

Abstract
PURPOSE:
This study aimed to examine how accelerometer-assessed physical activity accumulation patterns (e.g., is activity performed daily or only one or two days a week or is activity accrued in bouts) may affect the association with mortality.
METHODS:
Adults (N = 3438), aged 40 years and older, who wore an accelerometer (ActiGraph 7164), were drawn from the longitudinal follow-up of the National Health and Nutritional Examination Survey (NHANES, 2003–2006), a population-based survey of the United States. Accelerometer-assessed moderate-to-vigorous physical (MVPA) was described by activity patterns. Participants engaging in the majority of their activity on only one or two days a week were classified as ‘weekend warriors’. Activity bouts were defined as a period of at least moderate intensity lasting at least 10 minutes. Bout characteristics included bout frequency and length. Mortality was assessed through National Death Index matching through 2013. Mortality rates were compared among groups with different activity patterns.
RESULTS:
Over an average follow-up of 77.4 months, 394 deaths occurred. Compared to participants with <37.5 minutes of MVPA per week, those with greater amounts of activity had a 60–69% mortality rate reduction after adjusting for relevant covariables. Similar risk reductions were found when contrasting weekend warriors with those who were more frequently active. An increase of one MVPA bout per week was associated with an 13% increased mortality rate. Bout duration was not associated with mortality.
CONCLUSION:
Physical activity is associated with decreased mortality rate, even among those who are active one or two days a week.
Keywords: Epidemiology, accelerometer, exercise, adults, population-based
INTRODUCTION
While there is consensus that physical activity can provide many health benefits(1–5), it remains under debate as to how best to accrue physical activity and if different activity patterns have similar benefits. United States (U.S.) federal physical activity guidelines recommend at least 150 minutes of moderate-to-vigorous intensity physical activity per week, performed in bouts of at least 10 minutes.(6) However, there is little guidance as to how people should accumulate that activity (e.g., on how many days of the week?). In fact, other physical activity guidelines have recommended activity be performed five days a week or “most days of the week”(7, 8), leaving the issue unresolved.
There remains a question if there are similar health benefits when someone performs the majority of their activity on a few days rather than a smaller amount each day, a pattern sometimes called the ‘weekend warrior’ pattern. Previous studies have shown that weekend warriors have at least as much reduced mortality risk as more regular exercisers,(9–12) but also may be susceptible to greater injury rates.(13) However, these studies of the weekend warrior have relied on self-reported activity, which may be susceptible to recall limitations and may not provide detailed enough data to look at activity sessions or bout characteristics in greater detail. The next logical question may be “for the same total activity time, is it better to engage in many sessions of shorter duration, or fewer longer sessions of activity”.
Objective measures of assessment such as those from accelerometers, may allow us to examine in greater detail the impact of physical activity patterns on health. Accelerometers objectively assess activity continuously in real-time, capturing all the activity throughout the day and not just leisure-time activity.(14) In addition, detailed time data allows for the examination of patterns characteristics such as frequency and duration of activity with greater precision. Few studies have used accelerometers to examine activity patterns and mortality.(15, 16) Evenson et al, using latent class analysis, identified participants who were most active only on the weekends, but did not observe any deaths within this group using this definition.(15) It remains of interest to expand upon this work by relaxing the definition to one or two days, without requiring them to be weekend days, and examining a wider range of weekly total activity. Saint-Maurice et al reported that similar reductions in mortality were observed independent of the proportion of activity performed in activity bouts.(16) The aim of this study was to utilize detailed information from accelerometer-assessed physical activity to examine the association of physical activity patterns, such as the weekend warrior and activity bouts, with mortality in a population-based cohort study.
METHODS
Study Population
Participants were drawn from the National Health and Nutrition Examination Survey (NHANES), a population-based study of the U.S., comprising both an interview and an in-person medical examination.(17) Accelerometry was first added to NHANES in 2003–2004 and 2005–2006 to objectively assess physical activity and sedentary behavior.(18) This study included 5461 adults (aged ≥ 40 years) who wore an accelerometer during the 2003–2004 or 2005–2006 NHANES cycles. Participants were excluded if the monitor was not properly calibrated or reliable (n = 341), had fewer than six valid days of wear (described below, n = 1678), or were lost to mortality follow-up as of 2013 (n = 4). The final analytical sample was 3438 participants. All participants provided written consent and all study procedures were approved by the research ethics review board at the National Center for Health Statistics.
