

Abstract
Introduction:
Vitamin D deficiency is a recognized pandemic. Even in a tropical country like India, where there is plentiful sunshine, vitamin D deficiency is widely prevalent. Adult females, particularly those above the age of 40, are mostly affected because vitamin D determines the pattern of post-menopausal bone loss and age-related osteoporosis.
Methods:
A community-based cross-sectional study was conducted from April–December 2017 among 194 women aged 40 years and above residing in the village of Singur, West Bengal. For this study, multistage random sampling method was used. Each respondent was interviewed using a structured schedule to collect data on sociodemographic characteristics, dietary pattern, their daily sun exposure, tobacco use, and morbidity profile. Individuals with 25OH vitamin D <30ng/ml were said to have vitamin D insufficiency (VDI). Data entry and analysis was done using SPSS version 16.0.
Results:
Out of 194 participants, 70.6% had VDI (Vitamin D deficient-19.6%, Vitamin D insufficient-51.0%). Mean (SD) age of the participant was 56.9 (8.9) years. Mean (SD) duration of daily sun exposure was 138.5 (59.2) minutes. 74 (38.1%) had overweight/obesity. Only 73 (37.6%) had adequate diet. Test results revealed low SES, decreasing duration of daily sun exposure, diabetes, overweight/obesity, and inadequate diet as significant predictors of VDI, explaining 39.3% of the variance with model fit.
Conclusion:
The study has identified factors associated with VDI among the study participants. Emphasis on promoting consumption of vitamin D rich food and with vitamin D supplements, outdoor activities to increase sun exposure, maintaining optimum body weight, and strictly adhering to diabetes control will help alleviate the problem at large.
Keywords: Community-based, daily sun exposure, rural community, vitamin D insufficiency, women
Introduction
Vitamin D is a fat-soluble vitamin. Owing to its role in calcium homeostasis, it is also known as the ‘sunshine vitamin’ or ‘anti-rachitic factor.’[1] The human body obtains sufficient amounts of vitamin D either from diet or adequate exposure to sunlight. Usually, 50–90% of vitamin D is produced by the skin on exposure to sun.[1] Natural diet that most humans consume contains less amounts of vitamin D. Important dietary sources of vitamin D are egg yolk, fatty fish, beef liver, and fortified dairy products.[2] The extra skeletal effects of vitamin D are related to glycemic control, immunity, and prevention of cardiovascular diseases and cancer.[3,4]
Vitamin D deficiency is a recognized pandemic. Even in a tropical country like India, vitamin D deficiency is widely prevalent in spite of plentiful sunshine. Various studies from different parts of India have highlighted that vitamin D insufficiency or deficiency across different age groups range from 70–100%.[5] Adult females, particularly those above 40 years of age, are mostly affected because vitamin D determines the pattern of post-menopausal bone loss and age-related osteoporosis.
This is the most underdiagnosed and undertreated nutritional deficiency in the world.[6,7,8] In India, vitamin D insufficiency (VDI) is not a National Health Priority (NHP). Of the NHPs, the most important is the supplementation of pregnant women with calcium and vitamin D tablets. However, the adult and geriatric population that is mostly vulnerable has been ignored. Although VDI has increasingly become an important public health issue, it is not included in any national health program.
There is a dearth of research regarding VDI in eastern India, and specifically in the rural community. This study was conducted to quantify the burden of VDI and find out its predictors among women aged 40 and above in a rural area of West Bengal.
Materials and Methods
Study design and setting
This was a cross-sectional, community based observational study, conducted over a period of nine months (April-December 2017). The Rural Health Unit and Training Centre, Singur is the rural field practice area of All India Institute of Hygiene and Public Health (AIIHPH), Kolkata, which caters to 64 villages through two Union Primary Health Centers (UPHCs).
Women aged 40 and above, residing in the villages under the purview of RHUTC, Singur, were the subjects of this study. The exclusion criteria included (i) pregnant and lactating women (ii) those that had not provided written informed consent (iii) patients who were critically ill and (iv) patients who were on vitamin D supplementation since the last 6 months.
Sample size and sampling technique
With reference to a study conducted in Mangalore[9], according to which the level of VDI was 80%, and taking into consideration 95% confidence level, 10% relative error and design effect of 2, the final sample size was calculated to be 194.
