

Abstract
Patient: Male, 20
Final Diagnosis: Anorexia nervosa with gelatinous transformation of bone marrow
Symptoms: Bradycardia • generalized weakness • weigh loss
Medication: —
Clinical Procedure: —
Specialty: General and Internal Medicine
Objective:
Rare disease
Background:
Anorexia nervosa is a relatively frequently encountered eating disorder. Beyond its psychiatric significance, it is associated with multiple hematological features such as cytopenia. It can be related to gelatinous transformation of the bone marrow.
Case Report:
We describe the case of a 20-year-old male admitted for rapid involuntarily weight loss. He presented with extreme bradycardia with a heart rate of 30 beats per minute with recent psychomotor impairment. Routine laboratory tests showed pancytopenia, and cytolysis on liver function tests. Cardiac investigations did not reveal abnormalities except for sinus bradycardia. Bone marrow aspirate revealed hypo-cellular marrow with infiltration by gelatinous substance. In addition, bone marrow biopsy showed fat cell atrophy along with loss of hematopoietic elements in areas of gelatinous transformation. During the patient’s hospital stay, he had a restrictive oral diet. Thus, after consulting with a psychiatric specialist, a diagnosis of anorexia nervosa complicated with gelatinous transformation of bone marrow, bradycardia, and acute hepatitis was made. After psychiatric treatment and nutritional care, the patient regained weight, had a normal heart rate and normal liver function tests, and his full blood count and bone marrow examination were within normal range.
Conclusions:
Gelatinous transformation of bone marrow can be the revealing feature of anorexia nervosa and some potentially reversible associations might prove life threatening if misdiagnosed. Furthermore, lack of suspicion can lead to unwarranted investigations increasing the cost incurred in healthcare delivery. Our patient had 3 systems involved: cardiac, hepatic, and hematological systems. Gelatinous transformation of bone marrow, although a rare condition, must be considered in such patients.
MeSH Keywords: Anorexia Nervosa, Bone Marrow Diseases, Bradycardia, Hepatitis
Background
Anorexia nervosa is a frequently encountered eating disorder that can be associated with various organic manifestations such as cardiac involvement in 80% of patients; liver involvement reported in up to 76% of patients; musculoskeletal problems such as reduced bone density; endocrine abnormalities, and hematological changes [1–4]. Hematological involvement usually features anemia (40%), leukopenia (30%), and thrombocytopenia in about 10% of patients [5]. However, bicytopenia and pancytopenia can also be observed, especially in cases of gelatinous transformation of the bone marrow [6]. Gelatinous transformation of bone marrow, also known as starvation marrow or serous atrophy, requires careful histological study of the bone marrow. This diagnosis was first established in a patient suffering from starvation, which has similar consequences to anorexia nervosa [7,8].
We report the case of a young male presenting with weight loss and bradycardia, along with abnormal liver test results and pancytopenia on preliminary laboratory investigations, who was diagnosed with anorexia nervosa complicated by gelatinous transformation of bone marrow and acute hepatitis, and who recovered completely after treatment.
Case Report
A 20-year-old male with no medical history was admitted in our Internal Medicine Department for extreme weight loss and generalized weakness. Patient reported involuntarily weight loss amounting to 47 kg during the last 6 months. He denied usage of licit or illicit toxic substances and any drug intake.
On clinical examination, the patient weighted 50 kg with a normal body mass index of 22 kg/m2. He presented with slight amyotrophy. He had a psychomotor impairment, which was reported to be recent by his family. Keratoconjunctivae were pale. Extreme bradycardia was noted with a heart rate of 30 beats per minute (bpm) and his blood pressure was stable at 85/60 mm Hg with no orthostatic change. General examination was essentially normal with no generalized lymphadenopathy. Electrocardiogram confirmed bradycardia with a sinus rhythm of 33 bpm with no conduction disorder.
Full blood count showed pancytopenia: white blood cell count was 2300/mL (4000–10 000/mL) with neutrophil count of 1200/mL (2000–7000/mL), hemoglobin of 9 g/dL (13–18 g/dL) with a mean corpuscular volume of 102 fL (80–100 fL), and a platelet count of 70 000/mL (150 000–450 000/mL). Cytolysis was noted in liver tests with both aspartate transaminase and alanine transaminase elevated respectively at 240 UI/L (normal range: 5–34 UI/L) and 290 UI/L (normal range: <55 UI/L).
