

Abstract
Background:
Health literacy can be considered as a factor affecting healthcare providers' decision-making. The aim of this study was to investigate health literacy status and its relationship with quality of life among the nurses working in teaching hospitals affiliated with Shiraz University of Medical Sciences in Iran.
Materials and Methods:
This cross-sectional study was conducted in 2017. To this end, 185 nurses from hospitals were selected by stratified random sampling. The data collection instruments included the standardized Health Literacy Questionnaire and the 36-Item Short Form Health Survey. The data were analyzed through descriptive statistics as well as t test, analysis of variance, Pearson correlation coefficient, and multivariate linear regression analysis using SPSS23 (α = 5%).
Results:
The mean scores for health literacy and quality of life were 70.06 (12.98) and 60.86 (17.26), respectively. A significant relationship was observed between the health literacy and quality of life (p <0.001), Access (p = 0.004), reading skills (p = 0.004), understanding (p = 0.016), and application of health information (p = 0.012) as the dimensions of health literacy were identified among the predictors of quality of life. In addition, there was a significant relationship among age (r = 0.22, p = 0.008), work experience (r = 0.27, p = 0.002), and employment relationship (F = 3.89, p = 0.005) and the mean score for nurses' health literacy status.
Conclusions:
A significant relationship was observed between health literacy and quality of life in nurses. Healthcare policy-makers are suggested to take measures to develop programs on promoting health literacy and related skills to improve the status of quality of life among nurses.
Keywords: Health literacy, hospitals, Iran, nurses, quality of life, teaching
Introduction
Health literacy refers to a wide range of skills and resources associated with individuals' ability and capacity to obtain, process, and understand health-related information that needs constant attention and updating during life.[1] World Health Organization (WHO) has defined health literacy as social and cognitive skills determining the individuals' motivation and quality in terms of obtaining, understanding, and applying information in a way that leads to their health promotion.[2] Moreover, health literacy can play an important role in providing quality services and care for patients within healthcare systems.[3]
Given the importance and effective position of health literacy in improving service provision and despite various domestic and international research studies in this domain, there have been few studies conducted on healthcare providers, especially the nurses. It should be noted that the nursing profession considered among the largest groups of healthcare service providers[4] required to have an acceptable level of health literacy with respect to their tasks and responsibilities and their relationships with patients. Additionally, the nurses' health literacy status and their awareness of this issue within the whole healthcare provision system are effective, particularly in the domain of patient relationships and safety.[5] Moreover, continuous scientific breakthroughs along with patients' variable status demand the integration of technical skills and professional knowledge by nurses to recognize the patients' problems and take steps in terms of designing, implementing, and evaluating programs to reduce errors and increase the quality of care.[6]
In this regard, the results of a study by Walker et al. revealed that individuals endowed with higher levels of health literacy had more information about their health status.[7] Moreover, Diviani et al. in their review reported study that people with low levels of health literacy had a smaller amount of ability to evaluate information, understand quality, and trust information.[8] In the same study in Iran, the results of an investigation by Tehrani Banihashemi et al. in 15 provinces and the findings of a study by Peyman and Samiee-Roudi among health community center workers suggested that health literacy had been rated at low levels.[9,10]
However, interest in measuring the quality of life as a concept has been growing along with numerous improvements in various aspects and levels of life.[11] The WHO has defined the quality of life as an individual's imaginations of his/her life status considering the culture and the value system in which they live and the relationship between these perceptions, expectations, and priorities.[12] It is also noteworthy that the quality of life is a multidimensional concept and reflects an individual's level of satisfaction and current functioning. In the meantime, the nurses' poor quality of life would negatively influence their professional satisfaction and their functioning.[13] In this domain, Cimete in a study on the relationship between job satisfaction and quality of life among 501 nurses showed that the nurses' quality of life items were significantly correlated with job satisfaction.[14] Moreover, Drobnic and Guillen in their investigation stated that good quality of life and overall welfare depended on the individuals' work and family conditions.[15]
