

Abstract
Background:
Nutritional status of the elderly population has become an important issue but often gets neglected. Both undernutrition and over nutrition are important public health priorities in this vulnerable group.
Objectives:
To determine the prevalence of malnutrition and factors associated with it among elderly population in rural Puducherry using mini-nutritional assessment (MNA) questionnaire.
Materials and Methods:
A community-based cross-sectional study was conducted among 279 elderly population between November and December 2016 in four villages of rural Puducherry, India. Information on sociodemographic characteristics and nutritional status of the elderlies were collected using validated MNA questionnaire. Body mass index was used to report obesity based on Asia-Pacific guidelines.
Results:
Among 279 participants, 178 (63.8%) were in the age group of 60–70 years, 190 (68.1%) were females, and 208 (74.6%) had no formal-education. Prevalence of malnutrition among elderly was found to be 17.9% (95% CI: 13.7–22.7) and about 58.8% (95% CI: 52.9–64.4) were at risk of malnutrition which was assessed using MNA questionnaire. Prevalence of obesity was found to be 32.5% (95% CI: 27.3–38.3) and 38.4% had inadequate fruits and vegetables intake. About 250 (89.6%) are living independently according to ADL score.
Conclusion:
Both undernutrition and over nutrition are important health issues to be considered among elderly population in this area. Primary healthcare strengthening to address and prevent this health issue by balanced dietary practices may improve their nutritional status, thereby enhancing their quality of life.
Keywords: Elderly, malnutrition, mini-nutritional assessment
Introduction
The World Health Organization (WHO) estimates that the total number of older or elderly people (≥60 years) worldwide would cross the figure of 1.2 billion by 2025, including around 840 million people from low-income countries.[1] In India too, the number is escalating with about 7.7% of the total population being elderly. Hence, the health status of the elder population has a significant impact on the well-being of the country.
Older persons are specifically susceptible to malnutrition as there are many practical issues encountered in providing adequate nutrition. With increasing age, though both lean body mass and basal metabolic rate declines that leads to reduction in energy requirement, the necessity for other vital nutrients rises.[1] Hence, the appropriate inclusion of all categories of food in diet needs to be taken care of. Since nutrition of the elderly affects immunity as well as functional ability, it is an important component of elderly care that warrants further attention.[2]
Factors like feeding difficulty, reduced mobility, psychological distress, being widowed, illiteracy, caring for children, poverty, and poor access to health and social services make elderly more vulnerable for malnutrition.[3] Several studies have shown that malnutrition among elderly can cause increase in morbidity and mortality.[4] Mini-nutritional assessment (MNA) tool is a simple and reliable tool for assessing elderlies at risk of malnutrition and has been designed especially for primary care physicians and health care providers involved in taking care of frail and sick elderly patients, at home or hospitals.[5]
Although some studies have been done to find the prevalence of malnutrition among elderly, it is still under-reported in several parts of India. Factors associated with malnutrition were also found to be under-reported. Very few studies have been done using MNA tool in South India which comprehensively covers multiple aspects leading to malnutrition. Planning of strategies and National Health Programs focusing on elderly also require data on malnutrition. Therefore, we aimed to determine the prevalence of malnutrition and factors associated with it among elderly population in rural Puducherry using MNA questionnaire.
Materials and Methods
A community-based cross-sectional study was carried out in the Rural Health Center (RHC) of a tertiary care institute that caters to a population of around 10,000 in the villages of Ramanathapuram, Thondamanatham, Pillaiyarkuppam, and Thuthipet during November to December 2016. RHC provides comprehensive primary health care to the whole population residing in the four villages that are similar in terms of sociodemographic and cultural factors. Individuals ≥60 years of age belonging to these areas were included in the study.
Sample size was calculated by OpenEpi v 3.01 using prevalence of malnutrition among elderly 24.8% based on a previous study.[4] With absolute precision of 5% and a confidence interval of 95%, sample size was calculated to be 287. However, 279 individuals were covered.
Primary sampling unit was households. Numbers of households needed from each of the four villages were calculated using proportionate sampling after which, systematic random sampling was employed to select the households from the villages. Individual >60 years of age was the study unit and were recruited into the study randomly from the selected households. Households which were locked even after three visits were excluded from the study.
