

Abstract
Background:
Treatment adherence and viral suppression remain sub-optimal in the US. Attachment insecurity may be one understudied factor affecting adherence. According to attachment theory, people develop generalized internal working models of interpersonal relationships, which shape their perceptions of the availability of others at times of stress and how they handle stressors as an individual. Two dimensions of attachment insecurity are attachment-related avoidance (avoidance of intimacy with others and avoidance of negative emotions) and attachment-related anxiety (feeling unable to deal with stressors without others’ help). For people living with chronic stressful health conditions that require life-long self-management, attachment-related avoidance and attachment-related anxiety may diminish the ability to cope with stressors as an individual leading to negative health outcomes.
Methods:
We examined cross-sectional associations of the two attachment-related insecurity dimensions with ART adherence, HIV visit adherence, CD4 cell counts, and viral suppression. Survey and clinical data from 453 women living with HIV in four US cities were analyzed controlling for age, education, income, time on ART, illicit drug use, and race.
Results:
Attachment-related avoidance was the only unique predictor of sub-optimal ART adherence, viral failure, and low CD4 count, and attachment-related anxiety was the only unique predictor of missed HIV care visits. These effects were over and above the effects of all covariates. ART adherence mediated the association of attachment-related avoidance with both viral failure and low CD4 counts.
Conclusions:
Interventions may need to focus on the vulnerable sub-population with high attachment insecurity and incorporate existing strategies that address insecure attachment models.
Keywords: Attachment, HIV, Psychosocial, Insecurity, Avoidance, Anxiety
Introduction
Antiretroviral treatment (ART) adherence and viral suppression remain sub-optimal for many people living with HIV (PLWH) in the US, with latest estimates of viral suppression rate only at around 49%.1 Many structural and social factors affecting adherence have been identified. However, in order to reduce the remaining barriers to achieving 90–90-90 targets, it is also important to understand key psychological factors affecting adherence so that we can identify all PLWH at risk for viral failure and develop effective interventions to help them achieve optimal health.
How PLWH feel and think about interpersonal relationships in general is an understudied factor in affecting their health behaviors and outcomes, with potential effects independent of already identified factors. Interpersonal relationship insecurity, a construct of attachment theory, is one of the most influential constructs in social/personality psychology research.2 According to attachment theory, based on previous support experiences with other people at times of stress, people develop generalized mental representations (internal working models) of close relationships, which affect their perceptions of others’ availability at times of stress and how they handle stressors as an individual.
Modern measures in social-personality psychology conceptualize two dimensions of insecure working models for adults: attachment-related avoidance and attachment-related anxiety. People with high levels of attachment-related avoidance have a tendency to not trust others to be supportive, avoid all forms of intimacy with others, avoid distress-related cognitions and emotions, and have a preference for over-independence when dealing with stressors. People with high levels of attachment-related anxiety have chronic worries about their own value and feel unable to deal with stressors by themselves.
There is extensive evidence (based on thousands of published research articles) that these two forms of chronic relationship insecurity are among the most important predictors of psychological and physical well-being, especially at times of stress. These effects are distinct from the effects of current relationship status and of constructs such as neuroticism, social support, or satisfaction with a current relationship.2 Attachment-related avoidance and anxiety are also not associated with most genetic factors examined, except for a modest Gene-by-Environment interaction for the HTR2A rs6313 single-nucleotide polymorphism for attachment-related avoidance found in only one study.3
According to attachment theory, mental representations of attachment relationships affect not only “view of others”, but also “view of the self”.2,4 As a result, attachment-related anxiety is associated with perceptions of the self as being less lovable, less valuable, and less able to deal with stressors without others’ help. Attachment-related anxiety leads to constantly seeking others’ help, preoccupation with stressful events, as well as higher depressive symptoms (in cross-sectional as well as longitudinal analyses).2 There is also substantial evidence that attachment-related avoidance is associated with negative psychological outcomes; however, effect sizes are smaller in healthy populations using self-reported outcomes, especially under non-stress conditions. Attachment-related avoidance leads to avoiding intimacy with others, denying the need for others’ help, coping by avoidance and with suppression of negative emotions, distress, and perceptions of weakness in order to feel and appear self-reliant. Therefore, individuals with high levels of attachment-related avoidance tend to underreport maladaptive tendencies, distress, lack of self-esteem, and low self-efficacy. However, it has been argued that this is part of a defensive strategy to appear self-reliant and breaks down when facing serious and persistent stressors.5 Indeed, the associations between attachment-related avoidance and negative outcomes are much stronger when people face severe real-life problems, including chronic diseases, especially when objectively measured (as opposed to self-reported) outcomes are examined.2,5,6
Thus, attachment-related insecurity predicts not only interpersonal outcomes, but also coping strategies and behaviors as an individual at times of stress.2 That is, models of attachment may affect outcomes through both interpersonal (e.g., not seeking others’ help) and intrapersonal (e.g., individual coping strategies) mechanisms. For people living with chronic, stressful, and burdensome health conditions that require life-long self-management, both attachment-related avoidance and attachment-related anxiety may interfere with treatment adherence. One possible mechanism is that both types of insecure attachment models (i.e., attachment-related avoidance and attachment-related anxiety) lead to low perceived self-efficacy and low ability to cope with stressors and interfere with a task-oriented focus and persistence with demanding daily self-care tasks.2 For individuals with high levels of attachment-related avoidance, the defensive strategy to avoid distress and negative emotions when dealing with a chronic and serious health condition often involves directing attention away from illness, which may be an additional factor that interferes with active engagement in self-care and optimal treatment behaviors.5
Therefore, we hypothesized that both insecurity dimensions are negatively associated with HIV-related health outcomes, although attachment-related avoidance may be the more important unique predictor, as it is when predicting diabetes-related outcomes.5 Attachment-related anxiety is associated with ambivalent attitudes toward others (requesting others’ help but also not being satisfied with the help provided and showing angry reactions to others’ input). Thus, attachment-related anxiety may have two effects in opposite directions through two different mechanisms. For example, when facing stressors, people with high attachment-related anxiety want more support because they perceive themselves unable to deal with stressors alone. At the same time, they may want less support because of anticipated negative interactions with the support provider.7 Therefore, attachment-related anxiety may predict scheduling more HIV care visits, but lower adherence to scheduled visits.
