

Abstract
Background:
Osteoarthritis (OA) is the most common articular disease of the developed country and cause of chronic disability, and may cause joint failure. OA is one of the most prevalent situation that gives rise to disability, especially in elderly population.
Aim:
To assess the knowledge of knee OA among general population in Aseer region.
Materials and Methods:
A cross-sectional survey was conducted in Aseer region including 1052 participants. The participants were included by visiting the public areas in different cities in Aseer region where many people of different social and economic level were available, and because of the the nature of Saudi community regarding home-to-home interviews.
Results:
The research included 1052 participants from different areas in Aseer region. The ages of participants ranged from 17 to 80 years old, with a mean age of 38 ± 12 years old. Approximately 89.0% of the sampled population had good awareness regarding preventive measures of knee OA. The second highest awareness level was recorded for relieving the measures of knee OA as 84.1% of the sampled population recorded good level of knowledge. In general, 82.6% of the population had good awareness level regarding OA in total.
Conclusions and Recommendations:
The current research revealed that the awareness of the general population in Aseer region regarding knee OA was more than satisfactory, especially for preventive measures, relieving measures, and its risk factors.
Keywords: Awareness, knee diseases, knee osteoarthritis, knowledge, osteoarthritis, population awareness
Background
Osteoarthritis (OA) is the most common articular disease of the developed country and cause of chronic disability, and may cause joint failure.[1,2] OA is one of the most prevalent situation gives rise to disability especially in elderly population.[1] Knee and hand OA more in females than males, especially after menopausal age.[3] Among the most common consequences of OA are pain and stiffness, and can lead to reduced physical activity and quality of life, and more affects the joints of knees, hands, and hips.[4] OA is classified into primary and secondary: primary OA is a gene-related disease and secondary OA occurs after a traumatic condition.[5] Supportive footwear is considered a protective factor for OA.[6] The prevalence of OA increases with age, especially after the age of 50 years.[7] In USA, OA is considered the most common joint disorder.[8] The treatment of OA are aerobic exercises, weight loss, acupuncture, glucosamine and chondroitin sulfate, and surgical.[9]
A previous attempt has been made to estimate the prevalence of knee OA in Saudi Arabia; however, that study was conducted clinically and without radiographic investigations and yielded a prevalence of 57.2% in a primary clinic setting.[10] Another study was done by Al Arfaj,[11] and the estimated prevalence of knee OA was found to be 53.3% in male and 60.9% in female patients. In addition, they found that the prevalence of radiographic knee OA increases with age. However, despite 64.3% of the patients complaining of knee joint pains, no case of radiographic OA was detected in those under 30 years old.
However, up to authors’ knowledge, no study has examined knowledge of knee OA among general population in Aseer region, which is located in the southern part of Saudi Arabia with special cultural aspects. Thus, our aim was to assess the knowledge of knee OA among general population in Aseer region.
Materials and Methods
A cross-sectional survey was conducted in Aseer region. The participants were included by visiting the public areas in different cities in Aseer region where many people of different social and economic level were available and because of the nature of Saudi community regarding home to home interviews. The included areas were Aseer Mall, Alrashed Mall, Asdaf Mall, Abha Mall, Aveneo Mall, Bisha mall, and Anamas mall. In addition, participants from Abha Airport, King Khalid University, Alsalam Park, and Alshallal Park were included. The data collection was done over a period of 6 months from January to June 2018. A self-administered questionnaire, which was valid and undergone back translation to Arabic language, has taken from previous study which was conducted in Malaysia.[6] The questionnaire covered data regarding population socio-demographics such as gender, age, education level, and occupation. Awareness of knee OA, immediate family members with knee OA, diagnosed clinically to have knee OA, risk factors, signs and symptoms, disabilities, prevention, and management were also covered.
Data analysis
After data were collected it was revised, coded, and fed to statistical software IBM SPSS version 21. The given graphs were constructed using Microsoft excel software. All statistical analysis was done using two tailed tests and alpha error of 0.05. The P value less than or equal to 0.05 was considered to be statistically significant. Descriptive statistics including frequencies and percent were used to describe the frequency of each categorical variable items. Chi-square test/Monte Carlo exact test and Fisher's exact test (if there were many small expected values) were used to test for association between population socio-demographic characteristics and their knowledge level. The knowledge level was assessed by scoring each correct answer by one point and zero for incorrect answer. The discrete scores of the different knowledge domains were summed and categorized into poor level of knowledge for those who had score less than 60% of the maximum level and good for those who had score 60% of the maximum score or more.