Accelerometer-Assessed Physical Activity
Accelerometers are small, portable devices that assess physical activity by measuring accelerations over time. Participants were asked to wear the accelerometer, an ActiGraph 7164 (ActiGraph Inc, Pensacola, FL), on their right hip for seven days during waking hours. Acceleration data were collected every minute along the vertical axis of the hip. After the week of wear, the data were then downloaded to a computer and assessed for ‘wear time’, periods of time the accelerometer was actually worn by the participant, using a standard algorithm. Briefly, non-wear time was defined as 90 consecutive minutes of no activity provided there were 30 minutes of no activity up and downstream.(19) A valid day was conventionally defined as day of 10 or more hours of wear.(18) To examine physical activity patterns over a week, a minimum of six valid days was required for the present analysis.
We first calculated the amount of time spent per week in moderate-to-vigorous intensity physical activity (MVPA) using previously validated cutpoints.(20) MVPA was defined as any minute where the accelerometer registered ≥ 1952 counts, where a count is a summary measure of the intensity of acceleration over time. We were interested in not only the amount of MVPA participants engaged in per week, but also how that MVPA was accrued over the week. To examine this, we created physical activity profiles based on the amount of MVPA and the weekly accrual pattern. The MVPA categories were based on the federally recommended 150 minutes of MVPA per week, but without any minimum bout length restriction.(6) Within each MVPA category (inactive: <37.5, insufficiently active: 37.5-<150, and sufficiently active: ≥150 minutes per week), we then examined two patterns of physical activity accrual: “weekend warriors”, who accrued ≥ 50% of their weekly MVPA on only one or two days, and “regularly active” participants who spread their activity over the entire week. This definition was chosen a priori to satisfy the definition of a ‘majority of activity on the weekends’. This resulted in a total of five physical activity profiles: 1) inactive group (< 37.5 minutes of MVPA per week); 2) regular, but insufficiently active group participating in 37.5 to <150 minutes; 3) weekend warrior with insufficient weekly activity group with 37.5 to <150 minutes; 4) regularly active group who met the guidelines (≥ 150 minutes per week); and 5) weekend warrior group who met the guidelines (≥ 150 minutes per week).
While the “weekend warrior” pattern focuses on the number of physically active days, we were also interested in smaller windows of time, i.e. sessions or bouts of physical activity. The U.S. federal physical activity guidelines recommend physical activity be accrued in periods of 10 minutes or more.(6) We defined MVPA bouts as periods of MVPA lasting at least 10 consecutive minutes with one or two minutes allowance below the MVPA threshold.(18) We calculated three bout characteristics: 1) the number of bouts per week, 2) the average bout duration, and 3) the maximum bout duration.
Participant Characteristics and Mortality Follow-up
Participant characteristics such as age, gender, race, education, smoking status, alcohol use, healthy eating index, body mass index, diabetes status (self-reported physician diagnosis), and physical function and limitations were assessed during the interview and in-person examination. Mortality follow-up was conducted via National Death Index linkage through December 31, 2013. Deaths were excluded if they occurred within the first 24 months of follow-up (n = 115) to minimize bias from individuals who were inactive because they were sick. Detailed survey protocols and mortality linkage procedures are described elsewhere.(17, 21)
Statistical Analyses
Participant characteristics were described by physical activity profile. To examine the rate of mortality between weekend warriors and regularly active participants, hazard ratios (95% confidence intervals) were calculated using Cox survival analysis. In order to compare weekend warriors and regularly active participants at the same total MVPA volume, we adjusted for weekly MVPA volume. Weekend warriors and regularly active participants were compared two ways: 1) within physical activity groups and 2) graphically, using a restricted cubic spline to visually compare the mortality rates of the two patterns continuously across the entire range of MVPA values. Hazard ratios were further adjusted for age, accelerometer wear time, gender, race, smoking status, alcohol use, and healthy eating index.