The relatively limited research examining the effects of working models of attachment in chronic health conditions has found that attachment insecurity predicts poor medication adherence and adverse health outcomes (including mortality) in chronic diseases such as diabetes,5,8–10 hepatitis,11 and lupus.12 However, there is little research on working models of attachment and HIV outcomes and effects may be even larger for HIV, since stigma and other interpersonal/psycho-social factors play important roles in HIV. Two previous small-scale studies reported that attachment-related insecurity is associated with psychological distress or maladjustment for PLWH.13,14 The goal of the present article is to examine the hypothesis that both attachment-related avoidance and attachment-related anxiety are associated with HIV-related outcomes (ART adherence, viral suppression, CD4 count, and HIV visit adherence) in a sample of women living with HIV in four cities in the United States. First, in multivariate models, we examined the unique predictive value of each dimension by controlling for the other dimension. Since the high correlation between the two dimensions may mask the unique contribution of the other, we also examined their effects on outcomes without controlling for the other dimension. Furthermore, we examined the interactive effect of the two dimensions.
Methods
Participants and Procedures
Data were drawn from the Women’s Adherence and Visit Engagement (WAVE) sub-study nested in the Women’s Interagency HIV Study (WIHS, a multi-site cohort study15). In the WAVE Study, data on psycho-social aspects of living with HIV are collected annually from women enrolled at the four WIHS sites: San Francisco, CA, Atlanta, GA, Birmingham, AL, and Jackson, MS. The current study uses data from the first round of WAVE questionnaires (2016–2017; N = 453). Participants completed an interviewer-assisted data collection procedure during a separate research visit, with similar methods to those used in the WIHS core data collection, and the data collected through WAVE are linked with data collected through WIHS, which includes ART adherence and HIV visit adherence, as well as blood draws for assessment for HIV RNA viral load and CD4 counts. Viral load was dichotomized as suppressed versus not suppressed (viral failure) using a cutoff value of 200 copies/mL. CD4 cell count values (cells/mm3) were square root-transformed to approximate a normal distribution (Kolmogorov-Smirnov test statistic = 0.2, p = .20 after transformation). All participants provided written informed consent. All study activities were approved by the sites’ Institutional Review Boards.
Measures
Insecure working models of interpersonal relationships:
A shorter 18-item version of the most widely used attachment style measure—Experiences in Close relationships (ECR16)—was used. ECR assesses two dimensions of generalized insecure attachment models with all interpersonal relationship partners: attachment-related avoidance and attachment-related anxiety. Sample items are “I prefer not to show a partner how I feel deep down” for the avoidance dimension and “My desire to be very close sometimes scares people away” for the anxiety dimension. Participants rated each item on a 7-point scale ranging from 1 (strongly disagree) to 7 (strongly agree). In the current sample, Cronbach’s alpha reliability coefficients for attachment-related avoidance and attachment-related anxiety were .88 and .90, respectively. The two dimensions showed a much higher correlation (r = .65, p < .001) compared to the typical correlation found in healthy populations (a meta-analysis reports r = .15).17
ART adherence:
In WIHS, ART adherence is assessed with a self-reported item asking how often participants took their medications as prescribed over the past six months. Response options were “100% of the time”, “95–99% of the time”, “75–94% of the time”, “<75% of the time”, and “I haven’t taken any of my prescribed medications”. Previous research provides support for the validity of this measure of adherence.18,19 As in previous studies,20,21 we used the cutoff for optimal versus sub-optimal adherence to be at 95%, resulting in a dichotomized variable (0 = optimal adherence; 1 = sub-optimal adherence).
HIV visit adherence:
In WIHS, visit adherence to HIV primary care appointments is assessed using self-reported data on whether participants missed any appointments since the last assessment. Previous studies provide evidence for the validity of self-reported missed visits, which showed associations with viral suppression and mortality.22–26 For the current analyses, sub-optimal visit adherence was defined as missing at least one HIV visit in the last two years in order to increase reliability of the measure as was done in previous research27 (0 = made all visits in the last two years; 1 = missed one or more visits in the last two years). The data also include perceived frequency of provider demand for visits: “How often do your HIV providers want to see you for your regular HIV care?” (dichotomized as less than three times a year vs. three times a year or more frequently).
