

Abstract
BACKGROUND:
When transitioning from high school to university, students tend to gain weight.
AIM:
The study aimed to identify whether Lebanese students experience weight changes during the transition and to identify predisposing factors.
METHODS:
Eighty freshman students from four campuses in Lebanon were recruited in October 2015. Students were assessed anthropometrically and biochemically at two-time points, seven months apart. Students filled out questionnaires assessing demographic and lifestyle habits, physical activity levels, nutrition knowledge, sleep quality, and stress.
RESULTS:
The students gained approximately 4.19 lbs. (1.90 kg). There was a significant increase in waist circumference, blood glucose and triglyceride levels. There were no significant changes in HDL-cholesterol, total cholesterol, knowledge score, stress level, physical activity, sleep and lifestyle habits.
CONCLUSIONS:
Lebanese students do gain weight during their first year of university enrollment. Future research is necessary to assess the reasons for weight gain and develop suitable prevention programs.
Keywords: Freshman 15, College students, Weight gain, Obesity, Stress
Introduction
Obesity rates are at an all-time high and have reached epidemic magnitudes. According to World Health Organization data, more than 600 million adults were obese in 2014 [1]. These estimates are alarming since obesity increases the risk of a multitude of physiological and psychological chronic diseases and can lead to premature morbidity and mortality. The fight against obesity is fierce with researchers, health, and governmental organisations combining their efforts to restrict the uprise of this epidemic.
One strategy that is promising in combating obesity is to identify critical periods of weight gain; pinpoint vulnerable groups and accordingly, plan preventive interventions. One such identified critical period of weight gain is during student transition from high school to university or college [2]. This critical period could potentially dictate whether these students will live as healthy adults or possibly become overweight or obese by acquiring unhealthy habits especially since nutrition habits acquired at an early age and weight problems tend to continue in adulthood [3] [4]. Unfortunately, once weight gain occurs, it becomes hard to manage and increases vulnerability to obesity and subsequent complications [5] [6].
University students are at an increased risk of gaining weight during the freshman year; it has previously been hypothesised that the average collegian may gain approximately 15 pounds; a phenomenon that has been coined “The Freshman 15” [7]. However, more recent empirical evidence, suggests that the 15-pound increase is exaggerated and that a 3 to 5-pound weight gain is more realistic [8] [9]. Nevertheless, even a slight weight gain is still significant and is higher than the gain experienced by the general population [9] [10] [11] which may negatively affect the future health of these students. Therefore, prevention of weight gain in such a vulnerable group during this critical period could prove to be key in fighting obesity in this population.12 Explanations for this weight gain vary; however, some key factors that have been previously identified as culprits include increased alcohol and fast food consumption, decreased physical activity, moving away from home accompanied by lack of parental supervision and increased stress levels [13] [14]. Notably, stress may have a differential effect of on BMI [15]; Serlachius and colleagues found that students with a lower body weight tend to lose weight as a consequence of high-stress levels as opposed to students who have a higher BMI who tend to gain weight secondary to the increased stress [15].
Although, the freshman weight gain phenomena have been extensively researched and proven in the United States and Europe borders [6]; it is still not clear whether this phenomenon also applies among Middle Eastern students.
Therefore, this study aimed to investigate whether Lebanese students do gain weight during the freshman year, and determine the predisposing factors.
Methods
The study had a longitudinal design and was conducted in a private university with many campuses in Lebanon. Using two-step sampling, four campuses from different geographical locations were selected. Afterwards, all first-year students were invited to participate in the study via mass e-mail and through classroom visits made by the primary investigator. Students were informed about the objectives and methods of the study, in addition to their right to withdraw from the study at any time. Criteria for students to be included in the study were: 1) first semester of enrollment at the university, 2) free of disease, 3) not pregnant. Students were excluded from the study if they were sick at the time of the study, suffered from chronic diseases or were not fasting. Students who did not meet inclusion criteria were excluded. In total 80 students who volunteered met the inclusion criteria and consented. Ethical approval for this study was obtained from the university’s committee on Research Ethics (CRE) (case number: LIUCRE-141117-2). Participants completed the primary assessment in their first semester (T0) and then 7 months later during enrollment in the second semester (T1.) Only 40 students returned for follow-up out of which 27 consented to blood withdrawal. The reasons for the high dropout rate could be due to change in class schedules and fear of blood collection.