Multistage random sampling was done. In the first stage, 3 villages were selected randomly from each UPHC. Women aged 40 and above were selected from villages, and the number of participants from each village was calculated by Population Proportionate to Size sampling method. Following this, the required number of samples was drawn from the list of women from each village using the simple random sampling method. If the selected individual did not meet the selection criteria or could not be contacted in two visits, simple random sampling without replacement was done to select another study participant.
Study tool
A pre-designed, pre-tested structured schedule in the local language (Bengali) was used to collect the data. Face validity and content validity of the instrument were ascertained by experts of the institution from which the authors were affiliated. The height and weight of the women were measured using standard operating procedures. In the past 7 days, individuals who consumed fish, egg yolk, milk, or dairy products for more than 3 days were considered to have satisfactory diet rich in vitamin D. Individuals with Body Mass Index (BMI) ≥25 kg/m2 were reported as overweight/obese.[10] Laboratory investigation of serum for 25-Hydroxyvitamin D [25(OH)D] was done. Individuals with 25OH Vitamin D <30 ng/ml were categorized into the VDI group.[3]
Data analysis and ethical approval
Data entry and analysis was performed using the statistical software SPSS (IBM SPSS Statistics for Windows, Version 16.0). Descriptive statistics (mean ± Standard Deviation [SD] and median for the continuous variables and frequency in percentage for the categorical variables) was used to describe the sociodemographic characteristics, dietary pattern, daily sun exposure, tobacco use, and morbidity profile. Univariate and multivariable logistic regressions were used to determine the factors related with VDI. Results were considered significant at P < 0.05 level.
Ethical approval was obtained from the Institutional Ethics Committee. At the end of the study, patients with VDI were treated and advised about the preventive measures.
Results
Out of 194 participants, 93 (47.9%) belonged to the 40–49 age group. Mean (SD) age of the participants was 56.9 (8.9) years. Among them, 169 (87.1%) were Hindu and 172 (88.6%) were currently married. Furthermore, 102 (52.6%) lived in joint families, while 112 (57.7%) were educated upto primary. Mean (SD) per capita income was 2754 (1097) INR, and 98 participants (50.5%) belonged to middle class (according to Modified B. G. Prasad scale January 2017).
Mean (SD) duration of daily sun exposure was 138.5 (59.2) minutes. 81 participants (41.7%) were current tobacco chewers, while 6 participants (3%) had a history of smoking bidis. 82 women (42.3%) had menopause. It was found that 55 (28.3%) were hypertensives and 68 (35.0%) were suffering from diabetes. The proportion of women with overweight/obesity was 38.1%. In the past 7 days, although 61 (31.4%) consumed fish for more than 3 days and 56 (28.8%) ate egg yolk for more than 3 days, only 35 (18.0%) had milk and dairy products for more than 3 days.
Out of the study participants, 57 (29.4%) had sufficient vitamin D (≥30ng/ml), while 99 (51.0%) had insufficient vitamin D (20-29.99ng/ml) and 38 (19.6%) had deficient vitamin D (<20ng/ml) [Table 1]. The mean (SD) vitamin D level was 25.9 (5.21) ng/ml. Overall, the proportion of women suffering from VDI was 70.6%.
Table 1.
Distribution of study participants according to their vitamin D status and vitamin D levels (n=194)

From Table 2, it was evident that factors such as the decreasing age, education up to primary, low SES, the decreasing duration of daily sun exposure, menopause, diabetes, overweight/obesity, and unsatisfactory diet were significantly associated with VDI.
Table 2.
Univariate logistic regression between VDI and different variables (n=194)

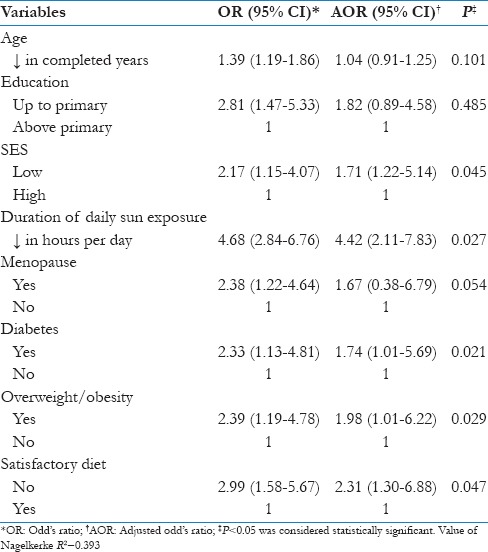
After adjusting for all the independent variables, only low SES, decreasing duration of daily sun exposure, diabetes, overweight/obesity, and unsatisfactory diet were significant predictors of VDI [Table 3]. The final model explained 39.3% of variance with non-significant Hosmer–Lemeshow statistics.
