

Abstract
The purpose of this study was to assess survival to discharge of animals with surgical or postmortem confirmation of a lung lobe torsion (LLT) as well as to evaluate pre-operative effusion, lung lobe affected, and patient size as prognostic indicators. Medical records search identified 35 dogs and 4 cats with a confirmed diagnosis including 17 small-breed dogs, 18 large-breed dogs, 3 domestic shorthair cats, and 1 minskin cat. Lobes affected included right middle (n = 18), left cranial (n = 18), right cranial (n = 2), left caudal (n = 1), and accessory (n = 1). Two animals died before surgery; the remaining 37 animals underwent thoracotomy. All treated small-breed dogs and cats survived; 12/18 large-breed dogs survived, with an overall survival to discharge of 87%. Pre-operative pleural effusion and affected lung lobe did not affect survival to discharge in this population. Small dogs and cats with LLT appear to have an excellent survival to discharge following thoracotomy and the survival is good in larger dogs.
Résumé
Torsion de lobe pulmonaire chez 35 chiens et 4 chats. Le but de cette étude est d’évaluer le taux de survie jusqu’à la sortie d’hôpital, chez des animaux ayant eu confirmation chirurgicale ou post-mortem de torsion de lobe pulmonaire (TLP), ainsi que d’évaluer la présence d’épanchement pleural, le lobe pulmonaire affecté et la taille des patients en tant que facteurs pronostics. Les dossiers médicaux de 35 chiens et 4 chats avec un diagnostic de TLP confirmé furent identifiés, comprenant 17 chiens de petite race, 18 chiens de grande race, 3 chats Européens et 1 Minskin. Les lobes pulmonaires affectés étaient le lobe moyen droit (n = 18), le lobe cranial gauche (n = 18), le lobe cranial droit (n = 2), le lobe caudal gauche (n = 1) et le lobe accessoire (n = 1). Deux animaux décédèrent avant chirurgie, et une thoracotomie fut pratiquées chez les 37 animaux restant. Tous les chiens de petites races et les chats survécurent à leur chirurgie; 12/18 des chiens de grande race survécurent, et le taux de survie global était de 87 %. La présence d’épanchement pleural et le lobe pulmonaire affecté n’avaient pas d’influence sur la probabilité de survie dans cette population. Le taux de survie au congé hospitalier semble excellent chez les chiens de petite taille et les chats diagnostiqués avec une torsion de lobe pulmonaire et il est bon pour les chiens de grande taille.
(Traduit par les auteurs)
Introduction
Lung lobe torsion (LLT) is uncommon in dogs and rare in cats, although it is commonly suggested as an important differential diagnosis following radiographic evidence of pulmonary consolidation (1–4). Lung lobe torsion occurs when a lung lobe twists on its pedicle, resulting in edema, emphysema, and necrosis of the lung lobe. Treatment of LLT includes most commonly a lateral thoracotomy and removal of the affected lobe. Median sternotomy may be performed if definitive diagnosis or the lung lobe affected is unclear, or if there is bilateral thoracic involvement. Like isolated splenic torsion, it is important that lobes are not untwisted before resection to avoid release of inflammatory cytokines and toxins (5).
Lung lobe torsion has been documented in both small and large breed dogs with pugs and Afghan hounds being over-represented (2,3). It has been suggested that, similar to the proposed mechanisms for gastric dilatation and volvulus, deeper-chested dogs may have more room in their thoracic cavity to allow for the lungs to shift and subsequently torse (2). In a study by Murphy and Brisson (3), 13/23 affected dogs were small breed, with pugs representing 7/13 (54%) of those dogs. No other specific breed predilections have been reported, nor has impact of breed or size on survival to discharge been previously evaluated. Lung lobe torsion is far less common in cats, in which it has been associated with chronic upper respiratory infection, asthma, diaphragmatic hernia, chylothorax, and neoplasia (6–11).
Diagnostics performed most commonly to identify LLT include thoracic radiographs, and abnormalities reported radiographically include increased lobar opacity or consolidation, vesicular gas pattern, displaced lung lobe or lobar bronchus, progressive bronchial opacification, mediastinal shift, tracheal displacement, axial rotation of the carina, irregular, narrowed, or blunted bronchus, and pleural effusion (1). Chronic pleural effusion has been considered a risk factor for the development of LLT, although primary LLT itself may trigger accumulation of pleural effusion due to associated necrosis and inflammation (2,3).