Results
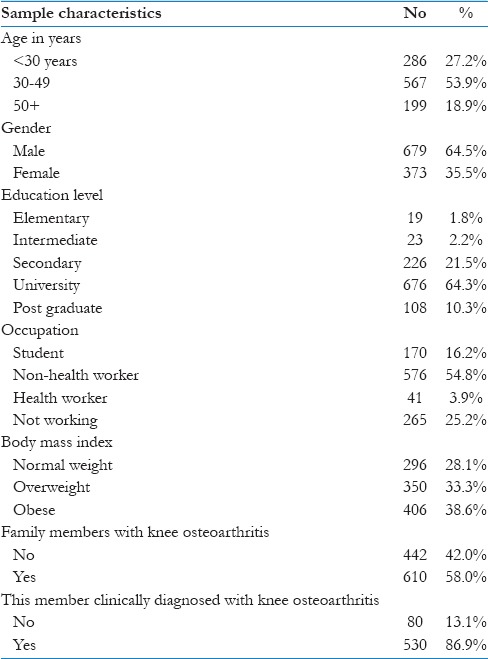
The research included 1052 participants from different areas in Aseer region. The ages of participants ranged from 17 to 80 years old with a mean age of 38 ± 12 years old. Approximately, 64% of the participants were males and 1.8% of them were of elementary level of education, while 74.6% were of university level of education or more. Students constituted 16.2% of the respondents and 3.9% of the participants were health workers, while 52.2% were non-health workers. Approximately, 39% of the participants were obese, and 28.1% were at normal weight level. Approximately, 60% of the participants had a family member with knee OA [Table 1].
Table 1.
Socio-demographic characteristics of sampled general population in Aseer region, Saudi Arabia, 2018
With regard to population awareness level regarding knee OA, Figure 1 demonstrates that 89.2% of the sampled population had good awareness level regarding preventive measures of knee OA. The second highest awareness level was recorded for relieving measures of knee OA as 84.1% of the sampled population recorded good level of knowledge. Approximately, 73% of the sampled population had good awareness level regarding OA risk factors, while only 8.9% of the participants had good level of awareness regarding consequences and disabilities of having knee OA. In general, 82.6% of the population had good awareness level regarding OA in total.
Figure 1.
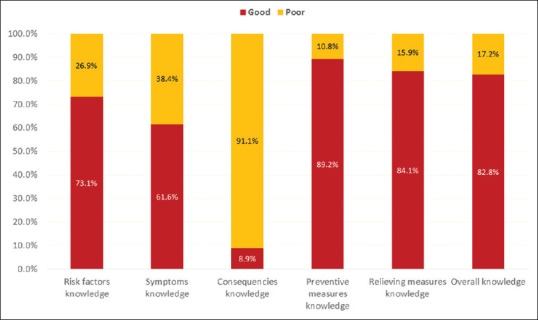
Knowledge level of general population in Aseer region regarding knee osteoarthritis, Saudi Arabia, 2018
On relating overall awareness level with the population characteristics [Table 2], it was clear that 87.4% of participants who were aged above 50 years had good awareness level compared to 79.4% of those who were below the age of 30 years with recorded statistical significance (P =0.048). In addition, 84.3% of university educated participants recorded good awareness level compared to 63.2% of those who had elementary level of education with significant difference found (P =0.050). Approximately, 97% of obese participants had good awareness level compared to 78% of normal weight population with significant difference recorded (P =.008). All other factors including gender and occupation were not significantly related with awareness level.
Table 2.
Distribution of knee osteoarthritis knowledge level by the sampled population characteristics, Aseer region, Saudi Arabia, 2018
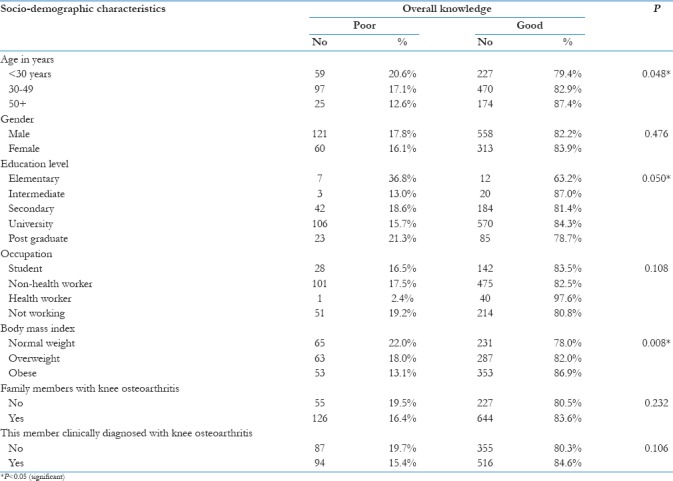
Figure 2 shows the distribution of knowledge score of the participants with their self-perceived awareness and it is clear that those who answered positively (yes) and others recorded nearly the same range of scores with nearly the same bulk (average) for both groups.
