

Abstract
Purpose
The incidence of paediatric fractures is known to peak during the summer as a consequence of unsupervised physical activity. A more sedentary lifestyle is a potential cause for changes in paediatric seasonal fracture frequency and severity. The aim of this study was to evaluate the current seasonal variations of paediatric fractures in order to determine resource allocation in hospitals, community clinics and prevention programs.
Methods
A single institutional review of historical data of all patients aged 0 to 16 years that were diagnosed with fractures between April 2014 and July 2017 in the emergency department of a level 3 orthopaedic trauma centre was conducted. In all, 3484 fractures were reviewed, of which 2991 were included. We stratified fractures according to patients’ variants and the hour, day and month with respect to holidays, weekends and weather.
Results
While the fracture rate on school days was 6.62 per day, the fracture rate during the summer vacation was 4.45 (p < 0.01). Hot weather was correlated with low fracture rates. The peak hours of admission were 12:00 to 13:00 and 18:00 to 22:00, with more moderate differences during non-school periods.
Conclusion
The local seasonal variation of paediatric fractures has a bimodal distribution, with similar nadirs during both summer and winter. These rates might reflect a shift to a more sedentary lifestyle during the summer vacation. The presented data can assist in improving the value of injury prevention measures and medical resources allocation.
Level of evidence:
II
Keywords: epidemiology, seasonal variation, paediatric fractures, children
Introduction
Fractures during childhood are common1,2 and have a great effect on the child’s and family’s daily life. They carry potentially significant social and economic consequences both in the short and long term.2,3 Sports and play are the leading cause for paediatric fractures1–4 and the vast majority of major paediatric injuries in emergency rooms are fractures.5 In order to allocate proper preventive measures and to plan the correct medical workforce and resources, an updated and geographically specific evaluation of the incidence and presentation of paediatric fractures is of needed.
It was previously shown that the incidence and presentation of paediatric fractures differ throughout the year.1,6,7 A common concept was that vacations and holidays were associated with injuries, while the effect of the peak of the summer season in increasing or decreasing the fracture rates was somewhat inconsistent.1–3,8–15 Most studies thus far have shown unimodal variability with peaks during the warm seasons that sometimes wane at peak summer.1–3,8–15 Many of these studies have originated in cold climate regions or were conducted on non-millennial children, and might not represent the fracture rate variability in warm countries nowadays.8,14,16,17 Our aim was to audit a single centre’s experience with paediatric fractures and determine the incidence variations and the variation in severity of fractures during the study period.
Materials and methods
A single institutional review of historical data was conducted following the approval of Meir Medical Centre institutional review board. The study took place in a level 3 orthopaedic trauma centre. We used the search engine on our hospital’s electronic archive to look for patients aged less than 16 years that were treated in the emergency department between 10 April 2014 and 30 July 2017 and whose diagnosis were coded as fractures or dislocations according to the International Classification of Disease (ICD)-9 (805.** to 839.**)18. The dates were chosen in concordance with the local computerized system record availability. The diagnosis was established in the emergency department setting by an orthopaedic surgery resident or attendant. We excluded records that were duplicates of referrals regarding the same injury. Since our department does not treat cranial and rib fractures, they were also excluded. A patient’s demographic data, as well as presentation timing and limb involvement were collected. Dates were stratified according to Saturdays (non-school-non-work days), holidays and vacations (non-school-days and mixes work vacations), summer vacation (01 July to 30 August) and school-days. Sundays are the first work-day of the week in Israel and were counted accordingly as week-days.
In all, 3484 fractures were reviewed. A total of 493 cases were excluded: 220 cases were diagnosed prior to January 2016, when the computed medical record system (Chameleon, ELAD HealthCare Solutions, Tel-Aviv, Israel) was introduced to the emergency department in our hospital. Due to a suboptimal application of the ICD-9 coding system prior to that date this period was unreliable for a computer-based patient search. In all, 273 cases were found to be duplicates. Eventually 2991 fractures in 2821 children during a 17-month period were included (Fig. 1). The gender distribution is presented in Table 1.