Information on sociodemographic variables and MNA questionnaire was administered to assess the nutritional status of elderly.
MNA questionnaire is an 18-item validated nutritional screening instrument widely used for assessing the nutritional status of elderly. A maximum score of 30 can be obtained. A score <17 indicates malnutrition; a score of 17-23.5 indicates a risk of malnutrition and a score of ≥24 indicates a satisfactory nutritional status.
Data collection was started after obtaining informed consent from the selected individual. Three training doctors posted in rural health center under JIPMER located in the study setting were chosen as data collectors. They were sensitized regarding the objectives of the study, confidentiality of information, and participant's right and informed consent, and were also trained to administer the questionnaire. The purpose of the study and procedure involved in the study was explained before administration of the questionnaire. Interview was conducted by house-to-house visit. Postgraduates posted in same rural health center supervised the data collection procedures by reviewing all questionnaires at the end of each day and also addressed any issues faced by data collectors. Questionnaire had been standardized for our research by forward translation, expert panel back translation, pretesting, and cognitive interviewing and was arrived at the final version.
The questionnaire consisted of two sections: screening and assessment sections. Screening section consisted of six parts that included a subjective assessment of decline in food intake and perceived psychological stress and weight loss during the past 3 months, mobility of the individual, subjective assessment of neuropsychiatric symptoms like dementia or depression, and anthropometric assessment, such as height, weight, and body mass index (BMI). Height was measured with a measuring tape to the nearest 0.1 cm and weight was measured using digital weighing scale to the nearest 0.1 kg. Next, the assessment section consisted of 12 parts that included questions pertaining to independent living status of the elderly; presence of pressure sores; number of prescription drugs taken; frequency of meals; assessment of protein intake by frequency of intake of meat, fish, legumes, dairy products, consumption of fruits and vegetables, fluid intake; mode of feeding; self-assessment of health and nutritional status; and anthropometric measurements, such as mid -rm circumference and calf circumference. Mid-arm circumference was measured using measuring tape at the mid-point between the tip of the shoulder and the tip of the elbow. Calf circumference was measured at the level of largest circumference of the calf. A maximum score of 14 and 16 were given to the screening and assessment sections, respectively. The study participants were then classified as: normal, at risk of malnutrition or malnutrition based on the total scores obtained.
Data were entered into Epidata v 3.01 software and analysis was done using SPSS version 19.0. Continuous variables such as age were summarized as mean and standard deviation (SD). Categorical variables such as gender, education, and occupation were summarized as proportions. Results of malnutrition status were summarized as proportion with 95% confidence interval. Bivariate analysis (Chi-square test/Fisher's exact test) was used to find the association between sociodemographic factors and malnutrition. Prevalence ratio with 95% confidence interval was calculated. P value less than 0.05 was considered statistically significant.
Results
There were totally 767 individuals belonging to the age group of ≥60 years in the study setting, out of which 287 were selected for the study. Out of the 287 elderly selected, 279 (97.2%) individuals responded to the questionnaire. Eight elderly were unable to respond to the questionnaire.
Table 1 shows the sociodemographic characteristics of the study participants. Among 279 individuals interviewed, majority 190 (68.1%) were females. The age of the study participants ranged from 60 to 100 years and the mean age ± SD was 69.37 ± 8.12 years. Majority 178 (63.8%) of the study participants were in the age group of 60–70 years, 208 (74.6%) had no formal education, and 264 (94.6%) were unemployed.
Table 1.
