

Abstract
Background and Objective:
Basic life support (BLS) and cardiopulmonary resuscitation (CPR) are urgently required and must be performed when cardiac arrest occurs. These lifesaving procedures must be learned by healthcare professionals. In developed countries, members of the public, academics, and students learn how to carry out these emergency procedures. Knowledge of these simple procedures determines successful outcome. This study was conducted to determine the level of awareness of BLS and CPR among female secondary students at governmental schools in Riyadh city, Saudi Arabia (SA).
Methods:
This cross-sectional study was conducted in five governmental secondary schools in Riyadh city, SA, between June 2015 and June 2016. Total of 1224 female students were selected randomly, and data were collected using a self-reported structured questionnaire.
Results:
A total of 1170 participants completed the questionnaire. Most of the participants (81.5%) were Saudis. More than 50% of the students (54.8%) did not have information about BLS, and 82.6% felt their knowledge about BLS was insufficient. Only 10.8% of the participants had taken a BLS course, and only 38.5% believe BLS courses should be mandatory.
Conclusion:
The level of awareness regarding BLS among female secondary school students in governmental schools in Riyadh was found to be insufficient. The introduction of BLS and CPR courses in the curriculum of governmental secondary schools in Riyadh city is highly recommended.
Keywords: Awareness, basic life support, female students, governmental schools, secondary school students
Introduction
Basic life support (BLS) is a simple and effective maneuver that if performed well and in a timely manner will increase survival rate in most emergency situations.[1,2,3]
This indicates the need for teaching and training non-health professionals and laypersons to provide effective and safe resuscitation prior to hospital care, as outcome would improve significantly according to several published studies.[4,5]
Many studies have been conducted internationally to explore the public knowledge and attitude toward BLS among different groups. In particular, studies done on high school students showed variable knowledge and attitude toward BLS.
In a Danish study, high school students were found to have poor knowledge about BLS, and the majority were afraid of doing BLS, but knowledge and self-confidence increased significantly after conducting training sessions.[6]
Another study done in Germany found that only 29.5% of high school students performed chest compression correctly. The rate increased to 99.2% post-training and to 99% in 4 months period.[7] With regard to attitude, a study in Norway which included 376 secondary school students showed that majority are willing to perform cardiopulmonary resuscitation (CPR).[8]
In Lublin, Poland, a study found poor knowledge of first aid, where 67% of high school students claimed that their skills are insufficient.[9] Similar findings were reported by Sosada et al. in another Polish study in 2002.[10] In New Zealand, a study done by Parnell et al. in 2006 revealed willingness and motivation among high school students toward learning CPR but poor knowledge score with a mean of 5.61 out of 18.[11] Positive attitude of secondary school students in Rivers State, Nigeria, toward learning of BLS was also reported.[12]
There is an increasing prevalence of risk factors for cardiac diseases among both youth and adults in Saudi Arabia (SA), which makes learning BLS essential for both public and healthcare professionals. The incidence of some chronic diseases, such as diabetes mellitus, hypertension, obesity, and hyperlipidemia, has increased in SA by 8%–9% in adults, and such conditions result in the urgent need to educate the population about BLS and CPR.[13,14,15]
In addition, children and young adults are the age groups most affected by trauma and injuries, and it is expected that a significant percentage of trauma and injuries occurs during school time since children and young adults spend a significant amount of time at school.[16]
Locally, insufficient studies are done to reveal school students’ knowledge of and attitude toward BLS. A study done in Riyadh, on 580 secondary school students, found that 56% of them did not have accurate CPR information, and about 67% of all students were willing to know more about CPR.[17]
In Taif, SA, a cross-sectional study was done on 360 male secondary school students to assess the awareness of secondary school students regarding first aid and BLS. The mean score of the students’ knowledge was 64.8%, and the trained students (79.6%) reported both better first aid knowledge and skills than untrained students (53.7%). This study emphasized the necessity for integrating the subject into the core curriculum of schools, which could help in disseminating the culture of emergency care in the general population.[18]
At the level of school teachers, a cross-sectional study was done and enrolled 118 female staff from different schools of both governmental and private sectors in Jeddah City, SA, and examined the readiness of primary school staff and students to respond to emergency situations, such as cardiac arrest. It was found that the participants had insufficient knowledge about CPR. However, participants’ attitude toward first aid training was positive, and such training was desired among the participants.[19] A similar study was done in Riyadh, which showed similar results.[20]
Since there are only few published studies done in SA about this topic, we conducted this study focusing on female students in governmental secondary schools in Riyadh, SA, to explore BLS and CPR awareness level and related factors.