Fig. 1.
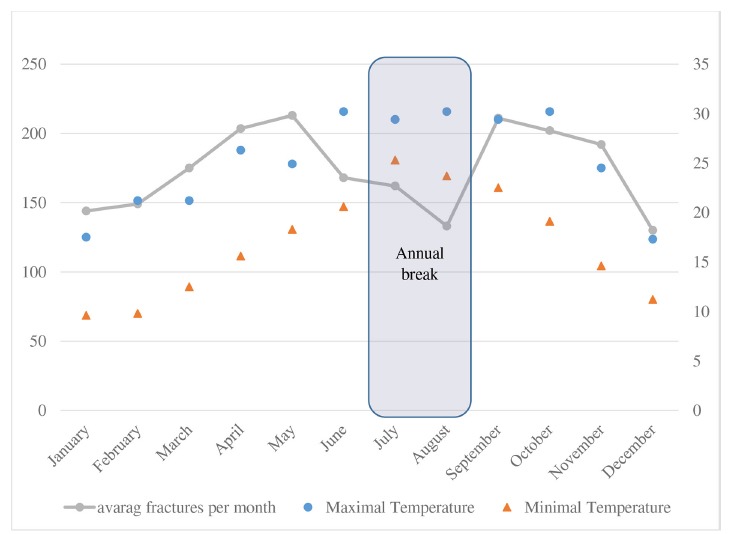
Weather and paediatric fracture risk (left Y axis: number of fractures, right Y axis: degrees (celsius)).
Table 1.
Fractures, operations and hospitalizations – the effect of gender
| Variable | Fractures, n | Total fracture (%)s | p-value | Operations, n | Total operations (%) | Fractures that were operated on (%) | p-value | Hospitalizations, n | Total hospitalizations (%) | Fractures that were hospitalized (%) | p-value |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | 1976 | 66.06 | < 0.001 | 160 | 76.19 | 8.10 | 0.001 | 285 | 70.72 | 14.42 | 0.049 |
| Female | 1015 | 33.94 | 50 | 23.81 | 4.93 | 118 | 29.28 | 11.63 | |||
| Total | 2991 | 100 | 210 | 100 | 7.02 | 403 | 100 | 13.47 |
p-values determined by chi-squared T-test
Weather data was collected through the online Israeli Meteorological Service archive for minimal and maximal daily temperatures and rain levels.19 These values were generalizable over the whole study area and were similar to previous years readings. The summer vacation in Israel takes place during July and August, which are also the hottest months of the year (Fig. 2). Extracurricular organized sports activities usually take place between September and June, and summer camps are run regularly throughout July and the beginning of August.
Fig. 2.