Sample Size: A statistical power analysis was performed using Power and sample size Calculations Software (version 3) to estimate the adequate number of participants needed for this study. Prior data indicate that the difference in the response of matched pairs is normally distributed with a standard deviation of 8.67. If the true difference in the mean response of matched pairs is 4.19, we would need 36 subjects to be able to reject the null hypothesis that this response difference is zero with probability (power) 0.8. Type I error probability associated with this test of this null hypothesis is 0.05. Therefore, this study was adequately powered.
Data collection took place during the first two weeks of the first semester, in the nutrition clinics of the selected campuses. The day before data collection, students were phone-called to remind them about the necessity of fasting for 12 hours before the blood draw and were given information on the location and time of meeting with the research team
Trained licensed dietitians assessed participant anthropometric which included: 1) height (cm) using a portable stadiometer, (ADE, Germany), measured to the nearest 0.1 cm, without shoes, with the subject stretching to the maximum height and the head positioned in the Frankfort plane; 2) weight (kg) using a calibrated beam scale, without shoes and while participants were wearing light clothes; waist circumference (cm) measured at the mid-point, half-way between the right iliac crest and the lower coastal region; [16] measured to the nearest 0.1 cm, using Accugirth measuring tapes. Body mass index (BMI) which is the ratio of weight (kg) and height squared (m2) was calculated. All participants were contacted after 7 months (T1) to recollect data using the same procedures adopted at baseline (T0).
Weight change was calculated by subtracting weight at T1 from weight at T0. A one pound difference(0.45 kg) was considered to be insignificant regarding weight change and was unaccounted for.
A blood sample of 5 ml was drawn from students by a licensed phlebotomist and samples were transported to the laboratory using a thermally insulated box. Serum was analyzed for cholesterol (mg/dl), triglyceride ((TG (mg/dl)), HDL-cholesterol ((HDL-C (mg/dl)), and fasting blood glucose (FBS (mg/dl)) concentrations. LDL-cholesterol ((LDL-C mg/dl)) was calculated. The analyses were performed using a Cobas C111 automated biochemical analyser (Roche Diagnostics, Indianapolis, IN, USA) based on spectrophotometric principles. Additionally, serum cortisol (nmol/L) was measured using Cobas e411 immunoassay automated analyser (Roche Diagnostics, Indianapolis, IN, USA) based on the electrochemiluminescence (ECLIA) principle. All blood collection was done early in the morning, after an overnight fast. After blood collection, students were served a light breakfast.
The students were then asked to fill a series of questionnaires:
1) Demographic and lifestyle habits questionnaire: adapted from Levitsky et al., (2004) [10], included 10 open-ended questions focused on some meals consumed daily and outside the home, living arrangements, smoking status, alcohol consumption. The questionnaire included questions about perceived weight changes by the students and whether they thought their weight had increased, decreased or remained constant
2) The International Physical Activity Questionnaire (IPAQ) (2014) short form: a validated tool used to measure the level of exercise [17] and consisting of seven questions assessing duration and frequency of light, moderate and vigorous physical activity completed in the past week. The Metabolic equivalent of tasks (METs) was calculated by multiplying the total minutes spent in the corresponding action with the frequency (days) and the constants of 3.3, 4.0 and 8.0 for light, moderate and vigorous activity respectively. The total MET value was computed by summing up the respective MET values for all activities that were done in bouts but were longer than 10 minutes in duration.
3) The General Nutrition Knowledge Questionnaire, adapted from Parmenter & Wardle, (1999) [18]: includes 28 open-ended and multiple choice questions. The choices were made to be culturally sensitive and specific to the food options consumed by the sample population. Cronbach’s alpha coefficient of the adapted questionnaire was 0.766, which is considered satisfactory;
4) The Pittsburgh Sleep Quality Index (PSQI), (2014), developed by Buysse et al (1989) [19]: a nine-item questionnaire where four questions assessed the duration (hours) of sleep, duration needed to fall asleep, time needed to wake up and awake time spent in bed; in addition to five other questions addressing the reasons of troubled sleep). Answers were converted to total scores using an algorithm adapted from the developers of the questionnaire, where higher scores indicated poor sleep quality.
5) The Perceived Stress Questionnaire [20]: a ten-item questionnaire is measuring stress levels in the last month. Answers followed a five-point scale with frequencies ranging from never to very often. The total score ranged between 0 and 40, where higher scores indicated higher stress levels.
