

Abstract
Introduction:
Isolated tibial tubercle fractures or patellar tendon ruptures are common injuries in adolescents. However, combined tubercle fractures with patellar tendon ruptures are rare, and hence, there are no definitive methods of surgical fixation or post-operative protocols.
Case Report:
A 13-year-old healthy girl sustained an extensor mechanism injury after the left knee hyperflexion during a fall from skateboarding. On examination, the extensor mechanism was not functional against gravity. Radiographic imaging revealed a displaced tibial tubercle fracture with patella alta, and magnetic resonance imaging revealed a concomitant patellar tendon avulsion from the tubercle. From a supine position on a radiolucent table, under general anesthesia and a femoral nerve block, the tibial tubercle fracture was fixed using two fully-threaded cortical screws. The patellar tendon was repaired with Fiber Wire through the Krakow method and secured through a tibial transosseous tunnel. A supplemental Fiber Wire was passed through a patellar tunnel and into a tibial tunnel to mitigate tension on the tendon repair. Post-operative knee motion was limited for 1 week to 60° of passive flexion, and full weight-bearing was permitted in a knee immobilizer.
Conclusion:
Given the rarity of this combined extensor mechanism injury in adolescents and despite several different fixation methods reported in the literature, there is no clearly superior surgical technique. This case demonstrates a technique allowing for stability of the tubercle fracture and robust repair of the patellar tendon that permits early range of motion and weight-bearing.
Keywords: Tibial tubercle fracture, patellar tendon avulsion, technique, surgery
Learning Point for this Article:
Although rare, combined tibial tubercle fractures with patellar tendon avulsions are an important consideration and require surgical technique that addresses both injuries.
Introduction
Physically, active adolescents are at particular risk for extensor mechanism injuries including patellar tendon ruptures or tibial tubercle fractures. Tibial tubercle avulsion fractures are uncommon and represent <1% of all physeal injuries [1], while patellar tendon ruptures are also uncommon with no clearly reported incidence. The combination of a tibial tubercle fracture with a concomitant patellar tendon rupture is a particularly rare occurrence, with only a few reported cases in the literature [2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13]. This unique combined injury to the extensor mechanism presents a challenge for operative fixation. Based on the aforementioned reported cases, a variety of surgical techniques to address the tibial tubercle fracture include open reduction and internal fixation with Kirschner wires, Sherman or cancellous screws, and cerclage wires, while the majority of techniques to address the patellar tendon rupture use suture repair of tendon to periosteum or transosseous sutures through the tibia. Moreover, there is variability with respect to recommended post-operative rehabilitation. The majority of post-operative protocols involve a short period of immobilization (4 weeks)with a cylinder or long leg cast and full weight-bearing, while few other authors have instituted early range of motion. There is no clearly favored approach toward operative fixation given the rarity of this type of injury. We present a case with this injury pattern and report on our surgical technique to facilitate early weight-bearing and knee range of motion. The authors have obtained the patient and parent’s informed written consent for print and electronic publication of the case report.
