

Abstract
Context:
Alpine skiing is a popular sport worldwide but has significant risk for injury. The epidemiology of skiing-related injuries has been described, which has led to the identification of risk factors for specific types of injuries.
Evidence Acquisition:
Pertinent literature from peer-reviewed publications was reviewed.
Study Design:
Clinical review.
Level of Evidence:
Level 5.
Results:
The adoption of international standards for ski-boot-binding systems has changed the profile of skiing-related injuries over time, as has the widespread use of helmets. An understanding of mechanisms of injury, risk factors, and preventative measures may decrease the incidence of skiing-related injuries.
Conclusion:
Advances in standards for skiing equipment have been effective at decreasing both the frequency and severity of skiing-related injuries, but additional efforts are required to improve the safety of the sport.
Keywords: alpine skiing, injury, anterior cruciate ligament (ACL), epidemiology, head injury
During the 2016-2017 ski season in the United States, there were 481 operating ski areas and an estimated 6.8 million active skiers.39,40 Moreover, there are an estimated 200 million active skiers worldwide.20 Participation in skiing, like any sport, carries with it an inherent risk of injury. Alpine skiing injuries are well documented.7-10,20,24,30,51-53,59,63,66,67 There has been considerable work done in classifying the types and severity of skiing-related injuries.7-10,20,24,30,51-53,59,63,66,67 There has been a change in injury patterns since the 1970s, particularly in the lower extremity.27,54 Anterior cruciate ligament (ACL) injuries continue to be very problematic and, unfortunately, have remained quite prevalent over time.25
As injury patterns have been established, risk factors have been identified.6,10,21,22,28,64,66 Efforts have been made to modify these risk factors through injury prevention programs.14 In a 34-year study, as of 2006, a 55% decrease in the overall injury rate was observed.25
The purpose of this review is 3-fold: (1) to describe the epidemiology of skiing injuries, (2) to discuss known risk factors and the relationship between equipment and injury, and (3) to highlight the effectiveness of skiing injury prevention programs and equipment advances and present strategies for reducing the risk of skiing injuries.
Methods
A comprehensive review of the published literature from 1985 to 2018 pertaining to alpine skiing injuries was performed. Pertinent articles were identified from PubMed, Ovid, and Google Scholar using the search terms ski, alpine skiing, injury, and epidemiology. Additional studies, including studies regarding specific skiing injuries, were identified from the references of relevant papers. Studies focused on primarily snowboarding injuries or on alpine ski racing injuries were excluded.
Epidemiology of Alpine Skiing Injuries
Multiple studies on the epidemiology of alpine skiing injuries have been published (Table 1).
Table 1.
Ski injury epidemiology studies
| Study | Year(s) of Study | Country | Sport | No. of Injuries | Mean Age, y | % Male/% Female |
|---|---|---|---|---|---|---|
| Coury et al5 | 1995-2000, 2009-2010 | USA | Skiing | 1196 | 35.4 | 48/52 |
| Patrick et al42 | 1996 | USA | Skiing | 124 | 34 | NR |
| Patrick et al42 | 2013 | USA | Skiing | 112 | 34 | NR |
| Kim et al27 | 1988-2006 | USA | Skiing | 9465 | 30 | 55.5/44.5 |
| Stenroos and Handolin63 | 2006-2012 | Finland | Skiing | 2911 | 24 | 57/43 |
| Langran and Selvaraj29 | 1999-2000 | Scotland | Skiing | 440 | 51.8/48.2 | |
| Sacco et al52 | 1990-1996 | USA | Skiing | 238 | 29 | 66/34 |
| Davidson and Laliotis7 | 1983-1992 | USA | Skiing | 24,340 | 27.9 | 50/50 |
| Rust et al51 | 2006-2008 | USA | Skiing | 811 | 39 | 55.2/44.8 |
| Sulheim et al66 | 2002 | Norway | Skiing | 3277 | 60/40 | |
| Ruedl et al49 | 2010-2011 | Austria | Skiing, snowboarding, telemark | 2326 | 36.2 | 51.3/48.7 |
| Burtscher et al4 | 1997-1998 | Austria | Skiing | 17,914 | 33 | 48/52 |
| Burtscher et al4 | 2002-2003 | Austria | Skiing | 2433 | 32 | 50/50 |
NR, not reported.
Age
Table 1 presents data from studies reporting on a total of 64,667 injuries.4,5,7,27,29,42,49,51,52,63,66 The mean age of injured patients evaluated in these studies ranged from 24 to 35.4 years, with an overall mean age of 30.3 years. In 2 studies,10,74 the populations at greatest risk for injury were children and adolescents and adults older than 50 years; however, in another study,59 there was no greater risk of injury in adults older than 55 years, with the exception of tibial plateau fractures. Because of the varying ways that data on the age of injured patients are presented, it is difficult to draw any conclusions about the effect of age on the overall risk of injury. Moreover, the age of the recreational skiing population is rising,59 further complicating analysis of age and skiing-related injuries.
Sex
Among reported injuries, there was a higher percentage of males injured than females (Table 1). Knee injuries, especially ACL sprains, are more common among females than males,31,54,57,71 while males are more likely to sustain fractures.57 Male sex is associated with greater risk-taking behavior,70 which may lead to a greater number of injuries with greater severity.
Injury Site
Most injuries occur to the lower extremity, with reports ranging from 43% to 77% of all alpine skiing–related injuries.4,7,49,51,52,63,66 This is followed by injuries to the upper extremity, which account for approximately 14% of injuries and primarily involve the thumb and shoulder.4,7,49,51,52,63,66 Head and neck injuries account for 13% of all injuries.4,7,49,51,52,63,66 This data is summarized in Table 2.
Table 2.