All questionnaires were available in both English and Arabic, and respondents were able to choose their language preference. All instruments were pilot-tested on a sample of students before the study was conducted for validation, the results of which were discarded. It took students between 30 and 50 minutes to complete the questionnaires.
All statistical analyses were conducted using Statistical Package for Social Sciences (SPSS) version 21.0, IBM. P-values < 0.05 were considered statistically significant. Descriptive analyses were performed to summarise participants’ characteristics and changes in measures and laboratory data through means and standard deviations for continuous variables and frequencies and percentages for categorical ones. The normality of the data distributions was evaluated using the Shapiro-Wilk test. Within-subjects significant differences of study parameters (nutrition knowledge, number of meals eaten per day, number of out of home meals per week, stress score, sleep score, physical activity and laboratory values) were assessed using paired sample T-test, and Wilcoxon Signed Ranks Tests for normally distributed and skewed continuous variables, respectively.
Additionally, a between-subjects analysis of relevant study parameters (sub-group analysis) was conducted between participants who gained weight at T1 and those who did not use independent sample T-test for normally distributed continuous variables and Mann-Whitney U test for skewed ones. Finally, the agreement between reported and actual weight change was calculated according to Cohen (1968) [21] using the MedCalc statistical software (https://www.medcalc.org). Linear weighted Kappa (k) values and their 95% confidence intervals were presented, whereby k < 0.2, 0.21-0.40, 0.41-0.6, 0.61-0.80, 0.81-1.00 were interpreted as the poor, fair, moderate, good and very good strength of agreement respectively.
Results
Out of a total of 80 participants, 40 completed the study. As evident in table one, the students had a mean age of 19.3± 2.04 years and had a waist circumference of 83.16 ± 11.15 cm. On average, the participants consumed around 3 meals per day and ate approximately 5 meals out of home weekly. Their mean knowledge score was 50.14 ± 10.08 %, where 100% indicates perfect knowledge. Mean stress level was 19.28 out of a total possible 40 points and where a higher score indicates higher stress. Average sleep score was 6.55 where a score above five indicates poor sleep quality. Weekly alcohol consumption average was fairly low (0.18 ± 0.63).
More than half of the participants were females (55%), the majority were single (97.5%), and 90% lived with their parents. Approximately, 19.5% held jobs parallel to their studies and 32.5% smoked. The mean BMI of the participants was 23.74 ± 4.49 kg/m2, and around two-thirds (62.5%) had a normal BMI. Forty per cent of the participants had a moderately active lifestyle.
During the first year of university enrollment (throughout 2 semesters), the cohort gained on average 4.19 ± 8.67 Lbs. (1.90 ± 3.93 kg), and the mean BMI of the participants significantly increased from 23.95 ± 5.38 to 24.64 ± 5.38 kg/m2 (p = 0.002) as evident in table 2. The vast majority of the students (70%; n = 28) gained weight, and 40% of whom (n = 16) accumulated more than 5 lbs. (2.26 kg). Three students (7.5%) gained 15 lbs. (6.82 kg).
Table 1.
Baseline characteristics of freshman students (n = 80)
| N | % | |
|---|---|---|
| Gender, male | 36 | 45.0 |
| Social status, single | 78 | 97.5 |
| Live with family, yes | 72 | 90.0 |
| Employment, none | 62 | 80.5 |
| Smoker, yes | 26 | 32.5 |
| BMI category (kg/m²) | ||
| Underweight | 5 | 6.3 |
| Normal weight | 50 | 62.5 |
| Overweight | 18 | 22.5 |
| Obese | 7 | 8.8 |
| Physical activity level | ||
| Light activity | 30 | 37.5 |
| Moderate activity | 32 | 40.0 |
| High activity | 18 | 22.5 |
| Mean ± SD | ||
| Age (year) | 19.30 ± 2.04 | |
| Waist Circumference (WC) (cm) | 83.16 ± 11.15 | |
| Lifestyle Questionnaire | ||
| Number of meals per day | 2.84 ± 1.07 | |
| Number of out of home meals per week | 4.79 ± 3.82 | |
| Alcohol consumption (drinks per week) | 0.18±0.63 | |
| Nutrition knowledge (%) | 50.14 ± 10.08 | |
| Sleep score | 6.55 ± 3.11 | |
| Stress score | 19.28± 5.95 | |
| Biochemical tests | ||
| Fasting Blood Glucose ( FBG) (mg/dl) | 82.09 ±7.49 | |
| Total cholesterol (mg/dl) | 158.71 ±27.13 | |
| LDL cholesterol (mg/dl) | 93.76 ±27.91 | |
| HDL cholesterol (mg/dl) | 51.79 ±11.70 | |
| Triglycerides (mg/dl) | 76.93 ±31.76 | |
| Cortisol (nmol/L) | 533.12 ±192.38 | |
Data are expressed as mean ± SD. LDL: low-density lipoprotein, HDL: high-density lipoprotein; Sleep score above five indicates poor sleep quality.BMI: body mass index
Table 2.
