

Abstract
Patent foramen ovale (PFO) is a congenital abnormality present in 25%–30% of healthy adults and rarely leads to any sequelae. 1 2 It is associated with a left-to-right shunt which usually does not lead to any haemodynamic compromise. Occasionally, the shunt can get reversed; that is, right-to-left shunt occurs due to worsening pulmonary hypertension and can lead to persistent hypoxia. It is rare for the shunt reversal to happen in the absence of pulmonary hypertension. Here, we present an exceedingly rare case in a 61-year-old man presenting with hypoxia, was found to have shunt reversal due to unilateral diaphragmatic paralysis. He was successfully treated with PFO closure. The purpose of this report is to consider rare possibilities of PFO shunt reversal when the right-sided heart pressure is normal and to highlight that a simple chest X-ray can be a clue to the diagnosis.
Keywords: cardiovascular medicine, interventional cardiology
Background
Unilateral diaphragmatic paralysis (UDP) is an uncommon condition found incidentally on chest X-rays done for other reasons.3 Similarly, patent foramen ovale (PFO) has no long-term detrimental effects on the body, but UDP and PFO can lead to interesting phenomena when they occur together. Distortion of the normal anatomy due to diaphragmatic paralysis can lead to right-to-left shunt (RLS) without reversal of the pressure gradient. Resulting intracardiac shunt causes severe hypoxia resistant to oxygen therapy. The diagnosis is difficult to reach due to the rarity of this condition and low index of suspicion. We are presenting a case of persistent hypoxia due to RLS due to idiopathic diaphragmatic paralysis in the absence of elevated right-sided cardiac pressure.
Case presentation
A 61-year-old otherwise healthy man was referred to the emergency room (ER) by his primary care physician (PCP) for worsening shortness of breath and hypoxia. Dyspnoea started 6 weeks before presentation and was progressive. Initially, he noticed it with exertion and later even while resting. He denied any fevers, chills, cough, sick contacts, recent travel, chest pain, palpitations, orthopnoea, paroxysmal nocturnal dyspnoea or leg swelling. He was a former smoker, smoked one to two packs a day for 10 years and quit about 30 years ago. He had alcohol abuse history in the past but had been sober for the last 2 years. He denied any illicit drug use. Medical history was significant for depression, sleep apnoea for which he underwent uvulopalatopharyngoplasty and a mechanical fall about 1 year ago.
At his PCP office, he was in moderate respiratory distress and was hypoxic with oxygen saturation in low 80s and was referred to ER of another hospital. His vitals in the ER included a temperature of 98°F, heart rate 88 beats/min, respiratory rate of 23/min and oxygen saturation (PO2) of 85% on a 6 L nasal cannula. His physical examination showed moderate respiratory distress; otherwise, respiratory examination was negative for wheezes/ronchi/crackles. Cardiovascular examination was negative for any cardiac murmurs; the rest of the examinations were unremarkable.
Investigations
Laboratory evaluation including complete blood count and metabolic profile was unremarkable. D-dimer was 464 ng/mL (n<230 ng/mL). His ECG was unremarkable. CT chest with pulmonary embolism (PE) protocol was negative for PE but showed elevated right hemidiaphragm with right lower and middle lobe atelectasis. Chest X-ray also showed elevated right hemidiaphragm (figure 1). Non-specific left upper lobe and peripheral interstitial opacities were also seen.
Figure 1.

Chest X-ray showing elevated right hemidiaphragm.
He was initially treated as pneumonitis and atypical infection with levofloxacin and steroids. Virus respiratory panel including influenza/parainfluenza, adenovirus and respiratory syncytial viruses were negative. Due to lack of improvement and significant oxygen requirement, he was transitioned back and forth between BiPAP and high flow nasal cannula with 100% FiO2, and antibiotics were broadened to include vancomycin and cefepime.
At this point, an echocardiogram (ECHO) was done to rule out cardiac causes of hypoxia which showed a possible intracardiac shunt. On the fifth postadmission day, he was transferred to our hospital for further evaluation.
A repeat transthoracic echo (TTE) with bubble study showed the significant passage of bubbles from right to left atrium signifying a PFO, and normal (55%–60%) ejection fraction (figure 2). The patient still required 100% FiO2 on Bilevel Positive Airway Pressure (BiPAP) to keep his saturation above 90%. He was electively intubated for transoesophageal echo (TOE) which showed a large PFO with significant RLS and the absence of an atrial septal defect or clot in the right atrium while Doppler studies showed a flow through the PFO (figure 3). Both TEE and TOE did not show any findings suggestive of raised pulmonary or right-sided heart pressures. Right and left ventricles size and function were normal. Antibiotics and steroids were discontinued as the patient remained afebrile during this time; all his viral, fungal and bacterial serologies were negative, and interstitial infiltrates were vague and not significant enough to explain this degree of hypoxaemia. This prompted us to perform a more specific test that is right heart catheterisation (RHC) to evaluate the intracardiac pressures, which showed mean left atrial pressure of 7 mm Hg and mean right atrial pressure of 4 mm Hg. Pulmonary capillary wedge pressure was 5 mm Hg and mean pulmonary artery pressure was 14 mm Hg which ruled out pulmonary hypertension as the cause of the RLS. During the RHC, intracardiac echo (ICE) was done which confirmed the presence of PFO and the three-dimensional images showing the size measured about 12 mm (figure 4).
Figure 2.