Table 3.
Multivariable logistic regression between VDI and explanatory variables (n=194)
Discussion
Our study found that 70.6% of the women aged 40 years and above had VDI. This was lower than 99.7% of VDI as reported by a study among adult women in the rural community of Ballabgarh development block in Faridabad in 2017.[11] The finding of this study was also lower than that of another study in rural Maharashtra in 2017, where prevalence of VDI was reported to be 88.9%.[12] However, the findings are in line with that of a study conducted in Raipur in 2016 among post-menopausal women.[13] This may be attributed to the fact that in West Bengal, fish and egg consumption is more, which happen to be among the very few dietary sources of vitamin D.
Our study suggests that the decreasing duration of sun exposure and diabetes are significantly associated with VDI. This finding is similar to that of a study[12] conducted among 640 rural patients in Mahad, Maharashtra in 2017, which identified that women with dark complexion, those who wear Burkha, women who get inadequate exposure to sunlight, and those with diabetes were the significant predictors of Vitamin D deficiency. Gender and hypertension were not significantly associated with vitamin D deficiency.
Another multi ethnic sample study of Asian adults also found that females, smokers, alcoholics, diabetes patients, young people, those with higher BMI or HbA1c, people who had no education and poor income levels are significantly associated with VDI.[14] This can be explained by the fact that vitamin D, a fat-soluble vitamin, gets sequestrated inside the adipose tissue (found more in obese individuals), resulting in pseudo VDI in the blood.
Various public health impacts of vitamin D deficiency require urgent attention. It is evident that vitamin D not only has a bearing on bone health, but also plays a crucial role in the overall health of an individual, right from its effect on glycemic control, immunity, cardiovascular diseases, neuromuscular function, pregnancy, and other aspects of health. An epidemiological study conducted in the United States among a cohort of 903 healthy individuals suggested that people with vitamin D deficiency may be at a much greater risk of developing diabetes.[15] It has been implicated that in people who suffer from cardiovascular diseases, maintenance of normal serum 25(OH) vitamin D level could reduce their mortality risk as a result of the disease by 30%.[16]
In the current global scenario, where non-communicable diseases have achieved pandemic potential and cardiovascular diseases remain the leading cause of death and disability, it has been recognized vitamin D3 significantly reduces the level of oxidative stress on the cardiovascular system.[17] Moreover, it has been implicated that deficiency of vitamin D3 increases the chances of heart attacks.[17] The increasing prevalence of obesity and physical inactivity, and decreased sun exposure due to lifestyle changes and unhealthy diet have all added to the increasing prevalence of VDI. The knowledge about the importance to maintain an adequate level of vitamin D is an emerging essential domain among the primary care physicians and is imperative to improve public health.
The main strength of the study was that it was conducted among women from the rural community and multistage random sampling, along with design effect was used to arrive at an apt sample size with generalizability of results. The study investigated 25OH Vitamin D, which is the most sensitive indicator for an individual's vitamin D status. However, the study had limitations of its own. As it was a cross-sectional study, temporal association could not be established. Body parts and their relation to sun exposure could not be assessed. Further, due to limited funds, the researchers were unable to conduct investigations like serum calcium, alkaline phosphatase, and Parathyroid Hormone (PTH), which are all important functional indicators of vitamin D status.