It should be noted that working life is an important and meaningful part of personal life so that Hsu citing Frell considered occupation as one of the factors affecting the quality of life[16] because occupational stress is recognized as a very important factor affecting a person's quality of life.[17] Meanwhile, hospitals, as organizations, can seriously exert pressure on clients and especially nurses, which will subsequently have their own physical and psychological effects because nursing profession is inherently stressful and stress can similarly affect the nurses' quality of life and health status.[18] Investigating the mental health status and quality of life in physicians, nurses, and other hospital professions, Su et al. concluded that quality of life among all groups working in hospitals was poor and problems were much more among nurses and pharmacists than other groups. The noteworthy issue is that nurses rarely think about their individual needs although they have received trainings in terms of patient care and quality of life.[19] Moreover, evidence suggests that healthcare service providers, especially nurses, play a key role in patient education owing to greater access to patients and their families have no knowledge and skills needed in the domain of health literacy.[20] Moreover, quality of life is included among the factors affecting daily life, functioning, efficiency, and job satisfaction in nurses. In this regard, Hosieni et al. in a study with the aim of the relationship between quality of life and health literacy in retired staff of Rafsanjan University of Medical Sciences, indicate that health literacy can be a determinant factor for the score of quality of life.[21] At the same time Kooshyar et al. stated that those with the adequate health literacy had higher level of quality of life.[22]
Therefore, conducting studies to determine the levels of health literacy and quality of life and investigating the relationship and impact of the first variable on the second one and if necessary informing the managers and relevant authorities with the purpose of planning in terms of improving the health status of this group of population is of utmost importance. Given the lack of similar investigations, the present study aimed at examining the status, relationship, and effect of health literacy on the quality of life among the nurses working in teaching hospitals affiliated with Shiraz University of Medical Sciences in Iran in 2017.
Materials and Methods
This study was a descriptive-analytic cross-sectional research conducted in 2017 (From September 17 to November 23). The study population consisted of nurses working in 10 teaching hospitals affiliated with Shiraz University of Medical Sciences. Given that the levels of health literacy and quality of life are measured depending on the nurses' perceptions, an individual was considered as the unit of analysis in this study. In addition, an initial sample was selected from the occupational group (nurses) examined, and then the correlation value of 0.20 between health literacy and quality of life was obtained. After that, from the population studied (2943 people), 185 individuals were determined as the sample size according to the confidence level of 95% and the test power of 0.08. The sample was distributed using a proportional stratified Random Sampling among 10 hospitals (including Namazi Hospital, Faghihi Hospital, Ali Asghar (AS) Hospital, Dastgheib Hospital, Rajaei Hospital, Chamran Hospital, Khalili Hospital, Zeynabiyeh Hospital, Ibn Sina Hospital, and Hafez Hospital). It should be noted that the nurses were selected randomly from their personnel codes and random number table.
To collect the data and describe the nurses' perspectives, two questionnaires were used. The data on quality of life were collected using the standardized 36-Item Short Form Health Survey. The given questionnaire contains 36 items composed of 8 subscales, each one containing 2 to 10 items. The eight subscales within this questionnaire are physical functioning (PF) (10 items), limits in playing a role because of the physical problems (PP) (4 items), limits in playing a role because of the emotional problems (EP) (3 items), energy/fatigue (E/F) (4 items), mental health (MH) (5 items), social functioning (SF) (2 items), bodily pain (BP) (2 items), and general health (GH) (5 items). In addition, two overall subscales emerged through integrating the given subscales entitled as physical health (sum of the subscales of PF, PP, BP, and GH) and mental health (sum of the subscales of EP, E/F, MH, and SF) totally reflecting the quality of life in nurses. Scoring the items ranged from 0 to 100 depending on the type of items. To determine the final score for the quality of life as a number between 0 and 100, first, we calculated the scores for all the eight subscales; then, the two subscales of physical health and mental health were estimated from the combination of the subscales; and finally, quality of life was calculated from the combination of these two overall subscales. Moreover, the quality of life was classified into High (score 75 and above), Moderate (scores from 50 to 74), and Low (score 50 and below) levels.