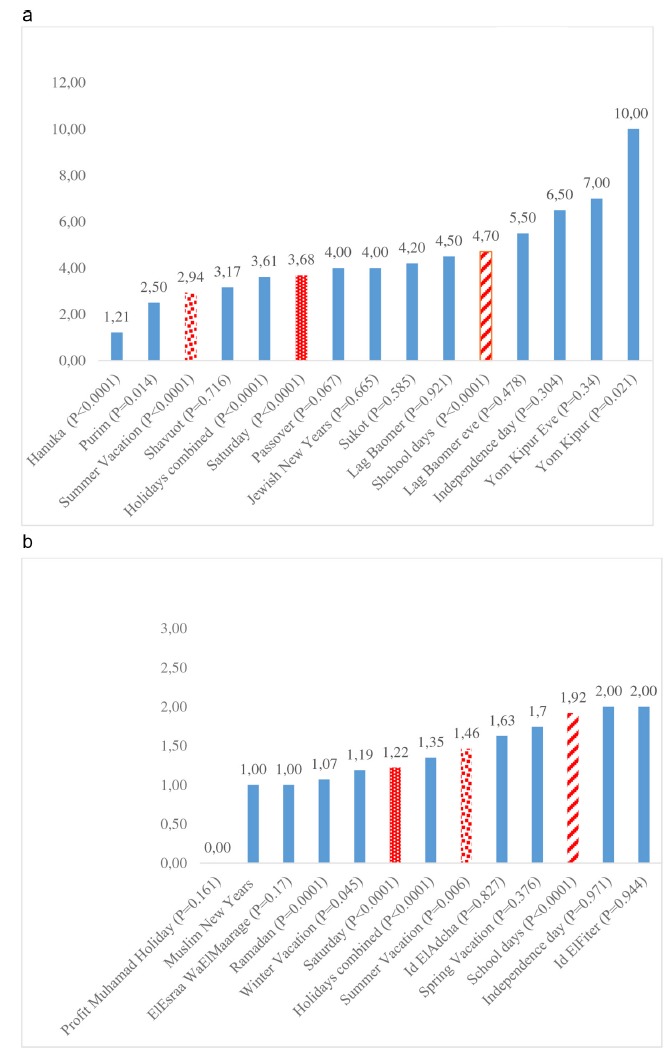
Number of: (a) fractures per day, the effect of Jewish holidays (fractures are presented as average incidence per day); (b) fractures per day, the effect of Muslim holidays (fractures are presented as average incidence per day).
Our hospital serves a population of approximately 1 000 000 people; of them around 26% are younger than 16 years (the Central Bureau of Statistics).20 The local population is composed of primarily two ethnicities: an Israeli Jewish majority and an Israeli Arab minority. The Jewish population is mainly urban and non-orthodox, and is composed of mixed Jewish Asian, African, Middle-Eastern or European ancestry. The Israeli Arab population is mainly urban. In this study the ratio between these populations was 79% versus 21%, respectively.
Statistical analysis
The decision on which statistical tools to use was based on a review of numerous seasonal variation studies.17,19,21–27 Data was sorted using Microsoft Excel software (Microsoft, Redmond, Washington). For the statistical analysis we used SPSS (version 25; IBM Corp., Armonk, New York). Data was presented as numbers, percentages and rates. Differences between patients, fractures and environment parameters were assessed using the chi-squared test. The correlation between continuous variables were measured with the Spearman correlation co-efficient. The effect of various risk factors on the fracture incidence was first evaluated by univariate Poisson regression analysis. Statistically significant variables were included in a stepwise backward and forward multivariate Poisson regression analysis model and were presented as incident rate ratio (IRR), 95% confidence interval (CI) and p-value, using a likelihood ratio. The goodness of fit was 1.17. The number of fractures on each day were used as the dependent variable. A p-vale < 0.05 was considered statistically significant.
Results
Holidays, Saturdays and the summer vacation
The fracture rates were found to be 6.62 fractures per day on school days, 3.67 on Saturdays, 4.96 during holidays and 4.45 during the summer vacation (Tables 2 and 3, Figs 2 and 3). The differences between school days and summer vacations were found to be statistically significant (p < 0.001). A specific Jewish holiday, Yom-Kipur, was found to be notably dangerous among the Jewish population, with ten fractures per day.
Table 2.
Fractures, operations and hospitalization – the effect of the calendar
| Day | Fractures/day | Fractures, n | Fractures that were hospitalized, n | Fractures that were hospitalized (%) | Difference, p-value (reference: school days) | Fractures that were operated, n | Fractures that were operated on (%) | Difference, p-value (reference: school days) |
|---|---|---|---|---|---|---|---|---|
| Holidays | 4.96 | 483 | 63 | 13.04 | N/S | 30 | 6.21 | N/S |
| Summer vacation | 4.45 | 259 | 56 | 21.62 | < 0.01 | 34 | 13.13 | <0.01 |
| School days | 6.62 | 1916 | 244 | 12.73 | N/S | 122 | 6.37 | N/S |
| Saturdays | 3.67 | 333 | 42 | 12.61 | N/S | 24 | 7.21 | N/S |
| Total | 5.99 | 2991 | 405 | 13.54 | N/S | 210 | 7.02 | N/S |
N/S, not significant
p-values determined by chi-squared T-test
Table 3.
