

Abstract
INTRODUCTION:
This study examined sexual orientation differences in eating behaviors, physical activity, and weight status among adolescents in the United States. Moreover, this study tested whether parental and peer influences contribute to sexual orientation disparities in adolescent eating behaviors, physical activity, Body Mass Index (BMI), and examined disparities in weight misperception.
METHODS:
Cross-sectional data were from 1926 adolescents who participated in the NEXT Generation Health Study in 2010/2011. Linear and multinomial logistic regressions conducted in 2017/2018 were used to test disparities and interactions with social influences.
RESULTS:
Relative to their heterosexual peers, sexual minority males and females consumed fruits and vegetables more frequently; sexual minority males engaged in less frequent physical activity; and sexual minority females were more likely to be overweight, perceive themselves as overweight, and to overestimate their weight. High parental expectation for physical activity was associated with more frequent vigorous physical activity among heterosexual adolescents, but less frequent vigorous physical activity among sexual minority males. Exercising with a same-sex peer buffered against the risk of higher BMI among sexual minority females.
CONCLUSIONS:
Parental and peer influences may serve as potential intervention targets to reduce disparities in weight-related behaviors. Longitudinal research is needed to understand the consequences of weight misperception among sexual minority females.
Keywords: LGBQ, health disparities, adolescence, social influences, physical health
Adolescents who consume more unhealthy food and engage in less physical activity are at risk for developing obesity and may experience downstream health problems such as cardiovascular diseases.1,2 While sexual minority adolescents experience more disordered eating behaviors, empirical evidence on sexual orientation disparities in eating behaviors, physical activity, and weight-related constructs is relatively limited.3 Moreover, despite the importance of parental and peer influences on healthy development among sexual minority adolescents,4 these factors have not been tested as moderators of sexual orientation disparities in physical health, which is needed to inform prevention and translational research.5 The present study examined parental and peer influences on sexual orientation disparities in eating behaviors, physical activity, and BMI in a nationally representative sample of male and female adolescents. This study further investigated whether sexual minority adolescents experienced disparities in weight misperception by comparing adolescents’ weight status to their weight perception.
Understanding eating habits during adolescence is critical as these habits may persist into adulthood and are linked to changes in BMI.6 Past studies on sexual orientation disparities in various eating behaviors have yielded mixed findings.3 Among adolescents in the Growing Up Today Study (GUTS), sexual minority females had higher rates of fast food consumption than heterosexual females, whereas sexual minority males had lower rates of fast food consumption than heterosexual males.7 Findings from the 2005 and 2007 Youth Risk Behavior Surveys (YRBS) indicated that male and female sexual minority adolescents consumed more fruits and vegetables relative to heterosexual peers,8 but this finding was not replicated in a female college student sample.9 Among college students in Minnesota, gay males consumed less sugar- sweetened soda but more artificially-sweetened soda than heterosexual males, and soda consumption did not differ between sexual minority and heterosexual females.10 Thus, additional research using more recent samples is warranted to clarify these mixed findings and examine a broader range of eating behaviors.
Consistent across various measures of physical activity, sexual orientation disparities were more consistently observed among male adolescents.3 Relative to heterosexual males, sexual minority males in the YRBS engaged in less frequent physical activity in the past seven days.8 Analyses of the GUTS dataset indicated increased risk of physical inactivity among sexual minority adolescents;11 in particular, sexual minority males engaged in 2 hours fewer per week of moderate-to-vigorous physical activity than their heterosexual peers.12 Sexual minority males in the Dane County Youth Assessment were less physically active and participated less in team sports.13 These lower rates have been attributed to greater gender nonconformity and lower athletic self-esteem,12 which could reduce participation in sports due to perceived or actual social rejection.14
Parents and peers play an important role in shaping health-related behaviors during the adolescent period.15,16 Their support of healthful nutrition and physical activity promotes a healthier diet and physical activity among adolescents in the general population.17–19 During adolescence, same-sex peers tend to influence diet and physical activity more strongly than opposite-sex peers.20,21 Whether this holds for sexual minority adolescents is unclear. Sexual minority adolescents more frequently encounter barriers to participate in physical activities;14,22,23 thus, parental expectations to engage in physical activities may be perceived more as a source of stress than of support. An improved understanding of whether parental and peer influences mitigate the association between sexual minority status and weight-related outcomes is needed to inform prevention and intervention efforts.