Methodology
This a cross-sectional study conducted in Riyadh, SA, between June 2015 and June 2016. The study targeted female students, Saudis, and non-Saudis in government secondary schools from grades 10, 11, and 12. To our knowledge, two studies had been conducted in SA to assess the knowledge of BLS and CPR among secondary school students. The first one, published 2015, was done in Taif, SA, among boy students with a sample size of 360 students.[12] The other study was conducted in 2013 with a sample size of 580 for both male and female secondary school students in Riyadh, SA.[13] We choose to do this study among female students with larger sample size for comparison with previous local studies. We also choose female students to investigate the assumption that female students may be less oriented than males in a country like SA due to less exposure of females to situations that need BLS.
Riyadh's population of secondary girl schools reached to 81,076 female students. The study's sample size was calculated assuming 50% anticipated prevalence (proportion), 95% confidence interval, and 5% error and was found to be 377 participants. Clustered stratified sampling was chosen, and Riyadh schools were divided into five female secondary school strata. The preliminary sample size was multiplied by the design effect, which equals 3.245, and the required sample size becomes 1,224 secondary school students. The list of all female governmental schools was obtained from the Ministry of Education in Riyadh, and the schools were distributed, as per geographical distribution of Riyadh provinces, into five main clusters (North, South, West, Central, and East). Then, using cluster sampling to account for the percentage of each school from the total population (81,067), the distribution of the sample size was allocated as follows: South area = 24.5% × 1,224 ≈ 299, North area = 21.2% × 1,224 ≈ 260, West area = 19.5% × 1,224 ≈ 239, Center area = 16.0% × 1,224 ≈ 196, and East area = 18.8% × 1,224 = 230 students. One school was chosen randomly to represent each geographical area in a clustered stratified sampling with two phases and a random technique.
Data were collected using a self-administered structured questionnaire that was administered to female students in class with explanation, and agreement to participate was considered as an informed consent.
The questionnaire was self-structured and modified with the help of a previous, similar study questionnaire.[21] The questionnaire was validated by three expert consultants and reliability was ensured after consulting a biostatistician and piloting. The questionnaire consisted of two main parts. The first part contained sociodemographic data (age, level of education, nationality, parent's level of education, parent's occupation, and family income). The second part contained questions about BLS and CPR awareness levels. The questionnaire was developed initially in English and then it was translated into Arabic language. Translation was verified by two experts.
After collection, data were coded with a 1 for “Yes” answers and a 2 for “No” answers. Multiple-choice questions were awarded numbers from 1 to 6, depending on the number of options provided. Data were then entered into Statistical Package for Social Sciences (SPSS) for Windows, version 21.0 (SPSS Inc., Armonk, New York, USA). Categorical data were presented as percentage and frequency. The association between different variables was calculated using Chi-squared test of association. P value less than 0.05 was considered to be statistically significant.
Ethical approval for the study was obtained from the Ethical Committee, Prince Sultan Military Medical City, and from the Ministry of Education, SA. Privacy and confidentiality were maintained during data collection. The age group of students ranged from 15 to 18 years old (grades 10, 11, and 12 secondary school). SA rules considered age above 14 years as an adult and competent to consent without a need for parental consent. The authors report no conflict of interest.
Results
Of 1224, 1170 participants completed the questionnaire with a response rate of 95.5%. As shown in Table 1, most of the participants (81.5%) were Saudis. With regard to school grades, students were distributed to grades 10, 11, and 12 with a percentage of 37.2%, 33.0%, and 29.8%, respectively.
Table 1.
Sociodemographic characteristics of participants (n=1170)
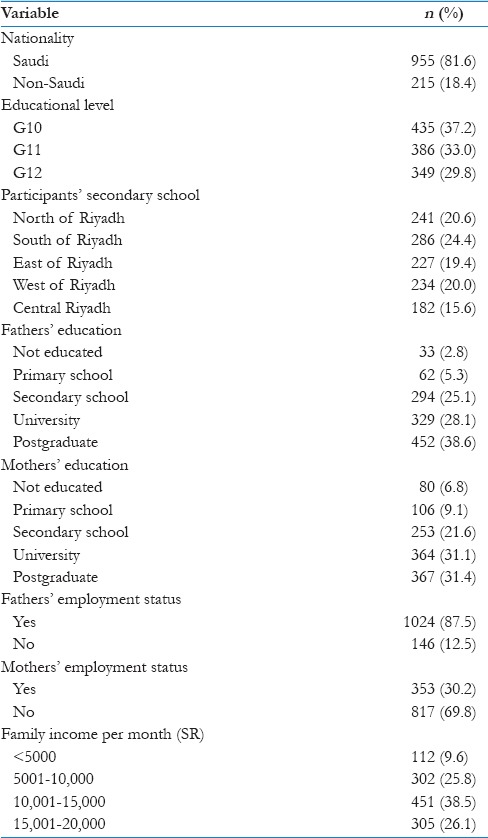
Regarding participants’ educational backgrounds, 38.6% of the students’ fathers had postgraduate degrees, while just 2.8% of the students’ fathers had no education. Similarly, 31.4% of the students’ mothers had postgraduate degrees, while 6.8% of the students’ mothers had no education. Most of the fathers (87.5%) were employed, while most of the mothers (69.8%) were not.
