

Abstract
Background:
Given the importance of spirituality in crisis situations including life-threatening diseases such as cancer, paying due attention to this aspect of care is of great importance. This study aims to investigate the barriers and facilitators in providing spiritual care for parents who have children suffering from cancer.
Methods:
This study was conducted using a qualitative approach and the common content analysis method. Fifteen people who participated in the study included 11 mothers and 4 fathers. A purposive sampling method was used. The environment for the research included the oncology and hematology departments of state children's hospitals around the country. Semi-structured interviews were conducted individually.
Results:
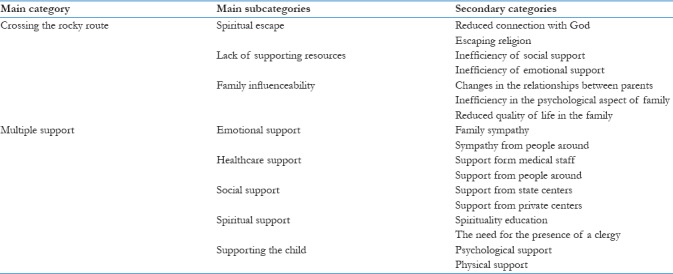
Analyzing the data yielded “crossing the rocky route” as the main category in barriers to spiritual care, which included the subcategories “spiritual escape,” “lack of supporting resources,” and “family influenceability.” In addition, “multiple support” was obtained as the main category in facilitators of spiritual care, which included the subcategories “emotional support,” “healthcare support,” “social support,” “spiritual support,” and “supporting the child.”
Conclusion:
The results of the study showed that spirituality plays an important role in helping parents deal with and adjust to their children's disease. Therefore, it is of great importance to pay due attention to the different aspects of spiritual care and enforce factors that can act as facilitators in this area and remove the barriers to spiritual care. This aim is attainable through educating the parents and medical staff.
Keywords: Barriers and facilitators, children suffering from cancer, content analysis, spirituality
Introduction
Spirituality as the humanitarian aspect of individuals is growing in importance due to an understanding of its role in helping people recover from diseases. Spirituality has been defined as that aspect of human beings that gives people the feeling of being with qualities such as human nature, the capacity for internal knowing, a source of enforcement, a sacred mental experience, ascending toward the capacity for love and larger knowledge, uniting with the entire shadow of all life, and finding a meaning for the being of the individual, which is pivot for all kinds of being.[1]
Spirituality has been defined in different ways, such as the search for the sacred matter, meaning, and the purpose of life, engaging in divine and transcendental affairs beyond the material life.[2,3] Also, spirituality is considered to be a set of values, attitudes, and hopes that are related to the universe and guide a person's life and is especially related to experiences that put the person in a state of uncertainty, in a way that the spiritual needs that exist in every patient become obvious when they face a state of uncertainty in life events.[1]
Spirituality and religion, which are interpreted as mental health and religious practices by some people, overlap in the sense that they both offer framework within which human being can understand the meaning, goal, and high values of their life. In our society, religion is one of the most important psychological supports which has the potential to give meaning to life throughout people's whole life and save them from feelings of absurdity. Religion can be a huge support especially in difficult and crisis situations.[4]
Spiritual care has been known as the most important factor in arriving at a balance in maintaining mental health and confronting diseases. Human experience in all cultures has shown that people always appeal for help from a sacred and divine source in crisis situations and when a disease threatens their life, and the need for spirituality becomes more important in such situations. There is no doubt that the total meaning of spiritual health is not limited to the effects that prayers and spiritual states of mind have in healing diseases, a substitute for common medical treatments, or a kind of supplementary medicine. It can be argued that religious beliefs have a deep effects on people's beliefs, attitudes, values, and behaviors.[5]
Developments in medical sciences help treat and prevent many diseases. With the recent developments in treating child cancer, more patients suffering from the disease survive. However, in comparison to other diseases with weak prognosis, cancer imposes greater fear and worries to patients and their families.[6]
Since family is the main source of support for a child, psychological, economic, and social pressures caused by the child's disease leaves a deep effect in the life of the family and affects all aspects of life and health of family members.[7,8]
Give the threatening nature of cancer, being diagnosed with the disease considerably increases the spiritual needs of the patient.[9,10] It is often the case that when facing difficult situations in life, people tend to appeal to a supreme (spiritual) power as a means for combating and adjusting to the situation.[11]
Raffay et al. (2016, as cited in Gordon, 2005) state that a clinical therapist's job is to treat sometimes, soothe often, and relieve all the time. Relief happens when the therapist supports that part of the patient's existence that inspires meaning and hope, and that is what many patients need.[12]
