 3 | Model 4 | ||||
| Cigarette Use at Age 18 | β (SE) | β (SE) | β (SE) | β (SE) | ||||
| Sexual Orientationa | 0.76*** | (0.12) | 0.74*** | (0.12) | 0.79*** | (0.13) | 0.77*** | (0.13) |
| Communication Trajectories | ||||||||
| Frequent Stable | Ref | Ref | ||||||
| Infrequent increasing | 0.25* | (0.12) | 0.32* | (0.13) | ||||
| Infrequent decreasing | 0.32 | (0.18) | 0.47* | (0.19) | ||||
| African Americanb | −0.71*** | (0.12) | −0.78*** | (0.12) | ||||
| Single Parentc | 0.11 | (0.11) | 0.11 | (0.11) | ||||
| SESd | 0.50*** | (0.12) | 0.44*** | (0.12) | ||||
| High Neighborhood Problemse | 0.02 | (0.10) | −0.02 | (0.10) | ||||
| Sobel Test Z-Score | 2.13* | (0.04) | 2.15* | (0.13) | ||||
| Marijuana Use | β (SE) | β (SE) | β (SE) | β (SE) | ||||
| Sexual Orientationa | 0.73*** | (0.12) | 0.72*** | (0.12) | 0.72*** | (0.12) | 0.71*** | (0.13) |
| Communication Trajectories | ||||||||
| Frequent Stable | Ref | Ref | ||||||
| Infrequent increasing | 0.28* | (0.12) | 0.26* | (0.12) | ||||
| Infrequent decreasing | 0.22 | (0.19) | 0.20 | (0.19) | ||||
| African Americanb | 0.01 | (0.11) | −0.03 | (0.11) | ||||
| Single Parentc | 0.10 | (0.10) | 0.10 | (0.10) | ||||
| SESd | 0.17 | (0.11) | 0.16 | (0.11) | ||||
| High Neighborhood Problemse | 0.05 | (0.10) | −0.06 | (0.10) | ||||
| Sobel Test Z-Score | 1.99 | (0.04)* | 2.02* | (0.03) | ||||
| Binge Drinking | β (SE) | β (SE) | β (SE) | β (SE) | ||||
| Sexual Orientationa | 0.41* | (0.19) | 0.41* | (0.19) | 0.45* | (0.19) | 0.44* | (0.19) |
| Communication Trajectories | ||||||||
| Frequent Stable | Ref | Ref | ||||||
| Infrequent increasing | −0.16 | (0.14) | −0.05 | (0.15) | ||||
| Infrequent decreasing | 0.21 | (0.28) | 0.37 | (0.29) | ||||
| African Americanb | −0.68*** | (0.13) | −0.69*** | (0.13) | ||||
| Single Parentc | 0.34* | (0.14) | 0.34* | (0.14) | ||||
| SESd | −0.12 | (0.15) | −0.12 | (0.15) | ||||
| High Neighborhood Problemse | −0.21 | (0.14) | −0.21 | (0.14) | ||||
| Sobel Test Z-Score | 0.21 | (0.04) | 0.98 | (0.04) | ||||
Note. Model 1 tests the association between substance use at age 18 and sexual orientation; Model 2 tests the association between sexual orientation and substance use at age 18 mediated by trajectories of parent-child communication; Model 3 tests the association between substance use at age 18 and sexual orientation adjusted for race, SES, single parent household, and neighborhood problems. Model 4 tests the association between sexual orientation and substance use at age 18 mediated by trajectories of parent-child communication and adjusted for race, SES, single parent household, and neighborhood problems; SE = standard error; SES = socioeconomic status
Heterosexual girls were used as reference
White girls were used as reference
Cohabitating parents were used as reference
Higher SES was used as reference
Low Neighborhood Problems was used a reference
p < 0.05
p < 0.01
p < 0.001
Parental Knowledge.
Table 5 summarizes the associations between sexual orientation, parental knowledge group trajectories, and substance use age 18. We also used the high group as the reference group because we were interested in how less protective parental knowledge trajectories mediate the relationship between sexual orientation and substance use. Model 1 showed that sexual orientation was a statistically significant predictor for all three substance use outcomes at age 18. The addition of the parental knowledge trajectories to the model (Model 2) reduced the β coefficient for sexual orientation on all substance use outcomes. The Sobel Test indicated that the mediated effect of the parent-child communication trajectories was statistically significant for cigarette use and marijuana use, but for binge drinking, it was marginally significant (p = 0.057). However, when adjusted for race, single-parent household, SES, and neighborhood problems, the parental knowledge trajectories were statistically significant mediators between sexual orientation and all three substance use outcomes at age 18 (Table 5, Models 3 and 4).
Table 5.