Poisson regression model used to assess the effect of variables on the risk for paediatric fractures. The variables were selected by a stepwise (forward and backward) variable selection procedure
| Variable | Incident rate ratio | 95% confidence interval | p-value |
|---|---|---|---|
| Univariate Poisson regression model for all-year weather | |||
| Gender-female (categorical) | 0.51 | 0.47 to 0.56 | < 0.001 |
| Maximal temperature (°C) | 1.01 | 1.00 to 1.02 | 0.031 |
| Minimal temperature (°C) | 1 | 1 to 1.012 | 0.18 |
| Mean temperature (°C) | 1.01 | 1 to 1.014 | 0.064 |
| Rain level (mm/day) | 1 | 0.99 to 1.01 | 0.48 |
| Summer vacation (categorical) | 0.8 | 0.69 to 0.93 | < 0.01 |
| Multivariate Poisson regression model for all-year weather | |||
| Gender-female (categorical) | 0.51 | 0.47 to 0.56 | < 0.001 |
| Mean temperature (°C) | 1.02 | 1.01 to 1.02 | < 0.001 |
| Summer vacation (categorical) | 0.71 | 0.61 to 0.82 | < 0.001 |
| Multivariate Poisson regression model only for days with maximal temperature above 28°C | |||
| Gender-female (categorical) | 0.51 | 0.45 to 0.57 | < 0.001 |
| Mean temperature (°C) | 0.97 | 0.95 to 0.99 | 0.02 |
| Summer vacation (categorical) | 0.84 | 0.71 to 0.99 | 0.03 |
| Poisson regression model only for days with maximal temperature below 28°C | |||
| Gender-female (categorical) | 0.52 | 0.47 to 0.58 | < 0.001 |
| Mean temperature (°C) | 1.04 | 1.03 to 1.06 | < 0.001 |
| Summer vacation (categorical) | - | - | - |
Fig. 3.
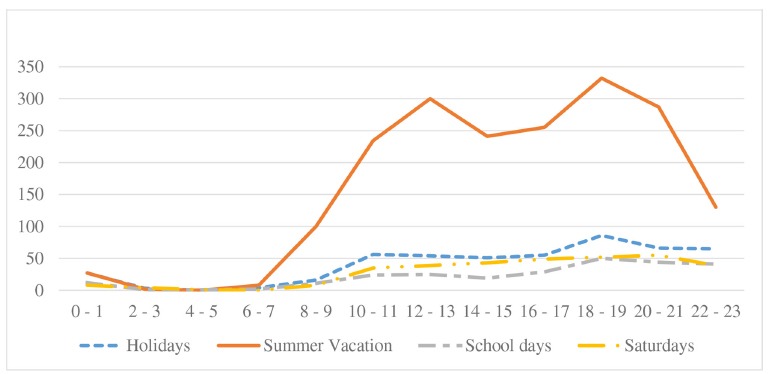
Paediatric fractures referral hours in a 17-month period, absolute numbers. Fractures (Y axis) are presented in absolute numbers, the hours (X axis) are presented in two-hour groups.
Weather
As a first step, the correlation between the daily temperatures (minimal, maximal and average) and the daily fracture incidence was assessed. Two different patterns were noted, with a daily maximal temperature of 28°C being the clearest cutoff. Below 28°C a positive correlation was found between temperature and fracture risk, r(s) = 0.853 (p < 0.001), while above it the correlation inversed, r(s) = −0.93 (p < 0.001) (Fig. 2). Following these findings a univariate Poisson regression analysis was conducted (Table 3). The statistically significant factors were included in a multivariate regression analysis that was conducted twice: the first was for the whole study period and the second was only for the days where maximal temperature reached above 28°C (Table 3). Using this method three independent protective factors against fractures were found: female gender, average temperatures above 28°C and the summer vacation (p < 0.05). In order to reassure the elimination of the temperature effect from the summer vacation effect, we further limited the dates to coupled 37 summer vacation days and 37 school days that had the exact same temperatures. In an analysis of the 386 fractures occurring on these days, fewer fractures per day occurred during the summer vacation (IRR 0.799, 95% CI 0.653 to 0.976, p = 0.028). Rain levels were found to have no influence on the fracture risk.