Injuries to each region
| Study | Head/Neck Injuries, n (%) | Thorax/Abdomen Injuries, n (%) | Spine Injuries, n (%) | Upper Extremity Injuries, n (%) | Lower Extremity Injuries, n (%) | Total Injuries, n |
|---|---|---|---|---|---|---|
| Sulheim et al66 | 642 (19.6) | 92 (2.8) | 167 (5.1) | 888 (27.1) | 1484 (45.3) | 3277 |
| Stenroos and Handolin63 | 437 (15) | 87 (3) | 146 (5) | 990 (34) | 1252 (43) | 2911 |
| Ruedl et al49 | 288 (12.4) | 56 (2.4) | 67 (2.9) | 637 (27.4) | 1277 (54.9) | 2326 |
| Sacco et al52 | 40 (17) | 43 (18) | 26 (11) | 17 (7) | 183 (77) | 238 |
| Davidson and Laliotis7 | 3894 (16) | 1460 (6) | 730 (3) | 4868 (20) | 12,657 (52) | 24,340 |
| Rust et al51 | 89 (11) | 97 (12) | NR | 251 (31) | 414 (51) | 811 |
| Burtscher et al4 | 1648 (8.1) | 692 (3.4) | NR | NR | 11,130 (54.7) | 20,347 |
| Total | 7038 (13) | 2527 (5) | 1136 (2) | 7651 (14) | 28,397 (52) | 54,250 |
NR, not reported.
Specific locations of injury are summarized in Table 3. The knee is the most common site of injury, with reports ranging from 27% to 41% of all injuries.4,5,7,24,29,42,49,66,67 Reports of the second most common site of injury vary widely between studies. Common sites of injury include the shoulder,4,5,49,67 hand/wrist,42 and the lower leg.7
Table 3.
Most common injury sites and percentage of injuries per study occurring at each site
| Study | First | % | Second | % | Third | % | Fourth | % | Fifth | % |
|---|---|---|---|---|---|---|---|---|---|---|
| Coury et al5 | Knee | 35 | Shoulder | 12 | Thumb | 8 | ||||
| Patrick et al42 | Knee | 27 | Wrist/hand | 20 | Shoulder/arm | 20 | Foot/ankle | 13 | Head | 10 |
| Langran and Selvaraj29 | Knee | 36.7 | Head/face | 14.2 | Ankle/calf | 8.1 | Thumb | 7.1 | Shoulder | 6.9 |
| Davidson and Laliotis7 | Knee | 34 | Leg | 9 | Head | 9 | Shoulder | 8 | Face | 6 |
| Sulheim et al66 | Knee | 27.3 | Head | 17.9 | Shoulder | 11.2 | Lower leg | 8.9 | Hand | 8.8 |
| Ruedl et al49 | Knee | 35.9 | Shoulder | 16.8 | Lower leg | 13 | Head/neck | 12.4 | Arm | 10.3 |
| Burtscher et al4 | Knee | 40.8 | Shoulder/back | 16.3 | Arm | 12.4 | Lower leg | 8.3 | Head | 8.1 |
| Urabe67 | Knee | 16.8 | Shoulder | 12.8 | Lower leg | 10.8 | Ankle | 10.0 | Head | 9.6 |
Injury Type and Severity
The most common type of knee injuries are ligamentous sprains involving the ACL and/or medial collateral ligament (MCL). Other common specific diagnoses include head contusions and concussions, glenohumeral dislocations, and sprains to the wrist and hand. A summary of the most commonly reported diagnoses is presented in Table 4. One limitation of many of the reviewed studies is that the ability to diagnose accurately is limited by the lack of imaging available at mountainside clinics, and it is therefore difficult to obtain a complete understanding of the injury type and severity.
Table 4.
Most common injuries
| Study | Country | n | First | Second | Third | Fourth | Fifth | Sixth |
|---|---|---|---|---|---|---|---|---|
| Coury et al5 | USA | 1196 | Knee ligament sprain/strain | Internal derangement of knee | Wrist and hand sprain/strain | Open wound of scalp/face | Shoulder dislocation | Tibia/fibula fracture |
| Rust et al51 | USA | 811 | ACL tear | Knee sprain | Closed head injury | Shoulder dislocation | Gastrocnemius tear | Tibial plateau fracture |
| Kim et al27 | USA | 9465 | ACL tear | MCL tear | MCP-UCL injury of thumb | Shoulder soft tissue | Leg contusion | Upper body laceration |
| Langran and Selvaraj29 | Scotland | 440 | Knee sprain | Head/face laceration | Tibia/fibula fracture | Thumb sprain | NR | NR |
| Sulheim et al66 | Norway | 3189a | Head contusion | Knee sprain | Wrist fracture | Back contusion | Knee contusion | Head wound |
| Johnson et al24 | USA | 20,045 | Knee sprain | MCP-UCL injury of thumb | Laceration | Soft tissue shoulder injury | Knee contusion | Upper extremity contusion |
ACL, anterior cruciate ligament; MCL, medial collateral ligament; MCP, metacarpophalangeal; NR, not reported; UCL, ulnar collateral ligament.
Only 3189 of 3277 subjects had information available on diagnosis.
Additionally, data have been collected on severe injuries. These injuries were beyond the scope of injuries treated at mountainside clinics and were treated at an emergency department. Data from the National Trauma Data Bank of the United States from 2007 through 2014 identified 1353 patients with severe (defined as Injury Severity Score [ISS] >15) skiing-related injuries in the United States.8 The median age reported was 38 years, and 78.9% of injuries occurred in males. These results were consistent with the results reported by Weber et al69 in their analysis of a trauma database including Germany, Austria, Switzerland, Finland, Slovenia, Belgium, Luxembourg, and the Netherlands. That study reported 174 skiers with major trauma (ISS > 9), with a mean age of 39.2 years and 78.2% of injuries occurring in males. Despite the fact that younger age is associated with increased risk-taking behavior,70 the mean reported age of skiers with severe injuries was higher than the mean reported age of those with mild to moderate injuries.4,5,7,27,29,42,49,51,52,63,66
Risk factors for skiing injuries that have been identified include age, sex, skiing experience level, self-assessed skill level, body mass index, and trail difficulty.2,5,7,42,49,51 However, these risk factors vary widely between studies.
