

Abstract
Female genital mutilation/cutting is a form of violence against women and girls. It includes all procedures that involve the partial or total removal of external genitalia or other injury to the female genital organs for non-medical reasons. It is estimated that over 200 million girls and women worldwide have suffered the effects of this practice and that approximately 3.6 million girls and women are at risk each year. Female genital mutilation/cutting violates several human rights outlined under the Universal Declaration of Human Rights, the Convention on the Elimination of all Forms of Discrimination against Women, and the Convention on the Rights of the Child. Human rights-based approaches to eradication include, but are not limited to, the enforcement of laws, education programs focused on empowerment, and campaigns to recruit change agents from within communities.
Introduction
Violence against women and girls affects females throughout the world and crosses cultural and economic boundaries. Throughout the past 20 years, extensive research has been done on such violence and its underlying causes and risk factors.1 Interventions in health care, justice systems, and the social sphere have grown rapidly to address violence against women and girls worldwide. These interventions include large-scale campaigns, education programs, skills building and economic empowerment programming, community mobilization, and participatory group education efforts. Such interventions aim to change attitudes and norms that support violence against women and girls, thereby empowering women and girls economically and socially, as well as promoting nonviolent, gender-equitable behaviors.2
The United Nations (UN) and the European Union have recently started a global multiyear initiative focused on eliminating all forms of violence against women and girls. This effort, titled “The Spotlight Initiative,” brings attention to violence against women and girls in order to achieve gender equality and women’s empowerment and is in line with the 2030 Agenda for Sustainable Development.3 It also highlights the importance of targeted investments in women and girls to achieve sustainable development, making this renewed commitment of the UN and the European Union visible worldwide. While the initiative addresses all forms of violence against women and girls, it focuses in particular on domestic and family violence, sexual and gender-based violence and harmful practices, femicide, trafficking in human beings, and sexual and economic exploitation.
One major indicator of gender inequality is female genital mutilation/cutting (FGM/C). FGM/C is linked to child marriage, forced sexual debut, and health complications across the life course.4 In order to eliminate the practice, addressing the empowerment of girls and women is key. This can have a positive impact on gender relations, sexual and reproductive health choices, and health-related behavior in general, thus accelerating progress in abandonment of the practice.5 The UN, United Nations Children’s Fund, World Health Organization (WHO), and other anti-FGM/C organizations have adopted various strategies in order to raise awareness of and work toward ending FGM/C.6
Definition of female genital mutilation/cutting
FGM/C includes all procedures that involve the partial or total removal of external genitalia or other injury to the female genital organs for non-medical reasons.7
Different types of FGM/C
WHO classifies FGM/C into four types:
Type I: partial or total removal of the clitoris (clitoridectomy) or prepuce
Type II: partial or total removal of the clitoris and labia minora, with or without excision of the labia majora (excision)
Type III: narrowing of the vaginal orifice with the creation of a covering seal by cutting and appositioning the labia minora or labia majora, with or without excision of the clitoris (infibu-lation)
Re-infibulation: a procedure to narrow the vaginal opening after a woman has been dein-fibulated (for example, after childbirth), also known as re-suturing
Type IV: all other harmful procedures done to the female genitalia for non-medical purposes (for example pricking, pulling, piercing, incising, scraping, and cauterization)8
Prevalence
FGM/C is prevalent in 30 countries in Africa and several countries in Asia and the Middle East.9 The practice has also been reported among certain ethnic groups in Central and South America.10 The rise in international migration has increased the number of girls and women in Europe, the United States, Australia, and Canada who have undergone or may undergo the practice.11 The greatest prevalence of FGM/C among women and girls aged 15–49 is reported in Somalia (98%), Guinea (97%), and Djibouti (93%).12 The greatest prevalence of FGM/C among girls under 14 years is reported in Gambia (56%), Mauritania (54%), and Indonesia (~50%).13 Despite overall declines in rates of FGM/C, high rates of population growth in practicing countries means that the number of affected women and girls will likely increase by 2030.14 It is estimated that more than 200 million girls and women worldwide are living with the effects of FGM/C and that every year approximately 3.6 million girls and women are at risk of FGM/C.15
Figure 1.