The need for improving the levels of vitamin D among the female population is both important and urgent. Emphasis must be given on promoting consumption of vitamin D rich foods and vitamin D supplements. They should also be encouraged to engage themselves in outdoor activities to increase exposure to sunlight. Women should be educated on the importance of maintaining optimum body weight and strict adherence to diabetes prevention and control measures. At the policy level, the provision for early diagnosis of vitamin D deficiency, framing of population-based programs to provide affordable vitamin D supplements, and vitamin D fortified food will help improve the situation at large.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson J, Loscalzo J, editors. Harrison's Principles of Internal Medicine. 18 ed. New York, NY: McGraw-Hill; 2012. [Google Scholar]
- 2.Heldenberg D, Tenenbaum G, Weisman Y. Effect of iron on serum 25-hydroxyvitamin D and 24,25-dihydroxyvitamin D concentrations. Am J Clin Nutr. 1992;56:533–6. doi: 10.1093/ajcn/56.3.533. [DOI] [PubMed] [Google Scholar]
- 3.Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357:266–81. doi: 10.1056/NEJMra070553. [DOI] [PubMed] [Google Scholar]
- 4.Li YC, Kong J, Wei M, Chen ZF, Liu SQ, Cao LP. 1,25-Dihydroxyvitamin D (3) is a negative endocrine regulator of the renin- angiotensin system. J Clin Invest. 2002;110(2):229–38. doi: 10.1172/JCI15219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ritu G, Gupta A. Vitamin D deficiency in India: Prevalence, causalities and interventions. Nutrients. 2014;6:729–75. doi: 10.3390/nu6020729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Van Schoor NM, Lips P. Worldwide Vitamin D status. Best Pract Res Clin Endocrinol Metab. 2011;25:671–80. doi: 10.1016/j.beem.2011.06.007. [DOI] [PubMed] [Google Scholar]
- 7.Mithal A, Wahl DA, Bonjour JP, Burckhardt P, Dawson-Hughes B, Eisman JA, et al. Global Vitamin D status and determinants of hypovitaminosis D. Osteoporos Int. 2009;20:1807–20. doi: 10.1007/s00198-009-0954-6. [DOI] [PubMed] [Google Scholar]
- 8.Van der Meer IM, Middelkoop BJ, Boeke AJ, Lips P. Prevalence of Vitamin D deficiency among Turkish, Moroccan, Indian and sub-Sahara African populations in Europe and their countries of origin: An overview. Osteoporos Int. 2011;22:1009–21. doi: 10.1007/s00198-010-1279-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nandini M, Prabhu AK, Kamath AK, Aishwinee VG. Profile Of Vitamin D Deficiency in Mangalore. Int J Pharm Bio Sci. 2014;5:179–86. [Google Scholar]
- 10.WHO/IASO/ITO. Asia Pacific Perspective Redefining Obesity and its Treatment, WHO Western Pacific Region. 2000. [Last accessed on April 27, 2018]. Available from: http://www.cadiresearch.org/topic/obesity/global-obesity/obesity-overview .
- 11.Misra P, Srivastava R, Misra A, Kant S, Kardam P, Vikram NK. Vitamin D status of adult females residing in Ballabgarh health and demographic surveillance system: A community-based study. Indian J Public Health. 2017;61:194–8. doi: 10.4103/ijph.IJPH_176_16. [DOI] [PubMed] [Google Scholar]
- 12.Bawaskar PH, Bawaskar HS, Bawaskar PH, Pakhare AP. Profile of Vitamin D in patients attending at general hospital Mahad India. Indian J Endocrinol Metab. 2017;21:125–30. doi: 10.4103/2230-8210.196004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mitra S, Nayak PP, Agrawal S, Sahoo JP, Kamalanathan S, Nanda R. Vitamin D Status and Cardio-Metabolic Risk in Indian Postmenopausal Women. J Clin Diagn Res. 2016;10:QC17–20. doi: 10.7860/JCDR/2016/17839.7438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Man REK, Li L-J, Cheng C-Y, Wong TY, Lamoureux E, Sabanayagam C. Prevalence and Determinants of Suboptimal Vitamin D Levels in a Multiethnic Asian Population. Nutrients. 2017;9:313. doi: 10.3390/nu9030313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Park SK, Garland CF, Gorham ED, BuDoff L, Barrett-Connor E. Plasma 25-hydroxyvitamin D concentration and risk of type 2 diabetes and pre-diabetes: 12-year cohort study. PLoS One. 2018;13:e0193070. doi: 10.1371/journal.pone.0193070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Degerud E, Nygård O, Vogel S, Hoff R, Svingen GFT, Pedersen ER, et al. Plasma 25-hydroxyvitamin D and mortality in patients with suspected stable angina pectoris. J Clin Endocrinol Metab. 2018;103:1161–70. doi: 10.1210/jc.2017-02328. [DOI] [PubMed] [Google Scholar]
- 17.Khan A, Dawoud H, Malinski T. Nanomedical studies of the restoration of nitric oxide/peroxynitrite balance in dysfunctional endothelium by 1,25-dihydroxy vitamin D3-clinical implications for cardiovascular diseases. Int J Nanomed. 2018;13:455–66. doi: 10.2147/IJN.S152822. [DOI] [PMC free article] [PubMed] [Google Scholar]