No cholestasis was noted and bilirubin was within normal range. Albumin serum level was low at 30 g/L (35–45 g/L). There was no laboratory evidence of inflammation or hemolysis. Blood smear did not reveal the presence of schistocytes. Lactate dehydrogenase level was normal. Renal and thyroid function tests, cholesterol serum level, and phosphate-calcium balance were within normal range. Prothrombin time was normal, and proteinuria was negative. Folate and B12 vitamin serum level were also within normal range.
Echocardiography and cardiac stress tests were normal. Rhythm Holter monitoring showed no abnormalities except for bradycardia. During the patient’s hospital stay, it was noted that he had restricted oral diet. Thus, a psychiatric opinion was requested, and anorexia nervosa was highly suspected. Given the pancytopenia and liver test abnormalities, infectious investigations were carried out. Serologies of hepatitis B, hepatitis C, cytomegalovirus, and leishmaniasis were negative. Tuberculin skin test as well as sputum and urine examination did not show evidence of tuberculosis. Immunologic workup showed negative antinuclear antibodies and negative rheumatoid factor. Considering the possibility of lymphoma, a full body computed tomography was performed, yet it did not yield any remarkable findings. Bone marrow aspiration revealed hypo-cellular marrow with infiltration by gelatinous substance. Bone marrow biopsy was performed and showed gelatinous transformation of the bone marrow with fat cell atrophy and loss of hematopoietic cells (Figures 1, 2). Cytokeratin, CD20, and CD3 immunohistochemistry did not show neoplastic cells. Diagnosis of gelatinous transformation of bone marrow complicating anorexia nervosa was retained. Liver function disorders and bradycardia were also associated with anorexia nervosa. The patient was discharged and referred to the psychiatric department where he was initiated on supervised oral diet. After 2 months, at the follow-up consultation, the patient had regained 27 kg, had a heart rate of 67 bpm and his peripheral blood count was normal. Also, his liver function tests were normalized. A control bone marrow examination was performed which confirmed complete regression of all abnormalities.
Figure 1.
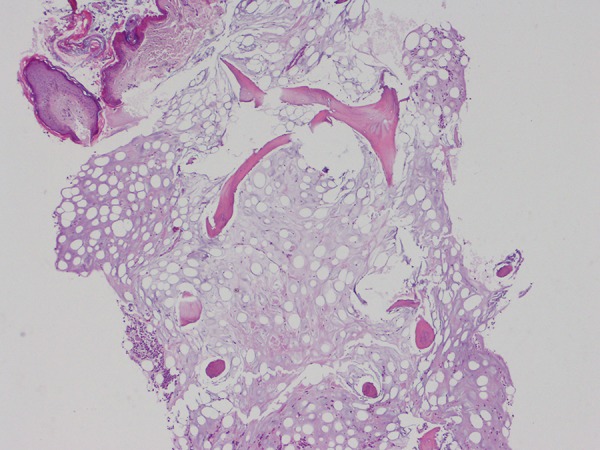
Histopathological features of the bone marrow combining an atrophy of fat cells and a loss of hematopoietic cells; hematoxylin and eosin, 40×.
Figure 2.
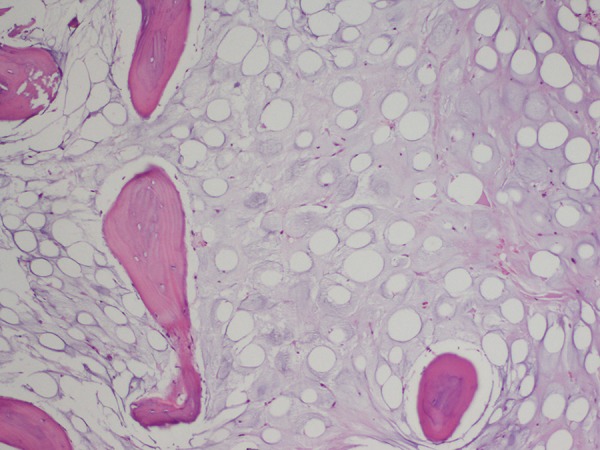
Marrow fat cells being surrounded by an extracellular homogeneous fibrillary pale material; hematoxylin and eosin, 200×.