The measures needed for spiritually evaluating patients include organizing the resources, supporting spiritual beliefs, and taking part in spiritual activities. After the patient or client's religious and spiritual needs are recognized, the decision needs to be made as to whether the therapist is able to satisfy their spiritual needs or they should be referred to a religious or spiritual person. Sometimes simple interventions on the part of the physician can easily satisfy the patient's spiritual and religious needs without any need to be referred to a clergy. This is especially important because some patients avoid visiting a clergy or religious consultant.[13]
In this study, spiritual care is considered as a mental and abstract phenomenon that people understand in a unique way based on their perceptions. In other words, using a qualitative research approach allows the researcher to explore the attitudes of families with children suffering from cancer toward spirituality by entering their mental world and to identify factors that inhibit or facilitate their search for spirituality.
Methods
This study used the common content analysis method. The participants were selected using a purposive sampling procedure. The participants were selected from parents with children suffering from cancer in state hospital throughout the country. The criteria for entering the study included having a child suffering from cancer and the willingness to participate in the study and express their experiences. To have maximum diversity, participants from different age groups with different cultural, social, and economic backgrounds were selected. Throughout the study, 15 parents were selected for the study, and the sampling continued until data saturation was achieved. The main data-gathering instrument was a semi-structured interview, and each interview lasted for 60 min on average. The time and place of the interview were determined at the participant's convenience. The core of the interview questions was the parents’ experiences regarding spiritual care. A general question was asked at first: “What does it feel to have a child suffering from cancer?” The path the interview took was guided by the participant's response to the first question. Exploratory and follow-up questions were then asked to gain more information and better understand the participant's responses, with the responses being the guide for the follow-up questions. The interviews were recorded on a voice-recorder and immediately transcribed as text files. According to Graneheim and Lundman's content analysis method, the process of analyzing the data was in progress as the data were being collected.[14] The interviews were first typed. They were then read word by word to extract the initial codes. The codes were reread several times so that they can be categorized in the main or subcategories based on their meaning similarities. The data were organized at different levels, and the levels were labeled using abstract titles. Finally, the core of the study was determined by revisiting the data and code levels. In all stages of the study, it was tried not to let the researcher's assumptions affect the data analysis. Written informed consent was obtained from the participants, and they were informed that, if necessary, they might be contacted again to complete the conversations.
Results
Analyzing the data from the 15 participants in the study, including 11 mothers and 4 fathers, who ranged in age from 22 to 50 years and had one or two children suffering from cancer yielded the results as shown in Table 1.
Table 1.
Categories and subcategories for barriers and facilitators in spiritual support for families having children suffering from cancer
Spiritual escape
One of the categories obtained was “spiritual escape,” which included the subcategories “reduced connection with God” and “escaping religion.”
Despite the consensus among all the participants on the importance of spiritual care in cancer, they admitted that they are sometimes distracted from their connection with God and practicing religious rituals due to the psychological stress caused by the disease.
Regarding this issue, the participants stated that the psychological pressure experienced by the parents due to the child's disease creates negative mental states and causes them to lose their connection with God. For example, participant number 3 who was a patient's mother stated,
”Some parents lose their faith in religion and deny the existence of God and even hate God and stop saying their prayers and would ask themselves the question as to why God make the problem for me. They are mad at God. I have seen and experienced these things with my own eyes.”
Also, avoiding religious affairs is another consequence caused by the child's disease, as expressed by participant number 8 who stated,
”I keep saying that I will lose faith in religion if I lose my son.”
Lack of supporting resources
Another issue mentioned by the participants is the lack of supporting resources, which can include both an emotional source and the support provided by the hospital, medical staff, or the presence of a clergy in department.