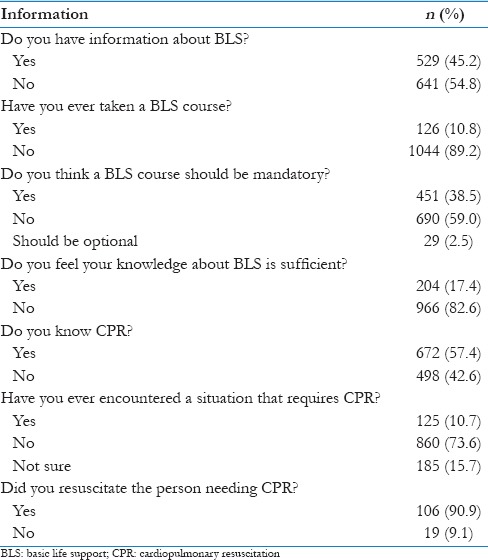
The level of BLS and CPR knowledge as reported by participants themselves and their perception of sufficiency of their knowledge are presented in Table 2. The results showed that 54.8% of participants considered themselves not having information about BLS, only 10.8% had taken a BLS course, 82.6% think they have insufficient knowledge about BLS, and 38.5% thought BLS courses should be mandatory in school curriculum. With regard to participants, CPR knowledge results showed that 42.6% did not know what CPR means, 10.7% had encountered a situation that requires CPR, and 90.9% of them conducted the resuscitation process.
Table 2.
Perception, attitude, and practice of participants about basic life support and cardiopulmonary resuscitation (n=1170)
The association between students’ educational levels and nationality with BLS awareness is presented in Table 3. The results showed a statistically significant association between grade 12 level and taking BLS course (P = 0.056). There was also an association between grade 10 students and sufficient BLS knowledge (P = 0.001). Grade 12 students believed that BLS courses should be mandatory (P = 0.001).
Table 3.
Association between education level and nationality with perception, attitude, and practice of basic life support/cardiopulmonary resuscitation (n=1170)
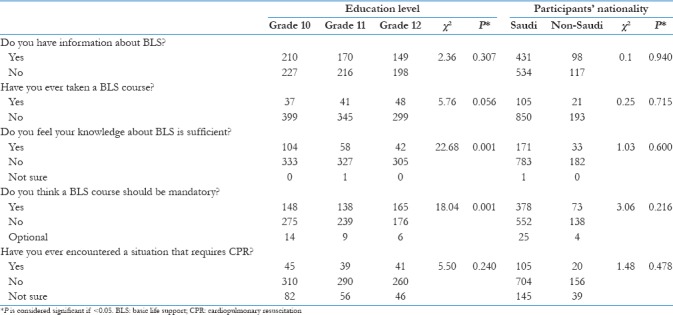
No significant association was found between participants’ BLS knowledge and their nationality. As shown in Table 4, there was an association between family monthly income and BLS awareness. Students with a high income took BLS courses more than students with a low income (P = 0.026), and students with moderate-to-high income had more BLS information than students with low income (P = 0.003). With regard to association between school location within Riyadh and BLS awareness, southern area's school students have more information about BLS than other areas, followed by the Eastern area, and the least student awareness was in the Northern area (P = 0.001). Furthermore, Southern area's school students were more interested in having BLS courses as a mandatory subject in their curriculum when compared with other areas (P = 0.012).
Table 4.
