

Abstract
BACKGROUND:
The pathogenesis of inflammatory neuronal cell damage will continue after traumatic brain injury in which contributed to subsequent mortality. Serum S100B levels were shown to be an early predictor of mortality due to traumatic brain injury.
AIM:
This Meta-Analysis will analyse the mean and diagnostic strength of serum S100B levels between survived and died subjects with head injuries based on the various follow-up times of nine studies.
METHODS:
We conducted a meta-anelysis in accordance with PRISMA guidelines and adhering to Cochrane Handbook for Systematic Review of Interventions. Literature search was conducted on March 16, 2018 from Medline and Scopus in the past 10 years, using various keywords related to S100, brain injury, and outcome. Duplicate journals were sorted out via EndNote. Included articles were as follows: original data from the group, clinical trials, case series, patients undergoing serum S100B levels with both short- and long-term follow-up mortality. Data were collected for mortality, serum S100B levels, and its diagnostic strength. All data were analyzed using Review Manager 5.3 (Cochrane, Denmark).
RESULTS:
The results of the meta-analysis showed a significant difference in S100B levels between survived and died subjects with head injuries on overall follow-up timeline (0.91, 95.9% CI 0.7-1.12, I2 = 98%, p < 0.001), during treatment (1.43, 95% CI 0.97 to 1.89, I2 = 98%, p < 0.001), or 6 months (0.19; 95%CI 0.1-0.29, I2 = 76%, p < 0.001) with an average threshold value that varies according to the study method used. The mean diagnostic strength was also promising to predict early mortality (sensitivity of 77.18% and 92.33%, specificity of 78.35% and 50.6%, respectively).
CONCLUSION:
S100B serum levels in the future will be potential biomarkers, and it is expected that there will be standardised guidelines for their application.
Keywords: Traumatic brain injury, S100B serum level, Mortality
Introduction
Traumatic brain injury is a trauma that causes abnormal functioning of the brain due to impact or blows to the head. Every year, millions of people enter the ED due to head injuries, and 1.5 million of them die [1]. In Sanglah General Hospital in Denpasar, the incidence of annual head injuries averages over 2000 cases, of which 30% are moderate and severe traumatic brain injury patients [2]. Many deaths that occur before the patient arrives at the hospital or during the period of treatment [3]. However, continued inflammatory processes in secondary traumatic brain injury [4] cause molecular cell damage, changes in metabolism and cerebral blood flow, axonal disruption, and apoptosis which contribute to long-term mortality [5]. Predictors of traumatic brain injury mortality such as low Glasgow coma scores, unresponsive pupillary reactions, and hemodynamic disorders [6] are not quantitative and specific so biomarkers are needed to predict mortality in traumatic brain injury [7]. Among potential new biomarkers, S100B has high specificity for neural networks associated with mortality and a prognosis that does not benefit [8].
S100B is released after brain injury and released more as a structural factor (at high concentrations) and repair (at low concentrations), so it will be very useful in the diagnosis of traumatic brain injury [9]. The S100B ability as a predictor of traumatic brain injury mortality has been shown in studies, [10] [11] [12] some of these studies oppose these results [13]. Different results can be due to methodological differences, sample size, non-standardized tests, and different subject demographics. To further deepen the usefulness of serum S100B levels as a predictor of traumatic brain injury mortality, this meta-analysis will present an analysis of several studies both S100B as a predictor of initial and later mortality.
This study aims to analyse the difference in mean serum S100B levels between patients who died or survived traumatic brain injury based on follow-up time.
Methods
This study presents a meta-analysis of the role of serum S100B as a predictor of mortality in traumatic brain injury. The study design follows the PRISMA guidelines for meta-analysis [13]. The steps follow the Cochrane Handbook for Systematic Review of Interventions [14] guidelines.
A comprehensive literature search was conducted by the author on March 16, 2018. Relevant studies were obtained from Medline (2008-2018) and SCOPUS (2008-2018) in the last 10 years. References from all studies are further reviewed to identify additional relevant research. The author uses a search strategy with (((((((((S100B) OR S100) OR S-100) OR S-100B) OR S100β) OR S-100β) AND ((MORTALITY) OR OUTCOME) AND (BRAIN INJURY)) AND “last 10 years” [PDat]).