To confirm the face and content validity, the questionnaire was reviewed and approved by six healthcare management specialists of faculty member of Shiraz University of Medical Sciences. To assay the reliability of the questionnaire, we used Cronbach's alpha method. To this end, a primary sample including 40 questionnaires were pre-assayed and then using the data from these questionnaires the amount of reliance ratio was calculated as 0.821, applying Cronbach's alpha method.
The data related to health literacy were also collected using the Health Literacy Questionnaire designed by Montazeri et al.[23] in 2014. This questionnaire consists of two parts: general items and specific items. The general items include age, gender, level of education, work experience, and employment status; the specific ones include items related to the variables examined from the objectives of the study. This part is comprised of 33 items and 5 components including access (6 items), reading skills (health information, forms, records, tests, etc.; 4 items), understanding and perception (7 items), ability to evaluate (4 items), and application of health information (decision-making) (12 items). A 5-point Likert-type scale was also used for the answers in this questionnaire; the responses are categorized and graded at a 5-option range. These options are as follows: Always (100 points), usually (75 points), Sometimes (50 points), rarely (25 points), and Never (0 point) were considered for the components of access, understanding and perception, evaluation, and application of health information. The options for the component of reading skills were also Quite Easy (100 points), Easy (75 points), Neither Easy Nor Hard (50 points), Hard (25 points), and Quite Hard (0 point). Given the scoring, the mean score of total literacy level was a number between 0 and 100, so the total mean score below 50 reflects low level of health literacy, the mean score between 50 and 74 represents moderate level of health literacy, and those above 75 show high level of health literacy. The reliability of this questionnaire using Cronbach's alpha coefficient of 0.89 and its validity have been confirmed in a study by Montazeri et al.[23]
To collect the data, one of the researchers referred to the selected hospitals and after the coordination with the manager and nursing office, the researcher went to the clinical wards and distributed the questionnaires among the nurses. In this regard, he tried to stay in the wards at the times with the lower load work of the nurses.
Once the questionnaires were completed (Self-Administrated) and returned, the data were analyzed through descriptive statistics and t test, analysis of variance (ANOVA), Pearson correlation coefficient, and multivariate linear regression analysis using the SPSS software, version 13 (SPSS Inc., Chicago, IL, USA), considering the significance level of α = 5%.
Ethical considerations
The participants were justified about the objectives of the study; the principle of confidentiality was also emphasized and their verbal consent was obtained. Then, anonymous questionnaires without any first names and surnames were distributed among the respondents. In addition, participants were free to leave the study at any stage if they did not want to continue. The researcher tried to stay in the clinical wards at the time of completing the questionnaires by the nurses to assure the accuracy of the participants' answers. At the same time, he tried to justify the importance of the study topic for the participants to increase the response rate.
Results
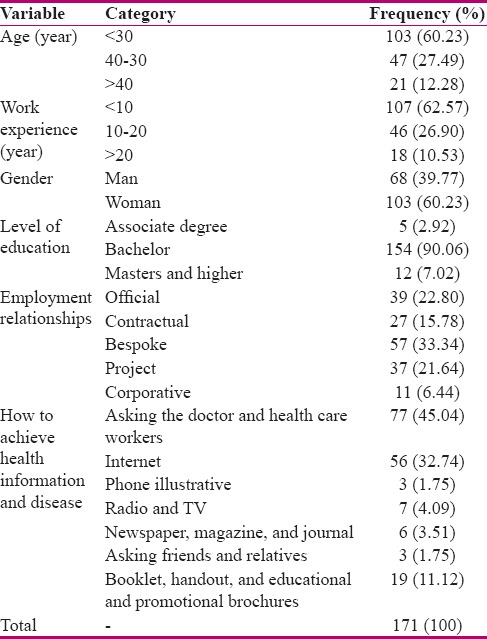
Out of the 185 questionnaires distributed, 171 were completed in full (92.43% response rate). The mean (SD) age of the nurses participating in this study was 30.94 (8.44) years, and most of these individuals (60.23%) were placed in the age group below 30 years. The mean (SD) of work experience was 7.82 (6.84) years, and most of the nurses (62.57%) were in the group with lower than 10 years of service. In terms of gender, 60.23% of the participants were female. The majority of the respondents had a bachelor's degree (90.06%) and their employment relationship was contractual recruitment (33.34). Most of the examined nurses were obtaining information about health issues and diseases through asking physicians, healthcare professionals (45.04), and the Internet (32.74). Table 1 shows the frequency distribution of the nurses participating in the present study.