Participant number 19 stated that,
”Using a clergy in the children's oncology department can be very effective. It is the missing chain in our medical system. We currently don’t have even one clergy either in the children's department or in the adults’ department so that the patient or the patient's companion can consult if they need spiritual support. The clergy may not be able to do anything in terms of medicine, but in terms of spiritual help he can relieve the patient and the companion's heart by reciting a couple of verse from the holy Quran, and it is very effective.”
Participant number 7 stated,
”The hospital doesn’t have enough staff. It's not that they are not accountable, they are just fed up with all the responsibilities. For example, a nurse would come here and be busy taking care of the patient and connecting a serum or administering the medicine, and she has to visit other patients as well. The nurse may not have enough information to inform us, and the doctors just tell us some general things. The mother and the father need to be informed about the nature of their child's disease. The parents should not be left in suspension. They need to tell the parents that, for example, their child suffers from this or that, but they don’t.”
Participant number 15 stated,
”I have seen families in which the father didn’t do anything after they had the problem, and he even bothered and the family and did not emotionally support his wife.”
Participant number 1 stated,
”My husband couldn’t psychologically support me much because he himself was not in a suitable psychological state.”
Family influenceability
One of the issues caused by cancer on family members of a child suffering from cancer is that it affects different aspects of their life, including affecting the relationship between parents and their relationship with other members of the family and other children, and the quality of life for family members is generally affected.
The participants pointed to the changes in their relationship with their spouse and stated that due to the pressure and tensions caused by the child's disease and the fact that they spend most of their time in the hospital and next to their child, their contact with their spouse is reduced. Some other participants stated that their child's disease has made them develop a stronger emotional relationship with their spouse, and they together deal with the problems caused by their child's disease.
For example, regarding this issue, participant number 11 stated,
”I keep telling my wife these things and try to help her in dealing with the conditions, because women are different from men, and they are more fragile and sensitive and can easily collapse under psychological pressure and stress and lose their spirit. That's why I try regularly talk to her and relieve her by my words so that she can promote her spirit and take care of our son. Of course, I come in the evenings to be with our son and send my wife home for a couple of hours so that she can rest for a while and get her energy back to take care of our son for the rest of the days.”
Participant number 8 stated,
”My husband puts a lot of effort in the issue, and we work shoulder to shoulder. He provides the medicine and sometimes stays with us in the hospital and helps us a lt. He is so upset about the situation and does everything he can do for us by providing financial and psychological support. He has high spirits and keeps telling me that our son will be OK, there is no need to worry and keeps talking to me.”
In addition to changing the relationship between the parents, the child's disease emotionally and psychologically affects the other family members as well.
Participant number 8 stated,
”When I am calm, my spirits are higher and I feel happier, and I can give positive to my son and talk to him. When I am down, my son realizes that I’m not in a good mood and it's a source of negative energy for him, but when I am in a good mood, the whole family gets positive energy.”
Participant number 7 stated,
”It's very difficult for his sister too. She doesn’t talk too much these days because of the situation. I here with our son most of the time, my husband too, so we have less time for her. My sister and my mother try to spend more time with my daughter though. It's very difficult for me. Although she doesn’t show it, she feels so upset. She didn’t want to come to the hospital and visit her brother until the day before yesterday, and she said she can’t do it.”
As was mentioned earlier, the participants complained about the changes in their conditions of life and their quality of life, since cancer affects all family members in all aspects of life and ultimately decreases their quality of life.
Participant Number 5 stated,
”You know, you will be fed up with the situation. Sometime I feel I’m going to give up. For example, the previous time my son was hospitalized here, I didn’t feel very well either, but I tried to control myself. I knew that if I give up, my son will give up too.”
Participant number 6 stated,
”My husband returned to our hometown a few days ago, because he was about to lose his job. He is trying to stand beside us and talks to us on the phone regularly. He says he will give up his job if necessary to come and be with us. He reassures me and things like that. He says he can come and be with us if I feel tired, and he helps a lot and talks to me a lot. But unfortunately our life has been affected a lot by the issue and we are under pressure from different aspects.”