Associations between sexual orientation, parental knowledge group trajectories, and substance use at age 18
| Simple Models | Adjusted Models | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Model 1 | Model 2 | Model 3 | Model 4 | ||||
| Cigarette Use | β (SE) | β (SE) | β (SE) | β (SE) | ||||
| Sexual Orientationa | 0.75*** | (0.13) | 0.68*** | (0.13) | 0.79*** | (0.13) | 0.73*** | (0.13) |
| Knowledge Trajectories | ||||||||
| Increasing | Ref | Ref | ||||||
| Quickly Decreasing | 0.41** | (0.13) | 0.39** | (0.13) | ||||
| Slowly Decreasing | 0.72*** | (0.12) | 0.78*** | (0.13) | ||||
| African Americanb | −0.72*** | (0.11) | −0.78*** | (0.12) | ||||
| Single Parentc | 0.09 | (0.11) | 0.05 | (0.12) | ||||
| SESd | 0.45*** | (0.12) | 0.42** | (0.12) | ||||
| High Neighborhood Problemse | 0.03 | (0.10) | −0.01 | (0.10) | ||||
| Sobel Test Z-Score | 3.88*** | (0.05) | 3.82*** | (0.05) | ||||
| Marijuana Use | β (SE) | β (SE) | β (SE) | β (SE) | ||||
| Sexual Orientation | 0.73*** | (0.12) | 0.65*** | (0.12) | 0.72*** | (0.12) | 0.65*** | (0.12) |
| Knowledge Trajectories | ||||||||
| Increasing | Ref | Ref | ||||||
| Quickly Decreasing | 0.74*** | (0.12) | 0.73*** | (0.12) | ||||
| Slowly Decreasing | 0.85*** | (0.13) | 0.83*** | (0.12) | ||||
| African Americanb | −0.01 | (0.11) | −0.01 | (0.11) | ||||
| Single Parentc | 0.08 | (0.10) | 0.04 | (0.11) | ||||
| SESd | 0.17 | (0.11) | 0.13 | (0.11) | ||||
| High Neighborhood Problemse | 0.08 | (0.10) | −0.01 | (0.10) | ||||
| Sobel Test Z-Score | 4.07*** | (0.06) | 3.89*** | (0.05) | ||||
| Binge Drinking | β (SE) | β (SE) | β (SE) | β (SE) | ||||
| Sexual Orientation | 0.39* | (0.18) | 0.36 | (0.18) | 0.43* | (0.19) | 0.40* | (0.19) |
| Knowledge Trajectories | ||||||||
| Increasing | Ref | Ref | ||||||
| Quickly Decreasing | 0.34* | (0.14) | 0.36* | (0.15) | ||||
| Slowly Decreasing | 0.26 | (0.15) | 0.37* | (0.15) | ||||
| African Americanb | −0.69*** | (0.13 | −0.69*** | (0.13) | ||||
| Single Parentc | 0.33* | (0.14) | 0.31* | (0.14) | ||||
| SESd | −0.12 | (0.15) | −0.14 | (0.15) | ||||
| High Neighborhood Problemse | −0.18 | (0.14) | −0.22 | (0.14) | ||||
| Sobel Test Z-Score | 1.90 | (0.04) | 2.32* | (0.04) | ||||
Note. Model 1 tests the association between substance use at age 18 and sexual orientation; Model 2 tests the association between sexual orientation and substance use at age 18 mediated by trajectories of parental knowledge; Model 3 tests the association between substance use at age 18 and sexual orientation adjusted for race, SES, single parent household, and neighborhood problems. Model 4 tests the association between sexual orientation and substance use at age 18 mediated by trajectories of parental knowledge and adjusted for race, SES, single parent household, and neighborhood problems; SE = standard error; SES = socioeconomic status
Heterosexual girls were used as reference
White girls were used as reference
Cohabitating parents were used as reference
Higher SES was used as reference
Low Neighborhood Problems was used a reference
p < 0.05
p < 0.01
p < 0.001
Discussion
This study characterized the relationships between sexual orientation, parental-child communication and parental knowledge trajectories, and substance use in an urban, populationbased sample of adolescent girls. We identified three group trajectories for parent-child communication and for parental knowledge. SMGs were generally more likely to follow low levels of parent-child communication and parental knowledge over time. Infrequent parent-child communication and lower levels of parental knowledge over time raised the risk for substance use at age 18. These findings have implications for preventing substance use and improving parent-child relationships among SMGs.
Sexual orientation as a predictor variable
Consistent with prior longitudinal studies of sexual minority youth (Corliss et al., 2013; Marshal et al., 2013), we used sexual orientation at age 17 as a predictor variable in our analyses. This approach, however, had the limitation that changes in sexual orientation over time in relation to frequency of parent-child communication, parental knowledge of activities, and substance use could not be examined. The low proportion (14%) of girls endorsing same-sex attraction at age 14 in the sample, and prior research indicating that most sexual minority youth do not disclose their sexual orientation until late adolescence or early adulthood (Friedman, et al., 2008) provided the rationale for using age 17 identity and attraction measures as a predictor variable for the analyses reported here.