Interactions by age, gender, and body mass index were tested. Three sets of sensitivity analyses were conducted: 1) additionally adjusting for body mass index, diabetes, and physical function; 2) using a more restrictive “weekend warrior” threshold of 67% (i.e., two-thirds) of weekly MVPA on only one or two days; and 3) applying a more liberal MVPA intensity threshold of 760 counts per minute or 1041 counts per minute, as suggested by some studies.(22, 23)
We also aimed to investigate the associations of bout characteristics (frequency, average duration, maximum duration) on mortality rate. To examine these associations, we calculated adjusted hazard ratios (95% confidence intervals) of an increase in one bout or 10-minutes in bout duration using Cox survival analyses. We additionally adjusted for total MVPA to examine bout characteristics independent of MVPA volume, as well as reported the Pearson correlation of the characteristics with total MVPA. Analyses were conducted using R software (version 3.4.3) and adjusted for NHANES survey design using sampling weights (MEC weights adjusted for a minimum valid wear time of six days).
RESULTS
On average, participants were 57.1 (standard error (SE) = 0.4) years old and wore the accelerometer for 6140 (SE = 26) minutes or approximately 14.6 hours per day. Examining participants based on physical activity profile, 36.6% were inactive, accruing < 37.5 minutes per week of MVPA; 32.3% were “weekend warriors”, performing ≥ 50% of their weekly activity in only one or two days; and 31.1% were “regularly active”, spreading their activity more evenly across the week. Compared to both the regularly active and weekend warrior participants, inactive participants tended to be older, female, less educated, less likely to use alcohol, more likely to have diabetes, and more likely to have difficulty walking or climbing steps (Table 1). Weekend warriors and regularly active participants appeared to be fairly similar in terms of most participant characteristics, except that regularly active participants engaged in ~ 50% more MVPA than weekend warriors.
Table 1.
Participant Characteristics by Moderate-to-Vigorous Physical Activity Profile, NHANES 2003–2006.
| Moderate-to-Vigorous Physical Activity Profilea | |||
|---|---|---|---|
| Inactive | Regularly Active | Weekend Warrior | |
| n | 1260 | 1068 | 1110 |
| Age (years) | 67.4 (0.8) | 52.3 (0.4) | 54.5 (0.4) |
| Female | 67.9 (1.3) | 44.2 (1.9) | 51.3 (2.1) |
| Race | |||
| Black | 11.1 (1.6) | 10.5 (1.6) | 9.8 (1.5) |
| Hispanic | 4.6 (1.1) | 8.0 (1.2) | 8.5 (1.3) |
| White | 80.4 (2.4) | 77.1 (2.7) | 77.2 (2.2) |
| Education | |||
| Less than High School | 24.6 (1.9) | 11.6 (1.3) | 13.4 (1.3) |
| High School | 31.6 (1.6) | 22.6 (1.4) | 24.9 (2.3) |
| More than High School | 43.8 (2.5) | 65.8 (1.5) | 61.7 (2.4) |
| Current Smoker | 18.2 (2.4) | 16.7 (1.2) | 18.3 (1.2) |
| Current Alcohol Use | 57.3 (1.9) | 78.6 (2.2) | 70.7 (2.5) |
| Healthy Eating Index | 50.0 (0.7) | 49.4 (0.5) | 50.1 (0.7) |
| Body Mass Index (kg/m2) | 29.2 (0.3) | 28.0 (0.2) | 28.3 (0.3) |
| Diabetes | 18.4 (1.3) | 6.0 (0.9) | 8.0 (1.2) |
| Any Difficulty Walking or Climbing Steps | 26.8 (1.4) | 5.1 (0.8) | 7.8 (1.2) |
| Wear time (min/week) | 6040 (42) | 6220 (41) | 6130 (43) |
| Moderate-to-Vigorous Physical Activity (min/week)b | 17 (0.4) | 227 (7) | 151 (4) |
| Number of Activity Bouts Per Weekc | 0.03 (0.01) | 3.1 (0.2) | 2.4 (0.1) |
Moderate-to-vigorous physical activity (MVPA) profile was determined by minutes per week of total weekly MVPA. Inactive participants participated in <37.5 minutes per week of MVPA. Participants with >=37.5 minutes per week of MVPA who performed >=50% of weekly MVPA in only 1 or 2 days were classified as weekend warriors, and others as regularly active.