Referral hours
Two daily high peaks were recognized. The first was between 12:00 and 14:00 and the second between 18:00 and 22:00 (Fig. 3). In both populations 30.2% to 35.2% of patients arrived at the hospital during the later peak. In the Arab population a late peak between 22:00 and 24:00 was noted during holidays and summer vacation.
Admission and operation risks
Altogether 13.45% of all fractures were hospitalized and 7.02% were operated on. In comparison with school days, during the summer vacations a higher percentage of patients needed to be hospitalized and operated on in order to treat their fractures (p ≤ 0.001 for both, Tables 1 and 2). The operation and hospitalization rates were found to be higher for male patients (p < 0.05).
Discussion
The seasonal variation of paediatric fractures has bimodal variations, with peaks during the spring and autumn and nadirs during the summer and winter. In the current study the decline in the paediatric fracture incidence during the summer break was more prominent than what was previously presented in literature.1–3,9–16,25 A few factors could be attributed to this phenomenon: 1) changes in children’s behaviour patterns during unstructured periods like long vacations; 2) hot weather that prevented/discouraged outdoor activities; 3) families travelling abroad during summer vacations and therefore causing a possible decrease in the general workload; 4) weather-induced alterations in bone health.
In a well-known Swedish study by Landin, the paediatric fracture incidence between the years 1950 and 1979 peaked between May and August, with only a slight decrease in July.3 Later publications originating in the United Kingdom, Sweden and Norway exhibited similar findings, with extra incidence-peaks on the first snowy days or winter sports weeks.1,10,14 In a 2003 United Kingdom study regarding the seasonal variation of forearm fractures,27 the highest fracture rates in children occurred during the spring rather than in the summer although the latter was still a high-rate season. Investigators from the United Kingdom13 (2005) and Boston9 (2016) have found that the highest rates of trauma consultations took place during warm dry non-school days, but also noted that this increase waned at the peak of summer. The incidence valley during the middle of summer in their studies was minor, and the rates were still higher than during most of the year. In these studies the figures might have been more similar to ours if the coldest winter months in Boston and the United Kingdom had been excluded (as might be implied from Figure 2). These studies suggest that although the hot season was more dangerous as a whole, it was not the summer, but rather the spring that had the highest fracture rates, and that the summer fracture rate decline might be growing over the years. In a Mediterranean climate the difference between the spring and the summer appears to have become even more substantial and the summer has evolved into a low fracture-incidence season (Fig. 2).
Changes in the way children spend their free time might also have contributed to the summer fracture incidence nadir. A few researchers have lately described the summer break as encompassing behaviour patterns that are associated with a lower risk for fractures, and revealed the alarming correlation between summer vacations and an increase in body mass index levels in young children.28,29 Obesogenic behaviour was found to be accentuated during unstructured days, such as weekends and summer vacations.1,15,21 This behaviour is characterized by lack of compulsory physical activity, increase in sedentary time and unbalanced diet and sleep. Structured days, on the contrary, are characterized by engagement in pre-planned physical activities, either at school or as part of extra curriculum activities. A great portion of paediatric fractures are related to outdoor injuries, mostly during sports activities, and regular daily vigorous physical activities increase the risk of fractures.4,30 Therefore it could be assumed that the behavioural change during vacations is related to fracture paucity.