Multiple support
One of the factors that can help parents deal with their child's disease is the support from people around them. The support can be in the form of emotional support and by expressing sympathy with them and helping them with accepting the disease and the situation or in the form of offering scientific information about the disease and informing the parents on the part of medical staff. Also, philanthropists and charities can be of great help. Support can take a spiritual form, and encouraging parents to engage in spiritual activities or talking to a clergy or the presence of a clergy in the department can help them feel relaxed and calm. Finally, the support from parents and the medical staff can help the child accept the disease and the situation.
In this regard, the following quotes have been used as examples.
Participant number 7 stated,
”I would have collapsed and given up if it hadn’t been for my husband. I tell him everything that happens in the hospital. Some people advise me not to tell my husband everything that happens here in the hospital because he would be upset by that. I do it, because it makes me feel better. He might get sad too, but this problem is for both of us. It's not just for one of us. I help him and he helps me.”
Participant number 17 stated,
”It made me feel much better that I saw everyone is by me and my family and the people around me supported me and don’t leave me alone in this situation.”
Participant number 16 stated,
”I would consult doctors and specialist. I would ask questions from every doctor I ran into. I would talk to nurses and families who had the same problem. The only thing I could do was to talk to them and see what their child's situation is like.”
Participant number 22 stated,
”Well, they bring their child and talk to the doctor and the residents, and ask questions like: What's the prognosis like? Will they get better? Will they recover? Does it end in death? And doctors, residents, and the nurses talk to them.”
”The doctor in the oncology department is just great and supports the patients in every way possible. He supports the families too and sets some time for them. When he is on leave or on holidays, he calls and asks about the patients. Whenever we call him, if there is a problem with the patient he either comes to the department in person or gives the required instructions to us and tells us what to do.”
Participant number 6 stated,
”The hospital has a prayers room, a prayers book, a Quran. There is also another prayers room where people can pray in group.”
Participant number 7 stated,
”Some philanthropists came here yesterday and gave us some money. I was badly in need myself, but I gave the money to the other mothers. I felt so good when I did that.”
Participant number 17 stated,
”The nurses tell us to trust in God and to ask God to help us. They also tell us to take part in the ceremonies and activities they have in the hospital.”
Participant number 2 stated,
”What I did was to pet my job, my friends, parties, and everything aside. We have always been together for the whole past two years. I have tried to make my son feel comfortable and have fun.”
Participant number 13 stated,
”As a mother, I think I have always been by my son. I mean I have never wanted something for myself. I didn’t want to spend the days I spent with my son for myself, even for my health. I focused all my attention and energy to my son even when I was sick and supported my son psychologically and financially. Not just me, his father has been like that too.”
Discussion
The results of this study identified the categories “escaping from spirituality,” “lack of supporting resources,” and “family influenceability” as the barriers and “emotional support,” healthcare support,” “social support,” “spiritual support,” and “supporting the child” as the facilitators in the spiritual care for parents who have a child suffering from cancer.
As shown by the results of this study, some parents experience negative reactions such as losing their faith and reducing their connections with God, as a result of their child's disease. They believed that their child's disease was God's will, and because of that they had no willingness to do religious practices or say prayers to God. Baljani, in line with this finding, showed that due to the threatening nature of cancer, being diagnosed with the disease causes people's religious beliefs be put at risk, and that spiritual support needs to be provided.[15]
Lack of supporting resources was another category identified in this study. The participants stated that they do not receive the required emotional and spiritual support from people around them, their spouse, or the medical staff, and that the society does not provide the required support to help them deal with and adjust to their problems caused by their child's disease.