Actual Weight change (n = 40)
| Weight change | N (%) | Mean± SD | Amount (Lbs.) | N (%) |
|---|---|---|---|---|
| Weight loss | 6 (15.0) | -7.16 ± 9.55 Lbs. | > 15 | 1 (2.5) |
| 5-15 | 1 (2.5) | |||
| <5 | 4 (10.0) | |||
| Stable | 6 (15.0) | 0 Lbs. | Stable (± 1) | 6 (15.0) |
| Weight gain | 28 (70.0) | +7.55 ± 6.87 Lbs. | < 5 | 12 (30.0) |
| 5 - 15 | 13 (32.5) | |||
| > 15 | 3 (7.5) |
Overall agreement between reported and measured weight change among the participants was fair (weighted Kappa = 0.21; 95% CI: 0.05 to 0.38). The discrepancy between actual and perceived weight gain was highest among two subgroups of students which were the ones who perceived they lost weight (yet 50% had gained weight) and the ones who perceived they had maintained weight (yet 71.4% had gained weight). The only subgroup of students who had perceived weight change which was by actual weight change were the ones who had reported weight gain (Figure 1).
Figure 1.
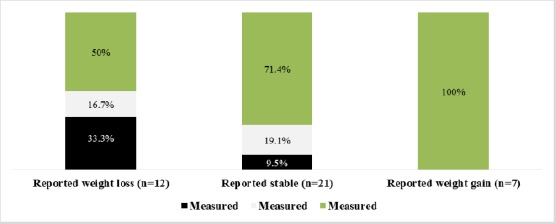
Weight change: Reported and actual
The effect of BMI on weight change in the first year of university is explained in Figure 2. The mean gain for all the 40 students was 4.2 ± 8.65lbs., whereby the underweight gained the most (7.2 lbs.), the normal and overweight participants gained approximately 5lbs., and the obese were the only subgroup who achieved weight loss during the 1st year of university enrollment.
Figure 2.
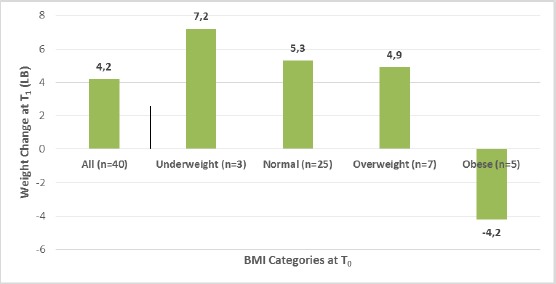
Effect of baseline BMI on Actual Weight Change
Lifestyle factors and, nutritional knowledge did not significantly change during the first year of university enrollment (Table 3). The absence of a pattern related to these characteristics was evident across the three weight change groups. No significant differences were noted between groups regarding the number of meals per day, the number of out of home meals consumed per week, nutrition knowledge (%), stress score, and sleep score.
Table 3.