When we used sexual identity (lesbian and bisexual compared to heterosexual) and sexual attraction as predictor variables, the patterns of associations were less consistent. For example, bisexual girls (n = 150) were more likely to follow the infrequent decreasing trajectory of parent-child communication relative to the frequent stable trajectory (Appendix B). Although bisexual girls may be at higher risk for many adverse health outcomes compared to lesbians (Arbeit, Fisher, Macapagal, & Mustanski, 2016), we caution against drawing the conclusion that these differences were associated with the girl’s sexual identity because of the small sample size for each sexual orientation subgroup. Thus, the absence of statistically significant findings for sexual identity and sexual attraction may be related to low statistical power.
Group Trajectories of Parent-child communication and Parental Knowledge
Although we identified three trajectories for both parent-child communication and for parental knowledge, an unexpected finding was that most girls reported frequent stable parentchild communication over time (72.4%). This challenges the notion that parent-child communication frequency decreases over time due to adolescents seeking autonomy from their parents (Branje et al., 2012); however, this is also gender-dependent, because previous research has suggested that girls tend to communicate more frequently with their parents than do boys (Cumsille, Darling, & Martínez, 2010).
In contrast, the proportion of girls reporting the three types of parental knowledge trajectories were more equally distributed. The most common group trajectory was girls reporting quickly decreasing levels of parental knowledge over time (36%), which previous research has supported as being normative (Masche, 2010). This may appear counterintuitive, given that a majority of girls reported a frequent stable trajectory of parent-child communication; however, the parent-child communication questions asked how often girls were disclosing to their parents, but not how much. Previous research has suggested that parent-child communication and adolescent secrecy should be two separate constructs (Frijns & Finkenauer, 2009). In other words, we suspect that girls may be frequently disclosing selective information to their parents. Additional studies which contain questions on both parent-child communication and secrecy may lend credence to the above hypothesis.
Predictors of Group Membership
Parent-child communication.
Findings supported our hypothesis that SMGs would be more likely to follow the infrequent decreasing (vs. frequent stable) trajectory of parent-child communication. This is consistent with other studies showing sexual minority youth were less likely to communicate with parents (Montano et al., 2016, 2017). Although this study cannot explain why SMGs were less likely to communicate frequently with their parents over time, we provide hypotheses that warrant further testing. Expectation of rejection from family is a major source of stress for sexual minorities according to the Minority Stress Theory (Meyer, 2003). Because of the stigma surrounding same-sex attraction, we hypothesize that SMGs may discuss their daily activities with their parents less frequently because they may be afraid of inadvertently disclosing any information that would implicate their same-sex sexual orientation. A second possibility is that some SMGs may have poor parent-adolescent relationships stemming from parental rejection of the girl’s sexual orientation. Previous research has found that adolescents are more likely to communicate with their parents if they perceive their parents as accepting (Hare, Marston, & Allen, 2011). Thus, we hypothesize that low levels of parentchild communication over time may be associated with the quality of parent-adolescent relationships among SMGs.
Parental Knowledge.
Our findings also supported the hypothesis that SMGs would be more likely to follow the slowly decreasing trajectory of parental knowledge over time, which is consistent with previous studies on perceived parental knowledge among SMGs (Montano et al., 2016, 2017). Nevertheless, it remains unknown why SMGs perceived low levels of parental knowledge throughout adolescence. Two factors warrant further investigation. First, there is evidence suggesting that parents withdraw from their adolescents after discovering their child’s sexual orientation (Saltzburg, 2007), which may impact how SMGs perceive parental knowledge. Alternatively, as with frequency of parent-child communication over time, SMGs may avoid disclosing any activity that would implicate their sexual orientation due to the expectation of rejection; thus, they may also perceive low levels of parental knowledge. Furthermore, the PGS lacked data on parental responses to a child revealing to them their sexual orientation and whether or not the SMGs were out to their parents; thus, we were unable to further investigate these relationships.
Parent-child communication and Parental Knowledge Trajectories as Mediators
Parent-child communication.
The positive correlation between sexual orientation and substance use at age 18 is consistent with previous research showing that sexual minority youth are more likely to use substances than are heterosexual youth (Marshal et al., 2013). Additionally, the positive correlation between low levels of parent-child communication and cigarette use is also consistent with previous studies (Metzger et al., 2013). These results suggest that SMGs are at risk for cigarette use not only because of their sexual orientation, but also because they tend to communicate less frequently with their parents. The process by which SMGs are at risk for cigarette use from low levels of parent-child communication remains unknown. The meta-monitoring theory of autonomy suggests changes in parent-child relationships may be determined by child-level characteristics, such as gender. In general, girls tend to remain closer to their parents during adolescence (Ryan & Lynch, 1989) and are also more likely to keep frequency of communication high (Cumsille et al., 2010). This frequent communication may give parents an opportunity to teach their child self-regulation skills as an alternative to substance use as a coping mechanism. However, we suspect that SMGs may be communicating less frequently with their parents possibly due to the expectation of rejection (Meyer, 2003). Future research should explore if this trajectory of parent-child communication may place SMGs at risk for substance use because they may not learn the self-regulation skills needed to manage stress, especially minority stress.