Association between family's income and school location with perception, attitude, and practice of basic life support/cardiopulmonary resuscitation (n=1170)
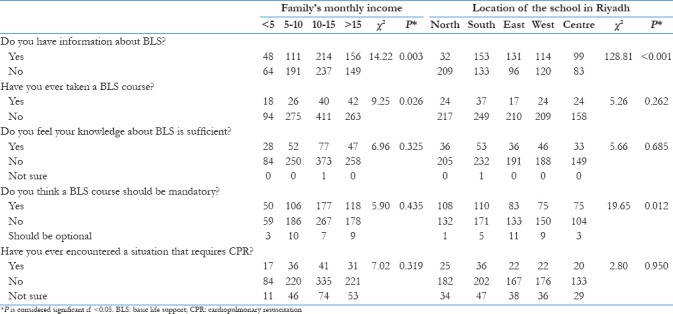
Figure 1 shows that majority of the students had obtained their BLS knowledge from the Internet, followed by information from their schools, while TV and radio presented the least source of information. Figure 2 describes the participants’ main reasons for taking a BLS course. The majority of the participants attended BLS course for personal benefit, while the remaining attended the course due to past experiences. Figure 3 shows that 82.50% participants believed that they have insufficient BLS knowledge. As shown in Figure 4, 57.40% of participants believed that they had CPR knowledge. Figure 5 shows that in an emergency, most of the participants (45.60%) would begin CPR, 32.30% would call an ambulance, and 22.10% would take victims to the hospital.
Figure 1.
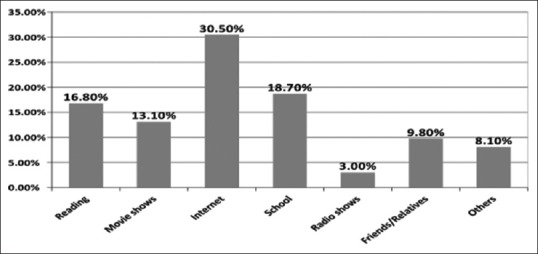
Source of basic life support information
Figure 2.
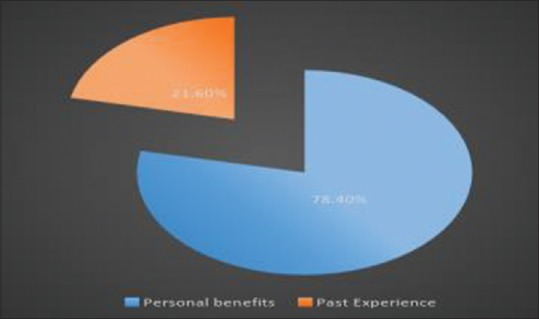
Reasons for taking a basic life support course
Figure 3.
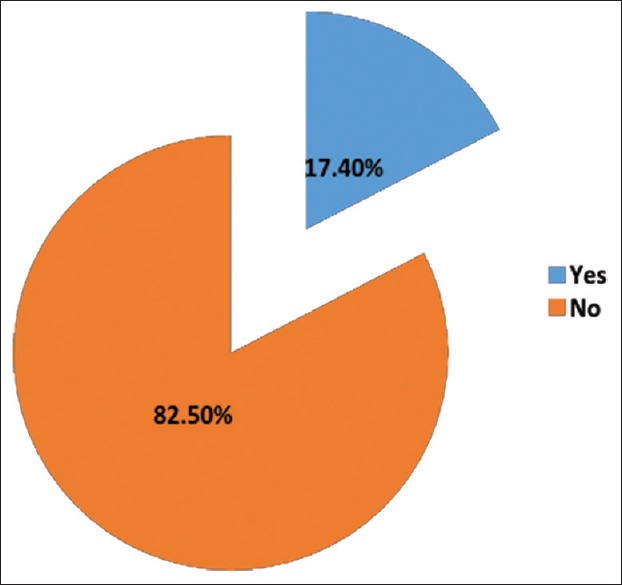
Do you feel your knowledge about basic life support is sufficient?
Figure 4.
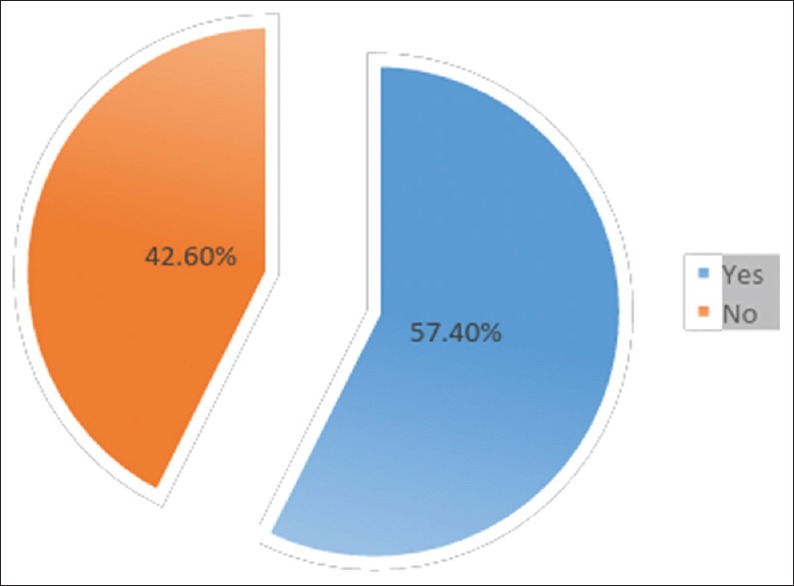
Do you feel your knowledge about cardiopulmonary resuscitation is sufficient?