Types of female genital mutilation/cutting
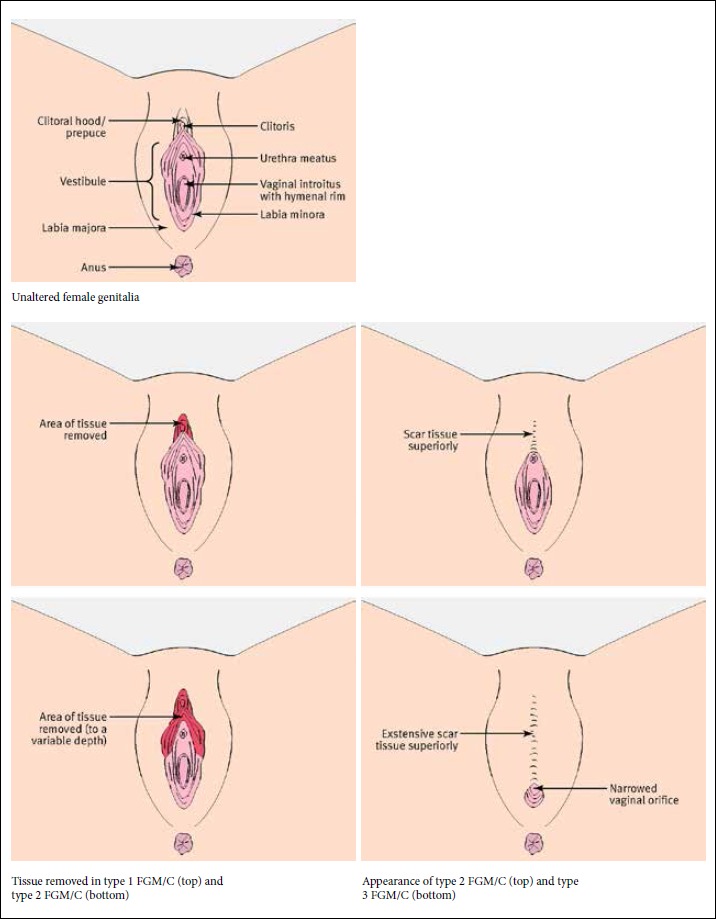
Source: J. Simpson, K. Robinson, S. Creighton, and D. Hodes, “Female genital mutilation: The role of health professionals in prevention, assessment, and management,” BMJ 344/e1361 (2012).
Health complications for girls and women
FGM/C is performed mainly on children and adolescents and has a ritual origin. The procedure is painful and traumatic, and there are no health benefits. It violates a series of human rights principles, including the principles of equality and non-discrimination on the basis of sex, the right to life (when the procedure results in death), the right to freedom from torture and cruel, inhuman, or degrading treatment or punishment, and the rights of the child.16
All forms of FGM/C carry the risk of adverse health consequences. Almost all girls and women who have undergone the procedure experience pain and bleeding.17 Immediate health complications include shock, hemorrhage, and infection. FG-M/C can also cause death, disability, miscarriage, stillbirth, problems during urination, infertility, ovarian cysts, open sores in the genital region, bacterial infections (tetanus or sepsis) during and after pregnancy, and increased risk of newborn deaths.18 The intervention itself is traumatic, as girls are usually physically held down during the procedure.19 Those who are infibulated often have their legs bound together for several days or weeks. The immediate consequences, such as infections, are usually documented only when girls and women seek hospital treatment.20
The long-term health risks of FGM/C include chronic pain, infection, keloids, fibrosis, primary infertility, and psychological suffering, such as post-traumatic stress disorder.21 FGM/C is often performed under unsterile conditions by a traditional female practitioner who has little knowledge of female anatomy or how to manage possible adverse events.22 Of all types of FGM/C, type III appears to pose the greatest risk of immediate harm, and these events tend to be considerably underreported.23
A 2006 WHO study in which more than 28,000 women participated concluded that women living with FGM/C are significantly more likely than those not living with FGM/C to experience adverse obstetric outcomes and that this risk seems to be greater with more extreme forms of the procedure.24 Given that some types of FGM/C involve the removal of or injury to sexually sensitive structures, including the clitoral glans and part of the labia minora, some women report a reduction in sexual response and diminished sexual satisfaction. In addition, scarring of the vulvar area may result in pain, including during sexual intercourse.25 Other findings from the WHO study confirm that women who have undergone FGM/C are at significantly increased risk of adverse events during childbirth.26 Such women also experience higher rates of Caesarean section and post-partum hemorrhage compared to those who have not undergone the procedure, and this risk increases with the severity of the procedure.27
Cultural reasons for FGM/C
The practice of FGM/C dates back thousands of years, with mummies in Egypt showing that it was a routine practice.28 There is evidence that FGM/C goes back at least to Pharaonic times and that the practice is prevalent among animists, Catholics, Jews, Muslims, Protestants, and those without religious beliefs.29 Some communities believe that FGM/C is a religious requirement, although it is not mentioned in major religious texts such as the Quran or the Bible.30 In the United Kingdom, clito-ridectomy was used in the management of epilepsy, sterility, and masturbation as recently as the 19th century.31 One of the first-known formal oppositions to the practice came from medical doctors in Egypt and from missionaries in Kenya, both in the early 20th century.32
In many societies, FGM/C is a rite of passage to womanhood with strong ancestral and sociocultural roots. Rationalizations for the procedure’s perpetuation include the preservation of ethnic and gender identity, femininity, female “purity,” and family honor; the maintenance of cleanliness and health; and assurance of women’s marriageability.33 In many contexts, social acceptance is the primary reason for continuing the practice. Other reasons include ensuring fidelity after marriage, preventing rape, providing a source of income for circumcis-ers, and enhancing aesthetic appeal.34
FGM/C is usually carried out by an older woman in the community, such as a relative or a traditional birth attendant, without the use of anesthetics, analgesics, aseptic techniques, or antibiotics. Immediate and long-term complications are common and can have a significant effect on the individual.35 Women who have undergone the procedure often refer to it as “cutting” or “being cut.” Nurses have heard patients use traditional names for FGM/C, such as halalays and qodiin (Somalia), kutairi (Kenya), megrez (Ethiopia), nia-ka (Gambia), thara (Egypt), and sunna (Nigeria and Sierra Leone).36 The English expression “female genital mutilation” emerged in the 1970s and eventually proved to be problematic, as parents resented the suggestion that they were mutilating their daughters. After the UN addressed the risk of demonizing certain cultures and traditions in 1999, the term “cutting” has been increasingly used to avoid alienating communities, hence the use of the more inclusive acronym FGM/C.37