Table 1.
Frequency of nurses in educational hospitals of Shiraz University of Medical Sciences
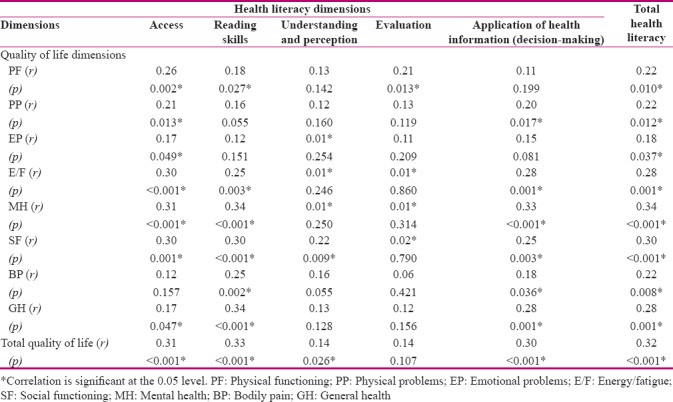
From the results, the mean (SD) score of “health literacy” was 76.06 (12.98), which represented a relatively high level of health literacy in nurses. Among the dimensions of this variable, the highest mean (SD) score was related to the component of understanding and perception (81.50 (13.75)), and the lowest mean (SD) score was assigned to the component of evaluation (74.37 (12.20)). Moreover, the mean (SD) score for “quality of life” was estimated by 60.86 (17.26), indicating its moderate level in nurses. Among the subscales of the quality of life, “PF” and “SF” obtained the highest (65.05 (17.19)) and the lowest (57.43 (21.42)) mean (SD) scores, respectively. In addition, the mean (SD) score for the scale of “physical health” as the sum of the combination of the PF, PP, BP, and GH sub-scales was estimated equal to 62.51 (18.65) and the mean (SD) score for the scale of “mental health” as the sum of the combination of the EP, E/F, MH, and SF sub-scales was calculated by 59.38 (19.16) [Table 2]. Moreover, the findings demonstrated a statistically significant and direct relationship between health literacy and quality of life (r = 0.32, p > 0.001) [Table 3].
Table 2.
The Frequency of health literacy and quality of life in nurses who worked in educational hospitals of Shiraz University of Medical Sciences
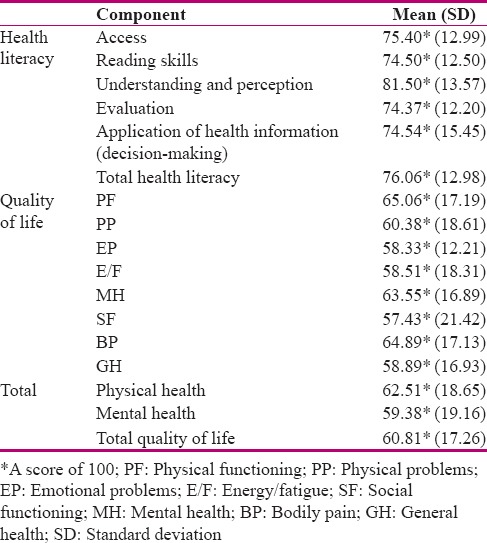
Table 3.
Correlation between Health Literacy and Quality of Life of Nurses in Educational Hospitals of Shiraz University of Medical Sciences
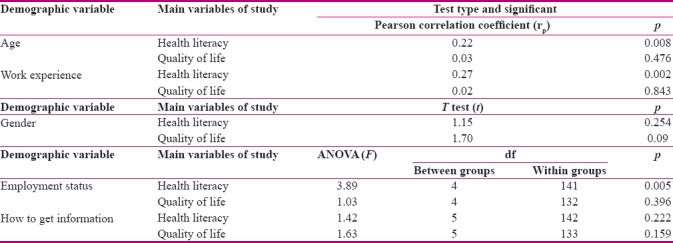
A relationship was also observed in the results for the mean scores of health literacy and age (r = 0.22, p = 0.008), work experience (r = 0.27, p = 0.002), and status employment relationship (F = 3.89, p = 0.005) [Table 4].