Statistical Analyses
In order to be consistent, we used the same covariates in all analyses that previous research and theory suggest as important: Age, site, education, income, time on ART, intimate partner status, illicit drug use, site, and race (categorized as non-Hispanic white versus others as in other analyses using WIHS cohort data21,28). Bivariate and multivariate logistic regression analyses were conducted with viral failure as the outcome. In multivariate analyses we first entered both insecurity dimensions together as predictors. Then, the non-significant insecurity dimension was entered without controlling for the other insecurity dimension to see if it becomes a significant predictor. Similar analyses were then conducted using CD4 count, sub-optimal ART adherence or missing HIV care visits as outcomes (using a multiple linear regression for continuous CD4 count).
A mediation analysis was conducted using the PROCESS software29 to examine whether the significant association of attachment-related avoidance with viral failure is mediated by ART adherence (used as a continuous variable with higher values indicating better adherence, since PROCESS mediation models cannot be used with binary mediators). The analysis for attachment-related avoidance was first performed without including attachment-related anxiety as a covariate and then including it in the model (all other covariates were included in all mediation analyses). Similar mediation analyses were then performed using CD4 counts as the outcome. These mediation models were conducted using bootstrapping, which provides a non-parametric test that does not rely on assumptions of normal distribution. The significance of the indirect effect of attachment-related avoidance on viral failure or on CD4 counts through ART adherence was evaulated.29 In this method, a significant indirect effect (indicated by a 95% confidence interval that does not include zero) provides evidence for mediation.
Results
Descriptive statistics for the study sample are presented in Table 1. Results using viral failure as the outcome are presented in Table 2. In the adjusted model, attachment-related avoidance was significantly (and uniquely) associated with viral failure, whereas attachment-related anxiety was not significantly associated with viral failure. When attachment-related avoidance was omitted from the model, attachment-related anxiety was not associated with viral failure (AOR = 1.15, p=.07, CI=0.99, 1.34). When added to the model, the interaction between attachment-related avoidance and attachment-related anxiety was not significantly associated with viral failure (AOR = 0.97, p=.62, CI=0.88, 1.08).
Table 1.
Descriptive Statistics for the Study Sample (N=453)
| n (%) | ||
|---|---|---|
| Variable | ||
| Race | ||
| Non-Hispanic white | 63 (14.0) | |
| African-American | 347 (76.7) | |
| Hispanic | 25 (5.5) | |
| Other (racial minority) | 17 (3.8) | |
| Either married or living with romantic partner | ||
| Yes | 118 (26.8) | |
| No | 323 (73.2) | |
| Household income | ||
| ≤ $ 12,000 | 250 (56.9) | |
| > $ 12,000 | 189 (43.1) | |
| Education | ||
| No college education | 270 (59.7) | |
| At least some college education | 182 (40.3) | |
| Illicit drug use | ||
| Yes | 145 (32.3) | |
| No | 304 (67.7) | |
| ART adherence | ||
| <95% | 76 (17.8) | |
| ≥95% | 351 (82.2) | |
| Viral failure (>200 copies/mL) | ||
| Yes | 147 (32.5) | |
| No | 305 (67.5) | |
| HIV care visit adherence | ||
| Adherent (did not miss visits) | 323 (70.5) | |
| Missed at least one visit | 135 (29.5) | |
| Variable | Mean (SD) | Range |
| Age (years) | 49.06 (9.44) | 28 – 82 |
| Viral load (copies/mL) | 2284.2 (18468.9) | 20 −328000 |
| Months on ART | 104.08 (71.8) | 1 −279 |
| Attachment-related avoidance | 3.36 (1.46) | 1 – 7 |
| Attachment-related anxiety | 3.66 (1.58) | 1 – 7 |
| CD4 count (cells/mm3) | 661.39 (329.9) | 35 – 2862 |
Table 2.
Unadjusted and adjusted logistic regression results using HIV viral failure as the outcome (>200 copies/mL).
|
Characteristics |
Unadjusteda | Adjustedb |
|---|---|---|
| OR (95% CI) | AOR (95% CI) | |
| Age | — | 1.00 (0.98, 1.03) |
| Site | — | Wald χ2=4.66 |
| Annual household income >$12,000 | — | 0.63 (0.38, 1.03) |
| More than high school education | — | 1.39 (0.86, 2.25) |
| Non-Hispanic white race/ethnicity | — | 1.05 (0.53, 2.10) |
| Married or living with partner | — | 1.71 (0.89, 3.26) |
| Illicit drug use since last visit | — | 1.66 (1.03, 2.69)* |
| Months on ART | — | 1.00 (1.00, 1.01) |
| Attachment-related avoidance | 1.16 (1.01, 1.33)* | 1.26 (1.02, 1.56)* |
| Attachment-related anxiety | 1.10 (0.97, 1.24) | 1.00 (0.83, 1.22) |
p<0.05
Unadjusted logistic regression using viral failure as the outcome and each attachment dimension separately as predictor (without controlling for any covariates or the other attachment dimension)
Logistic regression using viral failure as the outcome adjusting for age, study site, household income, education, race/ethnicity, intimate partner status, illicit drug use since last visit, months on ART, as well as the other attachment dimension.