Trends Over Time
With advances in equipment and increased helmet use, the trend has been toward a decreasing number of skiing-related injuries of all types.18,23,25,50,58 However, the number of traumatic fatalities has remained constant.15,61 The types of injuries sustained have changed with time, most notably with a decreased incidence of tibial fractures and an increased incidence of ACL injuries of the knee.23-25,27,62
Specific Injuries
Head and Neck
Brain injuries are the most common severe traumatic injury associated with skiing8,69 and the injury with the highest fatality prevalence.47,72 Disturbances in consciousness or signs of concussion have been reported in 22% to 42% of skiing-related head injuries.15,33 Notably, the incidence of head injuries and of potentially serious head injuries (PSHIs) has decreased with the widespread use of helmets.55 The most frequent cause of head injury is falling, followed by collisions with an object other than the skiing surface, which cause 23.1% to 42.5% of head injuries.15,16
Concussions have been reported as the most common head injury,51 although Coury et al5 reported that open wounds of the scalp and face were the most common. The inclusion of lacerations and open wounds is highly variable among studies.
Upper Extremity
While injuries to the upper extremity are more common in snowboarders than in skiers,27,34 they still make up 14% of skiing injuries (see Table 2). The most common injuries involving the shoulder include rotator cuff injury, anterior glenohumeral dislocations and subluxations, acromioclavicular sprains, proximal humeral fractures, and clavicular fractures.28,35,41 Injuries to the elbow and fractures of the mid- and distal humerus, radius, and ulna are uncommon.2,5,26-28,35,51,66
Injuries to the wrist include fractures and sprains, and injuries to the hand include fractures of the bones of the hand and digits.27,42 By far the most common is injury to the ulnar collateral ligament (UCL) of the thumb metacarpophalangeal joint—commonly known as skier’s thumb (Figure 1).5,27,73 In fact, skier’s thumb may be the most common ski injury, but it is frequently underreported due to the patients’ perception that this injury is not serious.19 Skier’s thumb is most commonly caused by a fall on an outstretched hand with the thumb abducted because the skier still grips the pole as the hand strikes the snow surface.21,46,73 Hard-packed snow or icy conditions aggravate this situation.73 Snowboarders experience this type of injury very infrequently, which implicates poles as the probable cause of this injury among skiers.27
Figure 1.

Skier’s thumb. (a) Radiograph of an avulsion injury, the bony equivalent of an ulnar collateral ligament sprain. (b) The proposed mechanism of skier’s thumb injury is insertion of the thumb into the snow while still grasping the pole.
The most common mechanisms of injury to the shoulder are axial loading and resistance to forced abduction of the humerus and a direct blow to the shoulder.28,35 Direct blows to the shoulder and axial loading are more likely to cause fracture of the clavicle or acromioclavicular sprain.35 Resistance to forced abduction is the most common mechanism of rotator cuff injury, and forced abduction with external rotation is the most common mechanism of anterior shoulder dislocation based on patient description of injury events; however, the exact proportion of injuries caused by these mechanisms is unclear.28 Posterior dislocations of the shoulder are infrequent, accounting for 0.4% of glenohumeral dislocations.41
In a case-control study evaluating 318 humeral fractures over the course of 34 ski seasons, Bissell et al2 reported that helmet use and sex were not risk factors for humeral fractures, while greater skill, increased age, and less frequent falling were all factors associated with the injured population.
Lower Extremity
Injuries of the lower extremity are the most common alpine skiing–related injuries.4,7,49,51,52,63,66 Ligamentous injury to the knee is by far the most common, with either the MCL or ACL described as the most commonly injured ligament, accounting for 10% to 33% of all skiing-related injuries (Table 4).5,27,29,51,66 Additionally, fractures of the tibia are still quite common, accounting for up to 6.4% of injuries (Table 4). More infrequently seen injuries of the lower extremity include partial gastrocnemius tears due to a failure of the binding to release in a forward fall, ankle sprains and fractures, and lacerations caused by the ski edge.
ACL
Between 1992 and 2000, the incidence of grade III ACL sprains increased,24 and while it has since decreased,25 the incidence of ACL injuries remains high, with the incidence reported as 0.23 ACL injuries per thousand skier days.24,25 This rate is comparable with the calculated 0.2 ACL tears per 1000 athlete-exposures (AEs) in female soccer players and higher than the 0.09 ACL tears per 1000 AEs in male soccer players.37 A great deal of research has been dedicated to identifying risk factors for and mechanisms of injury. Risk factors for ACL injury that have been identified include female sex,31,54,71 lower core strength,45 and nondominant leg.49 Moreover, Csapo et al6 demonstrated that exposure to cold decreases the rate of force development of the knee flexor muscles, decreasing the capacity to counter extension and anterior shear, and therefore increasing the risk of ACL injury.
Mechanisms of ACL Injury
While ACL injuries due to collisions with stationary objects or with other skiers do occur, they account for only 2% of ACL injuries.54 While a variety of mechanisms have been described, 3 major noncontact mechanisms have been identified. The valgus-external rotation mechanism has been reported as the most common20,66 and involves a fall forward with the inner edge of the front of the ski catching in the snow. This causes immediate abduction and external rotation of the tibia, generating a valgus force about the knee with the ski acting as a lever to maximize torque.20,66 This mechanism may produce a concomitant MCL sprain.44 In other studies, the “phantom foot” mechanism (Figure 2) has been identified as the most common cause of ACL injury.14 In this mechanism,
“the uphill arm is back and the skier is off balance to the rear with the hips below the knees. The uphill ski is unweighted, with all the weight on the inside edge of the downhill ski tail and the upper body is generally facing the downhill ski.”14
Figure 2.