Adolescents who perceive themselves as overweight despite having a normal BMI are more likely to develop obesity in young adulthood.24 It is largely unknown whether weight misperception is more common among sexual minority adolescents than heterosexual females, although BMI is higher among certain sexual minority subgroups and particularly among sexual minority females.7,8,10,25,26 Hadland et al. reported that sexual minority females were more likely than heterosexual females to report healthy/underweight perception despite having overweight status, whereas sexual minority males were more likely than heterosexual males to report overweight perception despite having healthy/underweight statuses.27 Weight perception may, therefore, be an important construct in furthering the understanding of sexual orientation disparities in weight-related behaviors.
This study has three goals. First, sexual orientation differences in eating behaviors, physical activity, and weight status were examined in a recent sample of U.S. adolescents. Second, this study investigated whether the presence of parents and peers who encourage healthful eating behaviors and physical activity would moderate the associations of sexual minority status with eating behaviors, physical activity, and BMI. Third, sexual minority adolescents experienced disparities in weight misperception were also tested.
Method
Participants
Data came from the NEXT Generation Health Study (NEXT), a nationally representative longitudinal study of 2785 adolescents who were enrolled in 10th grade in 2009/2010. A 3-stage stratified design was used to recruit a diverse sample of adolescents. Study participants came from U.S. high schools in 22 states and were followed for 7 years. Sexual orientation was measured at Wave 2 of this study; accordingly, we utilized cross-sectional data from Wave 2 participants (n = 2439; 87.6% of the full sample). The current analytic sample consisted of 1926 adolescents (79.0% of Wave 2 NEXT sample; mean age = 17.2, SD = 0.51) who provided valid responses to all study variables. Parents provided written consent and participants provided assent to participate in this study; upon turning 18 years of age, participants provided consent. The study was approved by the Institutional Review Board of the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Measures
Sexual Orientation.
A survey item on sexual attraction was used as an indicator of sexual orientation because sexual attraction is typically more relevant and easier to describe than sexual identity or behavior during the adolescent period.28,29 Participants were asked which of the following best described their sexual orientation: (1) “Attracted to opposite gender”; (2) “Attracted to same gender”; (3) “Attracted to both genders”; and (4) “Questioning.” Due to their low frequencies (see Table 1), the last three categories were collapsed for analyses.
Table 1.
Sample characteristics for the Wave 2 NEXT sample and the analytic sample
| Wave 2 NEXT sample (n = 2439) | Analytic sample (n = 1926) | |||||||
|---|---|---|---|---|---|---|---|---|
| Overall | Overall | Males (n = 811) | Females (n = 1115) | |||||
| Frequency | Percent | Frequency | Percent | Frequency | Percent | Frequency | Percent | |
| Sex | ||||||||
| Male | 1076 | 44.9% | 811 | 44.0% | -- | -- | -- | -- |
| Female | 1363 | 55.1% | 1115 | 56.0% | -- | -- | -- | -- |
| Race/Ethnicity | ||||||||
| Non-Hispanic White | 986 | 58.6% | 867 | 62.0% | 381 | 64.0% | 468 | 60.0% |
| Non-Hispanic African Americans | 611 | 17.5% | 443 | 16.0% | 153 | 12.0% | 290 | 19.0% |
| Hispanic | 715 | 19.6% | 517 | 18.0% | 238 | 18.0% | 279 | 18.0% |
| Other | 120 | 4.3% | 99 | 4.2% | 39 | 5.6% | 60 | 3.2% |
| Family affluence | ||||||||
| Low | 775 | 23.1% | 570 | 23.0% | 227 | 21.0% | 343 | 24.0% |
| Medium | 1148 | 49.8% | 922 | 50.0% | 398 | 54.0% | 524 | 57.0% |
| High | 516 | 27.1% | 434 | 27.0% | 186 | 25.0% | 248 | 28.0% |
| Sexual orientation | ||||||||
| Attracted to opposite gender | 2196 | 93.7% | 1772 | 94.0% | 776 | 97.0% | 996 | 92.4% |
| Attracted to same gender | 45 | 1.2% | 34 | 1.2% | 15 | 1.1% | 19 | 1.2% |
| Attracted to both genders | 119 | 3.7% | 94 | 3.3% | 13 | 0.8% | 81 | 5.3% |
| Questioning | 42 | 1.4% | 26 | 1.1% | 7 | 1.2% | 19 | 1.1% |
Unweighted frequencies and weighted percentages are presented.
Eating Behaviors.
Food group intake frequencies in the past 7 days were assessed using 8 items,30 covering intake of sugar-sweetened soda or pop (1 item), sweet or salty snacks (1 item), fruits/vegetables (5 items; fruit, fruit juice, green vegetables, orange vegetables, and beans), and whole grains (1 item). Participants were asked to report intake frequencies on a scale from 0 = “Never” to 3 = “1 time per day” to 6 = “4 or more times per day.” The variable was recoded to represent the number of times/day of each food group. A sum score was used to indicate frequencies of fruits/vegetables intake.