The sun exposure has a biological effect on bone turnover that was previously suspected to have a roll in altering the annual fracture risk. As winter begins, 1,25(OH)2D (Vitamin D) levels drop due to inadequate sun exposure.31 As a consequence the parathyroid hormone levels rise, usually at a one- to two-month delay, and promote bone resorption at mid-late winter.32 The consequence of this process is a poor bone quality which in turn leads to a higher fracture risk at the end of winter.33,34 While this effect might be more subtle in countries like Israel where winters are mild and the UVB exposure is consistently higher,30,35 in areas that have long and dark winters children might begin their spring sports activities with more vulnerable bones.3,16,33 During spring outdoor activities become frequent as the weather becomes friendlier. The combination of more frequent outdoor activities and presumably weaker bones would lead to a higher fracture rate as the spring emerges, and might be one of the reasons behind both the seasonal variation and geographical differences.3 Since in the current study a rise in the fracture rate was also revealed at the end of summer, which might correlate with the initiation of the school year, (Fig. 2) the biological effect is probably at most only a part of the explanation for the incidence variation.
Seven of every 100 fractures that were diagnosed in the emergency department needed operative treatment. We found that male patients sustained more fractures than female, and a higher percentage of their fractures were further hospitalized and operated on (8.8% versus 4.93%, p = 0.001). The difference in treatment modalities between the two genders might represent a difference in fracture severity, indicating that male patients sustain more robust fractures. This notion was in concordance with other authors25 that presented similar findings.
Local traditions and habits have a major effect on fracture incidence. Of note in the current study is Yom-Kipur, a 24-hour fast that begins around 18:00 on Yom Kipur’s Eve, and during which a complete sabbatical takes place. During this evening and the following day it is customary that vehicles do not drive on the roads and masses of non-religious children spend the holiday biking and skating the streets, and are therefore endangered. A specific record analysis of fractures that occurred during this holiday confirmed this habit correlates with the injury mechanisms. When analyzing the presentation of injuries, it is essential to be familiar with local habits and culture in order to properly understand the findings. The reproducibility of epidemiological findings is limited to these geographical variations.
We believe that our findings are relevant for comparable climate areas around the world such as Mediterranean countries and the middle and southern states of the United States. In countries with substantially different weather we propose this study as a platform for local analysis, but do expect the annual break to have similar effect.
This study has the basic weaknesses of a retrospective analysis. We did not collect data regarding fracture risk factors like medications or chronic diseases, but rather assumed that our cohort represents the general population since no relevant inclusion criteria were applied. A very high rate of too general coding (ICD-9) was found. Although the computed system was introduced to the emergency department at our hospital only in January 2016, it was used at the orthopaedic department by the same care givers many years before that. Therefore, we do not think it was the implementation process that led to this undesired phenomenon. Further research regarding the causes for this trend needs to be done in order to find means to improve our performance in that regard. The retrospective research method did not allow a valid method for analyzing the exact injury mechanism or the usage of a protective device, which could be conducted in a future prospective study. The fact that similar previous studies reached different findings should be held as representing trends within the time and place they were conducted, rather than misinterpreted as right or wrong.
Conclusions
The local seasonal variation of paediatric fractures has a bimodal pattern, with similar nadirs during both summer and winter. These rates might reflect a shift to a more sedentary lifestyle during the summer vacation. The presented data, followed by a prospective study that analyzes the specific injury mechanisms, can assist in improving the value of injury prevention measures and medical resources allocation.
Acknowledgements
The authors would like to thank Mrs Nava Jelin and Mr Yehoshua Enuka for the statistical analysis consultation.
Compliance with Ethical Standards
Funding Statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
OA Licence Text
This article is distributed under the terms of the Creative Commons Attribution-Non Commercial 4.0 International (CC BY-NC 4.0) license (https://creativecommons.org/licenses/by-nc/4.0/) which permits non-commercial use, reproduction and distribution of the work without further permission provided the original work is attributed.
Ethical Statement
Ethical approval: All procedures performed in this study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent: Not required for this work.