There are also barriers that affect nurses’ ability to provide care, which can be divided into two groups: the internal or intrapersonal barriers, which include inability to communicate, lack of information and knowledge about spirituality, and individual beliefs and values; and the external factors or healthcare and environmental situations, which include environmental limitations (providing a quiet environment for the patient), lack of personnel and time, short period of the patient staying in the hospital, and nurses’ high workload and tiredness. Although spiritual care is part of nursing care, nurses are often not willing to ask questions about client's spiritual needs while they are collecting data, and some nurses consider it a superstitious issue.[16] This happened in the study by Rahnama et al.; the participants who were patients suffering from cancer stated that they do not get positive energy from nurses, and nurses just pay attention to the physical aspect of their problem and pay no attention to what the patient says and do not spend time with the patient and do not soothe the patient. The participants mentioned the nurses’ high workload, lack of time, and tiredness as the barriers to spiritual support. The participants also pointed to the need for the presence of someone other than the nurse who can help them in doing religious practices and stated that there is no religious consultant or clergy in the department to help them overcome their worries. These are in line with the results of this study, and the participant in this study pointed to the necessity of having a clergy in the department. The participants also mentioned lack of a private space in the department for prayers and religious practices, which is contrary to this study. In this study, the participants were happy that there existed the required amenities for doing religious practice in the department.[17]
In addition, Moeini et al. pointed to the fact that one of the barriers to nurses providing spiritual care is that they solely pay attention to the patients’ physical problems and doing physical care.[18] In line with what they stated, Balboni et al. showed that most patients suffering from cancer do not receive spiritual care from doctors or nurses.[19] In another study conducted on mothers of children with blood cancer, Pourmovahed and Roozbeh showed that nurses do not provide the required support for mothers in terms of respecting their values, dignity, and credit.[20]
Kachoie et al. found out that doctors’ attitude toward spirituality and spiritual care is not adequate, and that doctors are unwilling to intervene in patients’ religious and spiritual affairs.[21] Also, van Leeuwen et al. concluded that nurses believe that although spirituality is one of the important areas of taking care of people suffering from cancer, it has not received due attention in taking care of patients.[22]
Family influenceability was another category in factors inhibiting spiritual care. Participants stated that the child's disease had caused some changes in their psychological state and had affected and reduced their quality of life. Economic problems and taking care of the other children were other problems that parents complained about.
In a study by Saifan et al., who investigated the experiences of parents with children suffering from cancer in the Muslim community of Jordan, parents stated that there had been changes in their family roles. For example, they stated that they were not able to provide the care they used to provide for their other children, and their presence in the hospital had caused contradiction in their parental role, and that they have to spend all their time with their ill child in the hospital or at home and, as a result, cannot pay enough attention to their other children, which leaves a negative effect on the other children.[23]
Modanloo et al. investigated family performance in parents with children suffering from cancer. The results showed that almost half of the parents with children suffering from cancer had an unhealthy general family performance. Most of the disorders were reported in the areas of solving problems and emotional blending.[24] Also, the participants in Saifan et al. stated that the permanent presence of parents in the hospital by the ill child had caused contradiction in doing their responsibilities and their jobs, and that they had to leave their job to take care of their child, which puts them in economic and financial pressure.[23]
The results of the study by Valizadeh et al. showed that the responsibility of taking care of a child suffering from cancer is above average level, and the disease affects the family in different aspects such as physical and emotional aspects of life.[25] In a study conducted by Jadidi et al. on the experiences of parents with children suffering from cancer, the participants stated that their child's disease had created a lot of problems for them, such as being fired from work, having problem paying for the expenses, or problems about taking care of the other children.[26]
With regard to factors facilitating spiritual care, five categories were identified, one of which being emotional support. The parents considered the role of emotional support on the part of their spouse, the people around them, and the medical staff to be very effective in helping them adjust to their child's disease. The support made them feel at peace.
Nurses and medical staff also play an important role in spiritual care. In a study on experiences of patients and their families, it was shown that based on their perceptions, providing spiritual care is contingent on having committed, kind, well-behaved, and committed to professional behavior nurses who are able to fulfill certain responsibilities such as expressing sympathy, giving hope to patients and their families, and helping with doing religious practices; having a cheerful and peaceful environment in the department during the hospitalization period has also been mentioned as a necessary factor.[27]
Jadidi et al. pointed to the fact that emotional support on the part of the people around plays an important role in helping parents adjust to their child's disease. Emotional support by the healthcare system also has a role to play. This support can take the form of expressing sympathy on the part of doctors, nurses, and medical staff, which pacifies the parents.[26]
In a study by Saifan et al., it was shown that the fathers offer the required support for the mothers and develop a closer relationship with their wives and, for example, help them with housework and help them better deal with the situation caused by the disease.[23]
Taheri Saeedi et al. intervened by performing a spiritual care plan based on kind heart, which involved engaging family members and their support and concluded that the spiritual care score of the patients increased in comparison to before the intervention, a finding indicating the positive effect of support on the part of people around.[28]
Healthcare support was another category obtained from the results of the study. It indicated that the medical staff, including doctors, nurses, and other people in the treatment team, can be a source of support for parents by offering information regarding the disease and providing spiritual care.