MVPA was defined as >= 1952 counts per minute.
Activity bouts were defined as periods of at least 10 minutes with >=1952 cpm.
Values are mean (SE) or percent (SE), unless otherwise noted.
All characteristic statistics are calculated adjusted for the survey design.
Between 2003 and 2013 (average follow-up = 77.4 months), there were 394 deaths among the initial analytical sample of 3438 participants. We observed an inverse dose response of time spent in MVPA and mortality rate for both regularly active and weekend warrior participants (Figure 1). The confidence intervals for the regularly active and weekend warrior participants were substantially overlapping across the range of MVPA. Compared to inactive participants, both insufficiently active and sufficiently active weekend warriors and regularly active participants experienced a 60–69% reduction in mortality rate after adjusting for age, gender, race, education, smoking status, alcohol consumption, and healthy eating index (Table 2). Weekend warriors, those performing a majority of their MVPA on one or two days only, had similar mortality rate reduction as regularly active participants when compared to inactive participants (Table 2). This was observed both among those meeting the guidelines of at least 150 minutes per week of MVPA(6) (hazard ratio (95% confidence interval) weekend warriors: 0.31 (0.17, 0.51) vs regularly active: (0.40 (0.26, 0.63)) and those with some but insufficient amounts of MVPA (weekend warriors: 0.33 (0.23, 0.46) vs regularly active (0.32 (0.19, 0.53)).
Figure 1.
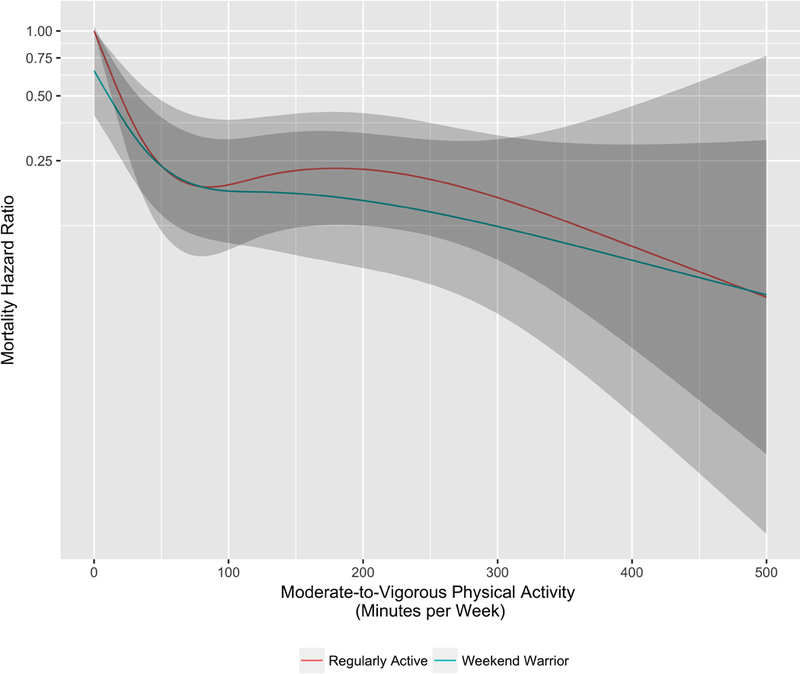
Comparing mortality rates between “weekend warriors” and “regularly active” participants by minutes per week of moderate-to-vigorous intensity physical activity, NHANES 2003–2006.
Table 2.