Table 4.
Relationship between variables of health literacy and quality of life with demographic characteristics of nurses in educational hospitals of Shiraz University of Medical Sciences
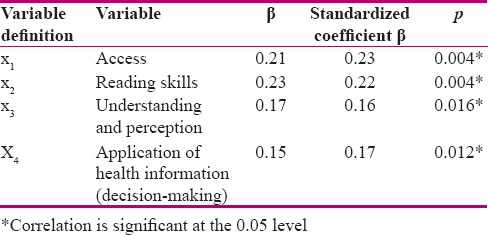
The findings of the multivariate linear regression analysis determining the impact of different dimensions of health literacy and demographic variables on quality of life in nurses indicated that the existing significant variables included in the model using the Enter method were access, reading skills, application of health information (decision-making), and understanding and perception. The β values associated with influential variables reflecting the priorities of effectiveness on quality of life are given in Table 5. This analysis also showed that the adjusted R-squared was equal to 0.207. This means that 20.70% of the changes in the quality of life scores could be explained by the variables in the given model. The linear equation of the quality of life scores in nurses was also obtained from the multivariate linear regression analysis and the model used could be a good predictor of the variable of quality of life at the significance level of 0.002. Y = 17.31 + 0.21x1 + 0.23x2 + 0.15x3 + 0.17x4 (Y: quality of life score and x1,2,3,4: variables affecting quality of life in nurses examined) [Table 5].
Table 5.
The variables affecting the quality of life in the nurses of the educational hospitals of Shiraz University of Medical Sciences from linear regression test
Discussion
This study aimed at investigating health literacy status and its relationship with quality of life in nurses working in teaching hospitals affiliated with Shiraz University of Medical Sciences in Iran. The findings of this study suggested that the nurses' level of health literacy was high; this is consistent with the results of an investigation performed by Owens[24] entitled as health literacy; a training program for professional acute care nurses. It should be noted that health literacy has been recognized as a critical and important index of healthcare results and costs, which is today a requirement for healthcare system. The given literacy in health professionals can also be an important factor affecting nurses' decision-making and functioning in health systems to improve public health.[25] Because nurses are among the groups employed in the domain of healthcare and also engaged in repeated relationships with healthcare issues in hospitals, they need to have an optimal level of health literacy; thus, the results obtained in the present study confirmed this issue. According to the findings of this study, quality of life in nurses was estimated at moderate levels. In this regard, factors such as occupational stress, high emotional disturbances, close relationships with patients, and responsibility for their mortality and life, as well as the presence of other factors can be considered as the stressors leading to a decline in quality of life and its moderate level. In this regard, Oujian et al.[26] also showed in their study that quality of life among the majority of nurses (90%) was at moderate levels. It should be noted that the quality of life is similarly considered among the factors affecting everyday life, functioning, efficiency, and job satisfaction in nurses.[27] Thus, this variable along with attempts to enhance it can play a significant role in individuals' health status as well as personal and social life.[28] Additionally, it is also considered as an important factor influencing the stability and effectiveness of healthcare systems.[29]
The results of the study correspondingly indicated a significant relationship between the levels of literacy and quality of life in nurses reflecting the impact of health literacy on improving the quality of life. In this line, an investigation by Song et al. showed that adequate health literacy was significantly accompanied by increased scores of physical and mental dimensions of quality of life in the study subjects.[30] Several studies have similarly suggested that low levels of health literacy can bring about undesirable consequences such as poor public health and physical fitness, increased disabilities and pains, decreased physical functioning, limited mobility and dynamicity, and consequently reduced quality of life.[31] In another research study, Ownby et al. investigating the relationship among the quality of life, health conditions, and available health services and health literacy suggested that health literacy status was significantly and positively correlated with conceptualization, quality of life, and health behaviors.[32] Furthermore, the findings by Muir et al. revealed that individuals with lower levels of health literacy had the worst quality of life.[33] Wallace et al. also examined the relationship between health literacy and health-related quality of life in Tanzania and showed that health literacy was significantly correlated with some of the components of quality of life such as public health. Additionally, people with low health literacy status could get through more physically unhealthy days along with more limited daily activities.[34] In addition, Dominick et al. in their study concluded that individuals with adequate health literacy were endowed with higher physical activity self-efficacy (playing a key role in changing behaviors and subsequently quality of life).[35] In this respect, Osborn et al. reported a significant relationship between health literacy and physical functioning as one of the dimensions of quality of life.[36]
Finally and given the investigation of the relationship between health literacy, quality of life, and demographic variables; the results of this study suggested a statistically significant relationship between the health literacy and variables of age, work experience, and employment relationship. In this line, several studies by Lee et al.,[37] Cho et al.,[38] and Paasche-Orlow et al.[39] also reported a significant relationship between age and health literacy status.