The goal of this study was to describe the clinical characteristics and survival to discharge of dogs and cats which develop LLT, specifically, to evaluate if pre-operative pleural effusion, lung lobe affected, or animal size has an effect on survival to discharge.
Materials and methods
Case selection criteria and medical records review
The electronic medical record database for the Cummings School of Veterinary Medicine at Tufts University was searched from January 1, 2002 to December 31, 2016 for “lung lobe torsion” and each medical record was reviewed. Animals were included if they had a confirmed diagnosis of LLT at the time of thoracotomy or necropsy regardless of any other patient characteristics. The medical records were reviewed and data recorded on breed, age and weight at presentation, gender, affected lung lobe, diagnostic imaging modalities used and imaging reports in the medical record, presence of pre-operative pleural effusion, presence of fever at presentation, surgical approach for animals undergoing surgery, peri-operative complications, potentially predisposing conditions, if any identified, and survival to discharge. Complete imaging reports for studies not performed at Tufts University were not included in the medical records and these images were not available for further review at the time of this retrospective study. Predisposing conditions included any disease predisposing a patient to pleural effusion, the presence of pleural effusion, or a history of thoracic trauma (2). Dogs were considered small breed if they weighed < 15 kg consistent with that used in a previous study (3). The institutional Animal Care and Use Committee approval and owner consent were waived due to the retrospective nature of the study.
Statistical analysis
Fisher’s exact test was used to compare survival to discharge based on patient size, lung lobe affected, surgical approach, number of surgeries performed, and presence or absence of pre-operative pleural effusion with a P-value < 0.05 considered significant. Odds ratios (OR) and 95% exact confidence intervals (CI) were calculated for each association.
Results
Signalment
Over the study period, 35 dogs and 4 cats met the inclusion criteria. Of the affected dogs, 10 (29%) were pugs, 8 (23%) were mixed breed, 2 (6%) each were Great Pyrenees, golden retriever, and Labrador retriever, and 1 (3%) each was a collie, Bernese mountain dog, boxer, English bulldog, Irish wolfhound, English springer spaniel, toy poodle, cocker spaniel, Pekingese, Lhasa apso, and French bulldog. Seventeen (49% of dogs) were small breed, and 18 (51% of dogs) were large breed, including 6 of the mixed breed dogs. Of the affected cats, 3 were domestic shorthairs and 1 was a minskin (12). Eighteen animals were castrated males, 17 were spayed females, 3 were intact males (including a 4-month-old Labrador retriever and a 5-month-old Great Pyrenees), and 1 was an intact female (French bulldog). Seven of the 10 affected pugs were male. Median age was 4 y (range: 4 mo to 12 y).
Presenting complaint and history
Presenting complaints included anorexia or decreased appetite (n = 23), respiratory distress (n = 20), lethargy (n = 16), cough (n = 13), tachypnea (n = 10), vomiting (n = 5), gagging (n = 2), weight loss (n = 2), and collapse (n = 1). Duration of clinical signs was both acute and chronic ranging from < 12 h to up to 3 mo. Thirteen animals (33%) also had a documented fever (temperature > 39.4°C), at the time of presentation. Eleven animals (28%) had received antimicrobials before confirmation of LLT. Three animals (8%) sustained vehicular trauma at 2, 3, or 5 wk before presentation and all 3 had a diaphragmatic hernia and pleural effusion identified on pre-operative imaging or at the time of thoracotomy in addition to the LLT. Cats and dogs appeared to display similar clinical signs. All cats and all but 3 dogs were presented with complaints of respiratory compromise including tachypnea, respiratory distress, and cough. The 3 dogs without respiratory signs had a combination of anorexia, lethargy, and fever and duration of clinical signs ranging from 3 to 10 d.
Diagnostic imaging: Thoracic radiographs
All 39 animals had thoracic radiographs taken within 72 h of initial presentation to Tufts University or their primary care veterinarian. Twenty-six animals had radiographs taken and interpreted by the diagnostic imaging service at Tufts University, while 13 animals had radiographs taken at their primary care veterinarian before referral. For the 26 animals with radiography done at Tufts University, the most commonly documented radiographic abnormalities included pulmonary consolidation (n = 26), pleural effusion (n = 20), vesicular pattern of an individual lung lobe (n = 14), and lack of visualization of the bronchus or vasculature within the affected lung lobe (n = 12) (Figures 1 and 2). Of these 26 animals, 15 had LLT as the primary differential diagnosis and 7 were considered to have LLT as a differential diagnosis. In the other 4 animals, LTT was not suspected based on radiographs, although 3 had pleural effusion obscuring visualization of the lung lobes and 1 had a large volume pneumothorax. Interestingly, in only 2 of the 4 cats was LLT suspected based on radiographs alone. Thirteen animals had thoracic radiographs taken at their primary care veterinarian with 8 of these cases suspected of having an LLT either by the referring veterinarian, admitting clinician at Tufts University, or a Tufts University radiologist. Overall, of 39 animals with thoracic radiography, LTT was suspected in 30 cases.
