

Abstract
Background:
Access to health care is important for persons with disability (PwD). The Government of India has launched the “Accessible India Campaign” (AIC) as a nationwide campaign for achieving universal accessibility for PwDs.
Objective:
To conduct an on-site assessment for physical accessibility of all primary health care centers (PHCs) of Dakshina Kannada (DK) district in Karnataka using the AIC checklist.
Materials and Methods:
A cross-sectional facility-based assessment of all 67 PHCs under the administrative control of the District Health and Family Welfare Office of the district was done using Physical Accessibility Audit Checklist prepared by the AIC. Ethics approval was obtained from the Institutional Ethics Committee and written permission was obtained from the District Health and Family Welfare Officer. Data were analyzed for frequencies and percentages.
Results:
The Accessible India Physical Accessibility Audit Checklist consists of more than116 numbers of items. Out of 67 PHCs, 57 (85%) PHCs had an accessible pathway and 60 (90%) PHCs had a ramp for wheelchair. Only 25 (36%) PHCs had accessible doors. No PHCs had height-adjustable examination table, disable friendly toilets and only two PHCs had accessible weighing scales.
Conclusion:
This unique on-site assessment finds that our PHCs are not well equipped for catering to PwD. To realize AIC in terms of health care access for the PwD, there is much that remains desirable at primary health care level, a point of first contact in the public health system.
Keywords: Accessibility, accessible India campaign, persons with disability, primary health care
Introduction
Universal access and barrier-free environment is critical for equal opportunity and independent living in an inclusive society. Accessibility of physical environment is important for everyone including for persons with disabilities (PwDs). Persons with Disabilities (Equal Opportunities, Protection of Rights and Full Participation) Act, 1995 under Sections 44, 45, and 46 categorically provides for non-discrimination in transport, non-discrimination on the road, and non-discrimination in built environment, respectively.[1] India was a signatory of United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) organized in 2006 to formulate and strengthen policies, laws, and administrative measures for securing the rights of PwD.[1,2] These include information, transportation, physical environment, communication technology, and accessibility to all services including emergency services. And these are also the target areas of the Accessible India Campaign (AIC).[2] The AIC has been launched in India since December 2015 as a nationwide flagship campaign for achieving universal accessibility for PwDs and to create an enabling and barrier-free environment.[2]
Global prevalence of some form of disability is about 15%, of which 110–190 million adults have significant functional disability.[3] This varies significantly in between and within countries. The access to health care in PwD is mainly hindered due to either prohibitive costs or limited availability of appropriate services.[3] The prevalence of disability is 2.21% in India, 2.16% in Karnataka, and 1.34% in Dakshina Kannada district.[4] This transforms to more than 27 million people in terms of absolute numbers in the country.
Primary health care is an essential health care, based on practical, scientifically sound, and socially acceptable methods and technology made universally accessible to individuals and families in the community.[5] PwD are integral part of these communities and primary health care centers (PHCs) that are not disable friendly can be deterrent to about 2% of these community members in accessing basic health services.
Accessibility issues in PwD have been studied using qualitative interviews and focus groups discussions in past. Individuals with disabilities report a number of problems and experiences that prevent their right to access basic health care services.[6] But on-site assessment of health facilities for accessibility audit of health facilities has not been studied in India or similar countries abroad.[6]
The objective of the present study was an on-site assessment of physical accessibility of PHCs for the PwDs using the checklist provided by the AIC.[7]
Materials and Methods
Study area, sample size, and sampling
This cross-sectional study was conducted in all the 67 functioning PHCs of Dakshina Kannada district, Karnataka state, India. The district lies between 12.57′ and 13.50 ′ North latitude and 74 and 7550′ East latitude on the west coast of Southern India with a geographical area of 4,859 km2. The total population of the district is 20,89,649 (Census India, 2011). The public health infrastructure of the district consists of one district hospital, eight sub-district hospitals, and sixty seven PHCs.
Data collection and analysis
All PHCs were physically visited by principal investigator from November 2016 to January 2017. Data collection was done using the Physical Accessibility Audit Checklist prepared by the AIC.[2,7] The data were entered and analyzed using the Microsoft excel for percentages and proportions.