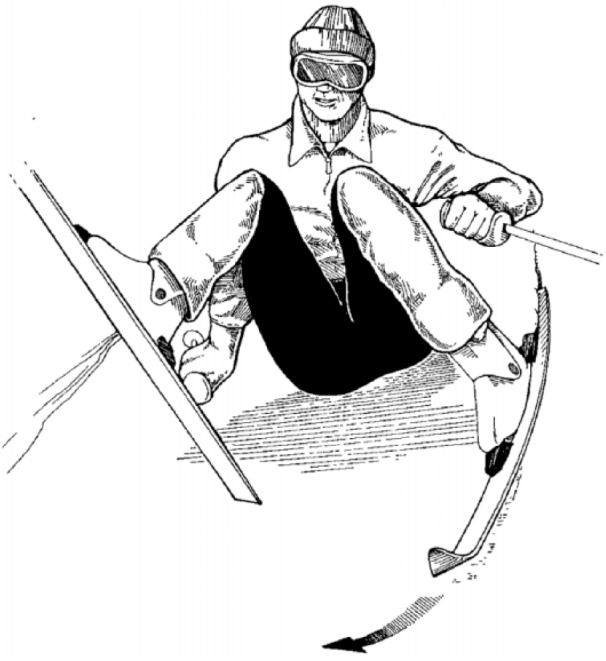
The phantom foot mechanism, reprinted with permission of Johnson et al.22 The phantom foot mechanism occurs when the skier is off-balance posteriorly and all the weight is on the inside edge of the tail of the downhill ski with the uphill ski unweighted. The upper body is facing the downhill ski with the uphill arm back and the hips below the knee. The injury occurs to the downhill leg.
This causes internal rotation of the downhill knee.9,14,20,53 Finally, a boot-induced mechanism has been described and involves an anterior force applied to the tibia by the boot top that occurs while landing from a jump on a fully-extended knee, which results in an anterior translation of the tibia relative to the femur, rupturing the ACL (Figure 3).14,20,36
Figure 3.
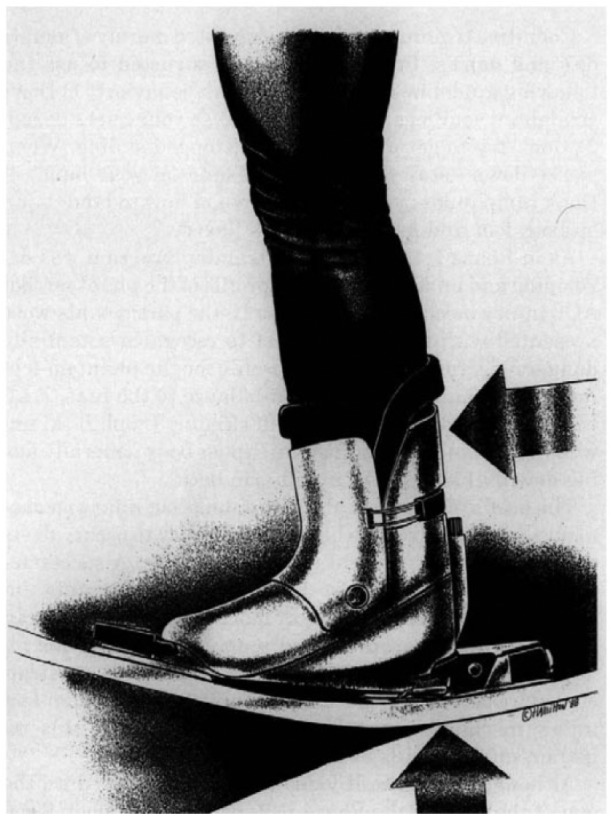
The boot-induced mechanism, reprinted with permission of Johnson et al.22 The boot-induced mechanism occurs when the skier is off-balance posteriorly during a jump and then lands on a fully extended leg. The impact of the landing causes the back of the boot to drive the tibia out from under the femur, causing an anterior cruciate ligament rupture.
Shea et al54 examined the frequency of these mechanisms in a study in which patients selected an option on a survey that most closely described their own injury mechanism. It is important to note that the study design relies on patient recall of the injury event, which is not reliable.32 They found that valgus-external rotation was the most common (32.9%), followed by phantom foot (22.5%), hyperextension (19.0%), boot-induced (7.8%), collision (2.2%), and other (15.6%).54 They also observed an increased risk for the phantom foot mechanism in the 30- to 40-year age group.54
Sex-Based Differences
Data from other sports have shown that females are at increased risk for ACL injury compared with males, and the same has been observed in skiing injuries.31,71 While Shea et al54 did note a significantly greater prevalence of ACL injuries in females than in males, analysis of self-reported mechanisms of injury (including phantom foot, valgus-external rotation, boot-induced, and hyperextension) did not indicate an increased risk for any mechanism of injury between males and females.