Rahnama et al. pointed to the need for spiritual empowerment of nurses and families of children suffering from cancer. They believe that people who take care of the children need to enhance their capabilities in this area. The empowerment can include educational and informational interventions for them. They also pointed to the necessity of forming a spiritual care team which should include doctors, nurses, family members of the ill child, the clergy, and the psychologist cooperate.[4]
According to a study by Atashzadeh-Shoorideh et al., spirituality affects nurses’ behavior in a positive way, and promoting spirituality in nurses results in patients and their families receiving better healthcare on the part of nurses.[29] Dunn also considers the role of spirituality in nurses, who are part of people providing care, to be very important and believes that a nurse with an inadequate level of spirituality cannot take care of patients in an appropriate way.[30]
Another issue that the participants pointed to was the role of social support, which can be achieved when hospitals provide the required amenities. Financial support from state organizations or private charities also can be effective in supporting families.
Sajadian et al. in a study conducted on healthcare problems of the companions of patients suffering from cancer pointed to the issue that paying attention to individual and social problems of the patients and their families by providing better social and economic supports results in patients and their companions better adjusting to the situation.[31] The participants in Jadidi et al.'s study, which was a qualitative study on parents with children suffering from cancer, stated that providing amenities for parents plays an important role in helping parents adjust to their children's disease.[26]
One of the important points emphasized by the participants in this study was the role played by spiritual care in helping them adjust to the situation caused by their child's disease. Spiritual help can include the people around the parents help them with performing religious practices or expressing sympathy and spending time with them and listening to their words.
Rahnama et al., in a qualitative study on spiritual care for patients suffering from cancer, observed that nurses can help the patients by taking a spiritual approach and being well-behaved, being kind, and trusting in God; trusting in God doing their job helps create a feeling of peace in patients. Nurses can provide the amenities needed by the patients to say their prayers and worship God, and whether the nurse herself believes in spiritual affairs is very effective in this regard.[17]
In a study by Mardani Hamolleh et al., which investigated spirituality in patients suffering from cancer from nurses’ perspective, the participants pointed to the importance of paying attention to and taking into consideration of the patient's spiritual values and helping the patients in this regard through, for example, trying to connect to God, spiritually supporting the patients, performing religious practices, and visiting the patient's room and listening to their words.[32]
Finally, supporting the child was identified as a facilitating category, since improving the child's spiritual and physical conditions and helping them in this regard puts their parents in a better spiritual condition and helps them adjust to their child's disease and can deal with the stressful situation caused by the disease in a better way.
Borjalilo et al., in a study on the experiences of parents regarding the spiritual challenges of having a child suffering from cancer, pointed to the issue that parents are great supporters for children and provide them with love and affection. Children face a crisis during the period of illness, and parents needs to be equipped with the abilities required for spiritually taking care of their children by identifying their children's needs and spiritual crises.[33] Also, the parents in Jadidi et al.'s study mentioned that they do their best to spiritually and psychologically support their children and satisfy their wants and wishes.[26]
Conclusion
Given that cancer is a life-threatening disease which causes tremendous stress for the patients and their families and affects their quality of life, it is necessary to take the required measures to help parents adjust to their children's disease, which of these measures being providing spiritual support. Spiritual support creates hope, peace, optimism, and adjustment to the patient's situation in crisis situations. In this regard, some factors were identified as facilitators. Enhancing these factors results in providing better spiritual care for parents. Also, eliminating or reducing factors known as inhibitors can be of great help for parents in this regard. This can be achieved through educating both parents and the medical staff.