Discussion
Anorexia nervosa, as a psychiatric disease, can have many organic presentations [6]. It can present with cardiac complications, with bradycardia being the most common [1]. Gastrointestinal involvement can also be observed such as dysphagia, hepatitis, and constipation [2]. It can also be responsible for amenorrhea, hypoglycemia, and other endocrine symptoms as well as various hematological changes like anemia, leukopenia, and thrombocytopenia, which can be related to gelatinous transformation of the bone marrow [3,5]. Out of the aforementioned complications, our patient presented with symptoms indicating involvement of 3 different systems.
The reported frequency of gelatinous transformation of bone marrow varies from 0.2% to 4.8% [8,9]. The increased number of case reports published in the last 2 decades point to the possibility of under diagnosis or missed diagnosis [8]. It is usually observed in young males [9]. Diagnosis can be suspected on the basis of peripheral blood count with the common presentation being bicytopenia or pancytopenia. However, no correlation between the peripheral hematological parameters and the severity of the bone marrow gelatinous transformation has been reported [10]. Only histological examination allows for the diagnosis. It highlights the presence of focal loss of hematopoietic cells associated with adi-pose cells atrophy and extracellular gelatinous substance infiltration [11]. This extracellular ground substance is usually amorphous, sometimes slightly granular and consists of acid mucopolysaccarides that stain positive with Alcian blue at pH 2.5 [12]. Physiopathology of gelatinous bone marrow transformation is still to be elucidated. It might be related to depletion of adipocyte cells due to important catabolism followed by the disposition of hyaluronic acid thus creating an unfavorable microenvironment for erythropoiesis [13]. Exact etiology of this condition remains unclear. Many underlying diseases have been reported to be associated with this condition, such as severe malnutrition, anorexia nervosa, acquired immuno-deficiency (AIDS), chronic infections, alcoholism, systemic lupus erythematosus, and elderly patients with lymphoma, carcinoma, and congestive heart failure [14]. One of the predominant risk factors seems to be the degree of weight loss more than the weight itself [15]. Such was observed in our case report as our patient had a body mass index of 22 kg/m2 yet he still lost over 40 kg in 6 months.
Our patient also presented with acute hepatitis. This can frequently be observed in anorexia nervosa cases; the American Psychiatric Association even recommends systematic checks of liver function in patients suffering from this disease [16]. Just like gelatinous transformation of bone marrow, this also is related to the degree of weight loss [14]. Cytolysis is observed more frequently than cholestasis. This disorder is secondary to hepatocyte autophagy due to severe caloric restriction [2].
Bradycardia is frequent found in association with anorexia nervosa. This condition can be associated with other cardiac complications in 80% of patients. It can be associated with pericardia effusion and mitral valve prolapse thus earning it the highest rate of mortality in a psychiatric disorder [1]. In our patient case, cardiac investigation did not reveal abnormalities other than sinus bradycardia.
Most disorders observed in anorexia nervosa are usually reversible upon correction of the nutritional balance, which must be associated with psychiatric care. This requires physicians to consider the various organic complications to ensure appropriate treatment. Gelatinous transformation of the bone marrow can sometimes be more challenging to treat, requiring the use of hematopoietic growth factors [17]. In our report, psychiatric support with a balanced oral diet allowed for complete regression of previous abnormalities.
Conclusions
Gelatinous transformation of the bone marrow can be the revealing feature of anorexia nervosa and some potentially reversible associations may prove life threatening if misdiagnosed. Further, lack of suspicion can lead to unwarranted investigations increasing the cost incurred in healthcare delivery. We reported a case involving 3 systems: cardiac, hematologic, and hepatic. Gelatinous transformation of the bone marrow must be considered in cases of unexplained hematological disorder in patients presenting with important weight loss, given the potential reversibility of the condition.
Footnotes
Conflict of interest
None.