Hazard Ratios (95% Confidence Intervals) of Mortality by Moderate-to-Vigorous Physical Activity Profile, NHANES 2003–2006.
| Moderate-to-Vigorous Physical Activity (minutes per week) | |||
|---|---|---|---|
| <37.5 | 37.5 to <150 | >=150 | |
| Regularly Active | |||
| N Deaths (Person-Months) | 295 (88 980) | 18 (33 697) | 27 (53 100) |
| Hazard Ratio (95% CI) | Reference | 0.32 (0.19, 0.53) | 0.40 (0.26, 0.63) |
| Weekend Warriors | |||
| N Deaths | 40 (60 270) | 14 (30 110) | |
| Hazard Ratio (95% CI) | 0.33 (0.23, 0.46) | 0.31 (0.17, 0.57) | |
Moderate-to-vigorous physical activity (MVPA) profile was determined by minutes per week of total weekly MVPA. Participants with >=37.5 minutes per week of MVPA who performed >=50% of weekly MVPA in only 1 or 2 days were classified as weekend warriors. MVPA was defined as >= 1952 counts per minute. Hazard ratios (95% confidence intervals) are adjusted for age, accelerometer weartime, gender, race, education, smoking status, and healthy eating index.
We observed no statistically significant interactions by age, gender, or body mass index (p > 0.10). We conducted sensitivity analyses, adjusting for additional variables, examining different definitions of ‘weekend warrior’ and using more lenient MVPA accelerometer thresholds. Further adjustment for body mass index, diabetes, or physical functioning status did not substantially alter the association of physical activity profile on mortality. Similarly, increasing the amount of MVPA performed on one or two days from 50% to 67% of the weekly volume, or using the more lenient MVPA thresholds of 760 and 1041 instead of 1952 counts per minute, did not substantially change the similar reductions between weekend warriors and regularly active participants.
Next, we examined the association of mortality and characteristics of sustained MVPA bouts (at least 10 minutes), specifically the frequency of bouts, average bout duration, and maximum bout. When examining the association of an additional MVPA bout per week, we observed an increased mortality rate of 13% (1.13 (1.04, 1.23)), meaning fewer bouts had a lower mortality rate. Both average and maximum bout duration were not statistically significant predictors of mortality after adjusting for total MVPA (Table 3). Bout frequency, average bout duration, and maximum bout duration were moderately to highly correlated with total MVPA (rho = 0.81, 0.58, and 0.70, respectively, Table 3). The mortality hazard ratios associated with an increase in bout frequency or 10-minutes in bout duration did not differ substantially when the analyses were restricted to those with at least one bout, removing those with no bouts.
Table 3.
Hazard ratio (95% confidence intervals) of mortality by moderate-to-vigorous physical activity bout characteristics, NHANES 2003–2006
| Number of MVPA Bouts Per Weeka | Average MVPA Bout Durationa (minutes) | Maximum MVPA Bout Durationa (minutes) | |
|---|---|---|---|
| Among All Participants | |||
| Per Bout or 10-Minute Increase | |||
| Hazard Ratio (95% CI)b | 0.92 (0.88, 0.98) | 0.74 (0.64, 0.85) | 0.79 (0.71, 0.88) |
| Additionally Adjusted for Total MVPA | 1.13 (1.04, 1.23) | 0.94 (0.79, 1.12) | 0.96 (0.83, 1.10) |
| Correlation with Total MVPA | 0.81 | 0.58 | 0.70 |
| Among Participants with 1+ Bout | |||
| Per Bout or 10-Minute Increase | |||
| Hazard Ratio (95% CI)b | 1.00 (0.94, 1.06) | 0.85 (0.65, 1.10) | 0.85 (0.71, 1.01) |
| Additionally Adjusted for Total MVPA | 1.12 (1.02, 1.24) | 0.92 (0.70, 1.21) | 0.91 (0.74, 1.11) |
| Correlation with Total MVPA | 0.77 | 0.22 | 0.52 |
MVPA was defined as >= 1952 counts per minute.
Bouts were defined as 10+ consecutive minutes of counts >= 1952, with up to 2 minutes below that threshold.
Hazard ratios (95% confidence intervals) are adjusted for age, accelerometer wear time, gender, race, education, smoking status, alcohol use, and healthy eating index.
