

Abstract
Background: The extensor digiti minimi (EDM) tendon is commonly divided into a radial slip (EDM-R) and an ulnar slip (EDM-U). To our knowledge, the degree to which each EDM slip concomitantly abducts the small finger with active extension has not been formally tested. This study sought to characterize the comparative contributions of finger abduction inherent to each slip of the EDM to observe the sequelae of active small finger extension following transfer of the contralateral slip. Methods: Eighteen fresh-frozen cadaveric hands were used in this study. Starting with the hand in resting position, a controlled traction of 10 N was applied to each slip of the EDM tendon. The range of small finger abduction with respect to the fixed ring finger was recorded utilizing infrared reflective markers tracked through the range of motion using a digital video camera. Results: The mean abduction of the small finger when the radial slip of the EDM tendon was tested was 13.33° (95% confidence interval [CI]: 10.10°-16.55°), which was significantly different (P ≤ .001) than small finger abduction produced by the ulnar slip of the EDM, with a mean of 23.72° (95% CI: 19.40°-28.04°). Conclusions: Given the fact that the ulnar slip of the EDM tendon is shown to be the major contributor of aberrant abduction with active small finger extension, as traction on this slip produces almost twice as much abduction as the radial slip, the EDM-U is the ideal donor graft with respect to tendon transfers of the EDM.
Keywords: EDM, EDM-R, EDM-U, EDM slip, Wartenberg sign, EDM tendon transfer, small finger abduction, radial slip, ulnar slip
Introduction
The Wartenberg sign is classically described as an abduction deformity of the small finger that occurs in the setting of ulnar neuropathy, wherein the radially innervated extrinsic extensors act unopposed to the hand intrinsics.16,17 The abducted position of the extended small finger can impede simple daily tasks that require moving the hand in confined spaces, as through the sleeves of a shirt or coat, when donning gloves, or reaching into a pocket.2,4,14
This persistent abduction of the fifth digit is present only during active finger extension, as the insertion and expansions of the extensor digiti minimi (EDM) lay ulnar to the longitudinal axis of the metacarpophalangeal (MCP) joint.2,15 With functional hand intrinsics, this abduction force is counteracted by the active contraction of the third palmar interosseous muscle.15
Prior descriptive anatomical studies have demonstrated that the vast majority of EDM tendons (75%-84%) are duplicated, presenting as 2 slips: 1 radial (EDM-R) and 1 ulnar (EDM-U).7,18 A number of different operations have been proposed to treat ulnar nerve palsy abduction deformities of the little finger via these 2 slips. Blacker et al described 2 techniques in which the ulnar slip of the EDM tendon is transposed radially: In the Fowler-Brooks transfer, the EDM-U is transferred to the volar radial flexor sheath, whereas in the other technique, it is transferred into the radial collateral ligament of the fifth MCP joint.2,3,5 Dellon described a modification to the latter procedure, wherein the EDM-U is transposed to the radial side of the extensor hood.4 van Aaken adapted a technique first proposed by Bellan et al, which transposed both slips of the EDM tendons to the radial aspect of the extensor hood.1,14 All these authors demonstrated successful clinical outcomes by correcting Wartenberg sign through radialization of the EDM slip(s) at the MCP joint.
To date, an important clinical implication of the relative contributions of the EDM-U and EDM-R that has not received as much recognition is the redundancy of small finger extension within the EDM extensor mechanism, making it an attractive option for tendon transfer. However, the extent to which the EDM-R and the EDM-U contribute to small finger abduction has not been formally tested. A deeper understanding of the extent to which sole contribution of each slip of the EDM extensor mechanism produces superfluous small finger abduction has major implications in the utilization of the EDM mechanism for tendon transfers. Therefore, this biomechanical study aims to characterize the relative contributions of each EDM slip to small finger abduction.