There were two unexpected findings. The first is that only the infrequent increasing trajectory of parent-child communication predicted higher levels of marijuana use but not the infrequent decreasing trajectory, which was inconsistent with our hypotheses. We must note that a small proportion of girls followed the infrequent decreasing parent-child communication trajectory (7.5%); thus, the lack of a statistically significant result may be due to low power. The second unexpected finding was that low levels of parent-child communication over time were not associated with a higher risk for binge drinking at age 18. There is some evidence to suggest that parent-child communication may not be protective against alcohol use because alcohol is more available at home, such that adolescents may more easily circumvent their parents’ restriction on alcohol (Friese, Grube, & Moore, 2013).
Parental Knowledge.
Both the quickly decreasing and low levels trajectories of parental knowledge were associated with a higher likelihood of cigarette use, marijuana use, and binge drinking at age 18. The protective relationship between parental knowledge and substance use is consistent with the literature (Fletcher, Steinberg, & Williams-Wheeler, 2004; Racz & McMahon, 2011). The mechanism for this relationship is still poorly understood. A study by Laird et al. (2008) suggests that higher parental knowledge interrupts the process by which peers introduce the adolescent to maladaptive behaviors. The quickly decreasing trajectory of parental knowledge was also associated with substance use at age 18. This trajectory is typical in parentadolescent relationships as children gain autonomy during adolescence (Laird, Marrero, & Sherwood, 2010), but a decrease in parental knowledge was also associated with increases in substance use (Laird et al., 2003). These trajectories of parental knowledge also place SMGs at risk for those three substances at age 18. It is interesting to note that in our simple model, the group trajectories of parental knowledge were not a statistically significant mediator between sexual orientation and binge drinking at age 18. However, when adjusted for race and singleparent household, these trajectory groups became statistically significant mediators (Table 5, model 4). These findings suggest that White SMGs living in single-parent households are at risk for both low levels of parental knowledge over time and binge drinking at age 18.
The mechanism by which low levels of parental knowledge over time raise the risk for substance use among SMGs remains unknown, but we suggest, based on our findings, examination of the following factors. First, research should examine whether SMGs experience low levels of parental knowledge because a) they may be selective of what they tell their parents for fear that they may inadvertently disclose their sexual orientation to them or b) their parents may react negatively to their sexual orientation disclosure, leading SMGs to perceive that their parents have low levels of knowledge of their activities. Second, it has been suggested that parental knowledge may prevent the adolescent from associating with delinquent peers (Laird et al., 2008). This is germane to SMGs because sexual minority youth—because of anti-gay stigma and discrimination—tend to belong to sexual minority social networks, which are more tolerant of alcohol use (Dermody et al., 2016). Thus, future research should examine if SMGs may be at risk for substance use because their parents are unaware that they are associating with substanceusing peers, especially for White SMGs living in single-parent households.
Implications
Our results show that SMGs are less likely to communicate with their parents over time and are also less likely to perceive that their parents are aware of their behaviors, which in turn, is associated with increased risk for cigarette and marijuana use at age 18. These results suggest that sexual minority orientation may influence the frequency of parent-child communication about the adolescent’s activities, which may influence risk for substance use. Future research should focus on why or what processes lead SMGs to experience lower levels of parent-child communication and parental knowledge over time. Potential factors to be explored include levels of parental support or rejection of the child’s sexual orientation. Describing such a process can inform substance use prevention efforts—namely, identifying critical targets for intervention that help to increase parent-child communication, and parental knowledge (and therefore decrease the risk for substance use) among SMGs.
Limitations
The parent-child communication and parental knowledge items asked participants how often they communicated with their parents, or how much they perceive that their parents know about their whereabouts and activities. They did not ask questions on specific whereabouts and activities that they disclosed or perceived that their parents knew. Adolescents can be selective in what they disclose to their parents (Tilton-Weaver et al., 2010). For example, they may communicate frequently with their parents about their activities at school or during the weekday but may not disclose activities associated with substance use (e.g. attending a weekend house party).
Second, this study examined the adolescent’s perspective of parent-child communication and parental knowledge, which may differ from the parental perspective. Future studies should examine possible divergent perspectives of parent-child communication and parental knowledge between parents and SMGs. However, there is some evidence to suggest that adolescent perspectives on parental knowledge are closely aligned with the parental perspective of parental knowledge (Stattin & Kerr, 2000). These limitations make it difficult to conclude whether the quantity of the information (i.e. the frequency of disclosure) or the quality of the information (disclosure of whereabouts or behaviors associated with substance use) disclosed or known is protective against substance use.
Furthermore, the Cronbach’s α was less than .70 for parental knowledge at younger ages. The small number of questions for the parental knowledge items may explain this low internal consistency (Tavakol & Dennick, 2011). Low internal consistency in these measures likely hindered our ability to identify confidently the group trajectories. Future work could include scales with more items to strengthen internal consistency and, hence, the precision of these models.
Additionally, we used the Sobel Test in our mediation models. One of the disadvantages of this test is its low power, especially in smaller sample sizes (MacKinnon, Fairchild, & Fritz, 2007). However, the large sample size of the PGS may mitigate the Sobel Test’s low statistical power.