Figure 1.

Left lateral radiograph showing torsion of the right middle lung lobe with abnormal positioning of the bronchus and vasculature (A), vesicular gas pattern (B), and moderate volume pleural effusion (C) as evidenced by the scalloping of the ventral lobe margins and retraction of the lobes from the thoracic wall and diaphragm.
Figure 2.

Left lateral radiograph with air-trapping in the ventral aspect of a torsed right middle lung lobe creating a vesicular gas pattern (*) with complete consolidation of the lobe.
Diagnostic imaging: Computed tomography
Eighteen animals (46%) had computed tomography (CT) performed either to confirm the presence of LLT before surgery, for surgical planning, or to exclude concurrent pathology. The most common findings on CT scan included pulmonary consolidation (n = 18), pleural effusion (n = 15), abnormal tapering or blunting of the bronchus (n = 15), vesicular pattern (n = 12), lack of visualization of the bronchus or vasculature within the affected lobe (n = 8), decreased or absent contrast enhancement (n = 8), and enlargement of the affected lobe (n = 7) (Figures 3–5). Following CT, 15 animals were identified with LLT, and 2 animals had LLT as the leading differential diagnosis. The 1 remaining dog was thought to have a cavitated, gas-filled, caudal thoracic mass on CT, and LLT was not suspected until it was identified surgically.
Figure 3.

Transverse CT image demonstrating abrupt tapering of the right middle lobar bronchus (A) just distal to the origin with central vesicular gas pattern (B) and peripheral soft tissue attenuation.
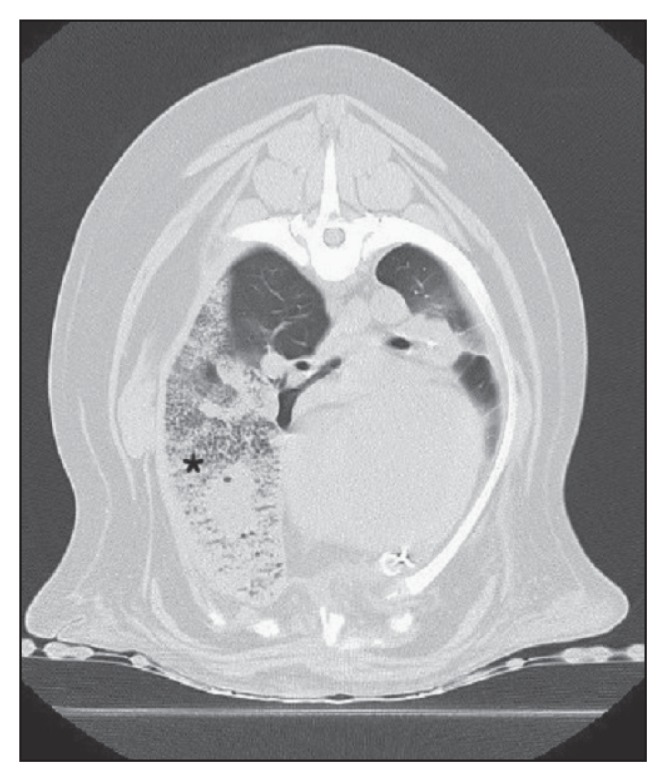
Figure 4.

Axial CT image demonstrating soft tissue attenuation of the left cranial lung lobe (*) with inability to trace the bronchi of the cranial and caudal segments.
Figure 5.
Transverse CT image demonstrating increased soft tissue attenuation in the region of the right cranial and right middle lung lobes with vesicular gas pattern (*).
Other diagnostic modalities
Eight animals (21%) had bronchoscopy performed, with 4 pugs suspected of having LLT based upon radiographs having the diagnosis confirmed on bronchoscopy alone. The choice to perform bronchoscopy in the pugs for confirmation of LLT was due to the quickness with which the procedure can be performed prior to surgery and the higher frequency with which pugs are affected with LLT, thus increasing the likelihood of confirming a diagnosis with bronchoscopy alone. Findings consistent with LLT were seen in all 8 animals on bronchoscopy and included a folding or pinching of the bronchus and inability to advance the scope into the affected lung lobe (Figure 6). Two dogs and 1 cat had thoracic ultrasonography with both color doppler and standard 2D images obtained; 1 study only documented pulmonary consolidation with severe pleural effusion, and the remaining 2 studies suggested a pulmonary mass or abscess. These studies were helpful in confirming the presence of pulmonary pathology, but did not further characterize the patient as having an LLT.