Physical Activity.
Two items, previously validated using accelerometer data, were taken from the YRBS questionnaire.31,32 Frequency of at least 60 minutes of physical activity (including sports, school activities, playing with friends, or walking to work or school) per day in the past 7 days was assessed (response options 0 to 7 days). Frequency of vigorous physical activity (any activity that increases heart rate and makes the participant get out of breath or sweat) in a typical week was also assessed (response options 0 = “none” to 5 = “7 hours or more”).
BMI-z.
Participants reported their weight without clothes in pounds and height without shoes in feet and inches, which were used to calculate BMI. To aid meaningful comparisons among adolescents, BMI z-scores were computed based on the CDC growth charts to adjust for age and sex differences.33
Weight Status.
BMI groups were classified based on the American Academy of Pediatrics weight guidelines according to age- and sex-specific CDC percentiles:34 underweight (<5th percentile adjusted for age and sex), normal weight (5th percentile ≤ BMI < 85th percentile), overweight (85th percentile ≤ BMI < 95th percentile), and obese (≥ 95th percentile). We coded weight status as a three-category variable: 0 = “underweight,” 1 = “normal weight,” and 2 = “overweight/obese.”
Weight Perception.
Participants were asked to rate whether they felt they were “very underweight,” “somewhat underweight,” “about the right weight,” “somewhat overweight,” or “very overweight.” We coded weight perception in a way that parallels the categorization of weight status: 0 = “feels underweight, 1 = “feels about right” and 2 = “feels overweight.”
Weight Misperception.
Three weight perception groups were created based on weight status and perception (see Supplementary Table 1). Participants whose weight perception was greater than their weight status were classified as over-estimators. Participants whose weight perception was lower than their weight status were classified as under-estimators. Participants whose weight perception was concurrent with their weight status were classified as concurrent-estimators.
Parental Expectations for Healthful Diet and Physical Activity.
Two items were adapted from prior studies examining parental influences on health-related behaviors.35,36 Participants were asked how important it is to their parents/guardians that they (1) “eat a healthful diet (including fruits & vegetables, and limiting junk food, sweets, & fatty foods)?” and (2) “get daily physical activity and/or exercise?” with response options ranging from 1 = “not at all” to 4 = “somewhat” to 7 = “Extremely.”
Same-Sex Peer Meal Consumption and Physical Activity.
Participants were asked whether (yes/no) they recently engaged in different types of activities with their same-sex best friend. Given the interest in eating behaviors and physical activity, two items were used to assess whether participants (1) “ate a meal with him/her in the last seven days,” and (2) “exercised or played sports with him/her in the last seven days.”
Covariates.
Age, race/ethnicity, and family affluence were included as covariates. Race/ethnicity was categorized into 4 groups (Non-Hispanic White, African American, Hispanic and other). Family affluence was measured using the Family Affluence Scale.37 Sample items include participants’ family car and computer ownership, and family holidays.
Analyses
Linear multiple regressions were used to examine sexual orientation differences in eating behaviors, physical activity, and BMI-z. Multinomial logistic regressions were used to examine sexual orientation differences in weight status, weight perception, and weight misperception, where Relative Risk Ratios (RRR) were obtained by exponentiating the regression coefficients. To test the moderation hypotheses, four continuous variables (social influences) by binary variable (sexual orientation) interaction terms were created. For eating behaviors, parental expectation for healthful diet and same-sex peer meal consumption were tested as moderators. For physical activity, parental expectation for physical activity and same-sex peer physical activity were tested as moderators. For BMI, all four moderators were tested. Significant interactions were probed using simple slope analyses.38 Statistical analyses were conducted separately for males and females. All analyses were conducted in 2017/2018 using STATA 14, accounting for clustering, weighting, and stratification of NEXT study design.
Results
Sample characteristics for the Wave 2 NEXT sample and the analytic sample were largely similar and are presented in Table 1. Descriptive statistics and results from the multiple regression analyses are presented in Table 2. In terms of eating behaviors, sexual minority males ate fruits and vegetables more frequently than their heterosexual peers (1.7 additional times per week) with similar intake of snacks, sodas, and whole grains. In terms of physical activity, sexual minority males engaged in one fewer day per week of 60 minutes of physical activity and 1.3 units fewer vigorous physical activity in a typical week relative to heterosexuals. Sexual minority males did not report higher BMI-z scores or higher odds of weight misperception than heterosexual males.