Finally, one must be cautious in labeling these group trajectories as discrete constructs, because although individuals were assigned to a group, this does not necessarily make the group a distinct entity. In our analysis, a SMG who belonged to a less protective trajectory (e.g., slowly decreasing parent-child communication) might also belong to a more protective trajectory (e.g., frequent stable parental knowledge). Additionally, the groups identified in this study were not immutable, and might change based on other factors (e.g. addition of covariates, or completeness of the data). For example, parental attitudes regarding same-sex attraction may be a factor that may influence adolescent trajectories and should be explored in future studies.
Conclusions
The strengths of this study include analyses of a large community-based sample of sexual minority and heterosexual girls that prospectively tracked changes in parent-child communication and parental knowledge over time. Most studies on this topic have looked at sexual minorities only using venue-based sampling (Bouris et al., 2010). This study also used a more comprehensive measurement of sexual orientation, making the results of this study more generalizable to sexual minority youth.
There is significant variation in how much parent-child communication and parental knowledge of an adolescent’s activities changes over time for adolescent girls. Additionally, SMGs are more likely to report low levels of parent-child communication of their activities and perceptions of parental knowledge of their activities over time. Finally, SMGs are at risk for substance use partially due to low levels of parent-child communication and parental knowledge of their activities throughout adolescence. These findings have implications for the development of clinic and community-based interventions that target groups of parents of SMGs who may benefit from interventions that strengthen these components of parent-child communication and parental knowledge.
Supplementary Material
Acknowledgments
This study was funded by the National Institute of Mental Health (MH056630) and the National Institute of Drug Abuse (DA012237). Special thanks go to the families of the Pittsburgh Girls Study for their participation in this research, and to our dedicated research team for their continued efforts. We would also like to thank Debra Bogen, Jill Radtke, Winfred Frazier, and Carla Chugani for their help in the preparation of this manuscript.
Footnotes
This study is a secondary data analysis of the Pittsburgh Girls Study.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributor Information
Gerald T. Montano, Department of Pediatrics, University of Pittsburgh School of Medicine, Michigan State University
Michael P. Marshal, Department of Psychiatry, University of Pittsburgh School of Medicine, Michigan State University
Heather L. McCauley, Department of Human Development and Family Studies, University of Pittsburgh School of Medicine, Michigan State University
Elizabeth Miller, Department of Pediatrics, University of Pittsburgh School of Medicine, Michigan State University.
Tammy Chung, Department of Psychiatry, University of Pittsburgh School of Medicine, Michigan State University.
Alison E. Hipwell, Department of Psychiatry, University of Pittsburgh School of Medicine, Michigan State University
References
- Arbeit MR, Fisher CB, Macapagal K, & Mustanski B (2016). Bisexual Invisibility and the Sexual Health Needs of Adolescent Girls. LGBT Health, 3(5), 342–349. doi:10.1089/lgbt.2016.0035 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barnes GM, Reifman AS, Farrell MP, & Dintcheff BA (2000). The Effects of Parenting on the Development of Adolescent Alcohol Misuse: A Six‐Wave Latent Growth Model. Journal of Marriage and Family, 62(1), 175–186. doi:doi:10.1111/j.1741-3737.2000.00175.x [Google Scholar]
- Beatty SE, Cross DS, & Shaw TM (2008). The impact of a parent-directed intervention on parent-child communication about tobacco and alcohol. Drug Alcohol Review, 27(6), 591–601. doi:10.1080/09595230801935698 [DOI] [PubMed] [Google Scholar]
- Bouris A, Guilamo-Ramos V, Pickard A, Shiu C, Loosier PS, Dittus P, . . . Michael Waldmiller J (2010). A systematic review of parental influences on the health and wellbeing of lesbian, gay, and bisexual youth: time for a new public health research and practice agenda. Journal of Primary Prevention, 31(5–6), 273–309. doi:10.1007/s10935-010-0229-1 [DOI] [PubMed] [Google Scholar]
- Branje SJ, Brett L, & Collins WA (2012). Parent-Child Communication During Adolescence. In Vangelisti AL (Ed.), The Routledge Handbook of Family Communication New York, NY: Taylor & Francis. [Google Scholar]