Figure 6.

Bronchoscopic image with collapse and twisting of the left cranial bronchus (*) with inability to advance the scope further into the bronchus.
Affected lung lobes
Lung lobes affected included the right middle (n = 18), left cranial (n = 17), right cranial (n = 2), left caudal (n = 1), and accessory lobe (n = 1) (Figure 7). Eight of 10 pugs (80%) had left cranial LLTs and 2 had right cranial LLTs. Fourteen of 18 large breed dogs had right middle LLTs which accounted for the majority (78%) of all right middle LLTs. The single left caudal LLT was in a domestic shorthair cat and the accessory LLT was in the English bulldog. Four of the remaining non-pug small breed dogs had left cranial LLTs and 3 had right middle LLTs.
Figure 7.

Affected lung lobes with number of animals affected in a population of 35 dogs and 4 cats with lung lobe torsion.
Pleural effusion
Thirty-five animals (90%) had pleural effusion at presentation or developed effusion before surgery. Of animals that were treated surgically with pre-operative pleural effusion, 27/33 survived to discharge; all 4 animals without pre-operative pleural effusion survived, but this difference was not significant (P = 0.59; OR: ∞; 95% CI: 0.12 to ∞). When comparing the 2 most commonly affected lung lobes, the right middle LLT was more commonly associated with pre-operative pleural effusion than was the left cranial LLT based on the Fisher exact test, but not based on the OR 95% CI (18/18, 100% versus 13/17, 76%, P = 0.04; OR: ∞; 95% CI: 0.76 to ∞), and a cause for this disparity was not identified.
Surgical intervention
Following diagnosis, 37 animals were treated with surgical removal of the affected lobe. Thirty-one (84%) had a lateral thoracotomy performed (15 right-sided, 16 left-sided) and 6 (16%) had a median sternotomy. The surgical approach was dictated by lung lobe affected, concurrent disease in the case of patients with diaphragmatic hernia, and surgeon preference.
Survival to discharge
One small breed dog was euthanized before surgery due to significant co-morbidities, including pleural effusion believed to be caused by a cranial vena cava thrombus associated with a transvenous pacemaker lead wire and 1 cat arrested after thoracocentesis due to a tension pneumothorax. Both animals which died before surgery had the diagnosis of LLT confirmed on postmortem examination. The cat was also identified to have a pulmonary carcinoma in addition to the LLT. Among the remaining 37 animals treated surgically, all animals survived the initial surgery but only 31 animals (28 dogs and 3 cats) survived to discharge. Thirteen of eighteen (72%) patients with right middle LLT survived to discharge and 14/17 (82%) patients with left cranial LLT survived to discharge. Small breed dogs, including pugs, had significantly improved survival over large breed dogs (17/17, 100% versus 12/18, 67%, P = 0.02; OR: ∞; 95% CI: 1.33 to ∞).
Six animals (16%) died post-thoracotomy. One, previously proteinuric, dog developed anuric renal failure and died 2 d after surgery, and another, the adult Great Pyrenees, developed torsion of a remaining lobe and was euthanized 2 d post-surgery after the owners declined a second surgery. Four animals underwent an additional rescue thoracotomy between 1 and 6 d following initial surgical intervention due to either persistent pneumothorax (n = 3) or hemorrhage (n = 1). All 4 animals which underwent a second thoracotomy died; 2 of the 4 were euthanized within 24 h of the second thoracotomy due to persistent air leak, and 2 suffered cardiopulmonary arrest — one within 24 h of surgery and one 3 d after surgery.
Dogs with a history of traumatic diaphragmatic hernia were seemingly less likely to survive to discharge (1/3, 33%) compared to animals without trauma (30/34, 88%), but this did not reach statistical significance (P = 0.06; OR: 15; 95% CI: 0.57 to 912). Animals which had a median sternotomy as the initial surgical approach were significantly less likely to survive to discharge than those with a lateral thoracotomy, based on Fisher exact test, but not based on the OR 95% CI (3/6, 50% versus 28/31, 90%, P = 0.04; OR: 9.3; 95% CI: 0.79 to 101). Additionally, requiring a second surgery to control air leak or hemorrhage was also a negative prognostic indicator as all dogs did not survive, compared with animals that had only 1 surgery (0/4, versus 31/33, P < 0.01; OR: ∞; 95% CI: 5.3 to ∞).