Limitations and suggestions
Given that this study was conducted only on parents of children suffering from cancer and other family members like siblings of the ill child who are also affected by the disease and the situation caused by the disease, it is suggested that further studies be done on the experiences of other members of the family. Also, the experiences of other people involved in the issue, like the medical staff, can be taken into account to enrich the data.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
This article was part of a PhD thesis in nursing and a product of a research plan approved by the Center for Religion and Health of Shahid Beheshti University of Medical Sciences with code number IR. SBMU. REC.1395.11. The researcher would like to express her sincere gratitude to the officials in the Faculty of Nursing and Midwifery and the Center for Religion and Health of Shahid Beheshti University of Medical Sciences. Also, grateful thanks are due to all the participants in the study and the officials in the hospitals where the study was conducted.
References
- 1.Kandasamy A, Chaturvedi SK, Desai G. Spirituality, distress, depression, anxiety, and quality of life in patients with advanced cancer. Indian J Cancer. 2011;48:55–9. doi: 10.4103/0019-509X.75828. [DOI] [PubMed] [Google Scholar]
- 2.Krause N, Pargament KI, Hill PC, Ironson G. Humility, stressful life events, and psychological well-being: Findings from the landmark spirituality and health survey. J Posit Psychol. 2016;11:499–510. [Google Scholar]
- 3.Schreiter RJ. The Ministry of Reconciliation: Spirituality & Strategies. Maryknoll, NY: Orbis Books; 1998. [Google Scholar]
- 4.Rahnama M, Fallahi Khoshkenab M, Maddah SS, Ahmadi F. Designing a model for spiritual care in rehabilitation of cancer patients. Med Surg Nurs J. 2014;3:61–70. [Google Scholar]
- 5.Höcker A, Krüll A, Koch U, Mehnert A. Exploring spiritual needs and their associated factors in an urban sample of early and advanced cancer patients. Eur J Cancer Care (Engl) 2014;23:786–94. doi: 10.1111/ecc.12200. [DOI] [PubMed] [Google Scholar]
- 6.Mehranfar M, Younesi J, Banihashem A. Effectiveness of mindfulness-based cognitive therapy on reduction of depression and anxiety symptoms in mothers of children with cancer. Iran J Cancer Prev. 2012;5:1–9. [PMC free article] [PubMed] [Google Scholar]
- 7.Masa’Deh R, Collier J, Hall C. Parental stress when caring for a child with cancer in Jordan: A cross-sectional survey. Health Qual Life Outcomes. 2012;10:88. doi: 10.1186/1477-7525-10-88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rosenberg AR, Dussel V, Kang T, Geyer JR, Gerhardt CA, Feudtner C, et al. Psychological distress in parents of children with advanced cancer. JAMA Pediatr. 2013;167:537–43. doi: 10.1001/jamapediatrics.2013.628. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Timmins F, Neill F. Teaching nursing students about spiritual care – A review of the literature. Nurse Educ Pract. 2013;13:499–505. doi: 10.1016/j.nepr.2013.01.011. [DOI] [PubMed] [Google Scholar]
- 10.Pearce MJ, Coan AD, Herndon JE, 2nd, Koenig HG, Abernethy AP. Unmet spiritual care needs impact emotional and spiritual well-being in advanced cancer patients. Support Care Cancer. 2012;20:2269–76. doi: 10.1007/s00520-011-1335-1. [DOI] [PubMed] [Google Scholar]
- 11.Karekla M, Constantinou M. Religious coping and cancer: Proposing an acceptance and commitment therapy approach. Cogn Behav Pract. 2010;17:371–81. [Google Scholar]
- 12.Raffay J, Wood E, Todd A. Service user views of spiritual and pastoral care (chaplaincy) in NHS mental health services: A co-produced constructivist grounded theory investigation. BMC Psychiatry. 2016;16:200. doi: 10.1186/s12888-016-0903-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Miller L. Health Care Clinicians’ Compliance with Conducting Spiritual Assessments and Providing Spiritual Care to Infertile Women. Lesa Miller, Walden University press: Walden University. 2015 [Google Scholar]