Ethics issues
Institutional ethics clearance was obtained along with a waiver of consent as no human participants were involved. Required permissions were obtained from the Office of the District Health and Family Welfare Department of Dakshina Kannada district.
Results
The results of the audit are described under broad categories: parking and exterior access, accessible entrance and internal environment, doors and doorways, and accessible toilet as described in Table 1. The findings that were universally absent in all the PHCs have not been described in the table. The exhaustive list of more than 116 variables is available for reference.[7]
Table 1.
Key findings of accessibility audit of the primary health centers, Dakshina Kannada district, India, 2017
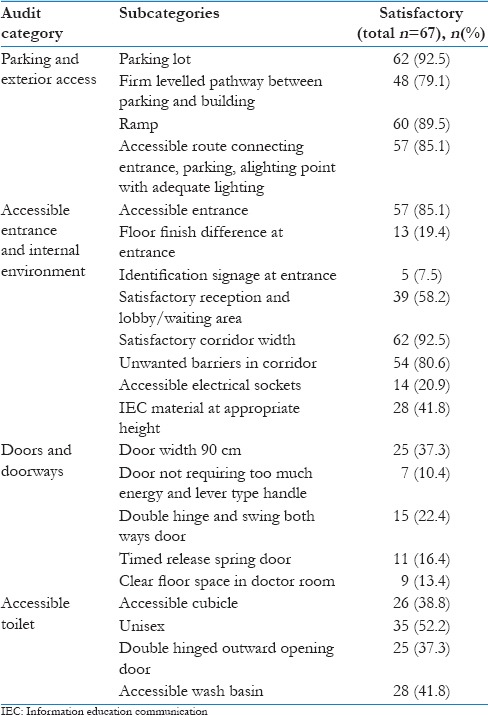
Parking and exterior access
There are 24 indicators in this category. Sixty two (92.5%) of the PHCs had parking area of required size, but none of the PHCs had reserved parking bays for PwD. 48 (71%) PHCs had firm, covered, leveled pathway minimally 4 ft wide connecting parking area with main entrance. However, none of the PHCs had tactile floor guidance (TFG), reserved parking area for PwD, signage, and shelter in the parking area. Sixty PHCs (90%) had a ramp for using wheelchairs of PwD.
Accessible entrance and internal environment
There are 31 indicators in this assessment. Fifty seven (85%) of PHCs had accessible entrance, but only five (7.5%) had accessible identification signage. None of the PHC staffs were trained in a sign language. Sixty two (92.5%) of the PHCs had corridors that were 4 ft wide, but 54 (80.6%) had various types of barriers including furniture, ornamental plants, and so on. While 39 (58.2%) PHCs had adequate space for turning the wheelchair, only 28 (41.8%) had health education material at a height accessible to PwDs. Electrical sockets at accessible height were present in only 14 (20.9%) primary health centers. Multiple questions about stairs, ramps, handrails, and lifts were not assessed as the PHCs were all situated on the ground floor.
Doors, doorways, and medical examination
Only 25 (37.3%) PHCs had accessible doors for PwD where the minimum width is 90 cm, very few (7, 10.4%) had lever type handle for doors. Double-hinged doors (15, 22.4%) that swing both ways and time-released spring (11, 16.4%) were other factors missing in most PHCs. None had kick plates, height adjustable examination table and only two PHCs had accessible weighing scales.
Accessible toilet
While 62 (92.5%) of the PHCs did not have an accessible toilet door, only 26 (38.8%) PHCs had accessible cubicle with appropriate dimensions for PwD. There were unisex toilets in 52% PHCs. All the facilities had squatting type of toilets with no western commode (WC). Twenty eight (41.8%) had accessible wash basin for hand washing. Many requirements such as color contrast scheme for floor, wall and sanitary fittings, alarm system, height of mirror, toilet accessories, and placement of flush were absent in all the toilets.
Discussion
This study gives the current situation about disability preparedness of PHCs in Dakshina Kannada district of Southern India. To the best of our knowledge, there have been no studies that have been done so far to study this aspect in the Indian subcontinent. The results of this facility-based study identified that PHCs are not fully geared towards the fulfillment of the needs of PwD. The AIC audit checklist is a long one with many questions and variables, unlikely to be fulfilled even in secondary and tertiary level health care facilities. Hence, we have assessed and discussed some of the starkest findings in this study. We discuss the findings of the study with respect to the larger context of various initiatives in the country. Lack of comparable studies in the country and abroad makes it difficult to compare or contrast the results of the present study.