Tibial Fractures
Tibial fractures once constituted greater than 20% of all skiing-related injuries, and while the incidence of fractures has decreased after the adoption of International Organization for Standardization (ISO) and ASTM International standard shop practices,4,11,23,24 they are still among the most common injuries to the lower leg. Skiers who are beginners, children, or adolescents are at increased risk for lower leg fractures, with children younger than 10 years having a 9 times greater risk than skiers older than 20 years.12,66 Additionally, Stenroos et al64 conducted a retrospective study of patients presenting to 4 trauma centers in Finland with tibial fractures sustained while skiing. They reported that the most common fracture in adult skiers was a fracture of the tibial shaft (63%), followed by a fracture of the proximal tibia (27%), and a fracture of the distal tibia (10%). They also found that adults were significantly more likely to sustain proximal tibial fractures than children and that the most common mechanism of fracture was a fall on the snow surface.64
Tibial Shaft Fractures
Tibial shaft fractures are the most common type of lower extremity fractures sustained by skiers.64 The frequency of these fractures has significantly decreased with the development of better boots and bindings, as well as the adoption of international standards for equipment and for equipment testing, including standards for ski-boot-binding (SBB) system compatibility.13,23,25 Bindings not releasing during falls has been identified as a major cause of tibial shaft fractures.3
Tibial Plateau Fractures
While tibial shaft fractures are more common, the incidence of tibial plateau fractures is rising.22,43,60 It is hypothesized that this rise in incidence is due to the increasing age of the skiing population, as age is a risk factor for tibial plateau fractures.22,59,60 Additional risk factors include female sex, less frequent falling, and greater self-reported level of experience.22,60 In a study using the AO (Arbeitsgemeinschaft fur Osteosynthesefragen) classification system to analyze 188 patients with proximal tibial fractures, 145 patients had intra-articular involvement, with 96 classified as type B fractures and 49 as type C fractures.43 The risk factors for type C fractures as compared with type A were increased age, greater body mass index, icy snow conditions, higher speed, and greater skiing skill.43
Fatalities
While fatalities due to skiing and snowboard–related accidents are extremely uncommon—it is estimated that just 0.01% of all skiing-related injuries are life-threatening30—approximately 38 fatalities occur each ski season in the United States, equaling 0.67 fatalities per million skier visits.13,58 This rate has remained constant over several decades.61 This report excludes deaths due to medical problems, so all fatalities reported were due to traumatic injury. In a study that did include these fatalities, acute cardiac events accounted for more than half of all deaths.47 Of the fatalities due to injury, brain trauma was the most common cause of death, and the injuries were mostly sustained in males due to a collision with objects other than the snow surface.47,72
Ski Equipment
Helmets
The use of helmets has been widely advocated, and the proportion of skiers wearing helmets has significantly increased in recent years to exceed 80% as of 2017-2018.42,55,65 While many of the injuries prevented by helmet use were minor, such as lacerations and contusions, there is evidence to support the reduction of PSHI with helmet use.55 However, there has been conflicting data surrounding the risk reduction of head injuries with helmet use,1,16,17,65 including widespread concerns that helmet use may lead to an increase in risk-taking behavior48,70 and increased risk of neck injury.50 Russell et al50 performed a meta-analysis of 12 studies analyzing the effect of helmets on head and neck injuries and found that skiers wearing helmets were significantly less likely to sustain a head injury and had no associated increased risk of neck injury. Haider et al18 confirmed these results with a systematic review of helmet use and relation to injury. They found that helmets do reduce prevalence and severity of head injury, with no apparent increase in risky behavior and in neck injury.18
The incidence of fatalities has remained constant even as helmet use has widely increased.56,61 This is likely because the accident scenarios that result in fatality exceed the protective capacity of helmets, and even if fatal head injury is prevented, the skier sustains other injuries capable of causing death.56
Overall, the data indicate that increased helmet use most likely reduces the risk of minor and moderate head injuries and PSHI55 but does not decrease the overall incidence of fatalities.56 There is no indication that there are any adverse effects of widespread helmet use.50
Ski-Boot-Binding Systems
SBB systems have been designed and optimized to protect the tibia and have reduced the incidence of tibial shaft fractures, boot-top contusions, and ankle injuries.13,23,25,62 Advancements in SBB systems in recent decades include the following: reduction of friction in boot to binding interface and boot to ski interface, standardization of SBB interfaces, stiffening of boots at the ankle to limit dorsiflexion and allow the system to transmit loads at the heel, and implementation of ISO standard shop practices that include mandatory inspection and testing of equipment.62 ISO and ASTM standards are similar to each other and exist to ensure optimal equipment function, including binding release. The inappropriate failure of bindings to release has been identified as one of the main causes of skiing-related lower leg injuries. In fact, it has been shown that greater than 75% of equipment associated with lower leg injuries does not meet ISO standards.13 A randomized controlled trial comparing a group of skiers who had their bindings checked and adjusted after standard shop practices with a control group of skiers with no intervention reported a decreased risk of lower extremity equipment-related injuries in the experimental group.19
While advances in SBB systems have succeeded in reducing the incidence of injuries to the lower leg and ankle, these changes were not designed to protect the knee from sprains.13 Therefore, it is possible to experience forces and moments that will result in an ACL injury without causing a normally functioning binding to release.23
Ski Poles
Ski poles may act as a lever to amplify forced abduction of the thumb when the skier’s hand makes contact with the snow surface while grasping the pole during a fall. There is evidence that ski pole grips with an anterior protective bow can prevent the catching of the thumb in the snow in a sudden fall.19 However, these grips are no longer made. Ideally, the skier should discard the pole prior to hitting the ground to avoid a skier’s thumb injury. As stated earlier, thumb UCL injuries are very uncommon in snowboarders.
Injury Prevention
Injury prevention has focused on international standards for SBB systems and the promotion of helmet use. The National Ski Areas Association has been very active in this regard, with campaigns such as “Lids on Kids” and “Heads Up,” as well as local efforts such as “PHAT” (Protect your Head at All Times). These programs have been highly effective, with an increase in helmet use for 14 consecutive years.38 Moreover, an estimated 80% of all skiers and snowboarders and 89% of all minors wore helmets in the 2016-2017 ski season.38
While the majority of injury prevention measures have centered on equipment, injury prevention educational programs have also been implemented in a limited capacity. Vermont Ski Safety Equipment has been promoting ski injury prevention through injury awareness training since 1971. Their website advocates methods for avoiding ACL injury related to both the boot-induced mechanism and the phantom foot mechanism.68 The tips include improved awareness of situations in which the skier is at greater risk for ACL injury and methods for falling safely and for regaining control. This is different from formal ski lessons, which have not been shown to reduce the likelihood of injury.23
The effectiveness of this awareness training was studied in a matched-cohort study of ski-area employees (ski instructors and ski patrollers).14 In this study, employees at 20 ski areas were exposed to an ACL injury awareness training program designed to educate participants on the situations that lead to ACL injury and how to respond appropriately. They reported a 62% decline in severe knee sprains in the group exposed to the injury prevention program, while no decline was observed in the control group of ski area employees who did not receive awareness training at 22 other ski areas.14 This data demonstrates that awareness training is the only proven intervention to reduce the incidence of severe knee injuries, although the participants were ski-area employees and a similar study has not been performed in the general population. More data is necessary to determine the actual effectiveness of awareness training on ACL injury prevention among recreational skiers.