Non-cultural and non-historical reasons for perpetuating FGM/C also exist. For example, people in countries such as Mali and Burkina Faso, as well as in most of West Africa, perceive the clitoris as a dangerous organ and require its removal.38 According to this view, the clitoris is poisonous and causes a man to become ill or die if it comes in contact with his penis. Other beliefs suggest that an uncut clitoris creates male impotency and kills babies upon delivery.39 Performing FGM/C is also perceived as a way to minimize a woman’s libido and assist her in resisting sexual activity by preventing her from acting promiscuously, thereby making her more appealing to her future husband.40
Human rights violations
A 2008 UN interagency statement defines FGM/C as a violation of human rights, a form of discrimination on the basis of gender, and a form of violence against girls.41 The practice violates several human rights outlined under the Universal Declaration of Human Rights, the Convention on the Elimination of All Forms of Discrimination against Women (CEDAW), and the Convention on the Rights of the Child.42 Article 3 of the Universal Declaration of Human Rights states that everyone has the right to life, liberty, and security of person. Unfortunately, in many countries, women and girls are not in full control of their lives, their liberty, or their bodies.43
On December 18, 1979, the United Nations General Assembly adopted CEDAW, which became effective on September 3, 1981.44 CEDAW defines discrimination against women and outlines an agenda for international action to end such discrimination.45 The convention’s underlying philosophy is that “discrimination against women violates the principles of equality of rights and respect for human dignity.”46 Article 5 requires states parties to take measures to achieve “the elimination of prejudices and customary and all other practices which are based on the idea of the inferiority or the superiority of either of the sexes.”47
Although CEDAW is intended to change the “social and cultural patterns of conduct of men and women,” not all countries are willing participants. Somalia is one of the few countries that has neither signed nor ratified this convention, indicating an unwillingness to recognize certain basic human rights. Somalia’s lack of participation in CEDAW may also suggest that the country’s political activity and traditions need to evolve from a legislative perspective.48
The Convention on the Rights of the Child refers to the ever-evolving capacity of children to make their own decisions regarding matters that directly affect them. However, in terms of FGM/C, even in cases where there is an apparent agreement by girls to undergo the procedure, the decision is a direct result of social pressure and community expectations. A girl’s decision to undergo FGM/C therefore cannot be deemed free, informed, or free of coercion.49 One of the guiding principles of the Convention on the Rights of the Child is the primary consideration of “the best interest of the child.”50 Some parents who decide to subject their daughters to FGM/C believe that the benefits outweigh the risks. However, this perception does not justify a permanent and life-changing practice that constitutes a violation of girls’ fundamental human rights.51 The convention makes explicit reference to harmful traditional practices such as FGM/C. The Committee on the Rights of the Child, as well as other United Nations treaty monitoring bodies, has frequently stated that FG-M/C is a violation of human rights, calling on states parties to take all effective and appropriate measures to abolish the practice.52
FGM/C violates a series of well-established human rights principles, norms, and standards, including the principles of equality and non-discrimination on the basis of sex, the right to life (when the procedure results in death), the right to freedom from torture and cruel, inhuman, or degrading treatment or punishment, and the rights of the child.53 Because it interferes with healthy genital tissue in the absence of medical necessity and can lead to severe consequences for a woman’s physical and mental health, FGM/C is also a violation of a person’s right to the highest attainable standard of health.54 Although many governments worldwide recognize FGM/C as an act of violence against women and girls and as a violation of human rights, the issue is clouded in debate because the practice is deeply entrenched in culture and tradition, making legislation difficult to approve and enforce.55
Legislation and resistance
Since 1965, 24 of the 29 countries with the highest prevalence of FGM/C have used a human rights-based approach to their legislation on FGM/C.56 Penalties can range from three months to life in prison. Several countries also impose monetary fines. Twelve developed countries with substantial FGM/C-practicing populations have also passed laws criminalizing the practice.57 Some laws ban the provision of FGM/C in government health facilities and by medical practitioners. Some criminalize FGM/C only when performed on minors, while others criminalize it in all cases. Fines may apply only to practitioners or to anyone who knows it is happening and does not report it. The crime may cover only cutting in the country itself or include taking a girl to another country to have it done.58
The right to participate in cultural life and the right to freedom of religion are protected by international law. However, international law stipulates that the freedom to manifest one’s religion or beliefs might be subject to limitations necessary to protect the fundamental rights and freedoms of others. Therefore, social and cultural claims such as those protected in article 4 of the International Covenant on Civil and Political Rights cannot be evoked to justify FGM/C.59 Legislation is an important tool for eradicating FGM/C, as it can challenge the traditional status quo by providing legitimacy to new behaviors—but unless it is accompanied by measures aimed at influencing cultural traditions and expectations, it tends to be ineffective.60