Figure 5.
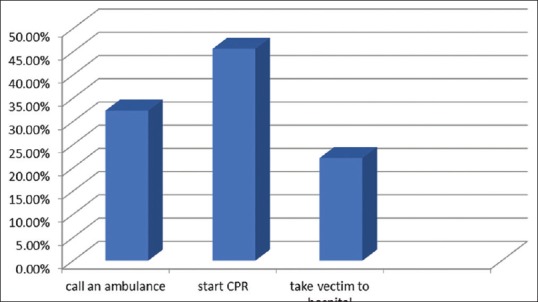
Participants’ reaction to BLS situation
Figure 6 shows the participants’ reactions to CPR situations. The majority of participants (45.5%) would first check the airways for breathing, while 25.9% would first do chest compressions, and 6.60% would first give mouth-to-mouth breathing.
Figure 6.
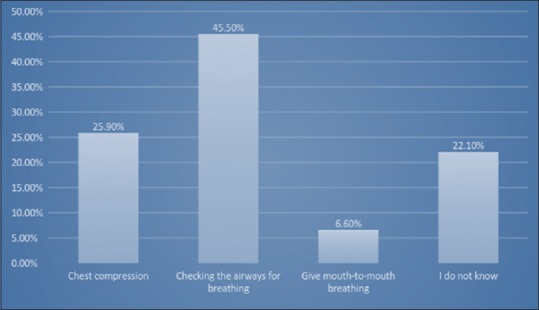
Participants’ reaction to a CPR situation
Discussion
This study comprised a relatively large sample size of female secondary school students (a total of 1224 with a response rate of 95.5%) compared with prior local studies, and this may enable investigator toward more generalizability.
The majority of students were Saudis, and this is expected since the governmental schools by law accept non-Saudis in a small proportion. The level of education and employment status of parents reflect the usual trends in Saudi community where both males and females have the same opportunity of higher education, but employment status is different. This finding was also documented in the study by Mobarak et al.[18]
In our study, we found poor level of awareness about BLS and CPR as perceived by the participants; 54.8% reported not having information about BLS and 42.6% did not know CPR. In comparison, this is similar to the study by Alanazi et al. where they found that only 58.1% and 58% for female and male students, respectively, have proper information about CPR.[17] This is also comparable to the findings of other study done in Taif, SA, where the mean participants’ first aid knowledge score was 64.8%.[18]
If compared to international study, New Zealand high school students showed poor theoretical CPR knowledge, with a mean score of 5.61 out of a maximum score of 18,[11] and in Denmark, only 28% students knew how to correctly recognize normal breathing.[6]
The finding of poor BLS and CPR knowledge in our study can be contributed to lack of structured educational and training course of first aid in public schools in SA. The school curriculum contains simple instruction for first aid measures like safety measures at home, but there are no structured courses of BLS, neither for teachers nor for students. Unfortunately, poor knowledge on BLS extended to university students. In a local study done to evaluate BLS knowledge among health students at a Saudi Women's University, 87.9% of the participants had very poor knowledge scores in BLS.[22]
With regard to the number of students who had attended BLS courses, only 10.8% reported taking BLS course and this was found more among grade 12 students and students of families with high income. The correlation of BLS course attendance with high grade is expected assuming students become more aware about importance of BLS as they grow, while correlating with high income may be explained by the fact that most of the organized BLS courses are not free in this country.
A similar finding was reported by Mobarak et al.,[18] and less to what was reported by the other local study where 35% of male and female high school students have some training in CPR.[17] The international figures are variable. For example, 63% of the Danish high school students had participated in prior BLS training,[21] 89% of high school students in Norway had BLS training,[6] 59% among Japanese students,[23] and one-third of students had attended a first aid course in a study done in Germany.[7]
Several reasons may contribute to poor attendance to BLS courses in our population, but at the top of the list may be the lack of awareness among decision-makers in the field of education about the importance of BLS/CPR and that secondary schools’ curriculum in SA does not include BLS/CPR training. Secondary school students may not recognize well the importance of this life-saving measure by themselves, despite the fact schools are the ideal setting to educate and train for BLS.