Table 2.
Results from linear and multinomial logistic regression models
| Male (n = 811) | Female (n = 1115) | |||||
|---|---|---|---|---|---|---|
| Heterosexual | Sexual Minority | Heterosexual | Sexual Minority | |||
| Mean (SE) | Mean (SE) | b (95% CI) | Mean (SE) | Mean (SE) | b (95% CI) | |
| Eating Behaviors (times/day) | ||||||
| Snack | 1.24 (0.19) | 1.39 (0.23) | 0.15 (−0.33, 0.63) | 1.16 (0.09) | 1.25 (0.17) | 0.09 (−0.25, 0.44) |
| Soda | 1.00 (0.20) | 0.80 (0.30) | −0.20 (−0.81, 0.41) | 1.20 (0.22) | 1.14 (0.21) | −0.06 (−0.49, 0.38) |
| Fruits and vegetables | 3.10 (0.22) | 4.83 (0.63) | 1.73 (0.43, 3.03) | 3.02 (0.25) | 3.84 (0.38) | 0.82 (0.03, 1.60) |
| Whole grains | 1.18 (0.12) | 1.75 (0.45) | 0.57 (−0.38, 1.51) | 1.22 (0.11) | 1.59 (0.21) | 0.38 (−0.06, 0.82) |
| Physical Activity | ||||||
| Days with 60 mins PA | 5.08 (0.20) | 3.97 (0.49) | −1.11 (−2.13, −0.08) | 3.32 (0.18) | 2.88 (0.39) | −0.44 (−1.26, 0.37) |
| Number of hours/week | 4.30 (0.18) | 2.97 (0.52) | −1.33 (−2.41, −0.26) | 3.42 (0.14) | 3.08 (0.30) | −0.34 (−0.96, 0.28) |
| BMI-z | 0.64 (0.17) | 0.68 (0.55) | 0.04 (−1.11, 1.19) | 0.26 (0.11) | 0.52 (0.16) | 0.26 (−0.06, 0.59) |
| Frequency (%) | Frequency (%) | RRR (95% CI) | Frequency (%) | Frequency (%) | RRR (95% CI) | |
| Weight Status | ||||||
| Underweight | 30 (3.48) | 2 (3.22) | 0.65 (0.05, 7.74) | 20 (1.80) | 4 (4.84) | 4.66 (0.97, 22.45) |
| Normal (ref) | 500 (66.05) | 25 (63.27) | -- | 696 (72.26) | 58 (45.79) | -- |
| Overweight | 246 (30.47) | 8 (33.51) | 1.08 (0.19, 6.09) | 280 (25.94) | 57 (49.79) | 2.62 (1.14, 6.02) |
| Weight Perception | ||||||
| Underweight | 113 (12.88) | 8 (28.28) | 2.32 (0.40, 13.59) | 74 (7.20) | 9 (6.40) | 1.64 (0.65, 4.14) |
| Normal (ref) | 466 (60.45) | 14 (33.97) | -- | 510 (55.56) | 39 (27.54) | -- |
| Overweight | 197 (26.67) | 13 (37.75) | 2.59 (0.55, 12.13) | 412 (37.24) | 71 (66.07) | 3.53 (1.87, 6.66) |
| Weight Misperception | ||||||
| Underestimate | 187 (20.85) | 7 (26.67) | 0.88 (0.14, 5.66) | 91 (10.15) | 15 (14.86) | 1.76 (0.71, 4.38) |
| Accurate estimate (ref) | 526 (70.79) | 22 (67.48) | -- | 724 (72.44) | 77 (52.06) | -- |
| Overestimate | 63 (8.35) | 6 (5.85) | 0.80 (0.18, 3.58) | 181 (17.41) | 27 (33.08) | 2.96 (1.12, 7.81) |
Analyses controlled for age, race/ethnicity and family affluence. Weighted means and standard errors are presented for eating behaviors, physical activity, and BMI-z scores. For weight status, perception, and misperception, unweighted frequencies are presented to indicate the number of participants for each weight category, whereas weighted percentages are presented to reflect nationally representative estimates. Additional information about model parameters can be found in Supplementary Table 2. After controlling for weight status, sexual minority status remained significantly associated with increased risk of weight overestimation among females (RRR = 5.76, 95% CI = 1.99–16.71). RRR = Relative Risk Ratio; CI = Confidence Intervals. p < 0.05 are in bold.