Discussion
This study reviews the characteristics and survival to discharge of dogs and cats affected with LLT. As previously described, younger to middle-aged dogs are most commonly affected, but LLT can occur in dogs of any age. In 1 study, the median age for small breed dogs affected was 7 y (range: 1 to 10 y); the median age for large breed dogs was 3.5 y (range: 2 to 7 y) (3). All pugs in that study were < 5 y old indicating this patient population may become affected at a younger age. Lung lobe torsion has been reported in other studies in dogs as young as 7 wk and as old as 14 y (2,13). In the current study, median age was 4 y, and 4 patients were < 1 y old. One Labrador retriever and 1 Great Pyrenees were 4- and 5-months-old, respectively, and 2 pugs were 8- and 10-months-old at the time of diagnosis. This is consistent with findings of a recent study of 7 juvenile dogs suffering from LLT (14) and emphasizes the importance of maintaining LLT as a differential diagnosis in young animals. The age range for affected pugs was 8 mo to 9 y (median: 2.5 y) with all but a single pug being < 6 y old, which is similar to previous reported findings (3,14).
Males appear to be over-represented in prior studies (2,3), but the case numbers were small in these studies as well as the current study. In this study, 21 animals (54%) were male with 7 pugs (70%) being male.
The most common presenting complaints observed in animals in this study were anorexia or decreased appetite and respiratory distress followed by lethargy, cough, and tachypnea. The duration of clinical signs for LLT is typically short, lasting from 1 to 3 wk, although in some cases, duration of clinical signs may be up to several months (2). In this study, the median duration of clinical signs before presentation was 6 d (range: < 12 h to 3 mo). Most animals (27/39, 69%) had clinical signs lasting ≤ 1 wk. Tachypnea and respiratory distress are the most common physical examination findings, though they are non-specific for LLT. Pale mucous membranes, abdominal discomfort, and fever may also be seen. In fact, fever was commonly identified in this study with a third of the patients having temperatures > 39.4°C. Fever has previously been reported in animals with LLT (2,3), and fever may prompt the clinician to consider pneumonia, particularly in the presence of pulmonary consolidation, which likely explains why many animals are often treated with antibiotics before identification of the LLT.
All animals had thoracic radiographs taken either at Tufts University or by their primary care veterinarian. Radiographs were considered diagnostic or suspicious for LLT in 30/39 cases (77%). A vesicular pattern, while typically associated with LLT (1), was only observed in 14/26 (54%) thoracic radiographs performed at Tufts University and in 12/18 (67%) CT scans, which is important, as the absence of a vesicular pattern does not exclude an LLT. A correct diagnosis of LLT was made following CT scan in 94% of cases. Computed tomography is likely more sensitive at identifying LLT in many cases due to its tomographic nature and the ability to more clearly visualize the pulmonary and bronchial structures without superimposition of concurrent pleural effusion. One dog in which CT did not accurately identify LLT had a torsion of the accessory lung lobe; the accessory lung lobe rarely torses (1–3,15), so this diagnosis was not suspected based upon CT.
Lung lobes affected are variable, with the left cranial lobe most commonly affected in pugs and the right middle lobe most commonly affected in large breed dogs (2,3). These findings were confirmed in the present study with the left cranial lobe affected in 80% of pugs and the right middle lobe affected in 78% of large breed dogs. However, the pathophysiology for development of LLT and why certain lobes are more commonly affected are poorly understood. Lung lobe torsion is thought to be associated with consolidation or atelectasis of the affected lobe(s) and a subsequently more freely moveable lobe (1). The predilection for different lobes to be affected may have to do with breed conformation or underlying cause (2,15); however, this could not be clarified from the current study. One study of bronchial abnormalities in brachycephalic dogs identified a higher rate of left cranial lobe collapse in pugs and suggested this anatomical variant may be relevant in the high frequency of LLT in this breed (16).
Overall survival to discharge was 87% which is improved from results reported in studies by Neath et al (2) and by Murphy and Brisson (3). Small breed dogs had a significantly improved survival compared with large breed dogs in this study. This is consistent with findings in a previous study (2) in which all 5 of the affected small breed dogs, including 2 pugs, survived. This is in contrast to the Murphy and Brisson study (3), in which the survival to discharge was 50% for both small and large breed dogs when pugs were excluded. In that study, 6/7 pugs survived, and in the current study, 10/10 pugs survived, supporting the previously suspected association with survival for pugs.