Duplicate journals are managed using EndNote. The title and abstract of the search results are reviewed, and the full text is analysed for inclusion in this meta-analysis. All articles are assessed using the inclusion and exclusion criteria determined by the author. The articles are included if they contain original data from the group, clinical trials, case series, patients undergoing serum S100B levels with both short and long-term follow-up mortality. Only English language journals and full text are included in this study. Data extracted from the study included using data extraction forms. The scope of data collection is about the place of study, method, number of mortality, serum S100B levels, and the diagnostic strength of serum S100B levels. The primary parameter of this study was the difference in S100B levels in patients who died and living head injuries. Secondary parameters are the diagnostic strength of serum S100B levels.
This meta-analysis will calculate the difference in mean serum S100B levels in subjects who died and lived head injuries with follow-up during treatment, 24 hours, 3 months, 6 months, and 1 year. Data were analysed by Review Manager 5.3 (Cochrane Collaboration, Copenhagen, Denmark) and the significance limit was 0.05.
Results
The study results yielded 9 studies to be analysed [10] [12] [13] [16] [17] [18] [19] [20] [21] (Table 1) which can be included in the study. The article searching process was carried out based on the PRISMA principle (Figure 1). In this meta-analysis, we will assess the difference in S100B levels in survived and dead subjects with traumatic brain injury. Also, the diagnostic strength of serum S100B levels will also be explained.
Table 1.
Studies included in this meta-analysis based on follow up time
| Study, year | Country | Methods | Time of follow up | Mortality | Mean value of S100B |
|---|---|---|---|---|---|
| During hospital stay | |||||
| Rodriguez et al., 201216 | Finland | ECLIA | Inpatient | 10/55 | S: 0.3 ± 0.2 ug/L |
| D: 1.7 ± 1.2 ug/L | |||||
| C: 0,461 ug/L | |||||
| AUC: 0,958 | |||||
| Sens: 90% | |||||
| Spe: 88,4% | |||||
| Shakeri et al., 201513 | Iran | ELISA | Inpatient | 30/72 | S: 1.04 ± 0.5 ug/mL D: 2.36 ± 0.94 ug/mL (p<0.001) |
| Pfortmueller et al., 201610 | Austria | ELISA | Inpatient | 52/1367 | D: 8.2 ± 3.5 ug/L |
| S: 2.2 ± 0.8 ug/L | |||||
| (p < 0.001) | |||||
| C: 2 ug/L | |||||
| Rodriguez et al., 201617 | Finland | ECLIA | Inpatient | 15/99 | S: 0.09 ± 0.03 ug/L |
| D: 0.36 ± 0.2 ug/L | |||||
| C: 0.2 ug/L | |||||
| (p = 0.003) | |||||
| AUC: 0.848 | |||||
| Sens: 86,7% | |||||
| Spe: 75% | |||||
| Duda et al., 201718 | Polandia | ELISA | Inpatient | 22/62 | S: 0.08 ± 0.03 ug/L |
| D: 0.6 ± 0.04 ug/L | |||||
| C: 0.12 ug/L | |||||
| Sens: 50% | |||||
| Spe: 90% | |||||
| 11/22 showed S100B higher than 0.12 ug/L | |||||
| 24 Hours | |||||
| Rainey et al., 200912 | UK | ELISA | 24 hours | 30/100 | S: 0.59 ± 0.23 ug/L |
| D: 1.44 ± 0.84 ug/L | |||||
| C: 0.53 ug/L | |||||
| AUC: 0.69 | |||||
| Sens: 82% | |||||
| Spe: 60% | |||||
| 3 Months | |||||
| Olivecrona et al., 200919 | Swedia | LIA | 3 months | 6/48 | S: 0,6 ± 0,2 ug/L |
| D: 2,38 ± 0,8 ug/L | |||||
| AUC: 0,687 | |||||
| Sens: 100% | |||||
| Spe: 38,1% | |||||
| C: 0.51 ug/L | |||||
| 6 Months | |||||
| Ballesteros et al., 201820 | Spain | ECLIA | 6 months | 46/83 | S: 0.15 ± 0.05 ug/L |
| D: 0.3 ± 0.15 ug/L | |||||
| AUC: 0.739 | |||||
| Rodriguez et al., 201617 | Finland | ECLIA | 6 months | 19/99 | S: 0.09 ± 0.03 ug/L |
| D: 0.28 ± 0.12 ug/L | |||||
| (p=0.002) | |||||
| C: 0.177 ug/L | |||||
| AUC: 0.855 | |||||
| Sens: 89.5% | |||||
| Spe: 76.2% | |||||
| Gradisek et al., 201221 | Slovenia | ELISA | 1 year | 26/73 | S: 0.77 ± 0.6 ug/L |
| D: 1.565 ± 1.1 ug/L ug/L(p<0.001) | |||||
| 1 Year | |||||
| Olivecrona et al., 200919 | Swedia | LIA | 1 year | 8/48 | S: 0.8 ± 0.3 ug/L |
| D: 3 ± 1.2 ug/L | |||||
| AUC: 0.647 | |||||
| Sens: 87.5% | |||||
| Spe: 37.5% | |||||
| C: 0.51 ug/L | |||||
S: Survived, D: Died, AUC: Area Under Curve: Sens: Sensitivity, Spe: Specificity, C: Cut off.