Materials and Methods
Eighteen fresh-frozen cadaveric hands were obtained from adult donors (ages 18-80) of both genders. Specimens from donors with structural deformities of the hand, or medical history of systemic conditions (eg, rheumatoid arthritis, gout) that could potentially confound biomechanical testing, were excluded. The 2 slips of the EDM tendon were identified (Figure 1) and separated within its connective tissue sheath following meticulous superficial dissection. Starting with the hand in resting position, a controlled traction of 10 N was applied to each slip through a 2-0 vicryl suture with the trajectory of the tension directed midline along the shaft of the fifth metacarpal. Reflective markers were placed at the distal phalanx of the ring finger and at the fourth web space as reference points for determining angular displacement during small finger abduction. A third marker was also placed at the distal phalanx of the small finger to measure abduction from the hand; 1.6-mm Kirschner wires were used to transfix the distal phalanges of the index and ring fingers to keep the hand fixed in place. The testing apparatus is demonstrated in Figure 2.
Figure 1.
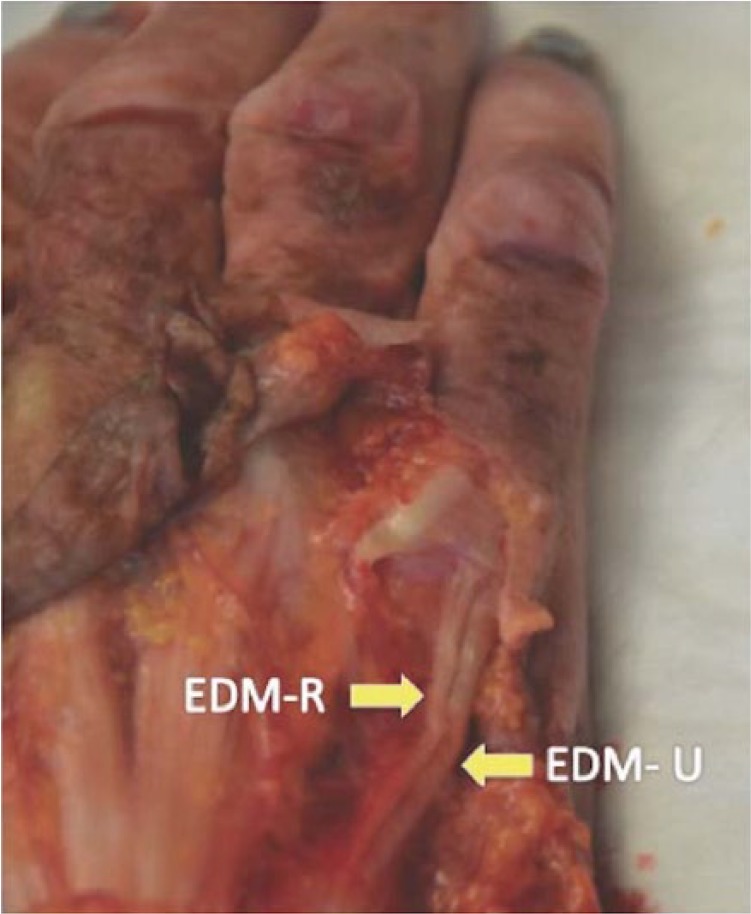
The 2 slips of the extensor digiti minimi tendon.
Note. EDM-U = extensor digiti minimi-ulnar; EDM-R = extensor digiti minimi-radial.
Figure 2.

Testing apparatus that facilitated duplicate tensioning of extensor digiti minimi-radial versus extensor digiti minimi-ulnar.
The range of small finger abduction with respect to the fixed ring finger was tracked using a 1.3-MP digital camera equipped with an infrared LED array (Hamswan, Shenzhen, China) fitted with an internal filter to reduce visible spectrum light transmission to the image sensor. The resultant footage was then analyzed with video analysis software to determine the range and maximum angle of small finger abduction. The degree of small finger extension was not examined in this study.
Infrared footage was imported into the Fiji software package running ImageJ version 1.49m12,13 to determine the range and maximum angle of small finger abduction for each of the 2 conditions. Mean values for angular displacement were generated for each condition along with ranges, standard deviations, and 95% confidence intervals.
