

Abstract
Angiokeratomas are benign tumors characterized by proliferation and dilatation of blood vessels in the upper dermis. They are divided into widespread and localized forms. The localized forms are further classified as angiokeratoma of Fordyce, angiokeratoma circumscriptum neviforme, circumscribed angiokeratoma, and angiokeratoma of Mibelli, of which angiokeratoma of Fordyce is the most common. A 38-year-old female, with no systemic comorbidities presented with recurrent, asymptomatic dark, raised lesions over the vulva for 15 years, progressively increasing in size and number. There were no similar complaints in the family or spouse. On examination, multiple pedunculated hyperpigmented papules and nodular lesions with a verrucous surface were present over the bilateral labia majora and pubic area. Per speculum examination revealed no abnormalities. The oral, conjunctival, and genital mucosae were normal. There were no similar lesions elsewhere over the body. Histopathological examination revealed marked dilatation of papillary dermal vessels forming large, blood-filled cavernous channels, suggestive of angiokeratoma. The lesions were removed using radiofrequency. We present this case due to the rarity of its occurrence and to emphasize the importance of ruling out nonvenereal causes of genital lesions.
Keywords: Angiokeratoma, nodulocystic, vulva
INTRODUCTION
Angiokeratomas are benign tumors characterized by proliferation and dilatation of blood vessels in the superficial dermis, along with epidermal hyperplasia and hyperkeratosis.[1]
They are divided into widespread and localized forms. The localized forms are further classified as angiokeratoma of Fordyce, angiokeratoma circumscriptum neviforme, circumscribed angiokeratoma, and angiokeratoma of Mibelli, of which angiokeratoma of Fordyce is the most common.[2] It was first described by John Addison Fordyce in 1896.[3]
It most commonly presents as asymptomatic, blue-to-red, scaly papules over the scrotum, shaft of the penis, labia majora, medial aspect of the thighs, or lower abdomen.[4] They may bleed spontaneously, after scratching, on trauma or following sexual intercourse.[5]
STUDY DETAILS
A female aged 38 years presented with an asymptomatic, dark, raised lesions over the vulva for 15 years, initially small in size, with a gradual increase in size, and number over a period of 1–2 years. There was no associated pain, bleeding, or oozing from the lesions. There were no similar complaints in siblings or parents. There was no history of similar lesions in the spouse.
She gave a history of chylous discharge per vaginum 20 years ago, for which she underwent laparotomy and underrunning of lymphatics. She underwent cauterization of the lesions 2 years ago, and histopathological examination revealed features suggestive of angiokeratoma. She presently complains of recurrence of lesions since 6 months.
On examination, multiple pedunculated hyperpigmented papules and nodular lesions with a verrucous surface were present over bilateral labia majora and pubic area [See Figure 1]. There was no oozing or bleeding from the lesions. Per speculum examination revealed no abnormalities. The oral, conjunctival, and genital mucosae were normal. There were no similar lesions elsewhere over the body. Systemic examination revealed no abnormalities.
Figure 1.

Multiple verrucous papules and nodules over the vulva
Her blood and urine routine investigations were within normal limits. HIV, Hepatitis B virus surface antigen, and venereal disease research laboratory tests were nonreactive. The lesions were cauterized, and histopathological examination revealed hyperkeratosis, irregular acanthosis, and elongation of rete ridges in the epidermis. There was marked dilatation of papillary dermal vessels forming large, blood-filled cavernous channels, suggestive of angiokeratoma [See Figures 2 and 3].
Figure 2.
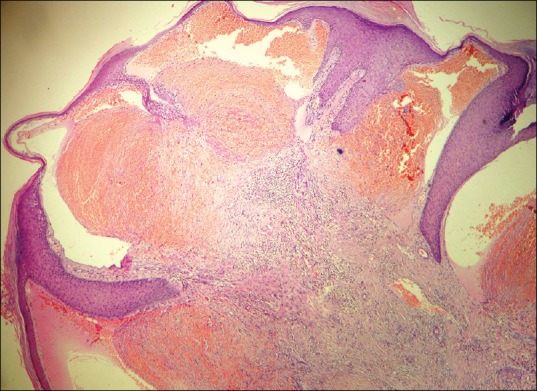
Dilated dermal blood vessels forming cavernous channels (H and E, ×10)
Figure 3.
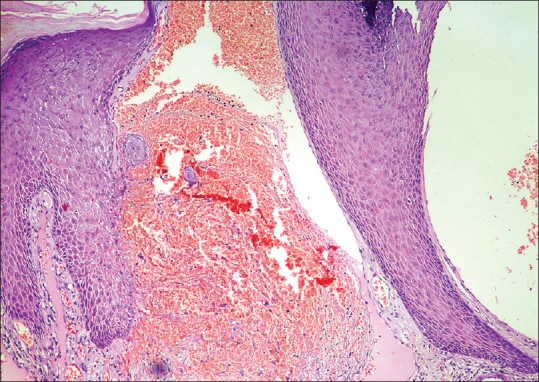
Dilated dermal vessels (H and E, ×40)
DISCUSSION
Angiokeratomas are benign tumors characterized by proliferation and dilatation of blood vessels in the superficial dermis, along with epidermal hyperplasia and hyperkeratosis.[1]
They are divided into widespread and localized forms. The localized forms are further classified as angiokeratoma of Fordyce, angiokeratoma circumscriptum neviforme, circumscribed angiokeratoma and angiokeratoma of Mibelli, of which angiokeratoma of Fordyce is the most common.[2] It was first described by John Addison Fordyce in 1896.[3]
It most commonly presents as asymptomatic, blue-to-red, scaly papules over the scrotum, shaft of the penis, labia majora, medial aspect of the thighs, or lower abdomen.[4] They may bleed spontaneously, after scratching, on trauma or following sexual intercourse.[5]
The various indications for the treatment of angiokeratomas are pruritis, bleeding, burning, and dyspareunia.[6] Treatment options include electrocautery, radiofrequency, cryotherapy, or ablative lasers, such as erbium-doped yttrium aluminum garnet laser or CO2 Laser, the last two modalities having the advantage of minimal scarring.[2]
We present this case due to the rarity of its occurrence, and to emphasize the importance of ruling out nonvenereal causes of genital lesions.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Fogagnolo L, Cintra ML, Velho PE. Angiokeratoma of the vulva. An Bras Dermatol. 2011;86:333–5. doi: 10.1590/s0365-05962011000200017. [DOI] [PubMed] [Google Scholar]
- 2.Kudur MH, Hulmani M. Giant angiokeratoma of fordyce over the vulva in a middle-aged woman: Case report and review of literature. Indian J Dermatol. 2013;58:242. doi: 10.4103/0019-5154.110856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Imperial R, Helwig EB. Angiokeratoma. A clinicopathological study. Arch Dermatol. 1967;95:166–75. doi: 10.1001/archderm.95.2.166. [DOI] [PubMed] [Google Scholar]
- 4.Blair C. Angiokeratoma of vulva. Br J Dermatol. 1970;83:401–11. doi: 10.1111/j.1365-2133.1970.tb15727.x. [DOI] [PubMed] [Google Scholar]
- 5.Laxmisha C, Dubey AK, Thappa DM, Jayanthi S. Angiokeratoma of fordyce. Indian J Sex Transm Dis. 2004;25:42–3. [Google Scholar]
- 6.Buljan M, Poduje S, Situm M, Bulat V, Bolanča Z, Tomas D, et al. Multiple angiokeratomas of the vulva: Case report and literature review. Acta Dermatovenerol Croat. 2010;18:271–5. [PubMed] [Google Scholar]