Figure 1.
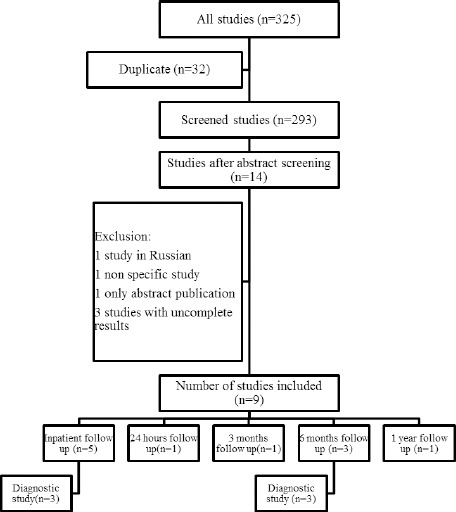
Flowchart PRISMA showed journal method of selection
Differences in serum S100B levels between survived and dead subjects based on follow-up time.
Overall, from the meta-analysis of the 11 studies, the mean difference calculated from random effects showed significant results (p < 0.001).
The total mean difference of serum S100B level before and after traumatic brain injury was significant statistically (0.91; 95%CI 0.7-1.12, I2 = 98%, p < 0.001; Figure 2a). If classified based on the length of follow-up time until, during treatment, there were 5 studies reviewed. From the meta-analysis of the five studies, the random effects mean difference showed significant results (p < 0.001). The total mean difference was 1.43 (95% CI 0.97-1.89, I2 = 98%, p < 0.001; Figure 2b). For up to 5 months of follow-up, from the three studies, the random effects mean difference also showed significant results (p < 0.001). The total mean difference was 0.19 (95% CI 0.1-0.29, I2 = 76%, p < 0.001; Figure 2c). In the study with a follow-up period of 24 hours, 3 months, and 1 year, there was only 1 study in each study (Table 1).
Figure 2.

Forest plot difference of S100B serum levels in survived and died subjects based on follow up the timeline (a) overall, (b) within treatment, (c) 6 months
The diagnostic strength of serum S100B levels in predicting early and late mortalities in subjects with a head injury
In this study, early mortality biomarkers were determined in samples which were taken during treatment or in the first 24 hours. The mean sensitivity of the four studies showed that the threshold value of S100B in the predicting short-term mortality was 0.328 ± 0.198 μg/L. The mean sensitivity was 77.18 ± 18.41%, and specificity was 78.35 ± 13.96%. Of the five studies, only three reported the results of AUC, with the mean AUC obtained from the four studies was 0.832 ± 0.134.
In this study, the final mortality predictions were taken with a follow-up period of more than 1 month. The mean sensitivity of the four studies showed that the threshold value of S100B in the prediction of short-term mortality was 0.399 ± 0.19 μg/L. The mean sensitivity was 92.33 ± 6.71%, and specificity was 50.6 ± 22.17%. Of the four studies, only three reported the results of AUC, so that the mean AUC obtained from the four studies was 0.732 ± 0.09.