Freshman students’ reported outcome measures and laboratory data
| Parameter (n = 40) | T0 | T1 | P value |
|---|---|---|---|
| Nutrition knowledge (%) | 49.48 ± 10.29 | 51.50 ± 10.82 | P = 0.25 |
| Number of meals eaten per day | 3.03 ± 1.09 | 2.73 ± 0.96 | P = 0.09 |
| Number of out of home meals per week | 5.11 ± 4.23 | 4.35 ± 6.74 | P = 0.06 |
| Stress score (max score: 40) | 19.33 ± 6.09 | 19.90 ± 4.89 | P = 0.64 |
| Sleep score (> 5 = poor sleep) | 6.05 ± 2.48 | 6.40 ± 3.19 | P = 0.73 |
| Physical activity (METs) per day | 1880.4 ± 2289.2 | 2148.59 ± 3078.61 | P = 0.62 |
| Laboratory values (n = 27) | T0 | T1 | P value |
| FBG (mg/dl) | 81.59 ± 6.29 | 85.30 ± 6.68 | P < 0.001* |
| Cortisol (nmol/L) | 527.9 ± 163.8 | 393.1 ± 133.9 | P = 0.003* |
| Triglycerides (mg/dl) | 71.44 ± 29.66 | 83.44 ± 36.10 | P = 0.02** |
| LDL (mg/dl) | 91.37 ± 27.32 | 84.19 ± 24.32 | P = 0.01* |
| HDL (mg/dl) | 54.33 ± 13.59 | 54.52 ± 13.273 | P = 0.85 |
| Cholesterol (mg/dl) | 159.37 ± 26.77 | 155.41 ± 24.46 | P = 0.15 |
METs: the metabolic equivalent of the task. FBG: fasting blood glucose; LDL: low-density lipoprotein, HDL: high-density lipoprotein. Data are expressed as mean ± SD. Statistically significantly difference: P<0.05
Paired Samples Test;
Wilcoxon Signed Ranks Test).
At last, all the objective study parameters were compared between T0 and T1 to detect changes over time. Results showed a significant increase in waist circumference in 40 students from 83.65 ± 12.7 cm to 86.9 ± 13.1 cm with p = 0.05. Additionally, as evident in Table 3, there was a significant increase in blood glucose and Triglyceride levels; on the other hand, there was a significant decrease in cortisol, and LDL. There were no significant changes in HDL cholesterol and total cholesterol between T0 and T1. Despite the changes, overall, all values were within normal limits. Furthermore, the results of the sub-analysis showed no statistically significant differences in all of the studied parameters between the weight gainers and non-weight gainers.
Discussion
This was the first study to longitudinally assess weight change during the freshman year among a sample of Lebanese university students. On average, the students gained 4.2 lbs. However there was considerable variability in weight change as 15% experienced no weight difference, 15% lost weight and 70% of the study participants put on weight. Health behaviours such as exercise, sleep, number of meals consumed and the total amount of meals eaten outside the home did not significantly differ between the first and second semester. Moreover, there were no significant changes in stress scores and nutrition knowledge throughout the study duration.
This study further supports evidence that first-year students do gain weight in the year of transition from high school to university. The changes in body weight are similar to previous literature as reported by Cooley and Turay [22], who found that students gained 4.4 pounds throughout 7 months and found no predictors for the weight gain [22]. Our results are also similar to those of Levitsky and colleagues [23] who concluded that their sample gained 4.4 lbs in 12 weeks but was also unable to determine the reasons for the weight changes [23].
There is, however, inconsistency in the literature about the average amount of weight that is typically gained during the freshman year as some studies have reported that the weight gain is typically lower than 5 lbs. For example, Vella Zarb & Elgar [13] found average weight gain to be approximately 2 lbs. (0.91 kg) whereas Butler and colleagues [24] found the increase to be 1.6 lbs. (0.72 kg). Speculation about the causes of the variability has been accounted to several factors which include the length of the study duration, intercountry variation and the socials lifestyle norms that come with them, study design and self-selection bias [8] [15] [25].
Additionally, the variation could be due to the method of how weight was reported, whether it was self-reported or measured by researchers. In the study conducted by Serlachius and colleagues [15], students gained approximately 3.4 lb (1.54 kg). However, the changes were self-reported which may have resulted in an underestimation of weight gain as students may not have realised that they had body mass [15] [25].
One potentially alarming finding in this study was the discrepancy between perceived and actual weight change, especially among weight gainers since 70% of those who gained weight were unaware of their increase. Misperception of weight status among overweight and obese adults has been associated with decreased attempts at weight loss [26], hence potentially exaggerating the obesity problem.