DISCUSSION
The few studies that have examined physical activity bout patterns in relation to health outcomes have primarily relied on self-reported activity with limited information on the bout length, duration, or frequency. The present study used accelerometers to objectively assess moderate-to-vigorous physical activity patterns and the association of those patterns with all-cause mortality. We examined the ‘weekend warrior’, finding that those participants who performed a majority of their MVPA on only one or two days, had similar mortality rate reduction as those who spread out their activity over more days during the week. Interestingly, this similar benefit between weekend warriors and regularly active participants was observed across a wide range of total activity volumes, not just among those who meeting the U.S. Federal physical activity guideline recommendations.(6)
Confirming previous studies(1, 24, 25), we observed an inverse dose-response of greater amount of MVPA and reduced mortality rates. Significant mortality rate reductions were observed with as little as 37.5 minutes of MVPA (or 25% of the U.S. Federal guideline recommendations(6)). Previous studies examining the weekend warrior have also found that weekend warriors experience mortality rate reductions similar to those who exercise more regularly.(10–12) However, these studies generally compare weekend warriors and regularly active participants only among those meet the recommendation of at least 150 minutes per week of MVPA. In our data using a wider range of activity levels, we observe that nearly one-third of participants actually engaged in a weekend warrior pattern. Restricting to higher activity levels only, previous studies reported approximately 4–5% of the population being classified as weekend warriors. For example, using latent class analysis, Evenson et al, identified participants who were most active on weekends.(15) This does not mean a lack of comparability between previous and the current study, however, as if we restrict to only those with high activity levels or only weekends (instead of any one or two days during the week), we also classified a similar proportion of participants weekend warriors (~3.5%).
A recent study by O’Donovan et al observed that even among those with lower levels of activity, those with only one or two sessions of activity maintained significant benefits.(11) Our spline analysis furthers this discussion showing similar hazard ratio curves for weekend warriors and regularly active participants over the entire range of activity volume. These data support the weekend warrior activity pattern for increased health benefits even at lower total activity levels. While previous literature has suggested weekend warriors may be more susceptible to injury(13), we observed very few deaths due to injury (<1%), but were unable to assess non-fatal injuries in these data.
Accelerometers provide an opportunity to examine physical activity patterns that are not limited to the number of days per week spent being active, but also the frequency and duration of individual sessions of activity. There are limited data examining activity patterns and long-term health outcomes. Parsons et al(26, 27), in a cross-sectional study of older men using accelerometers to describe activity patterns, reported that physical activity and sedentary bout duration was not associated with subclinical vascular disease. Evenson et al, using latent class analysis, show that mortality benefits were largely independent of the percent of MVPA bouts per day.(15) In addition, a recent study by Saint-Maurice et al, observed similar mortality benefits independent of the proportion of total MVPA that was accrued in bouts, using a lower threshold for MVPA.(16) In the present study, we observed that bout frequency but not bout duration was associated with a mortality rate.
An additional MVPA bout per week was associated with an increased mortality rate of 13%, indicating a potential preference for longer, fewer bouts. However, increased bout duration was not statistically significant. This may be the result of multicollinearity (moderate to high correlations with total MVPA were observed) or insufficient power to detect a difference by bout duration. One hypothesis to support longer, fewer bouts may be that the initial time during a bout may be at a lower intensity than the remainder of the bout, such as a ‘warm-up’, and thus a longer bout may have more time at the higher intensity. In the present study, we did not observe a threshold effect for the bout frequency or bout duration, but was most likely insufficiently powered to examine this. Further research is needed to fully examine the optimum bout duration and frequency.
This study has several strengths. This study used accelerometers to objectively assess MVPA, removing potential biases from self-reported assessment, as well as allowing for the detailed examination of activity accrual patterns over time. Participants were drawn from the National Health and Nutritional Examination Survey (NHANES), a U.S. population-based survey with 99% complete mortality follow-up, increasing the generalizability of the findings. NHANES has an extensive amount of participant information, both from questionnaires and an in-person clinical assessment, allowing for statistical adjustment of relevant covariables to limit residual confounding. Sensitivity analyses further accounting for body mass index, functional status, and diabetes status did not change the associations. In order to limit the potential for reverse causation, participants who died within 24 months of the accelerometer-assessment were excluded from the analyses. Lastly, sensitivity analyses allowing for different definitions of accelerometer-assessed MVPA and weekend warrior categorization were conducted and did not change the observed conclusions.