Results
All 18 of the tested specimens had 2 slips of the EDM tendon. Eight of the specimens had an extensor digitorum communis to the small finger (EDC-V), while the small fingers in the other 10 hands solely possessed the junctura tendinum from the EDC. As shown in Table 1, the mean abduction of the small finger when the EDM-U was tensioned was 23.72° (95% confidence interval [CI]: 19.40°-28.04°), which was significantly greater (P ≤ .001) than the abduction produced by tensioning the EDM-R of 13.33° (95% CI: 10.10°-16.55°). Figure 3 depicts the measurements recorded from the cadaveric hand with the most extreme difference in small finger abduction between the EDM-R and the EDM-U.
Table 1.
Small Finger Abduction With Respect to EDM Slip.
| EDM slip | Mean small finger abduction | EDM slip vs baseline abduction | EDM-U vs EDM-R abduction |
|---|---|---|---|
| EDM-U | 23.72° | P ≤ .001 | P ≤ .001 |
| EDM-R | 13.33° | P ≤ .001 |
Note. EDM = extensor digiti minimi; EDM-U = extensor digiti minimi-ulnar; EDM-R = extensor digiti minimi-radial.
Figure 3.

Exemplar of the 3 comparative measurements of small finger abduction within the same cadaveric specimen.
Note. EDC-V = extensor digitorum communis to the small finger; EDM = extensor digiti minimi.
Discussion
Wartenberg sign can result from ulnar nerve palsy, traumatic avulsion of the third palmar interosseous, contracture of the hypothenar musculature, a lax palmar plate, and rheumatoid arthritis.6,9,10,14,18 Regardless of the etiology, radialization of the EDM tendon to the extensor hood has repeatedly been shown to correct this abduction deformity.1,2,4,14 More specifically, the EDM-U is the workhorse of this transposition, as this branch of the EDM tendon is believed to be the principal causative force of the abduction deformity.2,4,8 Blacker et al accounted for this finding with the observation that the EDM-U runs ulnar to the metacarpal head and thus contributes to ulnar deviation of the small finger. Furthermore, it was demonstrated that this branch of the EDM tendon inserts on the abductor digiti minimi and, as a result, indirectly potentiates the abducting force.2
This study offers a biomechanical model that supports the notion that the EDM-U plays a more appreciable role in aberrant small finger abduction with active extension than that of the EDM-R tendon. The difference in measured small finger abduction was almost 2-fold higher in EDM-U, suggesting that isolated tendon transfer of the EDM-R tendon has a greater potential to cause iatrogenic Wartenberg sign. Conversely, isolated EDM-U tendon transfer would, in effect, radialize small finger extensor contribution, thus mitigating any unwanted small finger abduction.
Interestingly, the cadaveric hands in our series all possessed 2 slips of the EDM tendon, which has been found to be the most common variant, followed by single slips, and then triple slip EDM’s.18 Also, only 44% of hands in this study had a dedicated EDC-V; this corresponded to the frequency of this tendon morphology reported by other cadaveric studies.7,11 This variation in tendon anatomy has major implications in that a tendon transfer of the entire EDM tendon away from the fifth digit would be imprudent in hands in which both the EDC-V and junctura are absent.7
The scope of this study is limited in that only one plane of motion of the small finger was examined. There was no comparison of small finger extension between the 2 slips, which is the primary action of this complex. Such measurements could be very informative, particularly in the setting of tendon transfers, to determine whether there is also a significant difference of small finger extension between the EDM slips. Furthermore, while the ~10° difference in angular small finger abduction between the EDM-U and EDM-R was found to be statistically significant, this finding may not yield any clinical significance or functional deficit, as seen in Wartenberg sign. However, any amount of unwarranted small finger abduction following tendon transfer should be avoided, if possible; thus, we believe this contrast is still worth reporting.
This study illustrates the predominant role of the EDM-U in aberrant small finger abduction with active extension. Refined understanding of the role of this tendon has important implications, especially when considering tendon transfers to limit extraneous small finger abduction with active extension. This study supports the notion that tendon transfer of the EDM-U, rather than the EDM-R, is more likely to mitigate unwanted abduction of the small finger.