- Chung T, Kim KH, Hipwell AE, & Stepp SD (2013). White and black adolescent females differ in profiles and longitudinal patterns of alcohol, cigarette, and marijuana use. Psychology of Addictive Behaviors, 27(4), 1110–1121. doi:10.1037/a0031173 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen DA, Richardson J, & LaBree L (1994). Parenting behaviors and the onset of smoking and alcohol use: a longitudinal study. Pediatrics, 94(3), 368–375. [PubMed] [Google Scholar]
- Conover W, & Meredith. (2014). The queer delinquent: Impacts of risk and protective factors on sexual minority juvenile offending in the U.S. [References]. Handbook of LGBT communities, crime, and justice, 449–472. [Google Scholar]
- Corliss HL, Wadler BM, Jun H-J, Rosario M, Wypij D, Frazier AL, & Austin SB (2013). Sexual-Orientation Disparities in Cigarette Smoking in a Longitudinal Cohort Study of Adolescents. Nicotine & Tobacco Research, 15(1), 213–222. doi:10.1093/ntr/nts114 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Courtney KE, & Polich J (2009). Binge drinking in young adults: Data, definitions, and determinants. Psychological Bulletin, 135(1), 142–156. doi:10.1037/a0014414 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cumsille P, Darling N, & Martínez ML (2010). Shading the truth: The patterning of adolescents’ decisions to avoid issues, disclose, or lie to parents. Journal of Adolescence, 33(2), 285–296. doi:10.1016/j.adolescence.2009.10.008 [DOI] [PubMed] [Google Scholar]
- Dermody SS, Marshal MP, Burton CM, & Chisolm DJ (2016). Risk of heavy drinking among sexual minority adolescents: indirect pathways through sexual orientation-related victimization and affiliation with substance-using peers. Addiction, 111(9), 1599–1606. doi:10.1111/add.13409 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dermody SS, Marshal MP, Cheong J, Chung T, S DS, & Hipwell A (2016). Adolescent Sexual Minority Girls Are at Elevated Risk for Use of Multiple Substances. Substance Use and Misuse, 51(5), 574–585. doi:10.3109/10826084.2015.1126743 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dillon FR, Pantin H, Robbins MS, & Szapocznik J (2008). Exploring the Role of Parental Monitoring of Peers on the Relationship Between Family Functioning and Delinquency in the Lives of African American and Hispanic Adolescents. Crime & Delinquency, 54(1), 65–94. doi:10.1177/0011128707305744 [Google Scholar]
- Dishion TJ, & Kavanagh K (2003). Intervening in Adolescent Problem Behavior : a Familycentered Approach New York: Guilford Press. [Google Scholar]
- Dong Y, & Peng C-YJ (2013). Principled missing data methods for researchers. SpringerPlus, 2, 222. doi:10.1186/2193-1801-2-222 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fletcher AC, Steinberg L, & Williams-Wheeler M (2004). Parental influences on adolescent problem behavior: revisiting Stattin and Kerr. Child Development, 75(3), 781–796. doi:10.1111/j.1467-8624.2004.00706.x [DOI] [PubMed] [Google Scholar]
- Friese B, Grube JW, & Moore RS (2013). Youth Acquisition of Alcohol and Drinking Contexts: An In-Depth Look. Journal of Drug Education, 43(4), 385–403. doi:10.2190/DE.43.4.f [DOI] [PMC free article] [PubMed] [Google Scholar]
- Frijns T, & Finkenauer C (2009). Longitudinal associations between keeping a secret and psychosocial adjustment in adolescence. International Journal of Behavioral Development, 33(2), 145–154. doi:10.1177/0165025408098020 [Google Scholar]
- Hare AL, Marston EG, & Allen JP (2011). Maternal Acceptance and Adolescents’ Emotional Communication: A Longitudinal Study. Journal of Youth and Adolescence, 40(6), 744–751. doi:10.1007/s10964-010-9586-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hawkins JD, Catalano RF, & Miller JY (1992). Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: implications for substance abuse prevention. Psychological Bulletin, 112(1), 64–105. [DOI] [PubMed] [Google Scholar]
- Hipwell AE, Loeber R, Stouthamer-Loeber M, Keenan K, White HR, & Kroneman L (2002). Characteristics of girls with early onset disruptive and antisocial behaviour. Criminal Behaviour and Mental Health, 12(1), 99–118. doi:10.1002/cbm.489 [DOI] [PubMed] [Google Scholar]
- Hipwell AE, Stepp SD, Keenan K, Allen A, Hoffmann A, Rottingen L, & McAloon R (2013). Examining links between sexual risk behaviors and dating violence involvement as a function of sexual orientation. Journal of Pediatric & Adolescent Gynecology, 26(4), 212–218. doi:10.1016/j.jpag.2013.03.002 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karahalios A, Baglietto L, Carlin JB, English DR, & Simpson JA (2012). A review of the reporting and handling of missing data in cohort studies with repeated assessment of exposure measures. BioMed Central Medical Research Methodology, 12(1), 96. doi:10.1186/1471-2288-12-96 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keenan K, Hipwell A, Chung T, Stepp S, Stouthamer-Loeber M, Loeber R, & McTigue K (2010). The Pittsburgh Girls Study: overview and initial findings. Journal of Clinical Child and Adolescent Psychology, 39(4), 506–521. doi:10.1080/15374416.2010.486320 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keijsers L, & Poulin F (2013). Developmental changes in parent-child communication throughout adolescence. Develomental Psychology, 49(12), 2301–2308. doi:10.1037/a0032217 [DOI] [PubMed] [Google Scholar]