Among females, sexual minorities ate fruits and vegetables more frequently than their heterosexual peers (0.8 additional times per week). Sexual minority and heterosexual females consumed snacks, sodas and whole grains with similar frequency. No sexual orientation differences in physical activity or BMI-z scores were found among females. The odds of reporting overweight (RRR = 2.6), perceived overweight (RRR = 3.5), and weight overestimation (RRR = 3.0) were greater among sexual minority than heterosexual females.
Moderation analyses revealed two significant interactions. First, for heterosexual adolescents, higher parental expectation for physical activity was associated with more hours per week of vigorous physical activity (b = 0.14 among males, b = 0.21 among females). In contrast, for sexual minority adolescents, higher parental expectation for physical activity was associated with fewer hours per week of vigorous physical activity among males (b = −0.41) and no difference in frequency of vigorous physical activity among females (b = −0.15; Figure 1). Second, for females, sexual minorities who had not exercised with a same-sex best friend in the past week reported higher BMI-z scores compared to heterosexuals (b = 0.64; Figure 2). When female adolescents exercised with a same-sex peer, BMI-z scores did not differ across sexual orientation. This interaction was not significant among males.
Figure 1. Association between parental expectations of physical activity and vigorous physical activity for heterosexual and sexual minority males and females.
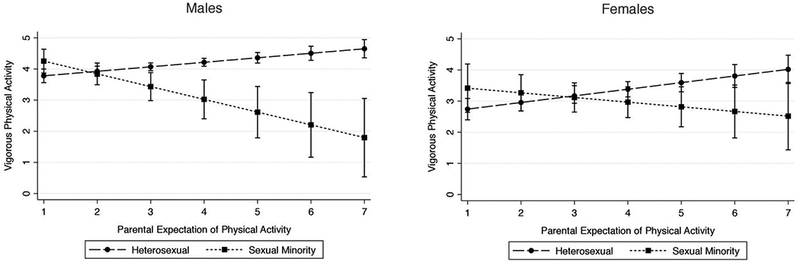
Footnote: Figures derived from multiple linear regression estimates controlling for age, race/ethnicity and family affluence. Vigorous physical activity measured in hours per week. Parental expectations measured in adolescents’ perceived degree of importance, ranging from 1 (“Not at All”) to 7 (“Extremely”). Error bars represent 95% confidence intervals.
Figure 2. Association between past week exercise with a same-sex peer and BMI-z score for heterosexual and sexual minority males and females.
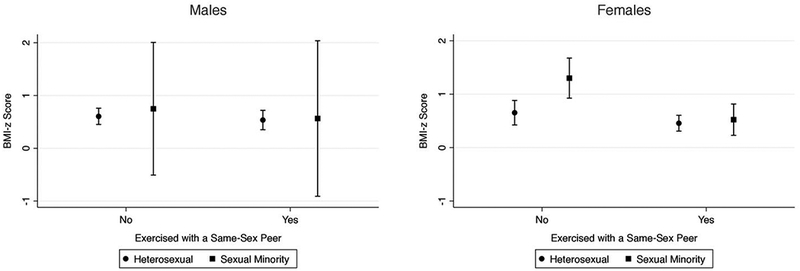
Footnote: Figures derived from multiple linear regression estimates controlling for age, race/ethnicity and family affluence. BMI-z scores reflect number of standard deviations from age-specific mean BMI. Error bars represent 95% confidence intervals.
Discussion
In this national study, sexual minority adolescents had similar snack, soda, and whole grains intake but greater fruits and vegetables consumption as compared to heterosexual adolescents, and sexual orientation differences in physical activity behaviors among males only. Weight perception and misperception were similar among sexual minority and heterosexual males, whereas overweight/obese weight status, perceived overweight/obese, and weight overestimation were both more prevalent among sexual minority than heterosexual females. Findings regarding sexual orientation disparities in weight status among females were consistent with prior research.8,10,25 However, no sexual orientation disparities were found in BMI-z score among both males and females, highlighting the importance of contrasting both overweight/obese and underweight against normal weight. Importantly, this study provides first evidence that parental expectations for physical activity and exercised with a same-sex peer may moderate sexual orientation disparities in adolescent physical activity and BMI.
Sexual minority females had greater odds of overweight and obesity based on self-reported height and weight, which is consistent with prior studies.3,25,27 Extending prior research on the role of physical activity-specific peer support in promoting adolescent physical activity,17,39 exercising with same-sex peers buffered against sexual orientation disparities in BMI among females. Compared to heterosexual adolescents, sexual minority adolescents do not only face common stressors related to adolescent development, but they also face unique stressors related to the development of their sexual identity and possible social rejection or victimization.40 Although information regarding the nature of the same-sex peer relationship (romantic vs. friendship) was not available in this study, exercising with a same-sex best friend could serve as an important source of peer support for sexual minority females to deal with general and minority specific stressors related to engagement in physical activity. More research is needed to understand whether this interaction effect is specific to same-sex romantic partner versus same-sex friend, which could further guide peer-based prevention efforts.