Figure 2.
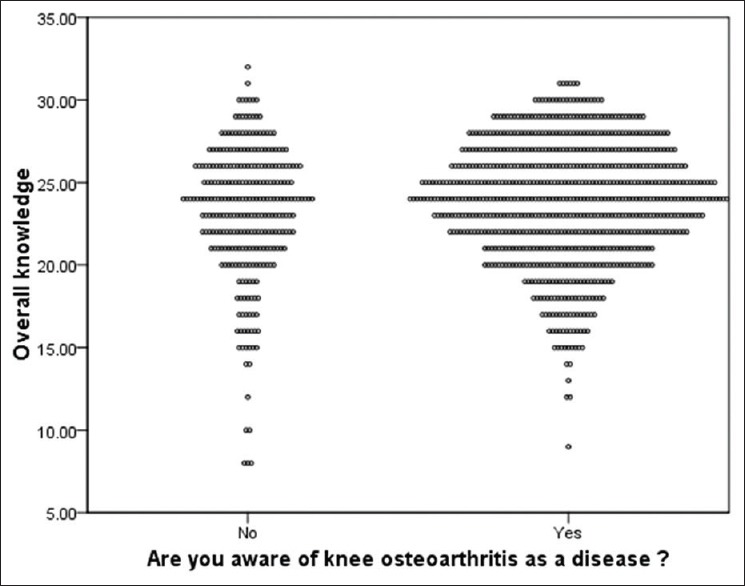
Relation between knee osteoarthritis knowledge level perceived awareness of the sampled general population, Aseer region, Saudi Arabia, 2018
Discussion
It is characterized by the breakdown of cartilage in the part of the joint that cushions the ends of bones. When cartilage breaks down, bones rub together causing pain and loss of movement. OA most often affects middle-aged and older adults. It can range from mild to severe, and most often occurs in the hands and weight-bearing joints such as the knees, hips, feet, and back.
This cross-sectional study was aimed at determining general population awareness level regarding knee OA in Aseer region, Saudi Arabia. It was clear that middle aged population with high level of education was the main core respondents and this may be because of the method of data collection, which is according to the electronic survey. The research revealed that the majority of participants were of satisfactory level of awareness regarding all aspects of knee OA such as risk factors, preventive measures, relieving measures, and symptoms. Only consequences and associated disabilities domain was not identified by the participants and this may be as a result of their age category and also disabilities with OA are not common in general. On literature review regarding OA data, data on risk factors, clinical manifestations, and available treatment options were well documented in numerous epidemiological studies and clinical trials.[8,12,13] Ganasegeran K, conducted a research on Level and Determinants of Knowledge of Symptomatic Knee OA among Railway Workers in Malaysia and found that of the 513 railway men surveyed, 53.6% reported low levels of knowledge. In addition, final regression model yielded four variables significantly influencing knee OA knowledge in this group: respondents over 50 years old, respondents previously aware of knee OA, immediate family members with knee OA, and respondents with knee OA diagnosed clinically by a doctor.[6] These findings nearly consistent with the current research especially for age factor. The current research found that age above 50 years, high education level, and obesity were the most important determinants for awareness level. Old age and obese persons are actually may have clinical experience for OA, so they recorded satisfactory awareness level. These findings were inconsistent with another study done by Abdulaziz S. Alharthi[14] focused on Awareness of OA among Saudi population and found that awareness about OA among Saudi is insufficient. To promote bone health, prevent osteoporosis, and improve the economic implications of osteoporosis, educational and awareness programs should be established targeting the whole population especially the elderly.
Study limitation
Regarding the effort made to collect and review the articles from its different areas, but the wide range made self-administered questionnaire to be the used method that may have the disadvantage of being applicable only for those who can read and interested to participate in the study. In addition, the validity of the given answers cannot be checked by this method resulting in some bias in results, but the community nature and wide area of the study setting were the barriers for using other methods.