However, our study also has several limitations. We only examined all-cause mortality and the findings may not be directly applicable to other outcomes such as cardiovascular disease, diabetes status, or musculoskeletal injury rates. In addition, there were few events in several of the bout analyses categories limiting the statistical power of the comparisons. Accelerometers detect movement and motion, not specific physical activity behaviors.(14) Thus is may be inappropriate to directly translate accelerometer-derived activity estimates to self-reported estimates. However, this paper we examine physical activity across a wide range of activity levels, including continuously. This provides interesting insight into the dose-response of movement and health, even if the absolute values of activity time are not directly translatable. Furthermore, we conducted sensitivity analyses at using several definitions of MVPA and weekend warrior in order to be able to generalize these relative comparisons independent of the MVPA threshold, a point of contention when translating accelerometer to self-reported estimates. Perhaps with the advance of machine learning and other statistical techniques, we will better be able to bridge motion and behavior estimates.(28–30) Accelerometers are limited in their ability to detect specific activities such as cycling and swimming, potentially underestimating weekly MVPA.
In conclusion, this study supports current physical activity guidelines that recommend physical activity for health, including reduced mortality risk. Weekend warriors experienced similar mortality rate reductions as participants who engaged in activity more frequently, when both groups had the same total amount of moderate-to-vigorous physical activity. Future research is needed to more fully examine the relative importance activity bout duration.
ACKNOWLEDGMENTS
The results of this study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation. The results of the present study do not constitute endorsement by ACSM.
FUNDING
This research is supported in part by the Intramural Research Program at the National Institute on Aging, National Institutes of Health (Harris, Schepps, Shiroma). MK was supported by the Overseas Research Fellowship of the Sasakawa Sports Foundation.
The results of this study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation. The results of the present study do not constitute endorsement by ACSM. This research is supported in part by the Intramural Research Program at the National Institute on Aging, National Institutes of Health (Harris, Schepps, Shiroma). MK was supported by the Overseas Research Fellowship of the Sasakawa Sports Foundation. The authors report no conflicts of interest.
Footnotes
CONFLICTS OF INTEREST
The authors report no conflicts of interest.
REFERENCES
- 1.Physical Activity Guidelines Committee. Physical Activity Guidelines Advisory Committee Report. [Internet]. Washington, DC: Department of Health and Human Services; Available from: http://health.gov/paguidelines/guidelines/report.aspx. [Google Scholar]
- 2.Katzmarzyk PT, Lee IM. Sedentary behaviour and life expectancy in the USA: a cause-deleted life table analysis. BMJ open. 2012;2(4). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lee IM, Shiroma EJ, Lobelo F et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380(9838):219–29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Arem H, Moore SC, Patel A et al. Leisure time physical activity and mortality: a detailed pooled analysis of the dose-response relationship. JAMA Intern Med. 2015;175(6):959–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Moore SC, Lee IM, Weiderpass E et al. Association of Leisure-Time Physical Activity With Risk of 26 Types of Cancer in 1.44 Million Adults. JAMA Intern Med. 2016;176(6):816–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.United States Department of Health and Human Services. 2008 Physical Activity Guidelines for Americans. [Internet]. Available from: http://www.health.gov/paguidelines/.