References:
- 1.Spaulding-Barclay MA, Stern J, Mehler PS. Cardiac changes in anorexia nervosa. Cardiol Young. 2016;26(4):623–28. doi: 10.1017/S104795111500267X. [DOI] [PubMed] [Google Scholar]
- 2.Gaudiani JL, Sabel AL, Mascolo M, Mehler PS. Severe anorexia nervosa: Outcomes from a medical stabilization unit. Int J Eat Disord. 2012;45(1):85–92. doi: 10.1002/eat.20889. [DOI] [PubMed] [Google Scholar]
- 3.Lo Sauro C, Ravaldi C, Cabras PL, et al. Stress, hypothalamic-pituitary-adrenal axis and eating disorder. Neuropsychobiology. 2008;57:95–101. doi: 10.1159/000138912. [DOI] [PubMed] [Google Scholar]
- 4.Kraeft JJ, Uppot RN, Heffess A. Imaging findings in anorexia nervosa. Am J Roentgenol. 2013;200:328–34. doi: 10.2214/AJR.12.9641. [DOI] [PubMed] [Google Scholar]
- 5.Hutter G, Ganepola S, Hofmann WK. The hematology of anorexia nervosa. Int J Eat Disord. 2009;42:293–300. doi: 10.1002/eat.20610. [DOI] [PubMed] [Google Scholar]
- 6.Boullu-Ciocca S, Darmon P, Sébahoun G, et al. Transformation gélatineuse de la moelle au cours de l’anorexie mentale. Ann Endocrinol. 2005;66(1):7–11. doi: 10.1016/s0003-4266(05)81680-4. [in French] [DOI] [PubMed] [Google Scholar]
- 7.Michael P. Gelatinous degeneration of the bone marrow. J Pathol Bacteriol. 1930;33(3):533–38. [Google Scholar]
- 8.Shergill KK, Shergill GS, Pillai HJ. Gelatinous transformation of bone marrow: Rare or underdiagnosed? Autops Case Rep. 2017;7(4):8–17. doi: 10.4322/acr.2017.039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Singh S, Gupta M, Singh G, et al. Gelatinous transformation of bone marrow: A prospective tertiary centre study, indicating varying trends in epidemiology and pathogenesis. Indian J Hematol Blood Transfus. 2016;32(Suppl. 1):358–60. doi: 10.1007/s12288-015-0514-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Das S, Mishra P, Kar R, Basu D. Gelatinous marrow transformation: A series of 11 cases from a tertiary care centre in South India. Turk J Haematol. 2014;31(2):175–79. doi: 10.4274/Tjh.2012.0151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Munfus DL, Menke DM. Case of severe serous fat atrophy. Mayo Clin Proc. 2009;84(7):570. doi: 10.1016/S0025-6196(11)60743-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Travlos GS. Histopathology of the bone marrow. Toxicol Pathol. 2006;34:566–98. doi: 10.1080/01926230600964706. [DOI] [PubMed] [Google Scholar]
- 13.Osgood E, Muddassir S, Jaju M, et al. Starvation marrow – gelatinous transformation of bone marrow. J Community Hosp Intern Med Perspect. 2014;4(4) doi: 10.3402/jchimp.v4.24811. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Rivièrea E, Pillot J, Saghi T, et al. [Gelatinous transformation of the bone marrow and acute hepatitis in a woman suffering from anorexia nervosa] Rev Med Interne. 2012;33(7):e38–40. doi: 10.1016/j.revmed.2011.11.011. [in French] [DOI] [PubMed] [Google Scholar]
- 15.Abella E, Feliu E, Granada I, et al. Bone marrow changes in anorexia nervosa are correlated with the amount of weight loss and not with other clinical findings. Am J Clin Pathol. 2002;118(4):582–8. doi: 10.1309/2Y7X-YDXK-006B-XLT2. [DOI] [PubMed] [Google Scholar]
- 16.American Psychiatric Association Treatment of patients with eating disorders, third edition. Am J Psychiatry. 2006;163(7 Suppl.):4–54. [PubMed] [Google Scholar]
- 17.Charania RS, Kern WF, Charkrabarty S, Holter J. Successful management of gelatinous transformation of the bone marrow in anorexia nervosa with hematopoietic growth factors. Int J Eat Disord. 2011;44:469–72. doi: 10.1002/eat.20833. [DOI] [PubMed] [Google Scholar]