- 14.Graneheim UH, Lundman B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24:105–12. doi: 10.1016/j.nedt.2003.10.001. [DOI] [PubMed] [Google Scholar]
- 15.Baljani E, Khashabi J, Amanpour E, Azimi N. Relationship between spiritual well-being religion and hope among patients with cancer. Haiat J. 2011;17:27–37. [Google Scholar]
- 16.Saeeidi Taheri Z, Asad Zandi M. Spirituality and spiritual care. J Schl Nurs Baqiyatallah. 2014;15:59–66. [Google Scholar]
- 17.Rahnama M, Fallahi Khoshkenab M, Maddah SS, Ahmadi F. Cancer patients perception of spiritual care. J Med Ethics Hist. 2013;5:64–80. [Google Scholar]
- 18.Moeini M, Moeini T, Musarezaie A, Sharifi S. Nurses spiritual well-being and their perspectives on barriers to providing. Iran J Crit Care Nurs. 2015;8:159–66. [Google Scholar]
- 19.Balboni MJ, Sullivan A, Amobi A, Phelps AC, Gorman DP, Zollfrank A, et al. Why is spiritual care infrequent at the end of life. Spiritual care perceptions among patients, nurses, and physicians and the role of training? J Clin Oncol. 2013;31:461–7. doi: 10.1200/JCO.2012.44.6443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Pourmovahed Z, Roozbeh B. Nursing support system for mothers of hospitalized leukemic children: A comparative study. Iran J Pediatr Hematol Oncol. 2016;6:2. [Google Scholar]
- 21.Kachoie A, Ahmari Tehran H, Dehghani F, Abbasi M, Parizad A. Physicians attitudes towards spirituality and pastoral care. J Mazandaran Univ Med Sci. 2016;26:151–60. [Google Scholar]
- 22.van Leeuwen R, Schep-Akkerman A, van Laarhoven HW. Screening patient spirituality and spiritual needs in oncology nursing. Holist Nurs Pract. 2013;27:207–16. doi: 10.1097/HNP.0b013e318294e690. [DOI] [PubMed] [Google Scholar]
- 23.Saifan A, Masa’Deh R, Hall C, Collier J. Experiences of jordanian mothers and fathers of children with cancer. J Am Sci. 2014;10:29–39. [Google Scholar]
- 24.Modanloo S, Rohani C, Abadi FS, Gholi PA. Assessment of family function among parents of children with cancer. Iran J Nurs Res. 2015;10:56–65. [Google Scholar]
- 25.Valizadeh L, Joonbakhsh F, Pashaee S. Determinants of care giving burden in parents of child with cancer at Tabriz children medical and training center. J Clin Nurs Midwifery. 2014;3:13–20. [Google Scholar]
- 26.Jadidi R, Hekmatpou D, Eghbali A, Memari F. The experiences of parents of children with leukemia: A qualitative research. Arak Med Univ J. 2013;15:28–40. [Google Scholar]
- 27.Mazaheri M, Fallahi Khoshkenab M, Maddah SS, Rahgozar M. Attitude to spirituality and spiritual care in nurses. Payesh J. 2009;8:31–7. [Google Scholar]
- 28.Taheri Saeedi Z, Asadzandi M, Ebadi A. The effect of spiritual care based on GHALBE SALIM model on spiritual experience in patients with coronary artery disease. J Psychiatr Nurs. 2013;1:45–53. [Google Scholar]
- 29.Atashzadeh-Shoorideh F, Abdoljabbar M, Karamkhani M, Khubestani MS, Pishgooie SA. The relationship between nurses’ spiritual health and their caring behaviors. J Res Relig Health. 2017;3:5–15. [Google Scholar]
- 30.Dunn LL. Spirituality and nursing: Personal responsibility. Online J Rural Nurs Health Care. 2012;8:3–4. [Google Scholar]
- 31.Sajadian A, Heidari L, Mokhtari Hesari P. The problems in caregivers of patients with breast cancer. Iran J Breast Dis. 2015;8:7–14. [Google Scholar]
- 32.Mardani Hamolleh M, Borimnejad L, SeiedFatemi N, Tahmasebi M. Palliative care based on spirituality in cancer patients from the perspective of nurses: Qualitative study. J Med Hist. 2013;5:141–65. [Google Scholar]
- 33.Borjalilo S, Shahidi S, Fathabadi J, Mazaheri MA. Spiritual issues and challenges children with cancer: Parents experience. Health Psychol. 2014;3:37–54. [Google Scholar]