Among the limitations of the present study was no investigation on health literacy and quality of life in nurses separately for each department whose one of its reasons was the high dispersion of departments within hospital departments.
Conclusion
The levels of health literacy and quality of life among the nurses were reported high and moderate, respectively. Moreover, a significant relationship was observed between these two variables. This issue highlighted the importance of more attention to health literacy as a relatively new concept in nursing health promotion programs and subsequently quality of life in nurses. Therefore, managers and policy-makers in the domain of healthcare were suggested to take steps in terms of planning and designing systematic and accurate programs targeting further development of health literacy and its relevant skills to improve the quality of life among nurses as one of the most important factors of healthcare provision in hospitals.
Financial support and sponsorship
Shiraz University of Medical Sciences
Conflicts of interest
Nothing to declare.
Acknowledgments
This article was the result of a research project approved by Shiraz University of Medical Sciences with the code number of 95-01-68-13805 (Date: 2017-09-17). We hereby appreciate and express our gratitude to the Vice-Chancellor's Office for Research at the given university for their spiritual and financial supports as well as all hospital administrators and nurses who cooperated in this study.
References
- 1.Norman C. EHealth literacy 2.0: Problems and opportunities with an evolving concept. J Med Internet Res. 2011;13:e125. doi: 10.2196/jmir.2035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.James BD, Boyle PA, Bennett JS, Bennett DA. The impact of health and financial literacy on decision making in community-based older adults. Gerontology. 2012;58:531–9. doi: 10.1159/000339094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Macabasco-O'Connell A, Fry-Bowers EK. Knowledge and perceptions of health literacy among nursing professionals. J Health Commun. 2011;16(Suppl 3):295–307. doi: 10.1080/10810730.2011.604389. [DOI] [PubMed] [Google Scholar]
- 4.Sanders LM, Thompson VT, Wilkinson JD. Caregiver health literacy and the use of child health services. Pediatrics. 2007;119:e86–92. doi: 10.1542/peds.2005-1738. [DOI] [PubMed] [Google Scholar]
- 5.Cafiero M. Nurse practitioners' knowledge, experience, and intention to use health literacy strategies in clinical practice. J Health Commun. 2013;18(Suppl 1):70–81. doi: 10.1080/10810730.2013.825665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hosseini F, Kazemi M, Akbari A. the role of general health, in the occurrence of nursing errors, among nurses in Rafsanjan university of medical sciences in 2012. J Community Health. 2014;7:27–35. [Google Scholar]
- 7.Walker J, Pepa C, Gerard PS. Assessing the health literacy levels of patients using selected hospital services. Clin Nurse Spec. 2010;24:31–7. doi: 10.1097/NUR.0b013e3181c4abd0. [DOI] [PubMed] [Google Scholar]
- 8.Diviani N, van den Putte B, Giani S, van Weert JC. Low health literacy and evaluation of online health information: A systematic review of the literature. J Med Internet Res. 2015;17:e112. doi: 10.2196/jmir.4018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tehrani Banihashemi S, Amirkhani MA, Haghdoost AA, Alavian S, Asgharifard H, Baradaran H, et al. Health literacy and the influencing factors: A study in five provinces of Iran. Strides Dev Med Educ. 2007;4:1–9. [Google Scholar]