Results using CD4 count as the outcome are presented in Table 3 (this time using multiple linear regression due to the continuous nature of this variable). In the adjusted model, attachment-related avoidance was significantly (and uniquely) associated with low CD4 count, whereas attachment-related anxiety was not significantly associated with CD4 count. When attachment-related avoidance was omitted from the model, attachment-related anxiety was significantly associated with low CD4 count (B = −0.79, SE = 0.20, p<.001). When added to the model, the interaction between attachment-related avoidance and attachment-related anxiety was not significantly associated with CD4 count (B = −0.16, SE = 0.14, p=.26).
Table 3.
Unadjusted and adjusted multiple linear regression results using CD4 cell count as the outcome (using square root transformation).
|
Characteristics |
Unadjusteda | Adjustedb |
|---|---|---|
| B (SE) | B (SE) | |
| Age | — | .00 (.04) |
| Site | — | F = 6.21*** |
| Average annual household income >$12,000 | — | −0.17 (0.67) |
| More than high school education | — | −0.56 (0.66) |
| Non-Hispanic white race/ethnicity | — | −0.56 (0.66) |
| Married or living with partner | — | 1.71 (0.89, 3.26) |
| Illicit drug use since last visit | — | −1.73 (0.70)* |
| Months on ART | — | −0.02 (0.01)** |
| Attachment-related avoidance | −0.90 (0.21)*** | −0.64 (0.29)* |
| Attachment-related anxiety | −0.73 (0.19)*** | −0.40 (0.27) |
p<0.05;
p<0.01;
p<0.001
Unadjusted multiple regression using CD4 cell count as the outcome and each attachment dimension separately as predictor (without controlling for any covariates or the other attachment dimension).
Multiple regression using CD4 cell count as the outcome adjusting for age, study site, household income, education, race/ethnicity, intimate partner status, illicit drug use since last visit, months on ART, as well as the other attachment dimension.
Results using sub-optimal ART adherence as the outcome are presented in Table 4. In the adjusted model, attachment-related avoidance was significantly (and uniquely) associated with sub-optimal ART adherence, whereas attachment-related anxiety was not significantly associated with sub-optimal ART adherence. When attachment-related avoidance was omitted from the model, attachment-related anxiety was significantly associated with sub-optimal ART adherence (AOR = 1.24, p=.02, CI=1.03, 1.50). When added to the model, the interaction between attachment-related avoidance and attachment-related anxiety was not significantly associated with sub-optimal ART adherence (AOR = 0.94, p=.36, CI=0.82, 1.08).
Table 4.
Unadjusted and adjusted logistic regression results using sub-optimal antiretroviral treatment (ART) adherence as the outcome.
|
Characteristics |
Unadjusteda | Adjustedb |
|---|---|---|
| OR (95% CI) | AOR (95% CI) | |
| Age | — | 0.99 (0.96, 1.03) |
| Site | — | Wald χ2=6.99 |
| Average annual household income >$12,000 | — | 0.85 (0.47, 1.57) |
| More than high school education | — | 1.36 (0.75, 2.47) |
| Non-Hispanic white race/ethnicity | — | 0.55 (0.21, 1.48) |
| Married or living with partner | — | 1.71 (0.89, 3.26) |
| Illicit drug use since last visit | — | 2.54 (1.41, 4.60)** |
| Months on ART | — | 1.00 (1.00, 1.01) |
| Attachment-related avoidance | 1.30 (1.10, 1.55)** | 1.35 (1.03, 1.76)* |
| Attachment-related anxiety | 1.14 (0.98, 1.34) | 1.04 (0.81, 1.33) |
p<0.05;
p<0.01
Unadjusted logistic regression using sub-optimal ART adherence as the outcome and each attachment dimension separately as predictor (without controlling for any covariates or the other attachment dimension)
Logistic regression using sub-optimal ART adherence as the outcome adjusting for age, study site, household income, education, race/ethnicity, intimate partner status, illicit drug use since last visit, months on ART, as well as the other attachment dimension.
Finally, results using sub-optimal visit adherence as the outcome are presented in Table 5. In the adjusted model, attachment-related anxiety was significantly (and uniquely) associated with sub-optimal visit adherence, whereas attachment-related avoidance was not significantly associated with sub-optimal visit adherence. When attachment-related anxiety was omitted from the model, attachment-related avoidance was significantly associated with sub-optimal visit adherence (AOR = 1.20, p=.02, CI=1.03, 1.40). When added to the model, the interaction between attachment-related avoidance and attachment-related anxiety was not significantly associated with sub-optimal visit adherence (AOR = 1.08, p=.14, CI=0.98, 1.20). Even though attachment-related anxiety was associated with sub-optimal visit adherence, it was associated with higher perceived frequency of provider demand for visits in adjusted analyses (AOR = 1.27, p=.04, CI=1.01, 1.49).