From the graph plotted regarding the S100B threshold value that predicts mortality during long-term care and mortality in 3-6 months, it was shown that the median value of the graph was approximately 0.5 μg/L (Figure 3).
Figure 3.
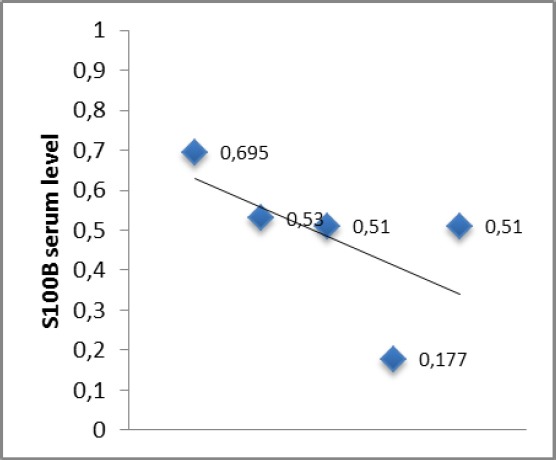
Cut off point of S100B serum levels which were taken during a hospital stay, 24 hours, 1 month, 3 months, 6 months, and 1 year
Discussion
Mortality rates due to TBI vary in several studies. Some studies also use different time methods and parameters to analyse this mortality. The fatality rate for TBI ranges from 13-22% [22]. After primary traumatic brain injury, secondary traumatic brain injury will continue in a few minutes, days, months, and years after primary traumatic brain injury due to excess metabolic, cellular and molecular inflammation activity [23].
S100 is a small dimeric cytosolic protein, 9-21 kDa, in the form of a homodimer with solubility in 100% ammonium sulfate liquid with a helical-loop-helical calcium bond [24]. S100B gene can be mapped on the long arm of chromosome 21q22.3. The S100B level is generally stable, not affected by storage, centrifugation, and temperature changes which will greatly facilitate sampling and reliability techniques in the analysis [25].
In TBI, S100B can be secreted into the systemic circulation along with the blood-brain barrier [26]. In the initial TBI phase, S100B is secreted as a TBI compensator with the effects of neurotrophic agents which have neuromodulating action and support the memory and thinking process [27]. In the final phase, where inflammation has been very high, and the blood-brain barrier has been disrupted, S100B acts as a destructor of neurons due to stimulation of proinflammatory cytokines and free radical activity which is often found in the pathophysiology of neurodegenerative disorders [28].
S100B as a TBI biomarker was first put forward in 1995 [29] where high S100B concentrations can be a primary and secondary TBI biomarker [30]. Researchers also found that this biomarker can be a TBI severity stratification based on GCS [31]. The ability of S100B in TBI output prediction has made some The researchers concluded that this biomarker was available as a predictor of TBI early and late diagnosis and mortality. From this meta-analysis, it was shown that high level of S100B was significantly different in the survive or died subjects with head injuries. The strength of short-term mortality predictors is also better than long-term mortality both from the significance of mean differences and diagnostic strength.
In another study, Unden in 33 patients (13%) showed that S100B could predict adverse outcomes (p = 0.03) but not mortality (p = 0.182) [32]. Shakeri et al., (2013) opposed the results that the level of S-100B could not be a predictor of mortality. The differences were due to variations in the time of collection of S100B in each study, ranging from the time of trauma to 84 hours after trauma. Research also takes heterogeneous long-term results between 1 month to several years so that the results of the study are also varied [13].
The weakness of this meta-analysis was not separating research based on varied sampling times. The optimal time for S100B sampling is still a warm discussion. Existing studies show different retrieval times [8]. In some studies, it was shown that the earlier sample was better [33]. However, some showed that the sample after 6 hours was better [34]. Some suggested 6-12 hours [3], 12 hour [35], 24 hours [36], 48 hours [37], 72 hours [11], and 84 hours [38].