Socio-Demographic characteristics of elderly residing in selected Rural areas of Puducherry (n=279)
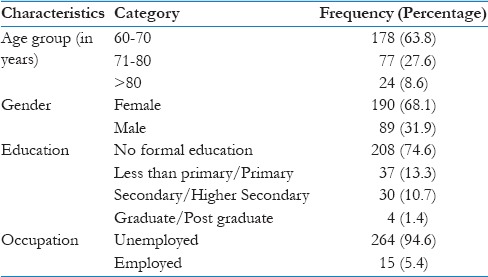
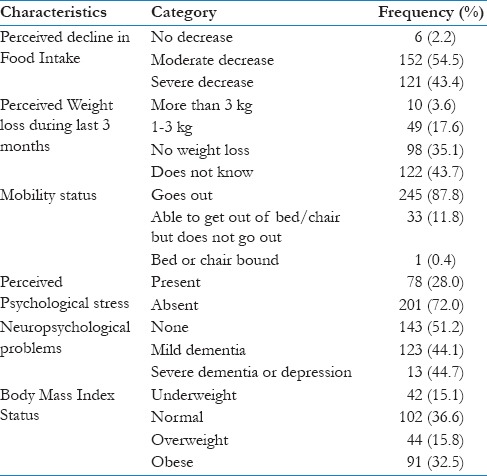
Table 2 states about the anthropometric and general assessment part of the questionnaire. Among 279 individuals interviewed, 121 (43.4%) had a severe decline in the food intake level. Majority of participants 245 (87.8%) had adequate mobility. During the past 3 months, 78 (28%) perceived psychological stress. About 42 (15.1%) were underweight and 91 (32.6%) were obese based on BMI.
Table 2.
Anthropometric and general assessment of elderly residing in selected rural areas of Puducherry using Mini-Nutritional Assessment (n=279)
Regarding the quality of life and activity of daily living status of elderly, about 250 (89.6) live independently, 77 (27.6%) takes more than three prescription drugs per day, and 15 (5.4%) have pressure sores or ulcers.
Regarding dietary habits of elderly, about 154 (55.2%) have three meals per day, 236 (84.5%) have at least one serving of dairy products every day and at least two servings of legumes or egg per day, and 172 (61.6%) have at least two servings of fruits or vegetables per day. Around 30% of participants have less than three cups (600 ml) of fluid per day. About 274 (98.2%) were self-fed without any difficulty.
Table 3 summarizes the self-perception of health and nutritional status in which about 124 (44.4%) perceived themselves as malnourished and 110 (39.3%) considered their health status lower as compared with the individuals in the same age group [Table 3].
Table 3.
Dietary habits and perceived nutritional status of elderly residing in selected rural areas of Puducherry using Mini-Nutritional Assessment (n=279)
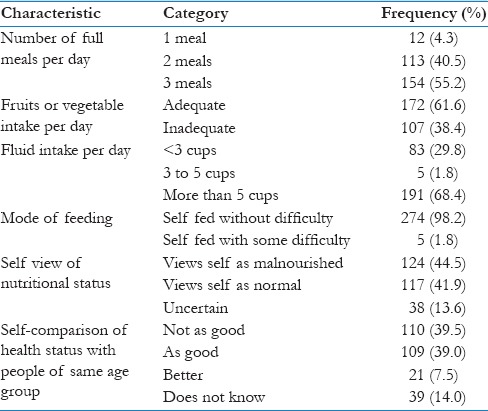
Figure 1 summarizes the nutritional status of the elderly in the study population. The prevalence of malnutrition among elderly was 17.9% (95% CI: 13.7%–22.7%) and 58.8% (95% CI: 52.9%–64.4%) were at risk of malnutrition.
Figure 1.

Nutritional status of elderly residing in selected rural areas of Puducherry using mini-nutritional assessment (N = 279)
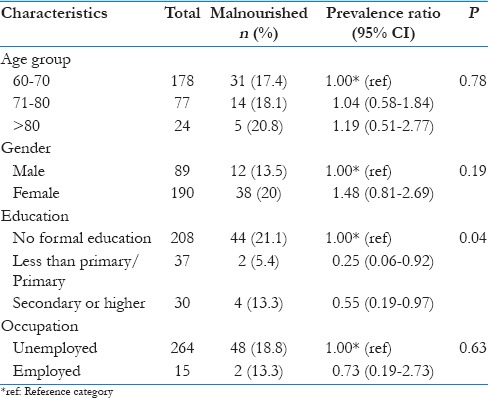
Table 4 shows the association between sociodemographic characteristics like age group, gender, education, and occupation and malnutrition status that was calculated using Chi-square test/Fisher's exact test. Except educational status (P = 0.04), none of the factors came as statistically significant.
Table 4.