Individuals, communities, and countries go through transitional stages in terms of their desire to adhere to FGM/C, to contemplate abandoning the practice, and to completely abandon the practice. The readiness to abandon FGM/C varies across countries. For example, in Somalia, there is a high prevalence of FGM/C (98%) and a strong desire to adhere to the practice; in Egypt, two-thirds of women want to adhere to FGM/C, and almost one-quarter want to abandon it; and in Nigeria, almost equal proportions (about 40%) want to adhere to and to abandon the practice, with 14% “reluctantly adhering” and 13% contemplating abandonment.61
Among these transitional stages of abandoning FGM/C, tensions remain between those who aim to abolish FGM/C and those who desire to perpetuate it.62 Since FGM/C is deeply embedded in culture and considered central to the identity of many Africans, the issue must be approached with great respect and effort on the part of Westerners to understand the cultural context and rationale of this tradition. If FGM/C is to be completely eradicated, African communities and international support agencies must work collectively at the grassroots level to evaluate the implications of the practice.63
Support for a culture of FGM/C is expressed through a reluctance to comply with anti-FGM/C laws and to present evidence against family members, friends, or neighbors, as well as criticism or sarcasm directed toward law enforcers.64 In a number of cases, local law enforcers and anti-FGM/C crusaders (such as pastors, chiefs, assistant chiefs, and other leaders) may experience a conflict of loyalty by enforcing the law, as it puts them at odds with the local culture, a process sometimes referred to as “social nullification.”65 While criminalizing harmful cultural practices such as FGM/C is necessary, it can equally generate rebellion geared toward circumventing or resisting the law.66
Education
Educational rights-based approaches to eradicating FGM/C present communities with a package of opportunities for learning. However, such interventions can sometimes be perceived by communities as an unsolicited top-down approach.67 Therefore, working with communities prior to implementation is of utmost importance. This increases community acceptance of an intervention, leading to its success.68
Education is often favored over other rights-based approaches, such as legislation, because it is less repressive.69 Although legal restrictions have been found to reduce the rate of FGM/C, they have also been found to drive the practice underground.70 In other instances, the law has led to parents subjecting their daughters to FGM/C at a younger age before they become susceptible to anti-FGM/C messages.
While legal and political measures are necessary to ending FGM/C, community-based educational initiatives are also critical and have become a key component of campaigns worldwide. Government action is necessary to create a political and legal environment that deters people from practicing FGM/C, but it is ultimately the women, their families, and their communities who must be convinced to abandon the practice.71
Community empowerment
Consideration of the target population’s characteristics must be present in order to contextualize educational interventions that use a rights-based approach. Contextualizing involves the full inclusion of the communities in planning the programs, such as by involving community members as facilitators or research assistants.72 Religious and other key leaders must be empowered by helping promote the interventions. In addition, community members can help disseminate information to relatives and friends, therefore encouraging public awareness and resistance to FGM/C.73 Furthermore, information about FGM/C must be tailored to fit the needs of the target populations, as this increases the acceptability of the program and leads to quicker dissemination of information among communities.74
Cultural competency training can help improve health outcomes and the quality of care. However, further research is needed to understand how best to involve different demographic groups, including non-practicing communities, in rights-based educational interventions in order to maximize the prevention of FGM/C.75 Multi-pronged, community-led programs in conjunction with legal efforts have been found to be successful in eradicating FGM/C. The largest decline has been seen in Kenya and Burkina Faso, where there has been a very strong legal response, as well as community-based education efforts.76
The first program for the prevention of FGM/C, which began in the mid-1970s, focused on informing and motivating communities about the adverse health effects of FGM/C in order to break the taboo. To transmit the message, the program used information, education, and communication materials, such as leaflets, booklets, training manuals, and guidebooks for professionals. Its emphasis was on awareness raising rather than behavior change and thus focused on short-term results, since behavior change takes time.77 Interventions must be directed toward the alleviation of stigma and provide technical and financial materials at the community level.78 Religious and community leaders must play a significant role in arranging trainings, workshops, media campaigns, and outreach in order to bring about the desired behavioral change. Moreover, it is important that programs address the long-term health consequences of FGM/C, general reproductive health issues, gender-based violence, parenting strategies, and communication and relationships skills. Community members must actively take part in these programs, while the government must ensure that the law is enforced. Finally, in rural areas, it is important that local organizations establish anti-FGM/C support groups in order to facilitate positive behavioral change.79