ICMJE Conflict of Interest Statement
All authors declare that they have no conflict of interest.
References
- 1.Hedström EM, Svensson O, Bergström U, Michno P. Epidemiology of fractures in children and adolescents. Acta Orthop 2010;81:148–153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Clark EM. The epidemiology of fractures in otherwise healthy children. Curr Osteoporos Rep 2014;12:272–278. [DOI] [PubMed] [Google Scholar]
- 3.Landin LA. Fracture patterns in children. Analysis of 8,682 fractures with special reference to incidence, etiology and secular changes in a Swedish urban population 1950–1979. Acta Orthop Scand Suppl 1983;202:1–109. [PubMed] [Google Scholar]
- 4.Wren TAL, Shepherd JA, Kalkwarf HJ, et al. . Racial disparity in fracture risk between white and nonwhite children in the United States. J Pediatr 2012;161:1035–1040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Voth M, Lustenberger T, Auner B, Frank J, Marzi I. What injuries should we expect in the emergency room? Injury 2017;48:2119–2124. [DOI] [PubMed] [Google Scholar]
- 6.D’Ippolito A, Collins CL, Comstock RD. Epidemiology of pediatric holiday-related injuries presenting to US emergency departments. Pediatrics 2010;125:931–937. [DOI] [PubMed] [Google Scholar]
- 7.Henrikson B. Isolated fractures of the proximal end of the radius in children epidemiology, treatment and prognosis. Acta Orthop Scand 1969;40:246–260. [DOI] [PubMed] [Google Scholar]
- 8.Sinikumpu J-J, Pokka T, Hyvönen H, Ruuhela R, Serlo W. Supracondylar humerus fractures in children: the effect of weather conditions on their risk. Eur J Orthop Surg Traumatol 2017;27:243–250. [DOI] [PubMed] [Google Scholar]
- 9.Livingston KS, Miller PE, Lierhaus A, Matheney TH, Mahan ST. Does weather matter? the effect of weather patterns and temporal factors on pediatric orthopedic trauma volume. Open Orthop J 2016;10:550–558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Randsborg P-H, Gulbrandsen P, Saltytė Benth J, et al. . Fractures in children: epidemiology and activity-specific fracture rates. J Bone Joint Surg [Am] 2013;95:e42. [DOI] [PubMed] [Google Scholar]
- 11.Lyons RA, Delahunty AM, Kraus D, et al. . Children’s fractures: a population based study. Inj Prev 1999;5:129–132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Milford KL, Navsaria PH, Nicol AJ, Edu S. Trauma unit attendance: is there a relationship with weather, sporting events and week/ month-end times? An audit at an urban tertiary trauma unit in Cape Town. S Afr J Surg 2016;54:22–27. [PubMed] [Google Scholar]
- 13.Atherton WG, Harper WM, Abrams KR. A year’s trauma admissions and the effect of the weather. Injury 2005;36:40–46. [DOI] [PubMed] [Google Scholar]
- 14.Cooper C, Dennison EM, Leufkens HGM, Bishop N, van Staa TP. Epidemiology of childhood fractures in Britain: a study using the general practice research database. J Bone Miner Res 2004;19:1976–1981. [DOI] [PubMed] [Google Scholar]
- 15.Brazendale K, Beets MW, Weaver RG, et al. . Understanding differences between summer vs. school obesogenic behaviors of children: the structured days hypothesis. Int J Behav Nutr Phys Act 2017;14:100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tiderius CJ, Landin L, Düppe H. Decreasing incidence of fractures in children: an epidemiological analysis of 1,673 fractures in Malmö, Sweden, 1993–1994. Acta Orthop Scand 1999;70:622–626. [DOI] [PubMed] [Google Scholar]
- 17.Zangbar B, Rhee P, Pandit V, et al. . Seasonal variation in emergency general surgery. Ann Surg 2016;263:76–81. [DOI] [PubMed] [Google Scholar]
- 18.No authors listed ICD - ICD-9-CM - International Classification of Diseases, Ninth Revision, Clinical Modification. https://www.cdc.gov/nchs/icd/icd9cm.htm (date last accessed 18September2018).