Every member of the community should have excellent BLS knowledge and practice, and the best strategy to reach to this goal would begin by educating the community's future leaders: school students. Once the initiatives have been taken by decision-makers, it is expected that students will be well-oriented and will have the chance to be trained on BLS/CPR in well-organized and free short courses in a protected time at school. An evidence-based educational pathway with educational goals concerning learning first aid for each age group is available.[24,25] This may be used to include first aid training in school curricula. It was shown that students will gain more knowledge and skills and be more confident in performing CPR if they attended BLS courses even if trained by school teachers not by health professionals.[26,27,28] Barriers should be considered in planning for structured BLS for school students such as large population, cost, and lack of instructors,[29] and other alternatives should also be considered such as video presentation, slide show, and software game platforms.[30]
Only 38.5% of students in this study thought BLS courses should be mandatory in school curriculum, and this was again found to be more among grade 12 students, which may reflect maturity of thinking and better awareness with time. This low percentage actually is worrisome and may be explained by the poor knowledge and awareness of BLS among the students themselves. If we compare this to international studies, the majority of school students in Croatia, for instance, have positive attitude toward BLS training even in primary schools.[31]
With regard to readiness of students to perform CPR, the findings of this study indicate that participants’ readiness is also low, where less than half (45.6%) stated they would start CPR immediately in a requiring situation, 32.3% would call an ambulance rather than starting CPR, and 20.1% prefer to take the victim immediately to the hospital. In the study by Alanazi et al., almost similar finding was obtained where 67% of students would be willing to perform CPR on a member of their families or relatives, but only one-third of them would be willing to perform it on strangers.[17] When compared to international findings, only 27% of high school students in Japan reported willingness to perform CPR[23] and it reached to 83% among students in Norway.[8]
There are certain factors that may negatively influence students with regard to BLS training and condition. This may include fear of failure as rescuer, fear of injuring victim, fear of dealing with strangers, fear of disease transmission, and fear of being in contact with victim secretions.[22,31] Addressing these concerns should be part of any future course of BLS/CPR. It was shown clearly that if students are trained and educated well about BLS, their concerns will be less and their readiness and willingness to perform CPR will improve.[6]
In our study, although only 10.7% had encountered a situation that requires CPR, 90.9% of them conducted the resuscitation process and that may reflect positive attitude toward BLS.
Southern area's school students were found to have more information about BLS and were more interested in having BLS courses as a mandatory subject. Although in Riyadh city there are certain social and financial characteristics that differentiate southern area from other areas, it is not fully understood how that difference affects knowledge and attitude of students toward BLS. The findings reflect unequal awareness between the different areas and schools and this would encourage authors to recommend adding BLS courses as a mandatory subject in the curriculum, and hence, awareness will be generalized and equalized among everyone.
Regarding source of information about BLS, almost one-third of participants had got their information from the Internet, followed by schools. This clearly shows that role of school in providing students with information about BLS is lacking and stresses the need for the Ministry of Education to include this vital information and such life-saving topics in the curriculum. Adding BLS to the secondary school curriculum will advance BLS knowledge in those parts of the country where Internet service is unavailable. In comparison to the other local study, findings are different where the main source of information about first aid was TV for 56.4% of participants, followed by parents (43.4%), books (39.2%), and teachers (33.6%).[12] This difference of findings may be due to different settings and population in both studies.
Conclusion
This study highlighted female secondary school students’ poor knowledge and awareness of BLS and CPR; therefore, this issue needs to be promptly addressed. To do this, BLS and CPR skills should be included in curriculum, the Ministry of Education must raise BLS awareness campaigns, and CPR training should be increased. Furthermore, it is recommended that BLS course should not only be incorporated in the curriculum but also regular refresher courses are necessary and should be designed to provide hands-on experience. Nowadays, things are changing and Saudi female have become more active in community participation in different aspects, mainly education and health sectors. It is expected that female can be activists in the field of first aid and life-saving projects.