Consistent with prior studies, sexual orientation disparities for physical activity were found among males.8,12 Although parental expectation for physical activity tends to promote physical activity among adolescents,18 the results suggest that this expected pattern does not generalize to sexual minority adolescents, and may have the opposite, inverse association among sexual minority males. For sexual minority males, behaviors consistent with parental expectations in this domain may be particularly challenging as they are more likely to be socially alienated in sports participation and be victimized in the gym or athletic fields.14,22,23 Thus, sexual minority males may experience psychological distress by what their parents expect them to do and the fear of being excluded or victimized, leading to greater avoidance of vigorous physical activity.
This study explored sexual orientation differences in multiple adolescent eating behaviors, including whole grains consumption, which was not examined previously.3 The current findings replicated Rosario et al.8 in showing that sexual minority adolescents consumed more fruits and vegetables than heterosexual peers, and extended their findings by demonstrating no sexual orientation differences in snack, sugar-sweetened soda, or whole grain consumption. Prior studies suggest that adolescents are vulnerable to messages from mass media41 and that sexual minority men are more sensitive to mass media messages regarding societal beauty norms than heterosexual men.42 One possible explanation for higher frequency of eating fruits and vegetables may reflect sexual minority adolescents’ attempt to become leaner.43 This speculation should be explicitly tested in future studies with direct measurement of media influence and motivations for leanness.
Extending Hadland et al.,27 both underestimation and overestimation of weight status in relation to sexual minority status were examined. Analyses of weight perception revealed that sexual minority females had greater odds of perceiving themselves as overweight relative to their heterosexual peers. The analyses of weight misperception further suggested that weight overestimation (but not underestimation) was more common among sexual minority females relative to heterosexual females. To better understand why this may be the case, it would be important to examine whether sexual minority and heterosexual females may have different standards for ideal weight and body image. As weight misperception is a risk factor for obesity,24 more research is needed to understand how weight misperception contributes to disparities in dietary and weight-related behaviors among sexual minority adolescents.
This study has several limitations. First, the analyses were cross-sectional and observational, so causal conclusions cannot be drawn. Second, the measure of sexual orientation focused on sexual attraction only and did not account for sexual behavior or identity. Third, the analyses collapsed all sexual orientation subgroups (i.e. lesbian, gay, bisexual, and questioning) into a single “sexual minority” group. As such, possible subgroup differences11 were not tested. Third, multiple self-reported single-item measures such as for parental expectation of healthful diet and physical activity were used. Finally, there were relatively few sexual minority males in this sample. Analyses to detect sexual orientation differences among males may be underpowered. Future studies could utilize longitudinal data to determine temporality and assess multiple dimensions of sexual orientation. Experimental research is also needed to evaluate whether tailored interventions targeting adolescents’ social contexts may lead to improvements in dietary behaviors and physical activity.
The present study is the first to illustrate physical activity-related social influences as moderators of sexual orientation disparities in physical activities and BMI. Study findings support the potential benefit of encouraging same-sex peer support for sexual minority females to reduce disparities in BMI. Moreover, during late adolescence, encouragement of higher parental expectation on physical activity alone may not be sufficient to promote vigorous physical activities among sexual minorities. For sexual minority adolescents whose sports preference differs from parents’ preference, acceptance strategies may be particularly helpful and should be evaluated in future studies. To best inform prevention and intervention efforts, additional research is needed to identify barriers to and social influences that promote physical activities among sexual minority adolescents.
Supplementary Material
Acknowledgments
Funding source: This project (contract HHSN275201200001I) was supported in part by the Intramural Research Program of the Eunice Kennedy Shriver National Institute of Child Health and Human Development; the National Heart, Lung, and Blood Institute; the National Institute on Alcohol Abuse and Alcoholism; the National Institute on Drug Abuse; the Maternal and Child Health Bureau of the Health Resources and Services Administration; and the NIH Amgen Scholars program.
Footnotes
Conflict of interest statement: The authors have no conflict of interest relevant to this article to disclose.
Financial disclosure: The authors have no financial relationships relevant to this article to disclose.