Table 5.
Unadjusted and adjusted logistic regression results using sub-optimal adherence to HIV care visits as the outcome.
|
Characteristics |
Unadjusteda | Adjustedb |
|---|---|---|
| OR (95% CI) | AOR (95% CI) | |
| Age | — | 0.97 (0.95, 1.00)* |
| Site | — | Wald χ2=3.21 |
| Average annual household income >$12,000 | — | 0.44 (0.27, 0.74)** |
| More than high school education | — | 1.15 (0.71, 1.87) |
| Non-Hispanic white race/ethnicity | — | 0.54 (0.24, 1.23) |
| Married or living with partner | — | 1.71 (0.89, 3.26) |
| Illicit drug use since last visit | — | 1.47 (0.89, 2.41) |
| Months on ART | — | 0.98 (0.99, 1.00) |
| Attachment-related avoidance | 1.22 (1.06, 1.41)** | 1.04 (0.85, 1.28) |
| Attachment-related anxiety | 1.26 (1.10, 1.43)** | 1.22 (1.01, 1.49)* |
p<0.05;
p<0.01
Unadjusted logistic regression using sub-optimal adherence to HIV care visits as the outcome and each attachment dimension separately as predictor (without controlling for any covariates or the other attachment dimension)
Logistic regression using sub-optimal adherence to HIV care visits as the outcome adjusting for age, study site, household income, education, race/ethnicity, intimate partner status, illicit drug use since last visit, months on ART, as well as the other attachment dimension.
Next, we examined the mediation hypothesis depicted in Figure 1: The association between attachment-related avoidance and viral failure is mediated by ART adherence. This indirect effect was significant (B=0.05, SE=0.02, CI=0.02, 0.11), suggesting mediation. In this model, the direct effect (after controlling for the mediating effect of ART adherence) was also significant (B=0.19, SE=0.09, CI=0.02, 0.36). When attachment-related anxiety was added as a control variable, the indirect effect of attachment-related avoidance was no longer significant (B=0.03, SE=0.02, CI=−0.01, 0.09). When attachment-related avoidance was not in the model, the indirect effect of attachment-related anxiety on viral failure through ART adherence was also significant (B=0.05, SE=0.02, CI=0.02, 0.10).
Figure 1.
The mediating role of ART adherence in the association between attachment-related avoidance and viral failure.
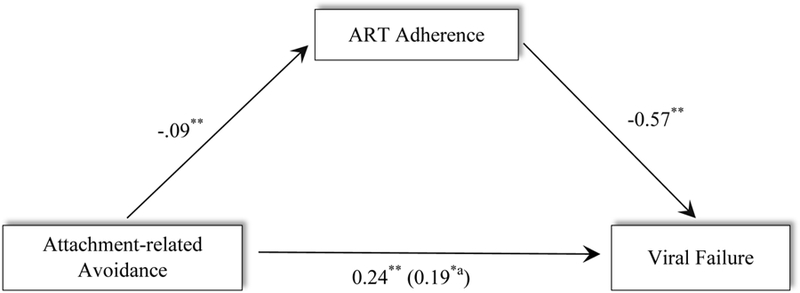
Note. Associations are presented as path coefficients (unstandardized). Age, site, education, income, time on ART, illicit drug use, romantic partner status, and race were used as covariates.
a When ART adherence is in the model.
*p <.05
** p < .01
The indirect effect of attachment-related avoidance through ART adherence on CD4 count was also significant (B=−0.07, SE=0.05, CI=−0.18, −0.004). In this model, the direct effect (after controlling for the mediating effect of ART adherence) was also significant (B=−0.93, SE=0.22, CI=−1.37, −0.49). When attachment-related anxiety was added as a control variable, the indirect effect of attachment-related avoidance was no longer significant (B=−0.04, SE=0.04, CI=−0.16, 0.003). When attachment-related avoidance was not in the model, the indirect effect of attachment-related anxiety on CD4 count through ART adherence was also significant (B=−0.07, SE=0.04, CI=−0.18, −0.01).
Discussion
In this sample of women living with HIV across different geographical contexts in the US, we found that attachment-related avoidance was uniquely associated with viral failure, lower CD4 count, and sub-optimal ART adherence. Attachment-related anxiety was associated with missing HIV care visits. These effects were over and above the effects of income, education, race, intimate partner status, and substance use, as well as the other attachment insecurity dimension. Given that attachment-related avoidance was the only unique predictor of most HIV outcomes, this dimension of attachment-related insecurity may be more important for women living with HIV. However, the two dimensions showed a substantial correlation, and this may have masked the unique effect of attachment-related anxiety on some outcomes. When examined without attachment-related avoidance in the model, attachment-related anxiety was also significantly associated with most outcomes. Similarly, when entered without attachment-related anxiety, attachment-related avoidance was significantly associated with missing HIV care visits. We also found that the effects of both attachment-related avoidance and attachment-related anxiety on viral failure and lower CD4 count were mediated by ART adherence.