Limitations
This study has some limitations that may partially affect the generalizability of results. The level of awareness and BLS/CPR skills in this study was based on self-report of students and not obtained through objective scoring or assessment method, and therefore, more objective methods need to be undertaken for more accurate knowledge assessment. Recall bias regarding BLS-specific questions could not be excluded from students’ responses.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Neumar RW, Shuster M, Callaway CW, Gent LM, Atkins DL, Bhanji F, et al. Part 1: Executive summary: 2015 American Heart Association Guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2015;132:S315–67. doi: 10.1161/CIR.0000000000000252. [DOI] [PubMed] [Google Scholar]
- 2.Geri G, Fahrenbruch C, Meischke H, Painter I, White L, Rea TD, et al. Effects of bystander CPR following out-of-hospital cardiac arrest on hospital costs and long-term survival. Resuscitation. 2017;115:129–34. doi: 10.1016/j.resuscitation.2017.04.016. [DOI] [PubMed] [Google Scholar]
- 3.Ringh M, Jonsson M, Nordberg P, Fredman D, Hasselqvist-Ax I, Håkansson F, et al. Survival after public access defibrillation in Stockholm, Sweden – A striking success. Resuscitation. 2015;91:1–7. doi: 10.1016/j.resuscitation.2015.02.032. [DOI] [PubMed] [Google Scholar]
- 4.Hasselqvist-Ax I, Riva G, Herlitz J, Rosenqvist M, Hollenberg J, Nordberg P, et al. Early cardiopulmonary resuscitation in out-of-hospital cardiac arrest. N Engl J Med. 2015;372:2307–15. doi: 10.1056/NEJMoa1405796. [DOI] [PubMed] [Google Scholar]
- 5.Plant N, Taylor K. How best to teach CPR to schoolchildren: A systematic review. Resuscitation. 2013;84:415–21. doi: 10.1016/j.resuscitation.2012.12.008. [DOI] [PubMed] [Google Scholar]
- 6.Aaberg AM, Larsen CE, Rasmussen BS, Hansen CM, Larsen JM. Basic life support knowledge, self-reported skills and fears in Danish high school students and effect of a single 45-min training session run by junior doctors; a prospective cohort study. Scand J Trauma Resusc Emerg Med. 2014;22:24. doi: 10.1186/1757-7241-22-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Meissner TM, Kloppe C, Hanefeld C. Basic life support skills of high school students before and after cardiopulmonary resuscitation training: A longitudinal investigation. Scand J Trauma Resusc Emerg Med. 2012;20:31. doi: 10.1186/1757-7241-20-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kanstad BK, Nilsen SA, Fredriksen K. CPR knowledge and attitude to performing bystander CPR among secondary school students in Norway. Resuscitation. 2011;82:1053–9. doi: 10.1016/j.resuscitation.2011.03.033. [DOI] [PubMed] [Google Scholar]
- 9.Goniewicz M, Chemperek E, Mikuła A. Attitude of students of high schools in lublin towards the problem of first aid. Wiad Lek. 2002;55(Suppl 1):679–85. [PubMed] [Google Scholar]
- 10.Sosada K, Zurawiński W, Stepień T, Makarska J, Myrcik D. Evaluation of the knowledge of teachers and high school students in Silesia on the principles of first aid. Wiad Lek. 2002;55(Suppl 1):883–9. [PubMed] [Google Scholar]
- 11.Parnell MM, Pearson J, Galletly DC, Larsen PD. Knowledge of and attitudes towards resuscitation in New Zealand high-school students. Emerg Med J. 2006;23:899–902. doi: 10.1136/emj.2006.041160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Onyeaso AO, Imogie AO. Attitude towards cardiopulmonary resuscitation among some secondary school students in Rivers State, Nigeria. Br J Educ. 2014;2:37–43. [Google Scholar]
- 13.Ng SW, Zaghloul S, Ali HI, Harrison G, Popkin BM. The prevalence and trends of overweight, obesity and nutrition-related non-communicable diseases in the Arabian Gulf states. Obes Rev. 2011;12:1–3. doi: 10.1111/j.1467-789X.2010.00750.x. [DOI] [PubMed] [Google Scholar]
- 14.Aljefree N, Ahmed F. Prevalence of cardiovascular disease and associated risk factors among adult population in the Gulf region: A systematic review. Advances in Public Health. 2015;2015:1–23. [Google Scholar]