References
- 1.Srinivasan SR, Bao W, Wattigney WA, Berenson GS. Adolescent overweight is associated with adult overweight and related multiple cardiovascular risk factors: the Bogalusa Heart Study. Metabolism. 1996;45(2):235–240. [DOI] [PubMed] [Google Scholar]
- 2.Kohl H 3rd Physical activity and cardiovascular disease: evidence for a dose response. Med Sci Sports Exerc. 2001;33(6 Suppl):S472–483. [DOI] [PubMed] [Google Scholar]
- 3.Miller JM, Luk JW. A systematic review of sexual orientation disparities in disordered eating and weight-related behaviors among adolescents and young adults: Toward a developmental model. Adolesc Res Rev. 2018:1–22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mustanski B, Birkett M, Greene GJ, Hatzenbuehler ML, Newcomb ME. Envisioning an America without sexual orientation inequities in adolescent health. Am J Public Health. 2014;104(2):218–225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mustanski B Future directions in research on sexual minority adolescent mental, behavioral, and sexual health. J Clin Child Psychol. 2015;44(1):204–219. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Neumark-Sztainer D, Wall M, Larson NI, Eisenberg ME, Loth K. Dieting and disordered eating behaviors from adolescence to young adulthood: Findings from a 10-Year longitudinal study. J Am Diet Assoc. 2011;111(7):1004–1011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Katz-Wise SL, Jun HJ, Corliss HL, Jackson B, Haines J, Austin SB. Child Abuse as a Predictor of gendered sexual orientation disparities in Body Mass Index trajectories among US youth from the Growing Up Today Study. J Adolesc Health. 2014;54(6):730–738. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Rosario M, Corliss HL, Everett BG, et al. Sexual orientation disparities in cancer-related risk behaviors of tobacco, alcohol, sexual behaviors, and diet and physical activity: Pooled Youth Risk Behavior Surveys. Am J Public Health. 2014;104(2):245–254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.McElroy JA, Jordan J. Disparate perceptions of weight between sexual minority and heterosexual female college students. LGBT health. 2014;1(2):122–130. [DOI] [PubMed] [Google Scholar]
- 10.Laska MN, VanKim NA, Erickson DJ, Lust K, Eisenberg ME, Rosser BR. Disparities in weight and weight behaviors by sexual orientation in college students. Am J Public Health. 2015;105(1):111–121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Rosario M, Li F, Wypij D, et al. Disparities by sexual orientation in frequent engagement in cancer-related risk behaviors: A 12-year follow-up. Am J Public Health. 2016;106(4):698–706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Calzo JP, Roberts AL, Corliss HL, Blood EA, Kroshus E, Austin SB. Physical activity disparities in heterosexual and sexual minority youth ages 12–22 years old: Roles of childhood gender nonconformity and athletic self-esteem. Ann Behav Med. 2014;47(1):17–27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Mereish EH, Poteat VP. Let’s get physical: sexual orientation disparities in physical activity, sports involvement, and obesity among a population-based sample of adolescents. Am J Public Health. 2015;105(9):1842–1848. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sartore ML, Cunningham GB. Gender, sexual prejudice and sport participation: Implications for sexual minorities. Sex Roles. 2009;60(1–2):100–113. [Google Scholar]
- 15.Ryan C, Huebner D, Diaz RM, Sanchez J. Family Rejection as a predictor of negative health outcomes in White and Latino lesbian, gay, and bisexual young adults. Pediatrics. 2009;123(1):346–352. [DOI] [PubMed] [Google Scholar]
- 16.Eisenberger NI, Taylor SE, Gable SL, Hilmert CJ, Lieberman MD. Neural pathways link social support to attenuated neuroendocrine stress responses. Neuroimage. 2007;35(4):1601–1612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hohepa M, Scragg R, Schofield G, Kolt GS, Schaaf D. Social support for youth physical activity: Importance of siblings, parents, friends and school support across a segmented school day. Int J Behav Nutr Phys Act. 2007;4:9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Golan M, Crow S. Parents are key players in the prevention and treatment of weight-related problems. Nutr Rev. 2004;62(1):39–50. [DOI] [PubMed] [Google Scholar]
- 19.Kulik NL, Fisher EB, Ward DS, Ennett ST, Bowling JM, Tate DF. Peer support enhanced social support in adolescent females during weight loss. Am J Health Behav. 2014;38(5):789–800. [DOI] [PubMed] [Google Scholar]
- 20.Davison KK, Birch LL. Childhood overweight: A contextual model and recommendations for future research. Obes Rev. 2001;2(3):159–171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Smith AL. Peer relationships in physical activity contexts: A road less traveled in youth sport and exercise psychology research. Psychol Sport Exerc. 2003;4(1):25–39. [Google Scholar]