Findings on the association between attachment-related avoidance and these HIV-related outcomes suggest the possibility that the defensive suppression of distress and weakness associated with attachment-related avoidance can break down under the considerable stress that women living with HIV experience.6 Another mechanism for the negative effects of attachment-related avoidance on HIV-related health outcomes may be avoidance of distress- and weakness-related cognitions. This strategy requires directing attention away from one’s HIV status, which would reduce a person’s ability to engage in effective health behaviors consistently.
The literature suggests that attachment-related anxiety is associated with higher healthcare utilization.30,31 However, using our operationalization of visit adherence based on missing any scheduled visits, we found that attachment-related anxiety was associated with sub-optimal visit adherence. Yet, attachment-related anxiety was also associated with higher perceived frequency of provider demand for visits. It is possible that providers sense that patients with high attachment-related anxiety want more frequent contact with providers and therefore schedule more visits with them. It is also possible that PLWH with higher attachment-related anxiety perceive erroneously that providers want to see them more often.
This study had limitations. Our adherence measures relied on participants’ self-reports and attachment-related avoidance and anxiety may affect the self-reporting bias of adherence. The data are cross-sectional; therefore, the temporal and causal direction of effects cannot be established. Another important limitation is that we did not examine the contribution of variables such as depression, recent traumatic experiences, or PTSD in the associations reported. Previous longitudinal research suggests that attachment insecurity leads to depressive symptoms.2 Therefore, future longitudinal research should examine the mediating role of depression (as well as trauma and PTSD) in the effects of attachment insecurity on HIV health outcomes. Other mediators of the effect of interpersonal relationship insecurity on HIV health outcomes may be quality of relationships with close others and with healthcare providers.30,32
The present sample consisted of only women and generalizability to men, transgender individuals, or gender non-conforming individuals should be tested. Nevertheless, given that few psychosocial constructs have been so clearly linked with biological health outcomes, such as CD4 count and viral load, these results highlight the importance of future research on the effects of working models of attachment on HIV-related health outcomes.
The present results suggest that women living with HIV with high levels of attachment-related insecurity are at risk for negative HIV-related health outcomes. Interventions may need to focus strongly on this vulnerable sub-population. These intervention efforts may involve existing strategies addressing treatment adherence. The findings of this study also suggest additional important targets for interventions aiming to improve health outcomes for women living with HIV. If future longitudinal research in this area can identify factors that mediate the effects of attachment-related insecurity on HIV outcomes (e.g., depressive symptoms, self-efficacy), these factors can be targeted in interventions. Another strategy may be to try to reduce attachment-related insecurity using existing interventions. There are very promising brief group-based interventions developed to improve attachment-related security, which may benefit women living with HIV with attachment-related insecurities.33–35 Research also suggests that attachment-related insecurity decreases during traditional psychological interventions (e.g., cognitive-behavioral treatments) delivered either in group settings,33 or individually,36 with downstream effects on reduced psychiatric symptoms.
Furthermore, knowing the level and nature of interpersonal relationship insecurity of an individual living with HIV may have important implications for successful HIV care as well as for the success of any intervention. Research suggests that those individuals living with diabetes who have high interpersonal relationship insecurity benefit more from depression interventions using collaborative care, whereas individuals with obesity who have low interpersonal relationship insecurity benefit more from standard weight-reduction programs.32,37 Following up on these findings, researchers evaluated a communication intervention for the families of critically ill patients in the intensive care unit that included attachment style training for facilitators (i.e., understanding of types of interpersonal relationship insecurity, consequences of each type for relationships, and communication approaches most appropriate for each type of insecurity). Results suggested that facilitation of communication based on an understanding of insecurity is successful in decreasing depressive symptoms, intensive care costs, and length of hospital stay for intensive care patients.38 Therefore, some researchers argue that providing attuned medical care management in an “attachment informed” way (e.g., providing care that accounts for the patient’s lack of trust, need to be highly autonomous, etc.) is more effective than interventions aiming to change the patient’s interpersonal relationship insecurity,32 and strategies for accomplishing this have been described.30,31
ACKNOWLEDGEMENTS
We wish to acknowledge the assistance of the WIHS program staff and the contributions of the participants who enrolled in this study. This study was funded by Women’s Interagency HIV Study (WIHS) sub-study grants from the National Institute of Mental Health, R01MH104114 and R01MH095683. The contents of this publication are solely the responsibility of the authors and do not represent the official views of the National Institutes of Health (NIH). WIHS (Principal Investigators): UAB-MS WIHS (Mirjam-Colette Kempf and Deborah Konkle-Parker), U01-AI-103401; Atlanta WIHS (Ighovwerha Ofotokun and Gina Wingood), U01-AI-103408; Bronx WIHS (Kathryn Anastos and Anjali Sharma), U01-AI-035004; Brooklyn WIHS (Howard Minkoff and Deborah Gustafson), U01-AI-031834; Chicago WIHS (Mardge Cohen and Audrey French), U01-AI-034993; Metropolitan Washington WIHS (Seble Kassaye), U01-AI-034994; Miami WIHS (Margaret Fischl and Lisa Metsch), U01-AI-103397; UNC WIHS (Adaora Adimora), U01-AI-103390; Connie Wofsy Women’s HIV Study, Northern California (Ruth Greenblatt, Bradley Aouizerat, and Phyllis Tien), U01-AI-034989; WIHS Data Management and Analysis Center (Stephen Gange and Elizabeth Golub), U01-AI-042590; Southern California WIHS (Joel Milam), U01-HD-032632 (WIHS I – WIHS IV). The WIHS is funded primarily by the National Institute of Allergy and Infectious Diseases (NIAID), with additional co-funding from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), the National Cancer Institute (NCI), the National Institute on Drug Abuse (NIDA), and the National Institute on Mental Health (NIMH). Targeted supplemental funding for specific projects is also provided by the National Institute of Dental and Craniofacial Research (NIDCR), the National Institute on Alcohol Abuse and Alcoholism (NIAAA), the National Institute on Deafness and other Communication Disorders (NIDCD), and the NIH Office of Research on Women’s Health. WIHS data collection is also supported by UL1-TR000004 (UCSF CTSA), UL1-TR000454 (Atlanta CTSA), and P30-AI-050410 (UNC CFAR). This research was also supported by the University of Alabama at Birmingham (UAB) Center for AIDS Research CFAR, an NIH funded program (P30 AI027767) that was made possible by the following institutes: NIAID, NCI, NICHD, NHLBI, NIDA, NIA, NIDDK, NIGMS, and OAR. Trainee support was provided by the Agency for Healthcare Research and Quality (grant number T32HS013852).