Many factors have been identified in the literature as possible determinants to weight gain during their freshman year which includes stress, leading a sedentary lifestyle, moving away from home and increased alcohol intake [8] [15] [27]. However, no association with any of the above factors as related to weight gain or loss was noticeable in the current study. Nutrition knowledge was very poor in our sample population at both times of data collection, and no relation with weight change was found. Nevertheless, this study did not have an educational component as participants were not exposed to any nutritional education within their curriculum that might have affected their knowledge scores or eating habits; which can explain the lack of association between these variables and weight change. Another possible explanation is that most individuals in the18-25 age category gain weight whether they attend college or not as this is a critical period, which has been named “emerging adulthood” and where individuals are at risk of gaining weight regardless of their circumstances [28].
Our results revealed that the obese lose weight. However, a sub-analysis of the data showed that only one of the students in this group had lost approximately 26 lbs and therefore skewed the results.
In parallel to the weight gain in the study participants, we also noted a significant increase in serum triglycerides, glucose and waist circumference. Although not clinically significant, the increases revealed a worsened metabolic profile which could potentially raise the risk of the future development metabolic syndrome [29]. As for the other biochemical markers, there was a significant decrease in cortisol and LDL levels. The unexpected decrease in cortisol level could be due to the intra-individual variability in cortisol response secondary to stress [30].
Our study presents numerous strengths. First, and to the best of the authors’ knowledge, this research pioneers assessment of weight changes of university students during the freshman year in a Middle Eastern country, by recruiting a sample from several Lebanese regions. The study was appropriately powered as mentioned in the methods. Additionally, weight gain was assessed objectively by trained researchers, in parallel to blood parameters, and validated questionnaires. Furthermore, the study had a sufficient duration to assess the effect throughout the whole academic year.
However, the present study also had some limitations. The sample used was a volunteer sample, and that could bias the results as students who were are not health conscious may have been reluctant to participate in this study. Moreover, although the sample was recruited from several geographical areas, the students were recruited from only one university, which hinders the generalizability of our findings. One additional limitation was the high attrition rate (50%), yet our analysis showed that participants who dropped out had similar baseline characteristics to those who completed the study; literature has shown that a low retention rate is common in such studies [8] [9]. Furthermore, the majority of the sample did not drink alcohol and lived at home; therefore these factors could not be appropriately analysed.
In conclusion, our results provide evidence that Lebanese students do gain weight during their freshman year which could be a potential public health problem, especially since Lebanon is a country experiencing a nutrition transition and increasing obesity rates.31 Future research should be conducted on a more representative sample and for or a longer duration to examine the predictors of weight gain. Additionally, public health interventions should be implemented by healthcare providers within universities, to raise awareness and prevent future weight gain.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.World Health Organization. World Health Organization obesity and overweight fact sheet. 2003 [Google Scholar]
- 2.Pierce EF, Butterworth SW, Lynn TD, O'Shea J, Hammer WG. Fitness profiles and activity patterns of entering college students. J Am Coll Health. 1992;41(2):59–62. doi: 10.1080/07448481.1992.10392819. https://doi.org/10.1080/07448481.1992.10392819 PMid:1460174. [DOI] [PubMed] [Google Scholar]