One successful rights-based health intervention has been to respect the importance of passage rites and promote alternatives that do not involve cutting.80 For example, grassroots campaigners in Sierra Leone are changing cultural practices by recognizing the importance of soweis, the women leaders who perform FGM/C. The goal is to find alternative income sources for these women and to reinvent their roles as the guardians of traditional culture, without the cutting. In Somalia, Save the Children and partners are supporting local nongovernmental organizations in modifying cultural perceptions of cutting as central to girls’ rites of passage and in finding alternate ways to elevate the status and value of women in the family and community. These rights-based approaches preserve communities’ cultural heritage and social values while shifting cultural beliefs away from FGM/C.81
Higher education, however, is the main factor associated with supporting the discontinuation of FGM/C.82 For community leaders, empowerment combined with higher education plays a significant role in the elimination of FGM/C.83 The interaction between empowerment and education is significant and predicts individuals’ intention to discontinue the practice.84
Involvement of men
FGM/C affects men as well as women. Many men feel that they too are victims of this practice and want to see it end. A sense of social obligation is an important barrier to stopping FGM/C, while higher educational attainment is one of the most important indicators for men’s support for abandoning the practice.85 Several studies demonstrate that men generally respond positively to being involved in sexual and reproductive health programs.86
The Global Alliance against FGM is an organization based in France and Switzerland that maintains a focus on men’s involvement in eliminating the practice. The alliance is at the forefront of the international effort to accelerate the total elimination of violence against women and girls worldwide. It works closely with WHO, UNESCO, the UN General Assembly, Permanent Missions to the UN, nongovernmental organizations, and individuals all over the world. Since 2009, the Global Alliance against FGM has hosted conferences and events focusing on men who said “no” to FGM/C. The alliance advocates for support and strengthened grassroots work with a priority on developing tools that help optimize efforts at the local, regional, national, and international levels.87
The involvement of men must complement current rights-based programs focusing on education and the empowerment of girls and women. Influential males in communities where the practice is prevalent must lead programs as advocates while facilitating dialogue between men and women, their communities, and government bodies.88
Conclusion
FGM/C is a manifestation of gender inequality, and the empowerment of women is of utmost importance to the elimination of the practice. A range of documented programmatic, research, and policy interventions—led by a variety of national and international nongovernmental organizations and UN agencies—is being implemented to encourage communities, families, and individuals to abandon FGM/C.89 These strategies have encompassed advocacy and education interventions aimed at communities and leaders, legislative interventions, capacity-building interventions, health care interventions, media interventions, and community dialogue.90
Addressing FGM/C through education brings to light the human rights of girls and women and the differential treatment of boys and men. Education can serve to influence gender relations and thus accelerate progress in the abandonment of the practice. Human rights-based programs that foster women’s economic empowerment contribute to progress, as they provide incentives for changing patterns of traditional behavior to which women and girls are bound as dependent members of the household. Gainful employment empowers women in various spheres of their lives, influencing their sexual and reproductive health choices, their education, and their health-related behavior in general.
There is a positive relationship between empowerment, community interventions, and knowledge about the health consequences of FG-M/C. Rights-based programs must be community led and must be tailored to take into consideration the ideological structure and ethnic and socioeconomic differences of each community. Responding to communities’ needs and priorities plays an integral part in gaining people’s trust and making change relevant.91
References
- 1.Heise L. STRIVE Research Consortium. “What works to prevent partner violence? An evidence overview,” working paper, London School of Hygiene and Tropical Medicine, London (2011).
- 2.Morrison A., Ellsberg M.. Bott S.. “Addressing gender-based violence: A critical review of interventions,”. World Bank Research Observer. 2007;22(1):25–51. and. [Google Scholar]
- 3. United Nations General Assembly, Res. 70/1, UN Doc. A/RES/70/1 (2015).