- 22.Osborne D, Wagner WE. Exploring the relationship between homophobia and participation in core sports among high school students. Sociol Perspect. 2007;50(4):597–613. [Google Scholar]
- 23.Zipp JF. Sport and Sexuality: Athletic participation by sexual minority and sexual majority adolescents in the U.S. Sex Roles. 2011;64(1–2):19–31. [Google Scholar]
- 24.Sutin AR, Terracciano A. Body weight misperception in adolescence and incident obesity in young adulthood. Psychol Sci. 2015;26(4):507–511. [DOI] [PubMed] [Google Scholar]
- 25.Austin SB, Ziyadeh NJ, Corliss HL, et al. Sexual orientation disparities in weight status in adolescence: Findings from a prospective study. Obesity. 2009;17(9):1776–1782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Austin SB, Nelson LA, Birkett MA, Calzo JP, Everett B. Eating disorder symptoms and obesity at the intersections of gender, ethnicity, and sexual orientation in US high school students. Am J Public Health. 2013;103(2):e16–e22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hadland SE, Austin SB, Goodenow CS, Calzo JP. Weight misperception and unhealthy weight control behaviors among sexual minorities in the general adolescent population. J Adolesc Health. 2014;54(3):296–303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Friedman MS, Silvestre AJ, Gold MA, et al. Adolescents define sexual orientation and suggest ways to measure it. J Adolesc. 2004;27(3):303–317. [DOI] [PubMed] [Google Scholar]
- 29.Saewyc EM. Research on adolescent sexual orientation: Development, health disparities, stigma, and resilience. J Res Adolesc. 2011;21(1):256–272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Lipsky LM, Haynie DL, Liu DP, et al. Trajectories of eating behaviors in a nationally representative cohort of US adolescents during the transition to young adulthood. Int J Behav Nutr Phys Act. 2015;12:11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Prochaska JJ, Sallis JF, Long B. A physical activity screening measure for use with adolescents in primary care. Arch Pediatr Adolesc Med. 2001;155(5):554–559. [DOI] [PubMed] [Google Scholar]
- 32.Eaton DK, Kann L, Kinchen S, et al. Youth risk behavior surveillance—United States, 2009. MMWR Surveill Summ. 2010;59(5):1–142. [PubMed] [Google Scholar]
- 33.Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, et al. CDC growth charts: United States. Adv Data. 2000(314):1–27. [PubMed] [Google Scholar]
- 34.Spear BA, Barlow SE, Ervin C, et al. Recommendations for treatment of child and adolescent overweight and obesity. Pediatrics. 2007;120(Supplement 4):S254–S288. [DOI] [PubMed] [Google Scholar]
- 35.Simons-Morton B, Haynie D, Liu DP, Chaurasia A, Li KG, Hingson R. The effect of residence, school status, work status, and social influence on the prevalence of alcohol use among emerging adults. J Stud Alcohol Drugs. 2016;77(1):121–132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Trost SG, Sallis JF, Pate RR, Freedson PS, Taylor WC, Dowda M. Evaluating a model of parental influence on youth physical activity. Am J Prev Med. 2003;25(4):277–282. [DOI] [PubMed] [Google Scholar]
- 37.Currie C, Molcho M, Boyce W, Holstein B, Torsheim T, Richter M. Researching health inequalities in adolescents: The development of the Health Behaviour in School-Aged Children (HBSC) Family Affluence Scale. Soc Sci Med. 2008;66(6):1429–1436. [DOI] [PubMed] [Google Scholar]
- 38.Aiken LS, West SG. Multiple regression: testing and interpreting interactions. California: Sage Publications; 1991. [Google Scholar]
- 39.Neumark-Sztainer DR, Wall MM, Haines JI, Story MT, Sherwood NE, van den Berg PA. Shared risk and protective factors for overweight and disordered eating in adolescents. Am J Prev Med. 2007;33(5):359–369. [DOI] [PubMed] [Google Scholar]
- 40.Goldbach JT, Gibbs JJ. A developmentally informed adaptation of minority stress for sexual minority adolescents. J Adolesc. 2017;55:36–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ata RN, Ludden AB, Lally MM. The effects of gender and family, friend, and media influences on eating behaviors and body image during adolescence. J Youth Adolesc. 2007;36(8):1024–1037. [Google Scholar]
- 42.Carper TL, Negy C, Tantleff-Dunn S. Relations among media influence, body image, eating concerns, and sexual orientation in men: A preliminary investigation. Body image. 2010;7(4):301–309. [DOI] [PubMed] [Google Scholar]
- 43.Calzo JP, Corliss HL, Blood EA, Field AE, Austin SB. Development of muscularity and weight concerns in heterosexual and sexual minority males. Health Psychol. 2013;32(1):42–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.