Case Report
The patient is a 13-year-old girl with no prior medical history who fell while skateboarding onto a hyper flexed left knee on the day of presentation. She experienced an immediate onset of knee pain with subsequent swelling and was unable to ambulate due to pain and weakness in her left leg. A review of systems was negative for sensory abnormalities or pain in other anatomical locations. On physical examination, the skin over the left knee was intact with no abrasions or open wounds. There was diffuse soft tissue swelling around the knee as well as a moderate knee joint effusion. She had exquisite tenderness to palpation directly over the tibial tubercle and patellar tendon, with an asymmetrically high-riding patella on palpation compared to the contralateral extremity. Although she was unable to straight leg raise against gravity, she was able to perform the maneuver with gravity eliminated, with moderate pain. Distally, she demonstrated full motor strength with ankle and great toe dorsi-and plantar flexion. Her sensation was grossly intact to light touch in all distributions distally. After examination, she underwent plain film imaging (Fig. 1), which demonstrated a displaced tibial tubercle fracture extending to the level of the proximal tibial physis (Ogden Type IIB) with concomitant patella alta. Given the latter finding, concern was raised for patellar tendon injury, and magnetic resonance imaging was obtained which demonstrated a patellar tendon rupture at the tubercle insertion site (Fig. 2). The patient’s left lower extremity was placed into a bulky jones dressing with a knee immobilizer and she was taken to the operating room the following day for operative intervention. The patient was positioned supine on a radiolucent table with a high left thigh tourniquet. After induction of general anesthesia, administration of prophylactic antibiotics and sterile preparation and draping, a regional femoral nerve block (0.25% Marcaine with epinephrine) was performed according to the surgeon’s preference to aid with post-operative pain control. The limb was exsanguinated using an Esmark wrap and the tourniquet was inflated. A longitudinal incision was made over the anterior aspect of the knee extending from the distal pole of the patella to 4cm below the tibial tubercle. Dissection was carried through the subcutaneous tissues down to the extensor mechanism, where the fracture and hematoma were encountered. The tibial tubercle fragment was found to be significantly rotated and displaced superiorly. Moreover, the anterior cortex of the tubercle was devoid of periosteum at the patellar tendon insertional footprint (consistent with a tendon avulsion), while some ruptured terminal tendon fibers remained attached to the tubercle. The tubercle’s periosteum was found to be attached to the undersurface of ruptured patellar tendon. After assessing the extent of the injury, the fracture edges were cleared of soft tissue, and the hematoma was suctioned and irrigated to allow for manual reduction. The reduction was provisionally held with two posteriorly directed 0.045-inch Kirschner wires, and definitive fixation was achieved using two fully-threaded 3.5-mm cortical screws(lengths, 38 mm and 45 mm) using standard AO technique. A large image intensifier was used to check the positioning of the wires and screws during this portion of the operation. After satisfactory reduction and screw position were achieved, attention was turned to the repair of the patellar tendon. The knee was positioned to 30oof flexion to avoid over tightening, and two #2 Fiber Wire sutures were placed into the patellar tendon using the Krakow method. A 3.5-mm drill was then used to introduce a transverse hole through the proximal tibia 2cm distal to the tubercle. The periosteum attached to the undersurface of the tendon was reapproximated onto its footprint on the tibial tubercle and was, thus, used as an anatomic landmark to help ensure appropriate tensioning of the tendon. The sutures were then passed through the bone tunnel and tied. To augment the repair, an additional #2 Fiber Wire was passed through a transverse drill hole introduced into the patella to a second transverse drill hole through the proximal tibia (4 cm below the tubercle). The suture was tensioned and corrected the patella alta and allowed the knee to flex to 60°without difficulty or undue tension on the tendon repair. This technique was previously described by Novacheck et al. [14] and is outlined in a diagram (Fig. 3). Final intraoperative fluoroscopic images were then obtained (Fig. 4). The wound was irrigated, the tourniquet was deflated, hemostasis was achieved, and a multilayered closure was performed. The remaining extensor mechanism tissue was repaired using 2-0 Ethibond in a figure-of-eight fashion, the deep soft tissue layers were approximated using 0vicryl, and the dermis and epidermis were approximated using 3-0 and 4-0 monocryl, respectively. Postoperatively, the left leg was placed into a knee immobilizer for the 1stweekduring full weight-bearing, and only taken out of the immobilizer to allow passive range of motion with up to 60° of flexion. After 1week, a hinged knee brace was used to allow full weight-bearing and active range of motion up to 60°, and physical therapy was initiated for range of motion exercises. At 4-week follow-up, radiographs of the knee demonstrated interval healing of the tubercle fracture (Fig. 5), and range of motion was advanced to 90°of flexion in the hinged knee brace.3-month postoperatively, the brace was discontinued, and at the 5-month follow-up visit and the patient had active knee range of motion from 0° to 130° with no clinically significant extensor lag.
Figure 1.