- 7.Pate RR, Pratt M, Blair SN et al. Physical activity and public health. A recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA. 1995;273(5):402–7. [DOI] [PubMed] [Google Scholar]
- 8.Haskell WL, Lee IM, Pate RR et al. Physical activity and public health: updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007;39(8):1423–34. [DOI] [PubMed] [Google Scholar]
- 9.Hamer M, Biddle SJH, Stamatakis E. Weekend warrior physical activity pattern and common mental disorder: a population wide study of 108,011 British adults. The international journal of behavioral nutrition and physical activity. 2017;14(1):96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Hamer M, O’Donovan G, Lee IM, Stamatakis E. The ‘weekend warrior’ physical activity pattern: how little is enough? Br. J. Sports Med. 2017;51(19):1384–5. [DOI] [PubMed] [Google Scholar]
- 11.O’Donovan G, Lee IM, Hamer M, Stamatakis E. Association of “Weekend Warrior” and Other Leisure Time Physical Activity Patterns With Risks for All-Cause, Cardiovascular Disease, and Cancer Mortality. JAMA Intern Med. 2017;177(3):335–42. [DOI] [PubMed] [Google Scholar]
- 12.Lee IM, Sesso HD, Oguma Y, Paffenbarger RS Jr. The “weekend warrior” and risk of mortality. Am. J. Epidemiol. 2004;160(7):636–41. [DOI] [PubMed] [Google Scholar]
- 13.Roberts DJ, Ouellet JF, McBeth PB, Kirkpatrick AW, Dixon E, Ball CG. The “weekend warrior”: fact or fiction for major trauma? Can. J. Surg. 2014;57(3):E62–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Troiano RP, McClain JJ, Brychta RJ, Chen KY. Evolution of accelerometer methods for physical activity research. Br. J. Sports Med. 2014;48(13):1019–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Evenson KR, Herring AH, Wen F. Accelerometry-Assessed Latent Class Patterns of Physical Activity and Sedentary Behavior With Mortality. Am. J. Prev. Med. 2017;52(2):135–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Saint-Maurice PF, Troiano RP, Matthews CE, Kraus WE. Moderate-to-Vigorous Physical Activity and All-Cause Mortality: Do Bouts Matter? J Am Heart Assoc. 2018;7(6). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.United States Center for Disease Control. National Health and Nutrition Examination Survey. [Internet]. Available from: https://www.cdc.gov/nchs/nhanes/.
- 18.Troiano RP, Berrigan D, Dodd KW, Masse LC, Tilert T, McDowell M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 2008;40(1):181–8. [DOI] [PubMed] [Google Scholar]
- 19.Choi L, Liu Z, Matthews CE, Buchowski MS. Validation of accelerometer wear and nonwear time classification algorithm. Med. Sci. Sports Exerc. 2011;43(2):357–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Freedson PS, Melanson E, Sirard J. Calibration of the Computer Science and Applications, Inc. accelerometer. Med. Sci. Sports Exerc 1998;30(5):777–81. [DOI] [PubMed] [Google Scholar]
- 21.United States Center for Disease Control. National Center for Health Statistics NDI Mortality Data. [Internet]. Available from: https://www.cdc.gov/nchs/data-linkage/mortality.htm.
- 22.Matthew CE. Calibration of accelerometer output for adults. Med. Sci. Sports Exerc. 2005;37(11 Suppl):S512–22. [DOI] [PubMed] [Google Scholar]
- 23.Copeland JL, Esliger DW. Accelerometer assessment of physical activity in active, healthy older adults. J Aging Phys Act. 2009;17(1):17–30. [DOI] [PubMed] [Google Scholar]
- 24.Lollgen H, Bockenhoff A, Knapp G. Physical activity and all-cause mortality: an updated meta-analysis with different intensity categories. Int. J. Sports Med. 2009;30(3):213–24. [DOI] [PubMed] [Google Scholar]
- 25.Evenson KR, Wen F, Herring AH. Associations of Accelerometry-Assessed and Self-Reported Physical Activity and Sedentary Behavior With All-Cause and Cardiovascular Mortality Among US Adults. Am. J. Epidemiol. 2016;184(9):621–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Parsons TJ, Sartini C, Ellins EA et al. Objectively measured physical activity, sedentary time and subclinical vascular disease: Cross-sectional study in older British men. Prev. Med. 2016;89:194–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Parsons TJ, Sartini C, Ellins EA et al. Objectively measured physical activity and sedentary behaviour and ankle brachial index: Cross-sectional and longitudinal associations in older men. Atherosclerosis. 2016;247:28–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Bassett DR, Troiano RP, McClain JJ, Wolff DL. Accelerometer-based physical activity: total volume per day and standardized measures. Med. Sci. Sports Exerc. 2015;47(4):833–8. [DOI] [PubMed] [Google Scholar]
- 29.Lyden K, Keadle SK, Staudenmayer J, Freedson PS. A method to estimate free-living active and sedentary behavior from an accelerometer. Med. Sci. Sports Exerc 2014;46(2):386–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Freedson PS, Lyden K, Kozey-Keadle S, Staudenmayer J. Evaluation of artificial neural network algorithms for predicting METs and activity type from accelerometer data: validation on an independent sample. J Appl Physiol (1985). 2011;111(6):1804–12. [DOI] [PMC free article] [PubMed] [Google Scholar]