Conclusion
Skiing, while a very popular sport, carries considerable risk for injury. Steps have been taken in recent decades to reduce the risk of injuries, which include advances in standards for equipment and increased education about safe practices. These advances have been effective at decreasing both the frequency and severity of skiing-related injuries, but additional efforts are required to improve the safety of the sport.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
References
- 1. Bergmann KR, Flood A, Kreykes NS, Kharbanda AB. Concussion among youth skiers and snowboarders: a review of the National Trauma Data Bank from 2009 to 2010. Pediatr Emerg Care. 2016;32:9-13. [DOI] [PubMed] [Google Scholar]
- 2. Bissell BT, Johnson RJ, Shafritz AB, Chase DC, Ettlinger CF. Epidemiology and risk factors of humerus fractures among skiers and snowboarders. Am J Sports Med. 2008;36:1880-1888. [DOI] [PubMed] [Google Scholar]
- 3. Bürkner A, Simmen HP. Fractures of the lower extremity in skiing—the influence of ski boots and injury pattern [in German]. Sportverletzung Sportschaden. 2008;22:207-212. [DOI] [PubMed] [Google Scholar]
- 4. Burtscher M, Gatterer H, Flatz M, et al. Effects of modern ski equipment on the overall injury rate and the pattern of injury location in Alpine skiing. Clin J Sport Med. 2008;18:355-357. [DOI] [PubMed] [Google Scholar]
- 5. Coury T, Napoli AM, Wilson M, Daniels J, Murray R, Milzman D. Injury patterns in recreational alpine skiing and snowboarding at a mountainside clinic. Wilderness Environ Med. 2013;24:417-421. [DOI] [PubMed] [Google Scholar]
- 6. Csapo R, Folie R, Hosp S, Hasler M, Nachbauer W. Why do we suffer more ACL injuries in the cold? A pilot study into potential risk factors. Phys Ther Sport. 2017;23:14-21. [DOI] [PubMed] [Google Scholar]
- 7. Davidson TM, Laliotis AT. Alpine skiing injuries. A nine-year study. West J Med. 1996;164:310-314. [PMC free article] [PubMed] [Google Scholar]
- 8. de Roulet A, Inaba K, Strumwasser A, et al. Severe injuries associated with skiing and snowboarding: a national trauma data bank study. J Trauma Acute Care Surg. 2017;82:781-786. [DOI] [PubMed] [Google Scholar]
- 9. Deady LH, Salonen D. Skiing and snowboarding injuries: a review with a focus on mechanism of injury. Radiol Clin North Am. 2010;48:1113-1124. [DOI] [PubMed] [Google Scholar]
- 10. Diebert MC, Aronsson DD, Johnson RJ, Ettlinger CF, Shealy JE. Skiing injuries in children, adolescents, and adults. J Bone Joint Surg Am. 1998;80:25-32. [PubMed] [Google Scholar]
- 11. Eberle R, Heinrich D, Kaps P, Oberguggenberger M, Nachbauer W. Effect of ski boot rear stiffness (SBRS) on maximal ACL force during injury prone landing movements in alpine ski racing: a study with a musculoskeletal simulation model. J Sports Sci. 2017;35:1125-1133. [DOI] [PubMed] [Google Scholar]
- 12. Ekeland A, Holtmoen A, Lystad H. Lower extremity equipment-related injuries in alpine recreational skiers. Am J Sports Med. 1993;21:201-205. [DOI] [PubMed] [Google Scholar]
- 13. Ettlinger CF, Johnson RJ, Shealy JE. Functional and release characteristics of alpine ski equipment. J ASTM Int. 2006;(STP1474):65-74. [Google Scholar]
- 14. Ettlinger CF, Johnson RJ, Shealy JE. A method to help reduce the risk of serious knee sprains incurred in alpine skiing. Am J Sports Med. 1995;23:531-537. [DOI] [PubMed] [Google Scholar]
- 15. Fukuda O, Takaba M, Saito T, Endo S. Head injuries in snowboarders compared with head injuries in skiers. A prospective analysis of 1076 patients from 1994 to 1999 in Niigata, Japan. Am J Sports Med. 2001;29:437-440. [DOI] [PubMed] [Google Scholar]
- 16. Greve MW, Young DJ, Goss AL, Degutis LC. Skiing and snowboarding head injuries in 2 areas of the United States. Wilderness Environ Med. 2009;20:234-238. [DOI] [PubMed] [Google Scholar]
- 17. Hagel BE, Pless IB, Goulet C, Platt RW, Robitaille Y. Effectiveness of helmets in skiers and snowboarders: case-control and case crossover study. BMJ. 2005;330:281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Haider AH, Saleem T, Bilaniuk JW, Barraco RD. An evidence-based review: efficacy of safety helmets in the reduction of head injuries in recreational skiers and snowboarders. J Trauma Acute Care Surg. 2012;73:1340-1347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Hauser W. Experimental prospective skiing injury study. J ASTM Int. 1989; (STP1022):18-24. [Google Scholar]
- 20. Hunter RE. Skiing injuries. Am J Sports Med. 1999;27:381-389. [DOI] [PubMed] [Google Scholar]
- 21. Johnson JW, Culp RW. Acute ulnar collateral ligament injury in the athlete. Hand Clin. 2009;25:437-442. [DOI] [PubMed] [Google Scholar]
- 22. Johnson RJ, Ettlinger CF, Ellowitz AS. Tibial plateau injuries in snow skiing. J ASTM Int. 1996;(STP 1266):295-302. [Google Scholar]