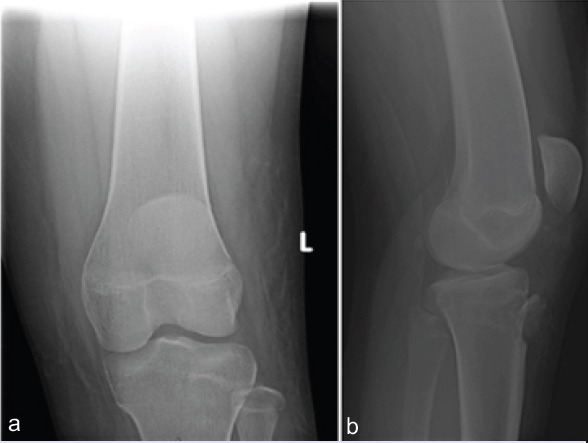
Anteroposterior (a) and lateral, (b) radiographs of the left knee demonstrating a displaced and rotated tibial tubercle fracture extending superiorly to the level of the proximal tibial physis and a high-riding patella.
Figure 2.
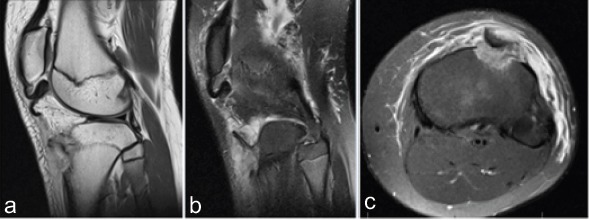
Sagittal plane T1 (a), T2 (b), and axial T2 (c) cuts from the magnetic resonance imaging study demonstrate the tibial tubercle fracture as well as the distal patellar tendon rupture occurring off of its tubercle insertion. The tubercle fragment is rotated 180°, as seen in the axial plane (c).
Figure 3.
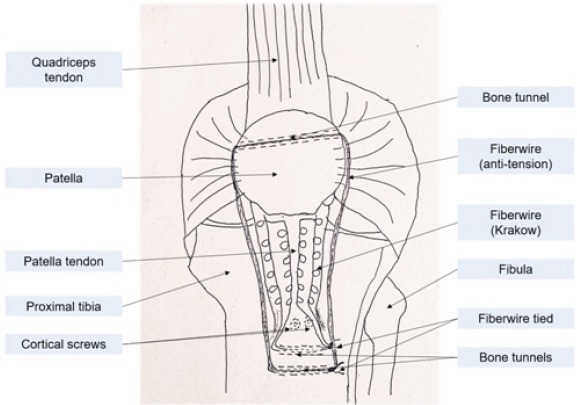
Diagram depicting the construct and technique of repair used to fix the tibial tubercle fracture with concomitant patellar tendon rupture.
Figure 4.
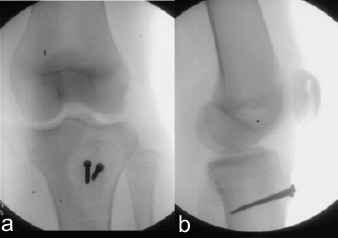
Anteroposterior (a) and lateral (b) views of the left knee obtained from intraoperative fluoroscopy demonstrating fixation of the tibial tubercle fracture with the use of two fully-threaded cortical screws. After FiberWire fixation of the patellar tendon, patellar height appears restored on the lateral view as compared with the lateral view in Figure 1.a
Figure 5.