Association of malnutrition with socio-demographic characteristics of of elderly residing in selected rural areas of Puducherry, South India (n=279)
Discussion
The current study in rural Puducherry showed that about 17.9% of elderly were malnourished and about 58.7% of elderly was at risk of malnutrition. The proportion of malnourished based on BMI status was also found to be similar to above findings (15.1%). Malnutrition status was found to be higher among individuals with no formal education, unemployed, and age >70 years. However, except educational status (P = 0.04), none of the other factors were statistically significant. The observed prevalence of obesity was 32.5% as per Asia-Pacific guidelines for assessment of BMI.
Studies around the world showed prevalence of malnutrition among elderly ranging from 13% to 54%.[3,6,7,8] Studies done using the MNA questionnaire in rural area of South India at Kaniyambadi (14%) have showed a prevalence similar to the current study findings.[7] In contrast, the findings of studies done in Northern India like Allahabad (25%), West Bengal (29.4%), and Haryana (53.4%) showed a higher prevalence.[6,9,10] Lesser prevalence in the current study can be attributed to the tool used which comprehensively covers anthropometric, psychological, dietary, and perceived nutritional status, whereas other studies used only anthropometric measurements, which might have overestimated the burden.
Prevalence of elderly who were at risk of malnutrition was found to be 58.7%. Similar findings were reported from studies done in Vellore and West Bengal, where around 50%–60% were at risk of malnutrition.[6,7] Higher prevalence in the current study and aforementioned studies emphasize the importance of assessing the nutritional status among elderly.
In the current study, prevalence of malnutrition was higher among elderly females as compared with males, which are similar to the findings found in studies done at Vellore, West Bengal, and Haryana, and other developing countries like Uganda and Ethiopia. However, the difference in current study was not statistically significant.
The prevalence of obesity was 32.5%, which was similar to the findings of a study done in rural area of Karnataka (36.7%).[11] However, previous studies done in rural areas of Tamil Nadu, Puducherry, and Chandigarh showed a much lesser prevalence of obesity (5%–20%).[12,13,14] Higher prevalence in the current study could be the result of using Asia-Pacific guidelines for diagnosing obesity, whereas other studies used WHO classification for obesity.
Current study has certain strengths. First, it was being a community-based study with high-response rate (97.2%). Second, include usage of a validated questionnaire that not only covered anthropometric factors but also addressed the dietary, psychological, and perceived nutritional factors to determine the prevalence of malnutrition.
Our study found that the elderly at risk of malnutrition was found to be 58.8%. Study conducted in Spain among elderly population has shown that about 27% were at high risk of malnutrition. This difference could be due to the fact that our setting was more of rural population when compared with the other study.[15] Another study done in Turkey also showed that the proportion of elderly at risk of malnutrition was found to be 18.6% using MNA scores.[16] Sordestrom et al. conducted a study in Sweden, where they concluded with the results exactly same as our findings and even stated that people >80 are at more risk for malnutrition that was similar to our study findings.[17]
However, there were certain limitations in the current study. Since this was cross-sectional study, establishing cause–effect relationship was not possible. Since study was done in smaller geographical region, generalisability to other areas will be difficult.
Current study has certain implications also. The findings of this study will help policy makers to formulate strategies for an inclusive engagement of primary care providers to identify and manage the cases of malnutrition among elderly at the earliest.
Conclusion and Recommendations
Although only one-fifth of the elderly were found to be malnourished, more than half of them were at risk of malnutrition. Malnutrition was higher as age increases, among females and individuals with no formal education. One-third of the elderly were obese. Both undernutrition and overnutrition were important health issues among elderly in this study. Therefore, it is empirical to identify those with malnutrition and at risk of malnutrition among geriatric population and address regarding healthy dietary practices.
Opportunistic screening can be helpful in doing these activities at primary care level.