The threshold value of serum S100B is still controversial. The wide range is shown by several studies. In this meta-analysis, the threshold value of S100B varies greatly depending on the method used. Although, the graph showed that the value is around 0.5 μg/L. Meta-analysis of Mercier et al., [8] on 39 studies in 1862 patients showed that serum S100B levels between 2.16-14.0 μg/L were effective for predicting adverse outcomes and mortality. Recently, a study of 3,893 patients showed a higher threshold value of 0.16-0.20 μg/L with a specificity of 51% for detecting intracranial abnormalities [11]. However, other clinicians stated that the threshold value lower than 0.1 μg/l was better for preventing false-negative cases, especially in epidural hematomas which usually indicate low S100B levels [16]. Unden et al., [32] did not find EDH subjects with S100B serum level higher than 0.14 μg/l [31]. Wolf et al., [39] have shown that the threshold value of S100B, 0.1 μg/l was found to be effective for detecting epidural hematoma at the initial presentation.
Giving the above results, it can be concluded that S100B serum level is very potential in predicting mortality due to traumatic brain injury. For further research, S100B biomarkers could be analysed in salivary and urine, which are useful as diagnostic markers. Urine and saliva samples could be obtained noninvasively so that they have the potential to be applied.
In conclusion, there is a significant difference in the mean serum S100B levels between patients who survived and died after traumatic brain injury. The diagnostic strength of serum S100B levels is promising in predicting mortality with a range of threshold values that vary according to the examination method used. S100B levels in the future will be a future potential biomarker, and it is expected that there will be a standardised guideline for its application.
Footnotes
Funding: This research did not receive any financial support
Competing Interests: The authors have declared that no competing interests exist
References
- 1.Marr AL, Coronado VG. Central nervous system injury surveillance data submission standards—2002. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control; 2004. [Google Scholar]
- 2.Medical records derived from Sanglah Hospital. Sanglah Hospital. 2011 [Google Scholar]
- 3.Pentland B, Hutton LS, Jones PA. Late mortality after traumatic brain injury. J Neurol Neurosurg Psychiatry. 2005;76:395–400. doi: 10.1136/jnnp.2004.037861. https://doi.org/10.1136/jnnp.2004.037861 PMid:15716535 PMCid: PMC1739527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bloomfield SM, McKinney J, Smith L, et al. Reliability of S100Βin predicting the severity of central nervous system injury. Neurocrit Care. 2007;6:121–38. doi: 10.1007/s12028-007-0008-x. https://doi.org/10.1007/s12028-007-0008-x PMid:17522796. [DOI] [PubMed] [Google Scholar]
- 5.Lafrenaye AD, Krahe TE, Povlishock JT. Moderately elevated intracranial pressure after diffuse traumatic brain injury is associated with exacerbated neuronal pathology and behavioural morbidity in the rat. J Cereb Blood Flow Metab. 2014;34(10):1628–36. doi: 10.1038/jcbfm.2014.122. https://doi.org/10.1038/jcbfm.2014.122 PMid:25027309 PMCid: PMC4269720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Van Beek JG, Mushkudiani NA, Steyerberg EW, Butcher I, McHugh GS, Lu J, Marmarou A, Murray GD, Maas AI. Prognostic value of admission laboratory parameters in traumatic brain injury: results from the IMPACT study. Journal of Neurotrauma. 2007;24(2):315–28. doi: 10.1089/neu.2006.0034. https://doi.org/10.1089/neu.2006.0034 PMid:17375996. [DOI] [PubMed] [Google Scholar]