- 15.El Bcheraoui C, Memish ZA, Tuffaha M, Daoud F, Robinson M, Jaber S, et al. Hypertension and its associated risk factors in the Kingdom of Saudi Arabia, 2013: A National Survey. Int J Hypertens 2014. 2014:564679. doi: 10.1155/2014/564679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.World Health Organization. Injuries and Violence: The Facts 2014. World Health Organization; 2014. [Google Scholar]
- 17.Alanazi A, Bin-Hotan AM, ALhalyabah H, Alanazi A, Al-oraibi S. Community awareness about cardiopulmonary resuscitation among secondary school students in Riyadh. World J Med Sci. 2013;8:186e–9. [Google Scholar]
- 18.Mobarak AS, Afifi RM, Qulali A. First aid knowledge and attitude of secondary school students in Saudi Arabia. Health. 2015;7:1366–78. [Google Scholar]
- 19.Bashir SM, Bakarman MA. Are our children in safe hands. Evaluating the preparedness of primary school staff in Jeddah, Saudi Arabia in responding to health related emergencies? Life Science J. 2014;11:986–9. [Google Scholar]
- 20.Alharbi MM, Horaib YF, Almutairi OM, Alsuaidan BH, Alghoraibi MS, Alhadeedi FH, et al. Exploring the extent of knowledge of CPR skills among school teachers in Riyadh, KSA. J Taibah Univ Med Sci. 2016;11:497–501. [Google Scholar]
- 21.Al-Turki YA, Al-Fraih YS, Jalaly JB, Al-Maghlouth IA, Al-Rashoudi FH, Al-Otaibi AF, et al. Knowledge and attitudes towards cardiopulmonary resuscitation among university students in Riyadh, Saudi Arabia. Saudi Med J. 2008;29:1306–9. [PubMed] [Google Scholar]
- 22.Al-Mohaissen MA. Knowledge and attitudes towards basic life support among health students at a Saudi women's university. Sultan Qaboos Univ Med J. 2017;17:e59–65. doi: 10.18295/squmj.2016.17.01.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Omi W, Taniguchi T, Kaburaki T, Okajima M, Takamura M, Noda T, et al. The attitudes of Japanese high school students toward cardiopulmonary resuscitation. Resuscitation. 2008;78:340–5. doi: 10.1016/j.resuscitation.2008.03.233. [DOI] [PubMed] [Google Scholar]
- 24.Cave DM, Aufderheide TP, Beeson J, Ellison A, Gregory A, Hazinski MF, et al. Importance and implementation of training in cardiopulmonary resuscitation and automated external defibrillation in schools: A science advisory from the American Heart Association. Circulation. 2011;123:691–706. doi: 10.1161/CIR.0b013e31820b5328. [DOI] [PubMed] [Google Scholar]
- 25.De Buck E, Van Remoortel H, Dieltjens T, Verstraeten H, Clarysse M, Moens O, et al. Evidence-based educational pathway for the integration of first aid training in school curricula. Resuscitation. 2015;94:8–22. doi: 10.1016/j.resuscitation.2015.06.008. [DOI] [PubMed] [Google Scholar]
- 26.Bohn A, Lukas RP, Breckwoldt J, Böttiger BW, Van Aken H. ‘Kids save lives’: Why schoolchildren should train in cardiopulmonary resuscitation. Curr Opin Crit Care. 2015;21:220–5. doi: 10.1097/MCC.0000000000000204. [DOI] [PubMed] [Google Scholar]
- 27.Naqvi S, Siddiqi R, Hussain SA, Batool H, Arshad H. School children training for basic life support. J Coll Physicians Surg Pak. 2011;21:611–5. doi: 10.2011/JCPSP.611615. [DOI] [PubMed] [Google Scholar]
- 28.Lukas RP, Van Aken H, Mölhoff T, Weber T, Rammert M, Wild E, et al. Kids save lives: A six-year longitudinal study of schoolchildren learning cardiopulmonary resuscitation: Who should do the teaching and will the effects last? Resuscitation. 2016;101:35–40. doi: 10.1016/j.resuscitation.2016.01.028. [DOI] [PubMed] [Google Scholar]
- 29.Hart D, Flores-Medrano O, Brooks S, Buick JE, Morrison LJ. Cardiopulmonary resuscitation and automatic external defibrillator training in schools: “Is anyone learning how to save a life? CJEM. 2013;15:270–8. doi: 10.2310/8000.2013.130898. [DOI] [PubMed] [Google Scholar]
- 30.Creutzfeldt J, Hedman L, Heinrichs L, Youngblood P, Felländer-Tsai L. Cardiopulmonary resuscitation training in high school using avatars in virtual worlds: An international feasibility study. J Med Internet Res. 2013;15:e9. doi: 10.2196/jmir.1715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Petrić J, Malički M, Marković D, Meštrović J. Students’ and parents’ attitudes toward basic life support training in primary schools. Croat Med J. 2013;54:376–80. doi: 10.3325/cmj.2013.54.376. [DOI] [PMC free article] [PubMed] [Google Scholar]