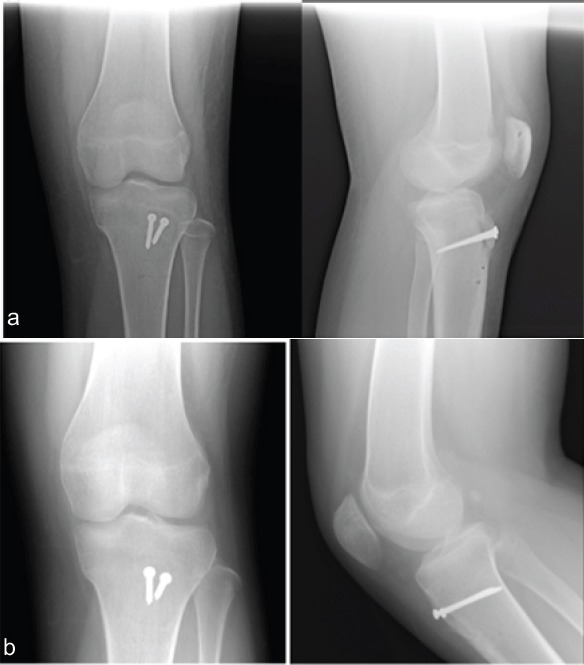
Anteroposterior and lateral radiographs of the left knee at 4 weeks (a) and 5 months (b) postoperatively showing healing of the tibial tubercle fracture with the two cortical screws in proper position. On the lateral views, the position of the transverse drill holes can be visualized in the patella and the proximal tibia.
Discussion
Isolated tibial tubercle fractures characteristically occur in adolescents aged 13—years through a mechanism involving eccentric contraction of the patellar tendon when the proximal tibial physis is closing [15]. However, in rare cases, failure of the extensor mechanism can be combined and involves rupture of the patellar tendon fromits tibial tubercle insertion with a concomitant tubercle fracture, as in the reported 15 cases [2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13]. In the current presented case of an adolescent with this type of injury, the mechanism appears similar to those reported in other cases. Nonetheless, it remains unclear why the extensor mechanism fails at two distinct locations, as there is no apparent difference in the mechanism for this injury compared with the typical isolated tubercle fractures or patellar tendon ruptures. Given the bifocal nature of this unique injury pattern, an operative intervention should be performed with the goals of anatomic reduction and biomechanically stable fixation of the tubercle fracture, as well as a repair of the patellar tendon to the proximal tibia that is strong enough to withstand tensile forces from early range of motion and also correct the patella alta. In our described technique, K-wires were used effectively to maintain reduction of the tubercle, while fully-threaded cortical screws were utilized to allow for compression and absolute stability of the fragment. Furthermore, the patellar tendon was repaired through proximal tibia transosseous tunnels, given that the tubercle periosteum was avulsed from the bone. The addition of a Fiber Wire construct through the patella into a separately drilled proximal tibial tunnel as previously described [14] offered adequate reinforcement to our tendon repair while off-loading tension on the repair. When performing this step, however, care must be taken to avoid over tensioning this suture, which would introduce excessive slack into the tendon repair and potentially weaken the extensor mechanism. Post-operative recovery protocols in the existing case reports range from leg casting for 4 weeks to early range of motion. Most protocols allow full weight-bearing immediately. With our performed surgical technique, we believe the repair is biomechanically strong enough to withstand early range of motion, with restriction to 60°of flexion to protect the repair from excessive tensile stress. A post-operative knee immobilizer was used for the 1stweek while weight-bearing to protect against potential injury to the repair from simultaneous flexion while bearing full weight. Further, follow-up will be continued to determine improvement in the patient’s functional capacity.
Conclusion
A combined tibial tubercle fracture and patellar tendon rupture is a rare injury in adolescents. Multiple fixation techniques and restricted post-operative range of motion protocols have been reported. This case report demonstrates a technique for screw and Fiber Wire surgical fixation to address both injuries and allow early range of motion and weight-bearing.
Clinical Message
This uncommon injury pattern results in an inherently unstable, incompetent extensor mechanism which necessitates surgical intervention. Screw fixation of the tibial tubercle and suture fixation of the patellar tendon, coupled with a tension-reducing, off-loading circumferential FiberWire suture, yield a stable construct that permits earlyfunctional range of motion.