- 23. Johnson RJ, Ettlinger CF, Shealy JE. Myths concerning alpine skiing injuries. Sports Health. 2009;1:486-492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Johnson RJ, Ettlinger CF, Shealy JE. Skier injury trends—1972 to 2012. Paper presented at: Congress of the International Society of Skiing Safety; August 5, 2013; Bariloche, Patagonia, Argentina. [Google Scholar]
- 25. Johnson RJ, Ettlinger CF, Shealy JE. Update on injury trends in alpine skiing. J ASTM Int. 2008;5(6):11-22. [Google Scholar]
- 26. Keramidas E, Miller G. Adult hand injuries on artificial ski slopes. Ann Plast Surg. 2005;55:357-358. [DOI] [PubMed] [Google Scholar]
- 27. Kim S, Endres NK, Johnson RJ, Ettlinger CF, Shealy JE. Snowboarding injuries: trends over time and comparisons with alpine skiing injuries. Am J Sports Med. 2012;40:770-776. [DOI] [PubMed] [Google Scholar]
- 28. Kocher MS, Feagin JA., Jr. Shoulder injuries during alpine skiing. Am J Sports Med. 1996;24:665-669. [DOI] [PubMed] [Google Scholar]
- 29. Langran M, Selvaraj S. Snow sports injuries in Scotland: a case-control study. Br J Sports Med. 2002;36(2):135-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Laporte JD, Bajolle L, Lamy D, Delay JB. Winter sports injuries in France over two decades. J ASTM Int. 2012;19(STP1553):201-215. [Google Scholar]
- 31. Lefevre N, Bohu Y, Klouche S, Lecocq J, Herman S. Anterior cruciate ligament tear during the menstrual cycle in female recreational skiers. Orthop Traumatol Surg Res. 2013;99:571-575. [DOI] [PubMed] [Google Scholar]
- 32. Lovalekar M, Abt JP, Sell TC, Lephart SM, Pletcher E, Beals K. Accuracy of recall of musculoskeletal injuries in elite military personnel: a cross-sectional study. BMJ Open. 2017;7:e017434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Macnab AJ, Cadman R. Demographics of alpine skiing and snowboarding injury: lessons for prevention programs. Inj Prev. 1996;2:286-289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Matsumoto K, Miyamoto K, Sumi H, Sumi Y, Shimizu K. Upper extremity injuries in snowboarding and skiing: a comparative study. Clin J Sport Med. 2002;12:354-359. [DOI] [PubMed] [Google Scholar]
- 35. McCall D, Safran MR. Injuries about the shoulder in skiing and snowboarding. Br J Sports Med. 2009;43:987-992. [DOI] [PubMed] [Google Scholar]
- 36. McConkey JP. Anterior cruciate ligament rupture in skiing. A new mechanism of injury. Am J Sports Med. 1986;14:160-164. [DOI] [PubMed] [Google Scholar]
- 37. Montalvo AM, Schneider DK, Silva PL, et al. What’s my risk of sustaining an ACL injury while playing football (soccer)? A systematic review with meta-analysis [published online March 29, 2018]. Br J Sports Med. doi: 10.1136/bjsports-2016-097261 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. National Ski Areas Association. Helmet Usage and Safety Fact Sheet. Lakewood, CO: National Ski Areas Association; 2017. [Google Scholar]
- 39. National Ski Areas Association. Number of Active U.S. Participants Overall by Equipment Type: 1996/97 to 2016/17. Lakewood, CO: National Ski Areas Association; 2017. [Google Scholar]
- 40. National Ski Areas Association. U.S. Ski Resorts in Operation During 2016/17 Season. Lakewood, CO: National Ski Areas Association; 2017. [Google Scholar]
- 41. Ogawa H, Sumi H, Sumi Y, Shimizu K. Glenohumeral dislocations in snowboarding and skiing. Injury. 2011;42:1241-1247. [DOI] [PubMed] [Google Scholar]
- 42. Patrick E, Cooper JG, Daniels J. Changes in skiing and snowboarding injury epidemiology and attitudes to safety in Big Sky, Montana, USA: a comparison of 2 cross-sectional studies in 1996 and 2013. Orthop J Sports Med. 2015;3:2325967115588280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Patzold R, Spiegl U, Wurster M, et al. Proximal tibial fractures sustained during alpine skiing—incidence and risk factors [in German]. Sportverletzung Sportschaden. 2013;27:207-211. [DOI] [PubMed] [Google Scholar]
- 44. Pressman A, Johnson DH. A review of ski injuries resulting in combined injury to the anterior cruciate ligament and medial collateral ligaments. Arthroscopy. 2003;19:194-202. [DOI] [PubMed] [Google Scholar]
- 45. Raschner C, Platzer HP, Patterson C, Werner I, Huber R, Hildebrandt C. The relationship between ACL injuries and physical fitness in young competitive ski racers: a 10-year longitudinal study. Br J Sports Med. 2012;46:1065-1071. [DOI] [PubMed] [Google Scholar]
- 46. Ritting AW, Baldwin PC, Rodner CM. Ulnar collateral ligament injury of the thumb metacarpophalangeal joint. Clin J Sport Med. 2010;20:106-112. [DOI] [PubMed] [Google Scholar]
- 47. Ruedl G, Bilek H, Ebner H, Gabl K, Kopp M, Burtscher M. Fatalities on Austrian ski slopes during a 5-year period. Wilderness Environ Med. 2011;22:326-328. [DOI] [PubMed] [Google Scholar]
- 48. Ruedl G, Burtscher M, Wolf M, et al. Are self-reported risk-taking behavior and helmet use associated with injury causes among skiers and snowboarders? Scand J Med Sci Sports. 2015;25:125-130. [DOI] [PubMed] [Google Scholar]