- 4.Battle J., Hennink M.. Yount K.. “Influence of female genital cutting on sexual experience in Southern Ethiopia,”. Fulu E., Miedema S., Roselli T.. Farage M., Miller K., Tzeghai G.. International Journal of Sexual Health. Lancet Global Health. Women’s Health. 2017;2017;2015;29511(2)(5)(1):173–186. 79–94. and. et al., “Pathways between childhood trauma, intimate partner violence, and harsh parenting: Findings from the UN multi-country study on men and violence in Asia and the Pacific,”. pp. e512–e522; et al., “Female genital cutting: Confronting cultural challenges and health complications across the lifespan,”. [Google Scholar]
- 5.Eliminating female genital mutilation: An interagency statement—OHCHR, UNAIDS, UNDP, UNECA, UNESCO, UNFPA, UNHCR, UNICEF, UNIFEM, WHO. Geneva: World Health Organization; 2008. World Health Organization, [Google Scholar]
- 6.Brown K., Beecham D. Barrett H. Obstetrics and Gynecology International. and. “The applicability of behaviour change in intervention programmes targeted at ending female genital mutilation in the EU: Integrating social cognitive and community level approaches,”. (2013). [DOI] [PMC free article] [PubMed]
- 7.WHO guidelines on the management of health complications from female genital mutilation: Policy brief. Geneva: World Health Organization; 2016. World Health Organization, [PubMed] [Google Scholar]
- 8. Ibid.
- 9.Reproductive Health Matters. UNICEF, “Female genital mutilation/cutting: A statistical overview and exploration of the dynamics of change,”. (2013), pp. 184–190; WHO (2016, see note 7).
- 10. WHO (2016, see note 7).
- 11.van Baelen L., Ortensi L.. Leye E.. “Estimates of first-generation women and girls with female genital mutilation in the European Union, Norway and Switzerland,”. Leye E., Mergaert L., Leye E., Ar-naut C.. Leye E., O’Brien Green S.. “Towards a better estimation of prevalence of female genital mutilation in the European Union: Interpreting existing evidence in all EU member states,”. Goldberg H., Stupp P., Oko-roh E.. “Female genital mutilation/cutting in the United States: Updated estimates of women and girls at risk,”. Dawson A., Turk-mani S., Fray S.. “Evidence to inform education, training and supportive work environments for midwives involved in the care of women with female genital mutilation: A review of global experience,”. Higginbottom G. M., Chiu Y., Mumtaz Z.. “‘I have to do what I believe’: Sudanese women’s beliefs and resistance to hegemonic practices at home and during experiences of maternity care in Canada,”. European Journal of Contraception and Reproductive Health Care. Genus. Public Health Reports. Midwifery. BMC Pregnancy Childbirth. 2016;2014;2016;2015;2013;21701313113(6)(1)(2)(1)(1):474–482. and. and. et al., pp. 340–347; et al. pp. 229–238; et al. p. 51; UNICEF (2013, see note 9). [Google Scholar]
- 12.Women and girls, aged 15–49 who have undergone some form of FGM. United Nations Population Fund FGM Dashboard, Available at https://www.unfpa.org/data/dashboard/fgm.
- 13. World Health Organization (2016, see note 7).
- 14. UNICEF (2013, see note 9).
- 15.Female genital mutilation/cutting: A global concern. New York: UNICEF; 2016. pp. 1–4. UNICEF, [Google Scholar]
- 16. World Health Organization (2016, see note 7).
- 17.Khosla R., Banerjee J., Chou D. Talle A. Hernlund Y., Shell-Duncan B. Reproductive Health. Transcultural bodies: Female genital cutting in global context. 1. Vol. 14. New Brunswick: Rutgers University Press; 2017. 2007. “Gender equality and human rights approaches to female genital mutilation: A review of international human rights norms and standards,”; p. 59.“Female circumcision in Africa and beyond: The anthropology of a difficult issue,”; et al., p. (eds), pp. 91−106; World Health Organization (2008, see note 5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Khosla et al. (see note 18); World Health Organization (2008, see note 5).
- 19. Talle (see note 17); World Health Organization (2008, see note 5).
- 20. Talle (see note 17); World Health Organization (2008, see note 5).
- 21.Alsibiani S.. Rouzi A.. “Sexual function in women with female genital mutilation,”. Chibber R., El-Saleh E., El Harmi J.. “Female circumcision: Obstetrical and psychological se-quelae continues unabated in the 21st century,”. Kizilhan J.. “Impact of psychological disorders after female genital mutilation among Kurdish girls in northern Iraq,”. Fertility and Sterility. Journal of Maternal-Fetal and Neonatal Medicine. European Journal of Psychiatry. 2010;2011;2011;932425(3)(6)(2):722–724. 833–836. and. 92–100; Talle (see note 17); World Health Organization (2008, see note 5). [Google Scholar]
- 22.Berg R., Underland V., Odgaard-Jensen J.. “Effects of female genital cutting on physical health outcomes: A systematic review and meta-analysis,”. BMJ Open. 2014;4(11) doi: 10.1136/bmjopen-2014-006316. et al., p. e006316; World Health Organization (2016, see note 7). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Berg et al. (see note 22); World Health Organization (2016, see note 7).