- 3.Craigie AM, Lake AA, Kelly SA, Adamson AJ, Mathers JC. Tracking of obesity-related behaviours from childhood to adulthood: A systematic review. Maturitas. 2011;70(3):266–284. doi: 10.1016/j.maturitas.2011.08.005. https://doi.org/10.1016/j.maturitas.2011.08.005 PMid:21920682. [DOI] [PubMed] [Google Scholar]
- 4.Guo SS, Wu W, Chumlea WC, Roche AF. Predicting overweight and obesity in adulthood from body mass index values in childhood and adolescence. The American journal of clinical nutrition. 2002;76(3):653–8. doi: 10.1093/ajcn/76.3.653. https://doi.org/10.1093/ajcn/76.3.653 PMid:12198014. [DOI] [PubMed] [Google Scholar]
- 5.American College Health Association. American college health association national college health assessment spring 2006 reference group data report (abridged) Journal of American College Health. 2007;55(4):195. doi: 10.3200/JACH.55.4.195-206. https://doi.org/10.3200/JACH.55.4.195-206 PMid:17319325. [DOI] [PubMed] [Google Scholar]
- 6.Steptoe A, Wardle J, Cui W, et al. Trends in smoking, diet, physical exercise, and attitudes toward health in European university students from 13 countries, 1990-2000. Preventive medicine. 2002;35(2):97–104. doi: 10.1006/pmed.2002.1048. https://doi.org/10.1006/pmed.2002.1048 PMid:12200093. [DOI] [PubMed] [Google Scholar]
- 7.Brown C. The information trail of the 'Freshman 15'—a systematic review of a health myth within the research and popular literature. Health Information & Libraries Journal. 2008;25(1):1–2. doi: 10.1111/j.1471-1842.2007.00762.x. https://doi.org/10.1111/j.1471-1842.2007.00762.x PMid:18251907. [DOI] [PubMed] [Google Scholar]
- 8.Vella-Zarb RA, Elgar FJ. The 'freshman 5': a meta-analysis of weight gain in the freshman year of college. Journal of American College Health. 2009;58(2):161–6. doi: 10.1080/07448480903221392. https://doi.org/10.1080/07448480903221392 PMid:19892653. [DOI] [PubMed] [Google Scholar]
- 9.Vadeboncoeur C, Townsend N, Foster C. A meta-analysis of weight gain in first year university students: is freshman 15 a myth? BMC Obesity. 2015;2(1):22. doi: 10.1186/s40608-015-0051-7. https://doi.org/10.1186/s40608-015-0051-7 PMid:26217537 PMCid: PMC4511069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Levitsky DA, Halbmaier CA, Mrdjenovic G. The freshman weight gain: a model for the study of the epidemic of obesity. International journal of obesity and related metabolic disorders: Journal of the International Association for the Study of Obesity. 2004;28(11):1435–1442. doi: 10.1038/sj.ijo.0802776. https://doi.org/10.1038/sj.ijo.0802776 PMid:15365585. [DOI] [PubMed] [Google Scholar]
- 11.Mihalopoulos NL, Auinger P, Klein JD. The Freshman 15: is it real? J Am Coll Health. 2008;56(5):531–533. doi: 10.3200/JACH.56.5.531-534. https://doi.org/10.3200/JACH.56.5.531-534 PMid:18400665 PMCid: PMC2532948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Girz L, Polivy J, Provencher V, et al. The four undergraduate years. Changes in weight, eating attitudes, and depression. Appetite. 2013;69:145–150. doi: 10.1016/j.appet.2013.06.002. https://doi.org/10.1016/j.appet.2013.06.002 PMid:23764239. [DOI] [PubMed] [Google Scholar]
- 13.Vella-Zarb RA, Elgar FJ. Predicting the 'freshman 15': Environmental and psychological predictors of weight gain in first-year university students. Health Education Journal. 2010;69(3):321–32. https://doi.org/10.1177/0017896910369416. [Google Scholar]
- 14.Economos CD, Hildebrandt ML, Hyatt RR. College freshman stress and weight change: differences by gender. American journal of health behavior. 2008;32(1):16–25. doi: 10.5555/ajhb.2008.32.1.16. https://doi.org/10.5993/AJHB.32.1.2 PMid:18021030. [DOI] [PubMed] [Google Scholar]
- 15.Serlachius A, Hamer M, Wardle J. Stress and weight change in university students in the United Kingdom. Physiology and Behavior. 2007;92(4):548–553. doi: 10.1016/j.physbeh.2007.04.032. https://doi.org/10.1016/j.physbeh.2007.04.032 PMid:17537466. [DOI] [PubMed] [Google Scholar]
- 16.van der Kooy K, Seidell JC. Techniques for the measurement of visceral fat: a practical guide. International journal of obesity and related metabolic disorders: journal of the International Association for the Study of Obesity. 1993;17(4):187–196. [PubMed] [Google Scholar]