- 7.Adrian H, Marten K, Salla N, Lasse V. Biomarkers of traumatic brain injury: temporal changes in body fluids. eNeuro. 2016;3(6):294–9. doi: 10.1523/ENEURO.0294-16.2016. https://doi.org/10.1523/ENEURO.0294-16.2016 PMid:28032118 PMCid: PMC5175263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mercier E, Boutin A, Lauzier F, Fergusson DA, Simard JF, Zarychanski R, et al. Predictive value of S-100beta protein for prognosis in patients with moderate and severe traumatic brain injury: systematic review and meta-analysis. BMJ. 2013;346:1757–9. doi: 10.1136/bmj.f1757. https://doi.org/10.1136/bmj.f1757 PMid:23558282. [DOI] [PubMed] [Google Scholar]
- 9.Donato R. S100: a multigenic family of calcium-modulated proteins of the EF-hand type with intracellular and extracellular functional roles. Int J Biochem Cell Biol. 2001;33:637–68. doi: 10.1016/s1357-2725(01)00046-2. https://doi.org/10.1016/S1357-2725(01)00046-2. [DOI] [PubMed] [Google Scholar]
- 10.Pfortmueller CA, Drexel C, Krahenmann-Muller S, Leichtle AB, Fiedler GM, Lindner G, et al. S-100 B Concentrations Are a Predictor of Decreased Survival in Patients with Major Trauma, Independently of Traumatic brain injury. PloS One. 2016;11(3):1–5. doi: 10.1371/journal.pone.0152822. https://doi.org/10.1371/journal.pone.0152822 PMid:27031106 PMCid: PMC4816449. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Murillo-Cabezas F, Mu-oz-Sánchez MA, Rincón-Ferrari MD, et al. The prognostic alue of the temporal course of S100B eta protein in the post-acute severe brain injury: a prospective and observational study. Brain Inj. 2010;24:609–19. doi: 10.3109/02699051003652823. https://doi.org/10.3109/02699051003652823 PMid:20235763. [DOI] [PubMed] [Google Scholar]
- 12.Rainey T, Lesko M, Sacho R, Lecky F, Childs C. Predicting outcome after severe traumatic brain injury using the serum S100B biomarker: results using a single (24 h) time-point. Resuscitation. 2009;80:341–5. doi: 10.1016/j.resuscitation.2008.11.021. https://doi.org/10.1016/j.resuscitation.2008.11.021 PMid:19150161. [DOI] [PubMed] [Google Scholar]
- 13.Shakeri M, Mahdkhah A, Panahi F. S100B Protein as a Post-traumatic Biomarker for Prediction of Brain Death in Association With Patient Outcomes. Arch Trauma Res. 2013;2:76–80. doi: 10.5812/atr.8549. https://doi.org/10.5812/atr.8549 PMid:24396798 PMCid: PMC3876553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ. 2009;339:b2700.12. doi: 10.1136/bmj.b2700. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.00. The Cochrane Collaboration. 2008. [(accessed 28 January 2010). 2008]. Available from www.cochrane-handbook.org .
- 16.Rodríguez-Rodríguez A, Egea-Guerrero JJ, Gordillo-Escobar E, Enamorado-Enamorado J, Hernández-García C, Ruiz de Azúa-López Z, Vilches-Arenas Á, Guerrero JM, Murillo-Cabezas F. S100B and Neuron-Specific Enolase as mortality predictors in patients with severe traumatic brain injury. Neurol Res. 2016;38(2):130–7. doi: 10.1080/01616412.2016.1144410. https://doi.org/10.1080/01616412.2016.1144410 PMid:27078699. [DOI] [PubMed] [Google Scholar]
- 17.Rodríguez-Rodríguez A, Egea-Guerrero JJ, León-Justel A, Gordillo-Escobar E, Revuelto-Rey J, Vilches-Arenas A, Carrillo-Vico A, Domínguez-Roldán JM, Murillo-Cabezas F, Guerrero JM. Role of S100B protein in urine and serum as an early predictor of mortality after severe traumatic brain injury in adults. Clin Chim Acta. 2012;414:228–33. doi: 10.1016/j.cca.2012.09.025. https://doi.org/10.1016/j.cca.2012.09.025 PMid:23031665. [DOI] [PubMed] [Google Scholar]