- 49. Ruedl G, Kopp M, Sommersacher R, Woldrich T, Burtscher M. Factors associated with injuries occurred on slope intersections and in snow parks compared to on-slope injuries. Accid Anal Prev. 2013;50:1221-1225. [DOI] [PubMed] [Google Scholar]
- 50. Russell K, Christie J, Hagel BE. The effect of helmets on the risk of head and neck injuries among skiers and snowboarders: a meta-analysis. CMAJ. 2010;182:333-340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Rust DA, Gilmore CJ, Treme G. Injury patterns at a large Western United States ski resort with and without snowboarders: the Taos experience. Am J Sports Med. 2013;41:652-656. [DOI] [PubMed] [Google Scholar]
- 52. Sacco DE, Sartorelli DH, Vane DW. Evaluation of alpine skiing and snowboarding injury in a northeastern state. J Trauma. 1998;44:654-659. [DOI] [PubMed] [Google Scholar]
- 53. Schneider T. Snow skiing injuries. Aust Fam Physician. 2003;32:499-502. [PubMed] [Google Scholar]
- 54. Shea KG, Archibald-Seiffer N, Murdock E, et al. Knee injuries in downhill skiers: a 6-year survey study. Orthop J Sports Med. 2014;2:2325967113519741. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55. Shealy JE, Johnson RJ, Ettlinger CF, Scher IS. Role of helmets in mitigation of head injuries: epidemiologic study of head injuries to skiers. In: Johnson RJ, Shealy JE, Greenwald RM. eds. Skiing Trauma and Safety: 20th Volume. Conshohocken, PA: ASTM International; 2015:22-38. [Google Scholar]
- 56. Shealy JE, Johnson RJ, Ettlinger CF. Do helmets reduce fatalities or merely alter the patterns of death? J ASTM Int. 2008;5(6). [Google Scholar]
- 57. Shealy JE, Ettlinger CF. Gender related injury patterns in snow skiing. J ASTM Int. 1996;(STP1266):45-57. [Google Scholar]
- 58. Shealy JE, Ettlinger CF, Johnson RJ. 2010/2011 NSAA 10-year interval injury study. J ASTM Int. 2013;(STP1582):93-111. [Google Scholar]
- 59. Shealy JE, Ettlinger CF, Johnson RJ. Aging trends in alpine skiing. J ASTM Int. 2011;7(4):130-138. [Google Scholar]
- 60. Shealy JE, Ettlinger CF, Johnson RJ. Femur and tibial plateau fractures in alpine skiing. J ASTM Int. 2003;(STP1440):140-148. [Google Scholar]
- 61. Shealy JE, Ettlinger CF, Johnson RJ. On-piste fatalities in recreational snow sports in the U.S. J ASTM Int. 2006;(STP1474):27-34. [Google Scholar]
- 62. Shealy JE, Ettlinger CF, Johnson RJ. What do we know about ski injury research that relates binding function to knee and lower leg injuries? J ASTM Int. 2003;(STP1440):36-52. [Google Scholar]
- 63. Stenroos A, Handolin L. Incidence of recreational alpine skiing and snowboarding injuries: six years’ experience in the largest ski resort in Finland. Scand J Surg. 2015;104:127-131. [DOI] [PubMed] [Google Scholar]
- 64. Stenroos A, Pakarinen H, Jalkanen J, Malkia T, Handolin L. Tibial fractures in alpine skiing and snowboarding in Finland: a retrospective study on fracture types and injury mechanisms in 363 patients. Scand J Surg. 2016;105:191-196. [DOI] [PubMed] [Google Scholar]
- 65. Sulheim S, Ekeland A, Holme I, Bahr R. Helmet use and risk of head injuries in alpine skiers and snowboarders: changes after an interval of one decade. Br J Sports Med. 2017;51:44-50. [DOI] [PubMed] [Google Scholar]
- 66. Sulheim S, Holme I, Rodven A, Ekeland A, Bahr R. Risk factors for injuries in alpine skiing, telemark skiing and snowboarding—case-control study. Br J Sports Med. 2011;45:1303-1309. [DOI] [PubMed] [Google Scholar]
- 67. Urabe Y. Injury trends in the past 5 years at a skiing area in western Japan. J ASTM Int. 2013;(STP1582):112-121. [Google Scholar]
- 68. Vermont Ski Safety. Tips for knee-friendly skiing. 2018. https://vermontskisafety.com/research/tips/. Accessed June 26, 2018.
- 69. Weber CD, Horst K, Lefering R, Hofman M, Dienstknecht T, Pape HC. Major trauma in winter sports: an international trauma database analysis. Eur J Trauma Emerg Surg. 2016;42:741-747. [DOI] [PubMed] [Google Scholar]
- 70. Willick SE, Wagner G, Ericson D, Josten G, Teramoto M, Davis J. Helmet use and risk-taking behavior among skiers and snowboarders [published online October 10, 2017]. Clin J Sports Med. doi: 10.1097/JSM.0000000000000527 [DOI] [PubMed] [Google Scholar]
- 71. Wojtys EM, Huston LJ, Lindenfeld TN, Hewett TE, Greenfield ML. Association between the menstrual cycle and anterior cruciate ligament injuries in female athletes. Am J Sports Med. 1998;26:614-619. [DOI] [PubMed] [Google Scholar]
- 72. Xiang H, Stallones L. Deaths associated with snow skiing in Colorado 1980-1981 to 2000-2001 ski seasons. Injury. 2003;34:892-896. [DOI] [PubMed] [Google Scholar]
- 73. Young LR, Crane HD. Thumbs up: the changing pattern of ski injuries. J ASTM Int. 1985;(STP860):382-394. [Google Scholar]
- 74. Zacharopoulos A, Smyrnis A, Vlastos I, Zafeiriou C. Skiing injuries in Greece: a six years case-control study (2007-2013). J ASTM Int. 2015;(STP1582):122-140. [Google Scholar]