Indian public health standards (IPHS) have been framed by the National Health Mission that guides the requirements of public health facilities. But the standards themselves have not included any specific requirements of PwD except ramp and hand rails. Guidelines have not addressed important issues like accessibility of entrance, corridor, out-patient consultation room, toilets, need for height adjustable examination table, and height at which the health education material on the wall should be located.[8] The IPHS guidelines came much before the AIC checklist was framed. Hence, it is necessary to incorporate accessibility standards in the IPHS guidelines in the next revision.
Many questions such as color contrast scheme for floor, door frame, wall and sanitary fittings in toilet, alarm system, height of mirror in toilet, toilet accessories, and placement of flush were inappropriate to assess as none of the toilets had even a minimum requirement of a WC.
The World Bank report identifies the following factors as the driving forces for reduced access to care among the PwD: poor disability identification and certification system, poor awareness among the PwD, attitude of health system and the community towards them, and financial barriers.[9] These are worse in rural areas and the report stresses the need to make built-up environment in public health facilities appropriate for PwD. In South India Disability Evidence (SIDE) study, it was reported that there are higher rates of past hospitalizations, higher risk of diabetes and depression with significant barriers to accessing health services.[10] In a community-based survey in Karnataka, South India, the prevalence of disability was almost 6% and around 50% of PwD received some medical or surgical services,[11] while there others in the same region have found the access to health services to be as low as 2%–3%.[12] This problem can be even more acute in elderly population where locomotion is significantly affected.[13]
While there are no similar studies in past in India to rate the improvement in accessibility, a similar study in California primary health centers in 2012 found accessible weighing scale in 3.6% and a height adjustable examination table in 8.4% of the PHCs.[14] Another study in Brazil where accessibility audit of toilet facilities in 157 PHCs was done found that the doorway width to allow a wheelchair access was inadequate in 77.7% PHC toilets.[15] In a qualitative exploration of accessibility aspects of PwD in primary health care system of Nepal, transportation and physical environment such as ramps, accessible treatment rooms, and mobility devices were pointed out by the health care providers as important barriers.[16]
Primary health centers are the first point of contact for health in rural in remote places in India and these are the least equipped to handle PwD at present. Unfortunately, this aspect does not figure in any significant manner in the AIC website and the mass media awareness material. This needs particular attention as one of the objectives of the campaign is to conduct an accessibility audit of 50 most important government buildings in 50 cities of the country and convert them into fully accessible buildings by July 2016.[2] As of now, no public updates are available on this website regarding the progress in this aspect. A balance needs to be created when resources are allocated so that accessibility is addressed not only in the cities, but also in remote and rural areas. The issue of access is especially important in rural areas where presently the access is challenging not only for the disabled but also for the able-bodied individuals.
The checklist that has been adapted for the AIC is a very elaborate one.[7] It seems to be adapted from criteria prepared by more developed countries. Many sections in it are out of sync with reality on the ground and have terminologies not commonly used in India. The country is very vast with huge disparities between states and within states, between urban and rural areas. Hence “one size fits all” will not work. We require a more pragmatic checklist tailored according to the local needs and availability of resources.
Conclusion
The present study indicates that ramps, railings, wheelchairs, tactile paths, toilets, and signage are important barriers to accessibility in the PHCs for PwDs. Findings of the study can provide insights into a rational checklist for health care facilities at all levels of health care and future nation-wide surveys. Universal access to primary health care for the PwDs in India can be achieved by adequate prioritization as there are competing demands and limited resources.
Financial support and sponsorship
This study received a funding of Rs 20,000 (approximately 290 USD) for the logistic expenditure of field visits for accessibility audit. It was provided by NGO “Family of Disabled” New Delhi.
Conflicts of interest
There are no conflicts of interest.