Footnotes
The authors declare no conflicts of interest.
References
- 1.Crepaz N, Tang T, Marks G, Mugavero MJ, Espinoza L, Hall HI. Durable viral suppression among HIV-diagnosed persons – United States, 2012–2013 Conference on Retroviruses and Opportunistic Infections (CROI); 2016; Boston. [Google Scholar]
- 2.Mikulincer M, Shaver PR. Attachment in adulthood: Structure, dynamics, and change. New York: Guilford; 2007. [Google Scholar]
- 3.Fraley RC, Roisman GI, Booth-LaForce C, Owen MT, Holland AS. Interpersonal and genetic origins of adult attachment styles: A longitudinal study from infancy to early adulthood. J Pers Soc Psychol. 2013;104(5):817. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bartholomew K, Horowitz LM. Attachment styles among young adults: A test of a four-category model. J Pers Soc Psychol. 1991;61(2):226–244. [DOI] [PubMed] [Google Scholar]
- 5.Turan B, Osar Z, Turan JM, Ilkova H, Damci T. Dismissing attachment and outcome in diabetes: The mediating role of coping. J Soc Clin Psychol. 2003;22(6):607–626. [Google Scholar]
- 6.Mikulincer M, Florian V. The relationship between adult attachment styles and emotional and cognitive reactions to stressful events. Attachment theory and close relationships. 1998;143:165. [Google Scholar]
- 7.Guo J, Turan B. Preferences for Social Support During Social Evaluation in Men: The Role of Worry About a Relationship Partner’s Negative Evaluation. The Journal of social psychology. 2016;156(1):122–129. [DOI] [PubMed] [Google Scholar]
- 8.Ciechanowski Paul S., Katon Wayne J., Russo Joan E., Walker Edward A. The Patient-Provider Relationship: Attachment Theory and Adherence to Treatment in Diabetes. Am J Psychiatry. 2001;158(1):29–35. [DOI] [PubMed] [Google Scholar]
- 9.Cohen O, Birnbaum GE, Meyuchas R, Levinger Z, Florian V, Mikulincer M. Attachment orientations and spouse support in adults with type 2 diabetes. Psychol Health Med. 2005;10(2):161–165. [Google Scholar]
- 10.Ciechanowski P, Russo J, Katon WJ, et al. Relationship styles and mortality in patients with diabetes. Diabetes Care. 2010;33(3):539–544. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sockalingam S, Blank D, Abdelhamid N, Abbey SE, Hirschfield GM. Identifying opportunities to improve management of autoimmune hepatitis: evaluation of drug adherence and psychosocial factors. J Hepatol. 2012;57(6):1299–1304. [DOI] [PubMed] [Google Scholar]
- 12.Bennett JK, Fuertes JN, Keitel M, Phillips R. The role of patient attachment and working alliance on patient adherence, satisfaction, and health-related quality of life in lupus treatment. Patient Educ Couns. 2011;85(1):53–59. [DOI] [PubMed] [Google Scholar]
- 13.Ciesla JA, Roberts JE, Hewitt RG. Adult Attachment and High-Risk Sexual Behavior Among HIV-Positive Patients. J Appl Soc Psychol. 2004;34(1):108–124. [Google Scholar]
- 14.Turner-Cobb JM, Gore-Felton C, Marouf F, et al. Coping, Social Support, and Attachment Style as Psychosocial Correlates of Adjustment in Men and Women with HIV/AIDS. J Behav Med. 2002;25(4):337–353. [DOI] [PubMed] [Google Scholar]
- 15.Adimora AA, Ramirez C, Benning L, et al. Cohort Profile: The Women’s Interagency HIV Study (WIHS). Int J Epidemiol. 2018;47(2):393–394i. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Brennan KA, Clark CL, Shaver PR. Self-report measurement of adult attachment: An integrative overview In: Simpson JA, Rholes WS, eds. Attachment theory and close relationships. New York: Guilford Press; 1998:46–76. [Google Scholar]
- 17.Cameron JJ, Finnegan H, Morry MM. Orthogonal dreams in an oblique world: A meta-analysis of the association between attachment anxiety and avoidance. J Res Pers. 2012;46(5):472–476. [Google Scholar]
- 18.Feldman BJ, Fredericksen RJ, Crane PK, et al. Evaluation of the single-item self-rating adherence scale for use in routine clinical care of people living with HIV. AIDS Behav. 2013;17(1):307–318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lu M, Safren SA, Skolnik PR, et al. Optimal recall period and response task for self-reported HIV medication adherence. AIDS Behav. 2008;12(1):86–94. [DOI] [PubMed] [Google Scholar]