- 19.No authors listed Israel Meteorological Service (IMS) Homepage. http://www.ims.gov.il/IMSENG/All_Tahazit/homepage.htm (date last accessed 16November2017).
- 20.No authors listed Central Bureau of Statistics. http://www.cbs.gov.il (date last accessed 15September2018).
- 21.Tanaka C, Reilly JJ, Tanaka M, Tanaka S. Seasonal changes in objectively measured sedentary behavior and physical activity in Japanese primary school children. BMC Public Health 2016;16:969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ma Y, Olendzki BC, Li W, et al. . Seasonal variation in food intake, physical activity, and body weight in a predominantly overweight population. Eur J Clin Nutr 2006;60:519–528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wellings K, Macdowall W, Catchpole M, Goodrich J. Seasonal variations in sexual activity and their implications for sexual health promotion. J R Soc Med 1999;92:60–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Atkin AJ, Sharp SJ, Harrison F, Brage S, Van Sluijs EMF. Seasonal variation in children’s physical activity and sedentary time. Med Sci Sports Exerc 2016;48:449–456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Rennie L, Court-Brown CM, Mok JYQ, Beattie TF. The epidemiology of fractures in children. Injury 2007;38:913–922. [DOI] [PubMed] [Google Scholar]
- 26.Voth M, Lustenberger T, Frank J, Marzi I. Pediatric finger and hand injuries: an epidemiological study. Chirurg 2017;88:871–878. [DOI] [PubMed] [Google Scholar]
- 27.Wareham K, Johansen A, Stone MD, et al. . Seasonal variation in the incidence of wrist and forearm fractures, and its consequences. Injury 2003;34:219–222. [DOI] [PubMed] [Google Scholar]
- 28.von Hippel PT, Workman J. From kindergarten through second grade, U.S. children’s obesity prevalence grows only during summer vacations. Obesity (Silver Spring) 2016;24:2296–2300. [DOI] [PubMed] [Google Scholar]
- 29.Moreno JP, Johnston CA, Woehler D. Changes in weight over the school year and summer vacation: results of a 5-year longitudinal study. J Sch Health 2013;83:473–477. [DOI] [PubMed] [Google Scholar]
- 30.Clark EM, Ness AR, Tobias JH. Vigorous physical activity increases fracture risk in children irrespective of bone mass: a prospective study of the independent risk factors for fractures in healthy children. J Bone Miner Res 2008;23:1012–1022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Braegger C, Campoy C, Colomb V, et al. . Vitamin D in the healthy European paediatric population. J Pediatr Gastroenterol Nutr 2013;56:692–701. [DOI] [PubMed] [Google Scholar]
- 32.Pasco JA, Henry MJ, Kotowicz MA, et al. . Seasonal periodicity of serum vitamin D and parathyroid hormone, bone resorption, and fractures: the Geelong Osteoporosis Study. J Bone Miner Res 2004;19:752–758. [DOI] [PubMed] [Google Scholar]
- 33.Ceroni D, Anderson de la Llana R, Martin X, et al. . Prevalence of vitamin D insufficiency in Swiss teenagers with appendicular fractures: a prospective study of 100 cases. J Child Orthop 2012;6:497–503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Saglam Y, Kizildag H, Toprak G, Alp NB, Yalcinkaya EY. Prevalence of vitamin D insufficiency in children with forearm fractures. J Child Orthop 2017;11:180–184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Erol M, Yiğit Ö, Küçük SH, Bostan Gayret Ö. Vitamin D deficiency in children and adolescents in Bağcılar, İstanbul. J Clin Res Pediatr Endocrinol 2015;7:134–139. [DOI] [PMC free article] [PubMed] [Google Scholar]