- 24. Berg et al. (see note 22); World Health Organization (2016, see note 7).
- 25. Berg et al. (see note 22); World Health Organization (2016, see note 7).
- 26. Berg et al. (see note 22); World Health Organization (2016, see note 7); WHO (2008, see note 5).
- 27. World Health Organization (2008, see note 5).
- 28. World Health Organization (2016, see note 7).
- 29.Abdulcadir J., Rodriguez M.. Say L.. “A systematic review of the evidence on clitoral reconstruction after female genital mutilation/cutting,”. Ali A.. “Knowledge and attitudes of female genital mutilation among midwives in Eastern Sudan,”. Vissandjée B., Denetto S., Migliardi P.. Proctor J.. “Female genital cutting (FGC) and the ethics of care: Community engagement and cultural sensitivity at the interface of migration experiences,”. International Journal of Gynecology and Obstetrics. Reproductive Health. BMC International Health and Human Rights. 2015;2012;2014;129914(2)(1)(1):9397. 23, 13. and. p. and. p. [Google Scholar]
- 30. Ali (see note 29).
- 31.Terry L.. Harris K.. “Female genital mutilation: A literature review,”. Nursing Standard. 2013;28(1):41–47. doi: 10.7748/ns2013.09.28.1.41.e7750. and. [DOI] [PubMed] [Google Scholar]
- 32. Abdulcadir et al. (see note 29).
- 33. Ali (see note 29).
- 34. Ibid.
- 35. UNICEF (2013, see note 9).
- 36. Terry and Harris (see note 31).
- 37.Dunn F.. “Is it possible to end female circumcision in Africa?”. Clinical Journal of Obstetric Gynecology. 2018;1:7–13. [Google Scholar]
- 38.Shah P.. “Cutting female genital mutilation from the United States: A European-influenced proposal to alter state and federal legal responses when affording relief to Somali victims in Minnesota,”. Cardozo Journal of Law and Gender. 2015;22:583. p. [Google Scholar]
- 39. Ibid.
- 40. Ibid.
- 41. World Health Organization (2008, see note 5).
- 42. Goldberg et al. (see note 11); World Health Organization (2008, see note 5).
- 43. Universal Declaration of Human Rights, G.A. Res. 217A (III) (1948), art. 3.
- 44. Shah (see note 38).
- 45.Broussard P.. “The importation of female genital mutilation to the West: The cruelest cut of all,”. University of San Francisco Law Review. 2009;44:787. p. Shah (see note 38). [Google Scholar]
- 46. Broussard (see note 45); Shah (see note 38).
- 47. Convention on the Elimination of All Forms of Discrimination against Women, G.A. Res. 34/180 (1979).
- 48. Shah (see note 38).
- 49. World Health Organization (2008, see note 5).
- 50. Convention on the Rights of the Child, G.A. Res. 44/25 (1989).
- 51. World Health Organization (2008, see note 5).
- 52. Ibid.
- 53. Ibid.
- 54. Ibid.
- 55.Nour N.. “Female genital cutting: A persisting practice,”. Salihu H., August E., Salemi J.. “The association between female genital mutilation and intimate partner violence,”. Reviews in Obstetrics and Gynecology. BJOG: An International Journal of Obstetrics and Gynaecology. Lancet. 2008;2012;2007;1119369(3)(13)(9567):135. 1069–1070. p. et al., pp. 1597–1605; W. Waka-bi, “Africa battles to make female genital mutilation history,”. [PMC free article] [PubMed] [Google Scholar]
- 56.Berer M.. “The history and role of the criminal law in anti-FGM campaigns: Is the criminal law what is needed, at least in countries like Great Britain?”. Reproductive Health Matters. 2015;23(46):145–157. doi: 10.1016/j.rhm.2015.10.001. UNICEF (2013, see note 9). [DOI] [PubMed] [Google Scholar]
- 57. Berer (see note 56).
- 58. Ibid.; UNICEF (2013, see note 9).
- 59. World Health Organization (2008, see note 5).
- 60. UNICEF (2013, see note 9).
- 61.Muteshi J., Miller S.. Belizán J.. “The ongoing violence against women: Female genital mutilation/cut-ting,”. Reproductive Health. 2016;13(1):44. doi: 10.1186/s12978-016-0159-3. and. p. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Dunn (see note 37).
- 63. Ibid.