- 10.Peyman N, Samiee-Roudi K. Investigating the status of health literacy among health providers of rural area. J Health Lit. 2016;1:46–52. [Google Scholar]
- 11.Landeiro F, Walsh K, Ghinai I, Mughal S, Nye E, Wace H, et al. Measuring quality of life of people with predementia and dementia and their caregivers: A systematic review protocol. BMJ Open. 2018;8:e019082. doi: 10.1136/bmjopen-2017-019082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.PrasannaKumar HR, Mahesh MG, Menon VB, Srinath KM, Shashidhara KC, Ashok P, et al. Patient self-reported quality of life assessment in type 2 diabetes mellitus: A pilot study. Niger J Clin Pract. 2018;21:343–9. doi: 10.4103/njcp.njcp_433_16. [DOI] [PubMed] [Google Scholar]
- 13.López Espuela F, Portilla Cuenca JC, Leno Díaz C, Párraga Sánchez JM, Gamez-Leyva G, Casado Naranjo I, et al. Sex differences in long-term quality of life after stroke: Influence of mood and functional status. Neurologia. 2017 doi: 10.1016/j.nrl.2017.10.002. pii: S0213-4853(17)30347-X. [DOI] [PubMed] [Google Scholar]
- 14.Cimete G, Gencalp NS, Keskin G. Quality of life and job satisfaction of nurses. J Nurs Care Qual. 2003;18:151–8. doi: 10.1097/00001786-200304000-00009. [DOI] [PubMed] [Google Scholar]
- 15.Drobnič S, Guillén Rodríguez AM. Tensions between work and home: Job quality and working conditions in the institutional contexts of Germany and Spain. Soc Polit. 2011;18:232–68. doi: 10.1093/sp/jxr008. [DOI] [PubMed] [Google Scholar]
- 16.Hsu MY. A quality of working life survey instrument for hospital nurses. J Nurs Res. 2016;24:87–99. doi: 10.1097/jnr.0000000000000098. [DOI] [PubMed] [Google Scholar]
- 17.Brooks BA, Anderson MA. Nursing work life in acute care. J Nurs Care Qual. 2004;19:269–75. doi: 10.1097/00001786-200407000-00014. [DOI] [PubMed] [Google Scholar]
- 18.Moradi T, Maghaminejad F, Azizi-Fini I. Quality of working life of nurses and its related factors. Nurs Midwifery Stud. 2014;3:e19450. [PMC free article] [PubMed] [Google Scholar]
- 19.Su JA, Weng H, Tsang H, Wu JL. Mental health and quality of life among doctors, nurses and other hospitals staff. Stress Health. 2009;25:423–30. [Google Scholar]
- 20.Hosieni F, Mirzaei T, Ravari A, Akbary A. The relationship between health literacy and quality of life in retirement Rafsanjan University of medical sciences. J Health Lit Summer. 2016;1:92–9. [Google Scholar]
- 21.Kooshyar H, Shoorvazi M, Dalir Z, Hosseini M. Health literacy and its relationship with medical adherence and health-related quality of life in diabetic community-residing elderly. J Mazandaran Univ Med Sci. 2014;23:134–43. [Google Scholar]
- 22.Coleman C. Teaching health care professionals about health literacy: A review of the literature. Nurs Outlook. 2011;59:70–8. doi: 10.1016/j.outlook.2010.12.004. [DOI] [PubMed] [Google Scholar]
- 23.Montazeri A, Tavousi M, Rakhshani F, Azin SA, Jahangiri K, Ebadi M, et al. Health literacy for Iranian adults (HELIA): Development and psychometric properties. Payesh. 2014;13:589–99. [Google Scholar]
- 24.Owens LM. Health Literacy: An Educational Program for the Acute Care Professional Nurse, Doctoral Dissertation. Capella University. 2015. [Last accessed on 2017 Sep 12]. Available from: http://www.nursinglibrary.org/vhl/handle/10755/565642 .