- 17.Craig CL, Marshall AL, Sjostrom M, et al. International physical activity questionnaire:12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–1395. doi: 10.1249/01.MSS.0000078924.61453.FB. https://doi.org/10.1249/01.MSS.0000078924.61453.FB PMid:12900694. [DOI] [PubMed] [Google Scholar]
- 18.Parmenter K, Wardle J. Development of a general nutrition knowledge questionnaire for adults. Eur J Clin Nutr. 1999;53(4):298–308. doi: 10.1038/sj.ejcn.1600726. https://doi.org/10.1038/sj.ejcn.1600726 PMid:10334656. [DOI] [PubMed] [Google Scholar]
- 19.Buysse DJ, Reynolds CF, 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry research. 1989;28(2):193–213. doi: 10.1016/0165-1781(89)90047-4. https://doi.org/10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- 20.Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. Journal of health and social behavior. 1983;24(4):385–396. https://doi.org/10.2307/2136404 PMid:6668417. [PubMed] [Google Scholar]
- 21.Cohen J. Weighted kappa: nominal scale agreement with provision for scaled disagreement or partial credit. Psychological bulletin. 1968;70(4):213–220. doi: 10.1037/h0026256. https://doi.org/10.1037/h0026256 PMid:19673146. [DOI] [PubMed] [Google Scholar]
- 22.Cooley E, Toray T. Disordered eating in college freshman women: A prospective study. Journal of American College Health. 2001;49(5):229–35. doi: 10.1080/07448480109596308. https://doi.org/10.1080/07448480109596308 PMid:11337898. [DOI] [PubMed] [Google Scholar]
- 23.Levitsky DA, Garay J, Nausbaum M, Neighbors L, Dellavalle DM. Monitoring weight daily blocks the freshman weight gain: a model for combating the epidemic of obesity. International journal of obesity. 2006;30(6):1003. doi: 10.1038/sj.ijo.0803221. https://doi.org/10.1038/sj.ijo.0803221 PMid:16446748. [DOI] [PubMed] [Google Scholar]
- 24.Butler SM, Black DR, Blue CL, Gretebeck RJ. Change in diet, physical activity, and body weight in female college freshman. American journal of health behavior. 2004;28(1):24–32. doi: 10.5993/ajhb.28.1.3. https://doi.org/10.5993/AJHB.28.1.3 PMid:14977156. [DOI] [PubMed] [Google Scholar]
- 25.Fedewa MV, Das BM, Evans EM, Dishman RK. Change in weight and adiposity in college students: a systematic review and meta-analysis. Am J Prev Med. 2014;47(5):641–652. doi: 10.1016/j.amepre.2014.07.035. https://doi.org/10.1016/j.amepre.2014.07.035 PMid:25241201. [DOI] [PubMed] [Google Scholar]
- 26.Duncan DT, Wolin KY, Scharoun-Lee M, Ding EL, Warner ET, Bennett GG. Does perception equal reality?Weight misperception in relation to weight-related attitudes and behaviors among overweight and obese US adults. International Journal of Behavioral Nutrition and Physical Activity. 2011;8(1):20. doi: 10.1186/1479-5868-8-20. https://doi.org/10.1186/1479-5868-8-20 PMid:21426567 PMCid: PMC3073863. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.de Vos P, Hanck C, Neisingh M, Prak D, Groen H, Faas MM. Weight gain in freshman college students and perceived health. Preventive medicine reports. 2015;2:229–234. doi: 10.1016/j.pmedr.2015.03.008. https://doi.org/10.1016/j.pmedr.2015.03.008 PMid:26844076 PMCid: PMC4721347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Nelson MC, Story M, Larson NI, Neumark-Sztainer D, Lytle LA. Emerging Adulthood and College-aged Youth: An Overlooked Age for Weight-related Behavior Change. Obesity. 2008;16(10):2205–2211. doi: 10.1038/oby.2008.365. https://doi.org/10.1038/oby.2008.365 PMid:18719665. [DOI] [PubMed] [Google Scholar]
- 29.Grundy SM. Overnutrition, ectopic lipid and the metabolic syndrome. Journal of Investigative Medicine. 2016 doi: 10.1136/jim-2016-000155. https://doi.org/10.1136/jim-2016-000155 PMid:27194746. [DOI] [PubMed] [Google Scholar]
- 30.van Eck MM, Nicolson NA, Berkhof H, Sulon J. Individual differences in cortisol responses to a laboratory speech task and their relationship to responses to stressful daily events. Biological psychology. 1996;43(1):69–84. doi: 10.1016/0301-0511(95)05159-7. https://doi.org/10.1016/0301-0511(95)05159-7. [DOI] [PubMed] [Google Scholar]
- 31.Nasreddine L, Naja F, Chamieh MC, Adra N, Sibai A-M, Hwalla N. Trends in overweight and obesity in Lebanon: evidence from two national cross-sectional surveys (1997 and 2009) BMC Public Health. 2012;12(1):798. doi: 10.1186/1471-2458-12-798. https://doi.org/10.1186/1471-2458-12-798 PMid:22984791 PMCid: PMC3527186. [DOI] [PMC free article] [PubMed] [Google Scholar]