Biography

Footnotes
Conflict of Interest: Nil
Source of Support: Nil
Consent: The authors confirm that Informed consent of the patient is taken for publication of this case report
References
- 1.Hamilton SW, Gibson PH. Simultaneous bilateral avulsion fractures of the tibial tuberosity in adolescence:A case report and a review of over 50 years of literature. Knee. 2006;13:404–7. doi: 10.1016/j.knee.2006.04.008. [DOI] [PubMed] [Google Scholar]
- 2.Clarke DO, Franklin SA, Wright DE. Avulsion fracture of the tibial tubercle associated with patellar tendon avulsion. Orthopedics. 2016;39:e561–4. doi: 10.3928/01477447-20160414-02. [DOI] [PubMed] [Google Scholar]
- 3.Frankl U, Wasilewski SA, Healy WL. Avulsion fracture of the tibial tubercle with avulsion of the patellar ligament. Report of two cases. J Bone Joint Surg Am. 1990;72:1411–3. [PubMed] [Google Scholar]
- 4.Frey S, Hosalkar H, Cameron DB, Heath A, David Horn B, Ganley TJ, et al. Tibial tuberosity fractures in adolescents. J Child Orthop. 2008;2:469–74. doi: 10.1007/s11832-008-0131-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Goodier D, Maffulli N, Good CJ. Tibial tuberosity avulsion associated with patellar tendon avulsion. Acta Orthop Belg. 1994;60:336–8. [PubMed] [Google Scholar]
- 6.Kaneko K, Miyazaki H, Yamaguchi T. Avulsion fracture of the tibial tubercle with avulsion of the patellar ligament in an adolescent female athlete. Clin J Sport Med. 2000;10:144–5. doi: 10.1097/00042752-200004000-00011. [DOI] [PubMed] [Google Scholar]
- 7.Kramer DE, Chang TL, Miller NH, Sponseller PD. Tibial tubercle fragmentation:A clue to simultaneous patellar ligament avulsion in pediatric tibial tubercle fractures. Orthopedics. 2008;31:501. doi: 10.3928/01477447-20080501-14. [DOI] [PubMed] [Google Scholar]
- 8.Mayba II. Avulsion fracture of the tibial tubercle apophysis with avulsion of patellar ligament. J Pediatr Orthop. 1982;2:303–5. doi: 10.1097/01241398-198208000-00012. [DOI] [PubMed] [Google Scholar]
- 9.Mosier SM, Stanitski CL. Acute tibial tubercle avulsion fractures. J Pediatr Orthop. 2004;24:181–4. doi: 10.1097/00004694-200403000-00009. [DOI] [PubMed] [Google Scholar]
- 10.Sie EJ, Kacou AD, Sery BL, Lambin Y. Avulsion fracture of the tibial tubercle associated with patellar ligament avulsion treated by staples. Afr J Paediatr Surg. 2011;8:105–8. doi: 10.4103/0189-6725.79071. [DOI] [PubMed] [Google Scholar]
- 11.Sullivan L, Lee CB, Simonian PT. Simultaneous avulsion fracture of the tibial tubercle with avulsion of the patellar ligament. Am J Knee Surg. 2000;13:156–8. [PubMed] [Google Scholar]
- 12.Swan K, Jr, Rizio L. Combined avulsion fracture of the tibial tubercle and avulsion of the patellar ligament. Orthopedics. 2007;30:571–2. doi: 10.3928/01477447-20070701-05. [DOI] [PubMed] [Google Scholar]
- 13.Uppal R, Lyne ED. Tibial tubercle fracture with avulsion of the patellar ligament:A case report. Am J Orthop (Belle Mead NJ) 2007;36:273–4. [PubMed] [Google Scholar]
- 14.Novacheck TF, Stout JL, Gage JR, Schwartz MH. Distal femoral extension osteotomy and patellar tendon advancement to treat persistent crouch gait in cerebral palsy. Surgical technique. J Bone Joint Surg Am. 2009;91(Suppl2):271–86. doi: 10.2106/JBJS.I.00316. [DOI] [PubMed] [Google Scholar]
- 15.Pandya NK, Edmonds EW, Roocroft JH, Mubarak SJ. Tibial tubercle fractures:Complications, classification, and the need for intra-articular assessment. J Pediatr Orthop. 2012;32:749–59. doi: 10.1097/BPO.0b013e318271bb05. [DOI] [PubMed] [Google Scholar]