Conclusions and Recommendations
The current research revealed that the awareness of the general population in Aseer region regarding knee OA was more than satisfactory especially for preventive measures, relieving measures, and its risk factors. The only aspect of knowledge that was defective is disabilities associated with OA. In addition, researchers concluded that older participants with some degree of overweight or obesity and educational level were more aware, while occupation and gender were of no role in awareness level. The researchers recommended that more attention should be paid for more improvement in awareness level regarding OA consequences especially among young people.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
Great acknowledgment should be provided to researchers of “Level and Determinants of Knowledge of Symptomatic Knee Osteoarthritis among Railway Workers in Malaysia” for their great contribution in the research by depending on their original questionnaire for designing our tool and validation.
We would like to thank Shahad Ahmed Asiri for her great contribution in the data collection for this paper.
References
- 1.Heidari B. Knee osteoarthritis prevalence, risk factors, pathogenesis and features: Part I. Casp J Intern Med. 2011;2:205–12. [PMC free article] [PubMed] [Google Scholar]
- 2.Bruyère O, Cooper C, Arden N, Branco J, Brandi ML, Herrero-Beaumont G, et al. Can we identify patients with high risk of osteoarthritis progression who will respond to treatment? A focus on epidemiology and phenotype of osteoarthritis. Drugs Aging. 2015;32:179–87. doi: 10.1007/s40266-015-0243-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Plotnikoff R, Karunamuni N, Lytvyak E, Penfold C, Schopflocher D, Imayama I, et al. Osteoarthritis prevalence and modifiable factors: A population study. BMC Public Health. 2015;15:1195. doi: 10.1186/s12889-015-2529-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Deleuran T, Vilstrup H, Overgaard S, Jepsen P. No increased risk for primary osteoarthritis in liver cirrhosis-A danish nationwide cohort study. PLoS One. 2016;11:e0167134. doi: 10.1371/journal.pone.0167134. doi: 10.1371/journal.pone.0167134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Musumeci G, Aiello FC, Szychlinska MA, Di Rosa M, Castrogiovanni P, Mobasheri A. Osteoarthritis in the XXIst century: Risk factors and behaviours that influence disease onset and progression. Int J Mol Sci. 2015;16:6093–112. doi: 10.3390/ijms16036093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ganasegeran K, Menke JM, Challakere Ramaswamy VM, Abdul Manaf R, Alabsi AM, Al-Dubai SAR. Level and determinants of knowledge of symptomatic knee osteoarthritis among railway workers in Malaysia. Biomed Res Int 2014. 2014 doi: 10.1155/2014/370273. 370273. doi: 10.1155/2014/370273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Felson DT, Hodgson R. Identifying and treating preclinical and early osteoarthritis. Rheum Dis Clin North Am. 2014;40:699–710. doi: 10.1016/j.rdc.2014.07.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Zhang Y, Jordan JM. Epidemiology of osteoarthritis. Clin Geriatr Med. 2010;26:355–69. doi: 10.1016/j.cger.2010.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Xia B, Di Chen D, Zhang J, Hu S, Jin H, Tong P. Osteoarthritis pathogenesis: A review of molecular mechanisms. Calcif Tissue Int. 2014;95:495–505. doi: 10.1007/s00223-014-9917-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Al-Shammari SA, Khoja TA, Alballa SR, Kremlin M. Obesityand clinical osteoarthritis of the knee in primary health care, Riyadh, Saudi Arabia. Med Sci Res. 1995;23:255–6. [Google Scholar]
- 11.Al Arfaj A, Alboukai AA. Prevalence of radiographic knee osteoarthritis in Saudi Arabia. Clin Rheumatol. 2002;21:142–5. doi: 10.1007/s10067-002-8273-8. [DOI] [PubMed] [Google Scholar]
- 12.Kim I, Kim HA, Seo YI, Song YW, Hunter DJ, Jeong JY, et al. Tibiofemoral osteoarthritis affects quality of life and function in elderly Koreans, with women more adversely affected than men. BMC Musculoskelet Disord. 2010;11:129. doi: 10.1186/1471-2474-11-129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Andrianakos AA, Kontelis LK, Karamitsos DG, Aslanidis SI, Georgountzos AI, Kaziolas GO, et al. Prevalence of symptomatic knee, hand, and hip osteoarthritis in Greece. The ESORDIG study. J Rheumatol. 2006;33:2507–14. [PubMed] [Google Scholar]
- 14.Alharthi AS. Awareness of osteoarthritis among saudipopulation. Int J Sci Eng Res. 2017;8:1688–92. [Google Scholar]