- Kingon YS, & O’Sullivan AL (2001). The Family as a Protective Asset in Adolescent Development. Journal of Holistic Nursing, 19(2), 102–121. doi:10.1177/089801010101900202 [DOI] [PubMed] [Google Scholar]
- Kobak R, & Cole H (1994). Attachment and meta-monitoring: Implications for adolescent autonomy and psychopathology. In Cicchetti D & Toth SL (Eds.), Rochester Symposium on Developmental Psychopathology: Disorders and Dysfunctions of the Self (pp. 267297). Rochester, NY: University of Rochester Press. [Google Scholar]
- Laird RD, Criss MM, Pettit GS, Bates JE, & Dodge KA (2009). Developmental Trajectories and Antecedents of Distal Parental Supervision. The Journal of Early Adolescence, 29(2), 258–284. doi:10.1177/0272431608320123 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laird RD, Criss MM, Pettit GS, Dodge KA, & Bates JE (2008). Parents’ monitoring knowledge attenuates the link between antisocial friends and adolescent delinquent behavior. Journal of Abnormal Child Psychology, 36(3), 299–310. doi:10.1007/s10802-007-9178-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laird RD, Marrero M, Sherwood JK (2010). Developmental and interactional antecedents of monitoring in early adolescence. In Guillamos-Ramos JJV, & Dittus P (Ed.), Parental Monitoring of Adolescents: Current Perspectives for Researchers and Practitioners (pp. 39–66). New York: Columbia University Press. [Google Scholar]
- Larson RW, Richards MH, Moneta G, Holmbeck G, & Duckett E (1996). Changes in adolescents’ daily interactions with their families from ages 10 to 18: Disengagement and transformation. Developmental Psychology, 32(4), 744–754. doi:10.1037/0012-1649.32.4.744 [Google Scholar]
- Latendresse SJ, Ye F, Chung T, Hipwell A, & Sartor CE (2017). Parental Monitoring and Alcohol Use Across Adolescence in Black and White Girls: A Cross-Lagged Panel Mixture Model. Alcoholism: Clinical and Experimental Research, 41(6), 1144–1153. doi:10.1111/acer.13386 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lezin N, Rolleri LA, Bean S, & Taylor J (2004). Parent-child Connectedness: Implications for Research, Interventions, and Positive Impacts on Adolescent Health Retrieved from Santa Cruz, CA: http://recapp.etr.org/recapp/documents/research/litreview.pdf [Google Scholar]
- Loeber R, & Farrington DP (1998). Serious and Violent Juvenile Offenders: Risk Factors and Successful Interventions: SAGE Publications. [Google Scholar]
- MacKinnon DP, Fairchild AJ, & Fritz MS (2007). Mediation analysis. Annual Review of Psychology, 58, 593–614. doi:10.1146/annurev.psych.58.110405.085542 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manuel Barrera J, Biglan A, Ary D, & Li F (2001). Replication of a Problem Behavior Model with American Indian, Hispanic, and Caucasian Youth. The Journal of Early Adolescence, 21(2), 133–157. doi:doi:10.1177/0272431601021002001 [Google Scholar]
- Marceau K, Abar CC, & Jackson KM (2015). Parental Knowledge is a Contextual Amplifier of Associations of Pubertal Maturation and Substance Use. Journal of Youth and Adolescence, 44(9), 1720–1734. doi:10.1007/s10964-015-0335-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP, Dermody SS, Cheong J, Burton CM, Friedman MS, Aranda F, & Hughes TL (2013). Trajectories of Depressive Symptoms and Suicidality Among Heterosexual and Sexual Minority Youth. Journal of Youth and Adolescence, 42(8), 1243–1256. doi:10.1007/s10964-013-9970-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP, Dermody SS, Shultz ML, Sucato GS, Stepp SD, Chung T, . . . Hipwell AE (2013). Mental health and substance use disparities among urban adolescent lesbian and bisexual girls. Journal of the American Psychiatric Nurses Association, 19(5), 271–279. doi:10.1177/1078390313503552 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP, Friedman MS, Stall R, King KM, Miles J, Gold MA, . . . Morse JQ (2008). Sexual orientation and adolescent substance use: a meta-analysis and methodological review. Addiction, 103(4), 546–556. doi:10.1111/j.1360-0443.2008.02149.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP, King KM, Stepp SD, Hipwell A, Smith H, Chung T, . . . Markovic N (2012). Trajectories of alcohol and cigarette use among sexual minority and heterosexual girls. Journal of Adolescent Health, 50(1), 97–99. doi:10.1016/j.jadohealth.2011.05.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP, Sucato G, Stepp SD, Hipwell A, Smith HA, Friedman MS, . . . Markovic N (2012). Substance use and mental health disparities among sexual minority girls: results from the Pittsburgh girls study. Journal of Pediatric & Adolescent Gynecology, 25(1), 15–18. doi:10.1016/j.jpag.2011.06.011 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Masche JG (2010). Explanation of normative declines in parents’ knowledge about their adolescent children. Journal of Adolescence, 33(2), 271–284. doi:https://doi.org/10.1016/j.adolescence.2009.08.002 [DOI] [PubMed] [Google Scholar]