- 64.Bunei E.. Rono J.. “A critical understanding of resistance to criminalization of female genital mutilation in Kenya,”. Palgrave Handbook of Criminology and the Global South. 2018:901–912. and. [Google Scholar]
- 65.Green E.. “Culture conflict between moonshiners and the government: An explanation of jury nullification and Nolle Prosequi in illicit alcohol offenses in rural communities,”. International Journal of Rural Criminology. 2016;3(1):50–57. [Google Scholar]
- 66.Dagistanli S.. “In defence of culture? Radicalised sexual violence and agency in legal and judicial narratives,”. International Journal for Crime, Justice and Social Democracy. 2015;4(3):57–72. [Google Scholar]
- 67.Waigwa S., Doos L., Bradbury-Jones C.. Taylor J.. “Effectiveness of health education as an intervention designed to prevent female genital mutilation/cutting (FG-M/C): A systematic review,”. Reproductive Health. 2018;15(1):62. doi: 10.1186/s12978-018-0503-x. and. p. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Babalola S., Brasington A., Agbasimal A.. “Impact of a communication programme on female genital cutting in eastern Nigeria,”. Tropical Medicine and International Health. 2006;11(10):1594–1603. doi: 10.1111/j.1365-3156.2006.01701.x. et al., [DOI] [PubMed] [Google Scholar]
- 69. Waigwa et al. (see note 67).
- 70.Boyle E.. Corl A.. “Law and culture in a global context: Interventions to eradicate female genital cutting,”. Annual Review of Law and Social Sciences. 2010;6:195–215. and. [Google Scholar]
- 71.Mohamud M., Kaba M.. Tamire M.. “Assessment of barriers of behavioral change to stop FGM practice among women of Kebri Beyah district, Somali regional state, eastern Ethiopia,”. Global Journal of Medical Research. 2017 and. [Google Scholar]
- 72.Asekun-Olarinmoye E., Amusan O.. “The impact of health education on attitudes towards female genital mutilation (FGM) in a rural Nigerian community,”. European Journal of Contraception and Reproductive Health Care. 2008;13(3):289–297. doi: 10.1080/13625180802075174. [DOI] [PubMed] [Google Scholar]
- 73.Diop N.. Askew I.. “The effectiveness of a community-based education program on abandoning female genital mutilation cutting in Senegal,”. Study in Family Planning. 2009;40(4):307–318. doi: 10.1111/j.1728-4465.2009.00213.x. and. [DOI] [PubMed] [Google Scholar]
- 74. Waigwa et al. (see note 67).
- 75. Ibid.
- 76.Varol N., Hall J., Black K., Turkmani S.. Dawson A.. “Evidence-based policy responses to strengthen health, community and legislative systems that care for women in Australia with female genital mutilation/cutting,”. Shell-Duncan B., Wander K., Hernlund Y.. Moreau A.. “Legislating change? Responses to criminalizing female genital cutting in Senegal,”. Reproductive Health. Law and Society Review. 2017;2013;1447(1)(4):63. 803–835. doi: 10.1186/s12978-017-0324-3. and. p. and. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Mohamud et al. (see note 71).
- 78.Costello S., Quinn M., Tatchell A.. ”A tradition in transition: Female genital mutilation/cutting; A literature review, an overview of prevention programs and demographic data for Victoria, Australia,”. Family Planning Victoria. 2014 et al., [Google Scholar]
- 79. Mohamud et al. (see note 71).
- 80.Kafatos F.. “Changing culture to end FGM,”. Lancet. 2018;391(10119):401. doi: 10.1016/S0140-6736(18)30151-X. p. [DOI] [PubMed] [Google Scholar]
- 81. Ibid.
- 82.Dalal K., Kalmatayeva Z., Mandal S.. “Adolescent girls’ attitudes toward female genital mutilation: A study in seven African countries,”. F1000Research. 2018;7 doi: 10.12688/f1000research.14142.1. et al., [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Afifi M.. “Women’s empowerment and the intention to continue the practice of female genital cutting in Egypt,”. Archives of Iranian Medicine. 2009;12(2) [PubMed] [Google Scholar]
- 84. Mohamud et al. (see note 71).
- 85.Varol N., Turkmani S., Black K.. “The role of men in abandonment of female genital mutilation: A systematic review,” . BMC Public Health. 2015;15(1):1034. doi: 10.1186/s12889-015-2373-2. et al., p. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86. Ibid.
- 87.About us. Global Alliance Against Female Genital Mutilation, Available at http://www.global-alliance-fgm.org/en-gb/aboutus.aspx.
- 88. Varol et al. (2015, see note 85).
- 89. Muteshi et al. (see note 61).
- 90. Ibid.
- 91.Berg R.. Denison E.. “Effectiveness of interventions designed to prevent female genital mutilation/cutting: A systematic review,”. Varol N., Fraser I., Ng C.. “Female genital mutilation/cutting: Towards abandonment of a harmful cultural practice,”. Studies in Family Planning. Australian and New Zealand Journal of Obstetrics and Gynaecology. 2012;2014;4354(2)(5):135–146. 400–405. doi: 10.1111/j.1728-4465.2012.00311.x. and. et al., [DOI] [PubMed] [Google Scholar]