- 25.Al-Yateem N, Rossiter RC, Robb WF, Slewa-Younan S. Mental health literacy of school nurses in the United Arab Emirates. Int J Ment Health Syst. 2018;12:6. doi: 10.1186/s13033-018-0184-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Oujian P, Alhani F, Tol A. Reviewing the work and family conflict and its association with quality of life among clinical nurses. J Health Syst Res. 2013;9:345–53. [Google Scholar]
- 27.Azizi M, Baroony Zadeh Z, Motamedzade M, Goli SH. Life study of nurses quality of life using who questionnaire in hospitals of Hamadan university of medical sciences. J Occup Hyg Eng. 2015;1:68–75. [Google Scholar]
- 28.Wu SY, Li HY, Tian J, Zhu W, Li J, Wang XR, et al. Health-related quality of life and its main related factors among nurses in China. Ind Health. 2011;49:158–65. doi: 10.2486/indhealth.ms1160. [DOI] [PubMed] [Google Scholar]
- 29.Mardani Hamole M, Shahraki Vahed A. The relationship between mental health and quality of life in cancer patients. JSSU. 2010;18:111–7. [Google Scholar]
- 30.Song L, Mishel M, Bensen JT, Chen RC, Knafl GJ, Blackard B, et al. How does health literacy affect quality of life among men with newly diagnosed clinically localized prostate cancer? Findings from the North Carolina-Louisiana prostate cancer project (PCaP) Cancer. 2012;118:3842–51. doi: 10.1002/cncr.26713. [DOI] [PubMed] [Google Scholar]
- 31.Bennett JS, Boyle PA, James BD, Bennett DA. Correlates of health and financial literacy in older adults without dementia. BMC Geriatr. 2012;12:30. doi: 10.1186/1471-2318-12-30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ownby RL, Acevedo A, Jacobs RJ, Caballero J, Waldrop-Valverde D. Quality of life, health status, and health service utilization related to a new measure of health literacy: FLIGHT/VIDAS. Patient Educ Couns. 2014;96:404–10. doi: 10.1016/j.pec.2014.05.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Muir KW, Santiago-Turla C, Stinnett SS, Herndon LW, Allingham RR, Challa P, et al. Health literacy and vision-related quality of life. Br J Ophthalmol. 2008;92:779–82. doi: 10.1136/bjo.2007.134452. [DOI] [PubMed] [Google Scholar]
- 34.Wallace LS, Rogers ES, Weiss BD. Relationship between health literacy and health-related quality of life among Tennesseans. Tenn Med. 2008;101:35–9. [PubMed] [Google Scholar]
- 35.Dominick GM, Dunsiger SI, Pekmezi DW, Marcus BH. Health literacy predicts change in physical activity self-efficacy among sedentary Latinas. J Immigr Minor Health. 2013;15:533–9. doi: 10.1007/s10903-012-9666-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Osborn CY, Paasche-Orlow MK, Bailey SC, Wolf MS. The mechanisms linking health literacy to behavior and health status. Am J Health Behav. 2011;35:118–28. doi: 10.5993/ajhb.35.1.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Lee SY, Tsai TI, Tsai YW, Kuo KN. Health literacy, health status, and healthcare utilization of Taiwanese adults: Results from a national survey. BMC Public Health. 2010;10:614. doi: 10.1186/1471-2458-10-614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Cho YI, Lee SY, Arozullah AM, Crittenden KS. Effects of health literacy on health status and health service utilization amongst the elderly. Soc Sci Med. 2008;66:1809–16. doi: 10.1016/j.socscimed.2008.01.003. [DOI] [PubMed] [Google Scholar]
- 39.Paasche-Orlow MK, Parker RM, Gazmararian JA, Nielsen-Bohlman LT, Rudd RR. The prevalence of limited health literacy. J Gen Intern Med. 2005;20:175–84. doi: 10.1111/j.1525-1497.2005.40245.x. [DOI] [PMC free article] [PubMed] [Google Scholar]