Pleural effusion is a common finding in animals with LLT, but whether it is a causative factor or is secondary to congestion and edema from the LLT is difficult to differentiate. Thirty-five animals (90%) in the current study had evidence of pleural effusion on imaging or at the time of surgery; however, in only 3 dogs was the presence of pleural effusion confirmed before the identification of LLT, including 1 dog with caval thrombosis associated with a pacemaker lead wire, 1 with chronic pleural effusion associated with protein-losing nephropathy, and 1 dog with mesothelioma. Conversely, in the Labrador retriever puppy being treated for suspected pneumonia, the absence of pleural effusion was documented, then within 12 h the puppy developed a large volume of pleural effusion and associated lung lobe torsion suggesting that pleural effusion could be either causative or a result of LLT, depending on the case. It is important to note that, in contrast to the study by Neath et al in 2000 (2), not all patients herein had pleural effusion, so the absence of pleural effusion must not be used to rule out LLT. When comparing the 2 most commonly affected lung lobes, the right middle LLT was more commonly associated with pre-operative pleural effusion than was left cranial LLT, but a cause for this disparity was not identified. The right middle lung lobe is considered the most mobile (15), so it may be more likely to result in pleural effusion when torsed or be the first lobe to torse in the presence of pleural effusion.
For surgical approach, most of the animals (84%) had a lateral thoracotomy to gain access to the affected lobe. Six animals (16%) had median sternotomies performed either because multiple lung lobes appeared to be affected or due to concurrent disease. Such was the case of 1 animal with a history of trauma and recently corrected diaphragmatic hernia to allow for exposure of all lung lobes to assess for any other undiagnosed thoracic injury. Animals which had a median sternotomy as the initial surgical approach may have been less likely to survive to discharge than those with a lateral thoracotomy, although statistical significance is uncertain based on the OR 95% CI. Furthermore, if true, this association may be, at least in part, a manifestation of concurrent disease such as previous thoracic trauma and not the result of surgical approach alone. A recent study compared short-term outcomes in dogs with median sternotomy versus intercostal thoracotomy for lung lobectomy (17). This study reported that a median sternotomy had increased post-operative hypoxemia and a trend toward an increased rate of hemorrhage and/or death compared with lateral thoracotomy, so increased morbidity due to surgical approach could play a role in decreased survival. Four dogs needed a second surgical procedure due to tension pneumothorax or persistent hemorrhage following initial lung lobectomy. None of these dogs survived, which was statistically significant compared with dogs that only required a single surgery (P < 0.01). To the authors’ knowledge, no previous studies have evaluated the effect of number of surgeries on survival to discharge for LLT.
The current study revealed a population of animals which developed LLT that, to the authors’ knowledge, has not previously been described; 3 dogs (8%) suffered from vehicular trauma and diaphragmatic hernia occurring 2 to 5 wk before the diagnosis of LLT. The diaphragmatic hernias are presumed to be initially acute secondary to the trauma, but all 3 of these dogs were presented ≥ 2 wk following the traumatic incident, classifying them as chronic at the time of surgery based on previous criteria used in an evaluation of chronic diaphragmatic hernias in dogs and cats (18). While thoracic trauma has been reported as a potential predisposing factor or cause for LLT (1–3), traumatic diaphragmatic hernia has not explicitly been shown to be a cause for LLT. There is a single case study of a Jack Russell terrier (19) that developed LLT 10 d following abdominal exploration and correction of a large diaphragmatic hernia, but this patient had no known history of trauma. The data available for these patients make it impossible to make a definitive causative association between traumatic diaphragmatic hernia and LLT. All dogs with traumatic diaphragmatic hernia also had large volumes of pleural effusion which may have predisposed them to development of the LLT. Alternatively, it is possible that the trauma itself resulted in both the diaphragmatic hernia and lung lobe torsion and subsequent formation of effusion. For dogs with trauma, the right middle (n = 2) and left cranial (n = 1) lobes were affected and all were large breed dogs. The survival rates reported by Minihan et al (18) for surgical repair of chronic diaphragmatic hernias are better than those in this study (86% versus 33%), which may indicate increased mortality associated with the LLT or differences in study populations.