- Metzger A, Wakschlag LS, Anderson R, Darfler A, Price J, Flores Z, & Mermelstein R (2013). Information Management Strategies Within Conversations About Cigarette Smoking: Parenting Correlates and Longitudinal Associations With Teen Smoking. Developmental Psychology, 49(8), 1565–1578. doi:10.1037/a0030720 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer IH (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychological Bulletin, 129(5), 674–697. doi:10.1037/0033-2909.129.5.674 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Montano GT, McCauley HL, Miller E, Chisolm DJ, & Marshal MP (2016). Differences in Parental Monitoring Components and Their Associated Health Indicators Between Sexual-Minority and Heterosexual Girls. Journal of GLBT Family Studies, 1–25. Retrieved from http://dx.doi.org/10.1080/1550428X.2016.1200507 doi:10.1080/1550428X.2016.1200507 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Montano GT, McCauley HL, Miller E, Chisolm DJ, & Marshal MP (2017). Trends in Parental Monitoring and Knowledge Over Time Between Sexual Minority and Heterosexual Girls. Journal of Research on Adolescence doi:10.1111/jora.12316 [DOI] [PubMed] [Google Scholar]
- Nagin D (2005). Group-based Modeling of Development Retrieved from http://pitt.idm.oclc.org/login?url=http://site.ebrary.com/lib/pitt/Top?id=10312815 [Google Scholar]
- Nagin DS, & Odgers CL (2010). Group-based trajectory modeling in clinical research. Annual Revivew of Clinical Psychology, 6, 109–138. doi:10.1146/annurev.clinpsy.121208.131413 [DOI] [PubMed] [Google Scholar]
- National Institute on Alcohol Abuse and Alcoholism. (2018). Drinking Levels Defined Retrieved from https://www.niaaa.nih.gov/alcohol-health/overview-alcoholconsumption/moderate-binge-drinking
- Otten R, Harakeh Z, Vermulst AA, Van den Eijnden RJ, & Engels RC (2007). Frequency and quality of parental communication as antecedents of adolescent smoking cognitions and smoking onset. Psychology of Addictive Behaviors, 21(1), 1–12. doi:10.1037/0893-164x.21.1.1 [DOI] [PubMed] [Google Scholar]
- Pandina RJ, Labouvie EW, & White HR (1984). Potential Contributions of the Life Span Developmental Approach to the Study of Adolescent Alcohol and Drug Use: The Rutgers Health and Human Development Project, a Working Model. Journal of Drug Issues, 14(2), 253–268. doi:10.1177/002204268401400206 [Google Scholar]
- Racz SJ, & McMahon RJ (2011). The relationship between parental knowledge and monitoring and child and adolescent conduct problems: a 10-year update. Clinical Child and Family Psychology Review, 14(4), 377–398. doi:10.1007/s10567-011-0099-y [DOI] [PubMed] [Google Scholar]
- Rubin DB (1976). Inference and missing data. Biometrika, 63(3), 581–592. doi:https://doi.org/10.1093/biomet/63.3.581 [Google Scholar]
- Ryan RM, & Lynch JH (1989). Emotional Autonomy versus Detachment: Revisiting the Vicissitudes of Adolescence and Young Adulthood. Child Development, 60(2), 340–356. doi:10.2307/1130981 [DOI] [PubMed] [Google Scholar]
- Ryan SM, Jorm AF, & Lubman DI (2010). Parenting factors associated with reduced adolescent alcohol use: A systematic review of longitudinal studies. Australian and New Zealand Journal of Psychiatry, 44(9), 774–783. doi:10.1080/00048674.2010.50175920815663 [DOI] [PubMed] [Google Scholar]
- Saltzburg S (2007). Narrative Therapy Pathways for Re-authoring with Parents of Adolescents Coming-out as Lesbian, Gay, and Bisexual. Contemporary Family Therapy, 29(1), 57–69. doi:10.1007/s10591-007-9035-1 [Google Scholar]
- Stattin H, & Kerr M (2000). Parental monitoring: a reinterpretation. Child Development, 71(4), 1072–1085. [DOI] [PubMed] [Google Scholar]
- Svensson R (2003). Gender differences in adolescent drug use: The impact of parental monitoring and peer deviance. Youth & Society, .34(3), pp. doi:10.1177/0044118X02250095 [Google Scholar]
- Tavakol M, & Dennick R (2011). Making sense of Cronbach’s alpha. International Journal of Medical Education, 2, 53–55. doi:10.5116/ijme.4dfb.8dfd [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tilton-Weaver L, Kerr M, Pakalniskeine V, Tokic A, Salihovic S, & Stattin H (2010). Open up or close down: how do parental reactions affect youth information management? Journal of Adolescence, 33(2), 333–346. doi:10.1016/j.adolescence.2009.07.011 [DOI] [PubMed] [Google Scholar]
- Tobler AL, & Komro KA (2010). Trajectories or parental monitoring and communication and effects on drug use among urban young adolescents. Journal of Adolescent Health, 46(6), 560–568. doi:10.1016/j.jadohealth.2009.12.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.