Footnotes
Ethical Approval: This study was approved by our institutional review board.
Statement of Human and Animal Rights: All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. This was a cadaveric study, in which the cadavers were obtained from a licensed tissue bank. There was no identifying information included in this article. There were no animal subjects in this study.
Statement of Informed Consent: Informed consent was not needed as this was a cadaveric study. The cadavers were obtained from a licensed tissue bank.
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Bellan N, Belkhiria F, Touam C, et al. Extensor digiti minimi tendon “rerouting” transfer in permanent abduction of the little finger. Chir Main. 1998;17(4):325-333. [DOI] [PubMed] [Google Scholar]
- 2. Blacker GJ, Lister GD, Kleinert HE. The abducted little finger in low ulnar nerve palsy. J Hand Surg Am. 1976;1(3):190-196. [DOI] [PubMed] [Google Scholar]
- 3. Brooks AL, Jones DS. A new intrinsic tendon transfer for the paralytic hand. J Bone Joint Surg Am. 1975;57:730. [Google Scholar]
- 4. Dellon AL. Extensor digiti minimi tendon transfer to correct abducted small finger in ulnar dysfunction. J Hand Surg Am. 1991;16(5):819-823. [DOI] [PubMed] [Google Scholar]
- 5. Fowler B. Extensor apparatus of the digits. J Bone Joint Surg Br. 1949;31:749. [Google Scholar]
- 6. Freeland AE, Barrett GR, Wheeless GS. Correction of abduction: deformity of the small finger caused by avulsion of the insertion of the third volar interosseous muscle. Am J Sports Med. 1985;13:273-276. [DOI] [PubMed] [Google Scholar]
- 7. Gonzalez MH, Gray T, Ortinau E, et al. The extensor tendons to the little finger: an anatomic study. J Hand Surg Am. 1995;20:844-847. [DOI] [PubMed] [Google Scholar]
- 8. Gottschalk HP, Bindra RR. Late reconstruction of ulnar nerve palsy. Orthop Clin North Am. 2012;43(4):495-507. [DOI] [PubMed] [Google Scholar]
- 9. Kilgus M, Burg D, Loss M, et al. Wartenberg’s sign of ulnar nerve lesion. A contribution to pathophysiology and to the differential diagnosis. Handchir Mikrochir Plast Chir. 2003;35(4):251-258. [DOI] [PubMed] [Google Scholar]
- 10. Lourie GM, Lundy DW, Rudolph HP, et al. Abducted, hyperextended small finger deformity of nonneurologic etiology. J Hand Surg Am. 1999;24(2):315-319. [DOI] [PubMed] [Google Scholar]
- 11. Schenck RR. Variations of the extensor tendons of the fingers: surgical significance. J Bone Joint Surg Am. 1964;46:103-110. [PubMed] [Google Scholar]
- 12. Schindelin J, Arganda-Carreras I, Frise E, et al. Fiji: an open-source platform for biological-image analysis. Nat Methods. 2012;9(7):676-682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Schneider CA, Rasband WS, Eliceiri KW. NIH image to ImageJ: 25 years of image analysis. Nat Methods. 2012;9(7):671-675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. van Aaken J, Zhu J, Fasel JH, et al. Investigation of radialization and rerouting of the extensor digiti minimi (EDM) in the abduction deformity of the little finger: a cadaver study. Hand (N Y). 2011;6(2):202-205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Voche P, Merle M. Wartenberg’s sign. A new method of surgical correction. J Hand Surg Br. 1995;20:49-52. [DOI] [PubMed] [Google Scholar]
- 16. Wartenberg R. A sign of ulnar nerve palsy. JAMA. 1939;112:1688. [Google Scholar]
- 17. Wartenberg R. Kleine Hilfsmittel der neurologischen Diagnostik. Nervenarzt. 1930;3:594-596. [Google Scholar]
- 18. Yammine K. The prevalence of the extensor digiti minimi tendon of the hand and its variants in humans: a systematic review and meta-analysis. Anat Sci Int. 2015;90(1):40-46. [DOI] [PubMed] [Google Scholar]