The surgical procedure recommended for treatment of LLT in animals is thoracotomy with resection of the affected lung lobe. In human medicine, LLT is primarily a post-operative complication following upper lung lobectomy and most commonly affects the right middle and left lower lobes (20,21), though it can be seen with thoracic trauma, large volume pleural effusion, or other invasive thoracic procedures. To minimize this risk of torsion following lung lobectomy in humans, clinicians describe surgical pexy of the remaining lobes (20,22,23) by various methods including use of a pleural flap, suturing lung to adjacent structures in the thorax, suturing the middle and lower lobes together, and the use of various medical grade adhesive materials. Post-surgical LLT is rarely recognized in dogs. In the current study, there was a single dog which developed additional LLT (identified on CT) of the right middle and right cranial lung lobes following surgical resection of a left cranial LLT and an initial good recovery. This dog was euthanized at the time of the second torsion and may have benefited from surgical pexy. Criteria have not been established for determining which animals, if any, are at increased risk for LLT following lung lobectomy and would benefit from lung pexy. Further veterinary studies on the safety and efficacy of lung lobe pexy are needed to determine if this would be of benefit in cases of lung lobectomy following lung lobe torsion. No recommendation can be made at this time concerning lung lobe pexy as a viable option for this patient population.
This study was limited by the retrospective study design and incomplete medical records, primarily pertaining to history and the possibility of any predisposing factors as well as conclusive radiographic findings for animals that did not have imaging performed at the teaching hospital. Reported findings for thoracic radiographs may have been skewed by incomplete documentation by the primary clinician of the findings on radiographs performed at primary care hospitals before referral. For those imaging studies performed at Tufts University, only the reports and not the individual images obtained were reviewed at the time of this study. Radiographic and other diagnostic imaging findings may have been biased by multiple reviewers instead of a single specialist reviewing all imaging. Furthermore, only short-term outcome (e.g., survival to discharge) could be ascertained as follow-up records were not available long-term for most animals. Finally, the small sample size of this study and in particular, the very small sample size of some of the analyzed groups may infer a significant bias, and results may not be corroborated when applied to the general population.
In conclusion, we found that lung lobe affected, and presence of pre-operative pleural effusion did not significantly affect survival to discharge for patients treated surgically for LLT in this population of dogs and cats. Small breed and large breed dogs were equally affected, but small breed dogs had significantly improved survival to discharge. As with other studies, pugs were over-represented, making up over 25% of the patients. Surgical complications necessitating a second surgical exploration were associated with a grave prognosis. Overall, this study supported a good survival to discharge for LLTs treated surgically. CVJ
Footnotes
Presented in abstract form at the 2017 American College of Veterinary Internal Medicine Forum, National Harbor, Maryland, USA, June 2017.
Use of this article is limited to a single copy for personal study. Anyone interested in obtaining reprints should contact the CVMA office (hbroughton@cvma-acmv.org) for additional copies or permission to use this material elsewhere.
References
- 1.d’Anjou MA, Tidwell AS, Hecht S. Radiographic diagnosis of lung lobe torsion. Vet Radiol Ultrasound. 2005;46:478–484. doi: 10.1111/j.1740-8261.2005.00087.x. [DOI] [PubMed] [Google Scholar]
- 2.Neath PR, Brockman DJ, King LG. Lung lobe torsion in dogs: 22 cases (1981–1999) J Am Vet Med Assoc. 2000;217:1041–1044. doi: 10.2460/javma.2000.217.1041. [DOI] [PubMed] [Google Scholar]