- 20.Kelso GA, Cohen MH, Weber KM, Dale SK, Cruise RC, Brody LR. Critical consciousness, racial and gender discrimination, and HIV disease markers in African American women with HIV. AIDS Behav. 2014;18(7):1237–1246. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Turan B, Smith W, Cohen MH, et al. Mechanisms for the Negative Effects of Internalized HIV-Related Stigma on Antiretroviral Therapy Adherence in Women: The Mediating Roles of Social Isolation and Depression. J Acquir Immune Defic Syndr. 2016;72(2):198–205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zinski A, Westfall AO, Gardner LI, et al. The contribution of missed clinic visits to disparities in HIV viral load outcomes. Am J Public Health. 2015;105(10):2068–2075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Horberg MA, Hurley LB, Silverberg MJ, Klein DB, Quesenberry CP, Mugavero MJ. Missed office visits and risk of mortality among HIV-infected subjects in a large healthcare system in the United States. AIDS Patient Care STDS. 2013;27(8):442–449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Mugavero MJ, Westfall AO, Cole SR, et al. Beyond core indicators of retention in HIV care: missed clinic visits are independently associated with all-cause mortality. Clin Infect Dis. 2014;59(10):1471–1479. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Craw JA, Gardner LI, Marks G, et al. Brief strengths-based case management promotes entry into HIV medical care: results of the antiretroviral treatment access study-II. J Acquir Immune Defic Syndr. 2008;47(5):597–606. [DOI] [PubMed] [Google Scholar]
- 26.Wilson TE, Kay ES, Turan B, et al. Healthcare Empowerment and HIV Viral Control: Mediating Roles of Adherence and Retention in Care. Am J Prev Med. In Press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Rice WS, Crockett KB, Mugavero MJ, Raper JL, Atkins GC, Turan B. Association Between Internalized HIV-Related Stigma and HIV Care Visit Adherence. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2017;76(5):482–487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Turan B, Rogers AJ, Rice WS, et al. Association between Perceived Discrimination in Healthcare Settings and HIV Medication Adherence: Mediating Psychosocial Mechanisms. AIDS Behav. 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hayes AF. Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. New York: Guilford Press; 2013. [Google Scholar]
- 30.Maunder R, Hunter J. Love, fear, and health: how our attachments to others shape health and health care. University of Toronto Press; 2015. [Google Scholar]
- 31.Hunter J, Maunder R. Improving patient treatment with attachment theory: A guide for primary care practitioners and specialists. Springer; 2015. [Google Scholar]
- 32.Ciechanowski PS, Russo JE, Katon WJ, et al. The association of patient relationship style and outcomes in collaborative care treatment for depression in patients with diabetes. Med Care. 2006;44(3):283–291. [DOI] [PubMed] [Google Scholar]
- 33.Page TF. Applications of Attachment Theory to Group Interventions: A Secure Base in Adulthood. In: Adult Attachment in Clinical Social Work. Springer; 2011:173–191. [Google Scholar]
- 34.Kilmann PR, Laughlin JE, Carranza LV, Downer JT, Major S, Parnell MM. Effects of an attachment-focused group preventive intervention on insecure women. Group Dyn. 1999;3(2):138–147. [Google Scholar]
- 35.Kilmann PR, Urbaniak GC, Parnell MM. Effects of attachment-focused versus relationship skills-focused group interventions for college students with insecure attachment patterns. Attachment & Human Development. 2006;8(1):47–62. [DOI] [PubMed] [Google Scholar]
- 36.Taylor P, Rietzschel J, Danquah A, Berry K. Changes in attachment representations during psychological therapy. Psychotherapy Research. 2015;25(2):222–238. [DOI] [PubMed] [Google Scholar]
- 37.Kiesewetter S, Köpsel A, Mai K, et al. Attachment style contributes to the outcome of a multimodal lifestyle intervention. Biopsychosoc Med. 2012;6(1):3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Curtis JR, Treece PD, Nielsen EL, et al. Randomized trial of communication facilitators to reduce family distress and intensity of end-of-life care. Am J Respir Crit Care Med. 2016;193(2):154–162. [DOI] [PMC free article] [PubMed] [Google Scholar]