References
- 1.United Nations. Convention on the Rights of Persons with Disabilities. New York: United Nations; 2006. [Last accessed on 2018 Jun 25]. Available from: http://www.un.org/disabilities/documents/convention/convention_accessible_pdf.pdf . [Google Scholar]
- 2.Accesible India Campaign. Department of Empowerment of Persons with Disabilities and Ministry of Social Justice and Empowerment. 2015. [Last accessed on 2018 Jun 25]. Available from: http://www.disabilityaffairs.gov.in/content/accessible_india.php .
- 3.World Health Organization. Disability and Health Fact Sheet. World Health Organization; 2017. [Last accessed on 2018 Jun 30]. Available from: http://www.who.int/mediacentre/factsheets/fs352/en/ [Google Scholar]
- 4.Census of India 2011. Data on Disability. Office of the Registrar General and Census Commissioner, India. 2011. [Last accessed on 2018 Jun 30]. Available from: http://www.censusindia.gov.in/2011census/Disability_Data/India/C_20.India.xls .
- 5.Alma-Ata. Declaration of Alma-Ata: International Conference on Primary Health Care. USSR; 6-12 September. 1978 [PubMed] [Google Scholar]
- 6.Mitra S, Posarac A, Vick B. Disability and poverty in developing countries: A multidimensional study. World Dev. 2013;41:1–18. [Google Scholar]
- 7.Pt. Deendayal Upadhyaya National Institute for Persons with Physical Disabilities (Divyangjan). Accessibility Audit Checklist. Department of Empowerment of Persons with Physical Disabilities. 2015. [Last accessed on 2018 Jun 25]. Available from: http://www.iphnewdelhi.in/WriteReadData/Access%20Audit%20Checklist.pdf .
- 8.Government of India. Indian Public Health Standards (IPHS) for Primary Health Centers, Directorate General of Health Services, Ministry of Health and Family Welfare, GOI; Revised. 2012. [Last accessed on 2018 May 30]. Available from: http://www.nrhm.gov.in/nhm/nrhm/guidelines/indian-public-health-standards.html .
- 9.World Bank. People with Disabilities in India: From Commitments to Outcomes. Human Development Unit, South Asia Region; July. 2009. [Last accessed on 2018 May 20]. Available from: http://www.documents.worldbank.org/curated/en/577801468259486686/pdf/502090WP0Peopl1Box0342042B01PUBLIC1.pdf .
- 10.Gudlavalleti MV, John N, Allagh K, Sagar J, Kamalakannan S, Ramachandra SS, et al. Access to health care and employment status of people with disabilities in South India, the SIDE (South India disability evidence) study. BMC Public Health. 2014;14:1125. doi: 10.1186/1471-2458-14-1125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kumar SG, Das A, Soans SJ. Quality of rehabilitation services to disabled in a rural community of Karnataka. Indian J Community Med. 2008;33:198–200. doi: 10.4103/0970-0218.42066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Thomas M, Pruthvish S. An initiative of MSRMC and WHO. Report of Ashakirana-Kaiwara CBR Programme. Bangalore: Kaiwara Community Based Rehabilitation Programme Community Based Rehabilitation of people with disabilities in Kaiwara Primary Health Centre Area. 2004 [Google Scholar]
- 13.Maroof M, Ahmad A, Khalique N, Ansari MA. Locomotor problems among rural elderly population in a district of Aligarh, North India. J Family Med Prim Care. 2017;6:522–5. doi: 10.4103/2249-4863.222055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mudrick NR, Breslin ML, Liang M, Yee S. Physical accessibility in primary health care settings: Results from California on-site reviews. Disabil Health J. 2012;5:159–67. doi: 10.1016/j.dhjo.2012.02.002. [DOI] [PubMed] [Google Scholar]
- 15.Áfio AC, de Carvalho LV, Marques JF, de Oliveira PM, de Almeida PC, Pagliuca LM. Physical accessibility for disabled people: Analysis of toilet facilities in primary health care units. Open J Nurs. 2016;6:948. [Google Scholar]
- 16.Van Hees S, Cornielje H, Wagle P, Veldman E. Disability inclusion in primary health care in Nepal: An explorative study of perceived barriers to access governmental health services. Disabil CBR Inclusive Dev. 2015;25:99–118. [Google Scholar]