- 18.Duda I, Krzych L, Jędrzejowska-Szypułka H, Lewin-Kowalik JL. Serum levels of the S100B protein and neuron-specific enolase are associated with mortality in critically ill patients. Biochimica Polonica. 2017;64:16–9. doi: 10.18388/abp.2017_1619. https://doi.org/10.18388/abp.2017_1619. [DOI] [PubMed] [Google Scholar]
- 19.Olivecrona M, Rodling-Wahlström M, Naredi S, Koskinen LO. S-100B and neuron specific enolase are poor outcome predictors in severe traumatic brain injury treated by an intracranial pressure targeted therapy. J Neurol Neurosurg Psychiatry. 2009;80(11):1241–7. doi: 10.1136/jnnp.2008.158196. https://doi.org/10.1136/jnnp.2008.158196 PMid:19602473. [DOI] [PubMed] [Google Scholar]
- 20.Ballesteros MA, Rubio-Lopez MI, San Martín M, Padilla A, López-Hoyos M, Llorca J, Mi-ambres E. Serum levels of S100B from jugular bulb as a biomarker of poor prognosis in patients with severe acute brain injury. J Neurol Sci. 2018;385:109–14. doi: 10.1016/j.jns.2017.12.017. https://doi.org/10.1016/j.jns.2017.12.017 PMid:29406887. [DOI] [PubMed] [Google Scholar]
- 21.Gradisek P, Osredkar J, Korsic M, Kremzar B. Multiple indicators model of long-term mortality in traumatic brain injury. Brain Inj. 2012;26(12):1472–81. doi: 10.3109/02699052.2012.694567. https://doi.org/10.3109/02699052.2012.694567 PMid:22721420. [DOI] [PubMed] [Google Scholar]
- 22.Gerber LM, Chiu YL, Carney N, Hartl R, Ghajar J. Marked reduction in mortality in patients with severe traumatic brain injury. J Neurosurg. 2013;119:1583–90. doi: 10.3171/2013.8.JNS13276. https://doi.org/10.3171/2013.8.JNS13276 PMid:24098983. [DOI] [PubMed] [Google Scholar]
- 23.Korfias S, Stranjalis G, Boviatsis E, et al. Serum S-100B protein monitoring in patients with severe traumatic brain injury. Intensive Care Med. 2007;33:255–60. doi: 10.1007/s00134-006-0463-4. https://doi.org/10.1007/s00134-006-0463-4 PMid:17143637. [DOI] [PubMed] [Google Scholar]
- 24.Raabe A, Grolms C, Sorge O, Zimmermann M, Seifert V. Serum S-100B protein in severe traumatic brain injury. Neurosurgery. 1999;45(3):477–83. doi: 10.1097/00006123-199909000-00012. https://doi.org/10.1097/00006123-199909000-00012 PMid:10493369. [DOI] [PubMed] [Google Scholar]
- 25.Goyal A, Failla MD, Niyonkuru C, Amin K, Fabio A, Berger RP, Wagner AK. S100b as a Prognostic Biomarker in Outcome Prediction for Patients with Severe Traumatic Brain Injury. J Neurotrauma. 2013;30(11):946–57. doi: 10.1089/neu.2012.2579. https://doi.org/10.1089/neu.2012.2579 PMid:23190274 PMCid: PMC3684103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Anderson RE, Hansson LO, Liska J, Settergren G, Vaage J. The effect of cardiotomy suction on the brain injury marker S100B after cardiopulmonary by-pass. Ann Thorac Surg. 2000;69:847–50. doi: 10.1016/s0003-4975(99)01526-x. https://doi.org/10.1016/S0003-4975(99)01526-X. [DOI] [PubMed] [Google Scholar]
- 27.Nishiyama H, Knopfel T, Endo S, Itohara S. Glial protein S100B modulates long-term neuronal synaptic plasticity. Proc Natl Acad Sci USA. 2002;99:4037–42. doi: 10.1073/pnas.052020999. https://doi.org/10.1073/pnas.052020999 PMid:11891290 PMCid: PMC122644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Herrmann M, Jost S, Kutz S, Ebert AD, Kratz T, Wunderlich MT, Synowitz H. Temporal profile of release of neurobiochemical markers of brain damage after traumatic brain injury is associated with intracranial pathology as demonstrated in cranial computerized tomography. J Neurotrauma. 2000;17:113–22. doi: 10.1089/neu.2000.17.113. https://doi.org/10.1089/neu.2000.17.113 PMid:10709869. [DOI] [PubMed] [Google Scholar]