- 3.Murphy KA, Brisson BA. Evaluation of lung lobe torsion in Pugs: 7 cases (1991–2004) J Am Vet Med Assoc. 2006;228:86–90. doi: 10.2460/javma.228.1.86. [DOI] [PubMed] [Google Scholar]
- 4.Gicking JC, Aumann M. Lung lobe torsion. Compend Contin Educ Vet. 2011;44:E1–E4. [PubMed] [Google Scholar]
- 5.Monnet E. Lungs. In: Tobias KM, Johnston SA, editors. Veterinary Surgery Small Animal. St Louis, Missouri: Saunders Elsevier; 2012. pp. 1752–1768. [Google Scholar]
- 6.Hambrook LE, Kudnig ST. Lung lobe torsion associated with a chronic diaphragmatic hernia and haemorrhagic pleural effusion in a cat. J Feline Med Surg. 2012;14:219–223. doi: 10.1177/1098612X12439270. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Mclane MJ, Buote NJ. Lung lobe torsion associated with chylothorax in a cat. J Feline Med Surg. 2011;13:135–138. doi: 10.1016/j.jfms.2010.09.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dye TL, Teague HD, Poundstone ML. Lung lobe torsion in a cat with chronic asthma. J Am Anim Hosp Assoc. 1998;34:493–495. doi: 10.5326/15473317-34-6-493. [DOI] [PubMed] [Google Scholar]
- 9.Brown NO, Zontine WJ. Lung lobe torsion in the cat. Vet Radiol Ultrasound. 1976;17:219–223. [Google Scholar]
- 10.Schultz RM, Peters J, Zwingenberger A. Radiography, computed tomography, and virtual bronchoscopy in four dogs and two cats with lung lobe torsion. J Small Anim Pract. 2009;50:360–363. doi: 10.1111/j.1748-5827.2009.00728.x. [DOI] [PubMed] [Google Scholar]
- 11.Millard RP, Myers JR, Novo RE. Spontaneous lung lobe torsion in a cat. J Vet Intern Med. 2008;22:671–673. doi: 10.1111/j.1939-1676.2008.0086.x. [DOI] [PubMed] [Google Scholar]
- 12.Sweeney JT, Oura TJ, Wulster KB, Aarsvold S. What is your diagnosis? J Am Vet Med Assoc. 2016;248:1235–1237. doi: 10.2460/javma.248.11.1235. [DOI] [PubMed] [Google Scholar]
- 13.Hansen NL, Hall SA, Lavelle R, Christie BA, Charles JA. Segmental lung lobe torsion in a 7-week-old Pug. J Vet Emerg Crit Care. 2006;16:215–218. [Google Scholar]
- 14.Latimer CR, Lux CN, Sutton JS, Culp WTN. Lung lobe torsion in seven juvenile dogs. J Am Vet Med Assoc. 2017;251:1450–1456. doi: 10.2460/javma.251.12.1450. [DOI] [PubMed] [Google Scholar]
- 15.Gelzer AR, Downs MO, Newell SM, Mahaffey MB, Fletcher J, Latimer KS. Accessory lung lobe torsion and chylothorax in an Afghan hound. J Am Anim Hosp Assoc. 1997;33:171–176. doi: 10.5326/15473317-33-2-171. [DOI] [PubMed] [Google Scholar]
- 16.De Lorenzi D, Bertoncello D. Bronchial abnormalities found in a consecutive series of 40 brachycephalic dogs. J Am Vet Med Assoc. 2009;235:835–840. doi: 10.2460/javma.235.7.835. [DOI] [PubMed] [Google Scholar]
- 17.Bleakley S, Phipps K, Petrovsky B, Monnet E. Median sternotomy versus intercostal thoracotomy for lung lobectomy: A comparison of short-term outcome in 134 dogs. Vet Surg. 2017;00:1–10. doi: 10.1111/vsu.12741. [DOI] [PubMed] [Google Scholar]
- 18.Minihan AC, Berg J, Evans KL. Chronic diaphragmatic hernia in 34 dogs and 16 cats. J Am Anim Hosp Assoc. 2004;40:51–63. doi: 10.5326/0400051. [DOI] [PubMed] [Google Scholar]
- 19.Terzo E, Pink J, Puggioni A, Shiel R, Andreoni V, McAllister H. Right cranial lung lobe torsion after a diaphragmatic rupture repair in a Jack Russell terrier. Ir Vet J. 2008;61:170–174. doi: 10.1186/2046-0481-61-3-170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Dai J, Xie D, Wang H, et al. Predictors of survival in lung torsion: A systematic review and pooled analysis. J Thorac Cardiovasc Surg. 2016;152:737–745. doi: 10.1016/j.jtcvs.2016.03.077. [DOI] [PubMed] [Google Scholar]
- 21.Cable DG, Deschamps C, Allen MS, et al. Lobar torsion after pulmonary resection: Presentation and outcome. J Thorac Cardiovasc Surg. 2001;122:1091–1093. doi: 10.1067/mtc.2001.117839. [DOI] [PubMed] [Google Scholar]
- 22.Le Pimpec-Barthes F, Arame A, Pricopi C, Riquet M. Prevention of middle lobe torsion or bronchial plication using anti-adhesive membrane: A simple, safe, and uncomplicated technique. Eur J Cardiothorac Surg. 2011;39:1059–1060. doi: 10.1016/j.ejcts.2010.09.033. [DOI] [PubMed] [Google Scholar]
- 23.Kutlu CA, Olgac G. Pleural flap to prevent lobar torsion: A novel technique. Eur J Cardiothorac Surg. 2006;30:943–944. doi: 10.1016/j.ejcts.2006.09.015. [DOI] [PubMed] [Google Scholar]