At the household level, training of primary care givers in identifying elderly at risk, counseling on nutritional support, and seeking care for prompt management can be helpful.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.WHO | Nutrition for older persons [Internet] WHO; [Last accessed on 2017 Jul 11]. Available from: http://www.who.int/nutrition/topics/ageing/en/index1.html . [Google Scholar]
- 2.Lesourd B. Nutrition: A major factor influencing immunity in the elderly. J Nutr Health Aging. 2004;8:28–37. [PubMed] [Google Scholar]
- 3.Kikafunda JK, Lukwago FB. Nutritional status and functional ability of the elderly aged 60 to 90 years in the Mpigi district of central Uganda. Nutrition. 2005;21:59–66. doi: 10.1016/j.nut.2004.09.009. [DOI] [PubMed] [Google Scholar]
- 4.Kalaiselvi S, Arjumand Y, Jayalakshmy R, Gomathi R, Pruthu T, Palanivel C. Prevalence of under-nutrition, associated factors and perceived nutritional status among elderly in a rural area of Puducherry, South India. Arch Gerontol Geriatr. 2016;65:156–60. doi: 10.1016/j.archger.2016.03.003. [DOI] [PubMed] [Google Scholar]
- 5.Vellas B, Guigoz Y, Garry PJ, Nourhashemi F, Bennahum D, Lauque S, et al. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutrition. 1999;15:116–22. doi: 10.1016/s0899-9007(98)00171-3. [DOI] [PubMed] [Google Scholar]
- 6.Lahiri S, Biswas A, Santra S, Lahiri S. Assessment of nutritional status among elderly population in a rural area of West Bengal, India. Int J Med Sci Public Health. 2015;4:569–72. [Google Scholar]
- 7.Vedantam A, Subramanian V, Vijay Rao N, John K. Malnutrition in free-living elderly in rural south India: Prevalence and risk factors. Public Health Nut. 2010;13:1328–32. doi: 10.1017/S1368980009991674. [DOI] [PubMed] [Google Scholar]
- 8.Mathew A, Das D, Sampath S, Vijayakumar M, Ramakrishnan N, Ravishankar S. Prevalence and correlates of malnutrition among elderly in an urban area in Coimbatore. Indian J Public Health. 2016;60:112–7. doi: 10.4103/0019-557X.184542. [DOI] [PubMed] [Google Scholar]
- 9.Yadav N, Ravindra R, Sharma S, Singh A, Mishra M, Dubey J, et al. Dietary habits and nutritional status of elderly living in urban areas of Allahabad district. Indian J Prev Soc Med. 2012;43:81–6. [Google Scholar]
- 10.Jamir L, Kalaivani M, Nongkynrih B, Misra P, Gupta SK. Anthropometric characteristics and undernutrition among older persons in a rural area of Northern India. Asia Pac J Public Health. 2015;27:NP2246–58. doi: 10.1177/1010539513490191. [DOI] [PubMed] [Google Scholar]
- 11.Ratnaprabha GK, Farah NF, Twinkle A, Naveen JT, Ashit BX. Prevalence of obesity and its associated factors among elderly in a rural area of South Karnataka. Ann Community Health. 2015;2:15–21. [Google Scholar]
- 12.Shankar R, Balamurugan SS. Prevalence of chronic energy deficiency, overweight and obesity among the geriatric population in rural area in Tamilnadu in Sri Ramchandra. J Med. 2011;4:24–9. [Google Scholar]
- 13.Swami HM, Bhatia V, Gupta AK, Bhatia SPS, others An epidemiological study of obesity among elderly in Chandigarh. Indian J Community Med. 2005;30:255–8. [Google Scholar]
- 14.Rajkamal R, Singh Z, Stalin P, Muthurajesh E. Prevalence and determinants of overweight and obesity among elderly population in an urban area of Puducherry. Int J Med Sci Public Health. 2015;4:369–72. [Google Scholar]
- 15.Julio MPM, Clavero AE, Soler MLM. Nutritional status and factors associated with non-institutionalized people over 75 years of age. Rev Bras Enferm. 2018;71:1007–12. doi: 10.1590/0034-7167-2017-0207. [DOI] [PubMed] [Google Scholar]
- 16.Son N, Kavak B. Evaluation of nutritional status of elderly patients presenting to the Family Health Center. Pak J Med Sci. 2018;34:446–51. doi: 10.12669/pjms.342.14936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Söderström L, Thors Adolfsson E, Rosenblad A, Frid H, Saletti A, Bergkvist L. Mealtime habits and meal provision are associated with malnutrition among elderly patients admitted to hospital. Clin Nutr. 2013;32:281–8. doi: 10.1016/j.clnu.2012.07.013. [DOI] [PubMed] [Google Scholar]