- 29.Ingebrigtsen T, Romner B, Kongstad P, Langbakk B. Increased serum concentrations of protein S-100 after minor traumatic brain injury: a biochemical serum marker with prognostic value? J Neurol Neurosurg Psychiatry. 1995;59:103–4. doi: 10.1136/jnnp.59.1.103-a. https://doi.org/10.1136/jnnp.59.1.103-a PMid:7608699 PMCid: PMC1073618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.de Kruijk JR, Leffers JR, Menheere PP, Meerhoff S, Twijnstra A. S100B and neuron-specific enolase in serum of mild traumatic brain injury patients. A comparison with healthy controls. Acta Neurol Scand. 2001;103:175–9. doi: 10.1034/j.1600-0404.2001.103003175.x. https://doi.org/10.1034/j.1600-0404.2001.103003175.x PMid:11240565. [DOI] [PubMed] [Google Scholar]
- 31.Kellermann I, Kleindienst A, Hore N, Buchfelder M, Brandner S. Early CSF and Serum S100B Concentrations for Outcome Prediction in Traumatic Brain Injury and Subarachnoid Hemorrhage. Clin Neurol Neurosurg. 2016;145:79–83. doi: 10.1016/j.clineuro.2016.04.005. https://doi.org/10.1016/j.clineuro.2016.04.005 PMid:27101088. [DOI] [PubMed] [Google Scholar]
- 32.Unden J, Bellner J, Astrand R, Romner B. Serum S100B levels in patients with epidural haematomas. Br J Neurosurg. 2005;19:43–45. doi: 10.1080/02688690500089381. https://doi.org/10.1080/02688690500089381 PMid:16147582. [DOI] [PubMed] [Google Scholar]
- 33.Schültke E, Sadanand V, Kelly ME, Griebel RW, Juurlink BHJ. Can admission S-100B predict the extent of brain damage in head trauma patients? Can J Neurol Sci. 2009;36:612–6. doi: 10.1017/s031716710000812x. https://doi.org/10.1017/S031716710000812X PMid:19831131. [DOI] [PubMed] [Google Scholar]
- 34.Woertgen C, Rothoerl RD, Brawanski A. Early S-100B serum level correlates to quality of life in patients after severe traumatic brain injury. Brain Inj. 2002;16:807–16. doi: 10.1080/02699050210128933. https://doi.org/10.1080/02699050210128933 PMid:12217206. [DOI] [PubMed] [Google Scholar]
- 35.Muller K, Townend W, Biasca N, Unden J, Waterloo K, Romner B, Ingebrigtsen T. S100B serum level predicts computed tomography findings after minor traumatic brain injury. J Trauma. 2007;62:1452–56. doi: 10.1097/TA.0b013e318047bfaa. https://doi.org/10.1097/TA.0b013e318047bfaa PMid:17563665. [DOI] [PubMed] [Google Scholar]
- 36.Murray GD, Butcher I, McHugh GS, Lu J, Mushkudiani NA, Maas AI, Marmarou A, Steyerberg EW. Multivariable prognostic analysis in traumatic brain injury: results from the IMPACT study. J Neurotrauma. 2007;24:329–37. doi: 10.1089/neu.2006.0035. https://doi.org/10.1089/neu.2006.0035 PMid:17375997. [DOI] [PubMed] [Google Scholar]
- 37.Thelin EP, Jeppsson E, Frostell A, Svensson M, Mondello S, Bellander BM, Nelson DW. Utility of neuron-specific enolase in traumatic brain injury;relations to S100B levels, outcome, and extracranial injury severity. Crit Care. 2016;20:285. doi: 10.1186/s13054-016-1450-y. https://doi.org/10.1186/s13054-016-1450-y PMid:27604350 PMCid: PMC5015335. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Pelinka LE, Toegel E, Mauritz W, Redl H. Serum S 100 B: a marker of brain damage in traumatic brain injury with and without multiple trauma. Shock. 2003;19:195–200. doi: 10.1097/00024382-200303000-00001. https://doi.org/10.1097/00024382-200303000-00001 PMid:12630517. [DOI] [PubMed] [Google Scholar]
- 39.Wolf H, Frantal S, Pajenda G, Leitgeb J, Sarahrudi K, Hajdu S. Analysis of S100 calcium binding protein B serum levels in different types of traumatic intracranial lesions. J Neurotrauma. 2015;32:23–27. doi: 10.1089/neu.2013.3202. https://doi.org/10.1089/neu.2013.3202 PMid:25068442. [DOI] [PubMed] [Google Scholar]