Transoesophageal echo showing a tunnel-shaped patent foramen ovale.
Figure 3.
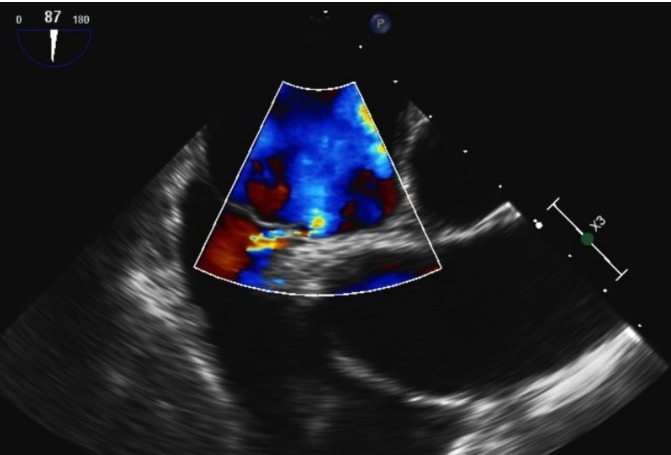
Doppler flow through the patent foramen ovale.
Figure 4.

Three-dimensional view of patent foramen ovale.
Treatment
A 12 mm occluder device was placed in and follow-up imaging with ICE showed no residual shunt.
Outcome and follow-up
Follow-up TTE after the procedure showed well-seated atrial septal occluder (ASO) device with no evidence of PFO. Patient’s oxygen requirement decreased radically after the procedure, and he was extubated the next day. He was weaned down to room air the same day and was transferred to the general medical floor. He did well post procedure and was discharged 3 days later. At his follow-up clinical appointment after a month, he was doing well doing his usual activities without any respiratory distress.
Discussion
Hypoxaemia is defined as the reduced PO2 in the blood while hypoxia means reduced tissue oxygenation. Most common causes of hypoxaemia include hypoventilation, for example, opioid overdose, ventilation-perfusion (V/Q) mismatch, for example, PE, decreased inspired oxygen tension, for example, high altitude, diffusion impairment, for example, pulmonary fibrosis and RLS. All of the causes mentioned above for hypoxaemia improve with supplemental oxygen, at least to some extent except RLS. RLS should always be a consideration when there is virtually no response to supplemental oxygen therapy.4
RLS can also be defined as the extreme form of V/Q mismatch as there is no perfusion in the presence of normal ventilation. RLS exists when blood from the right side of heart bypasses the standard circuitry and reaches the left side of the heart without getting oxygenated. RLS can be anatomical or physiological. The most common anatomical intracardiac cause of RLS is PFO.3 5 PFO is asymptomatic in most conditions as the defect is flap like and the left atrial pressure is 5–10 mm Hg higher than the right atrium, and the atrial septum is essentially closed.
RLS in PFO can occur in the presence of elevated right-sided cardiac pressure such as in severe pulmonary hypertension due to obstructive sleep apnoea, PE and chronic lung diseases. Interestingly, RLS in PFO can also occur in scuba divers possibly due to the reversal of pressure differential between the left and right atrium. Although causation is still debated, PFO has been associated with cryptogenic ischaemic stroke, migraine and fat embolism. RLS through PFO can result in hypoxia resistant to oxygenation due to venous admixture in the left atrium. RLS through PFO in the absence of elevated right-sided cardiac pressure has been previously reported due to right pneumonectomy, aortic root enlargement, abdominal surgery but very rarely with diaphragmatic paralysis.6–8
We did a comprehensive literature search and found only 12 cases reported previously with UDP associated RLS via PFO. The characteristics of these studies are shown in table 1. All of these patients were above the age of 50, and 8/12 (66%) patients were above the age of 60 indicating that PFO by itself is benign and it is the diaphragm paralysis later in life which triggers the hypoxia. Although the duration of hypoxia or dyspnoea was not mentioned in all cases, where it was said it was present for at least a few weeks duration. Precipitating cause for UDP in most cases was unknown (idiopathic UDP); however, in some cases, the definite reason was coronary artery bypass graft surgery, hepatic metastasis or arthrodesis of the lumbar spine. All these patients had normal right-sided heart pressures and successful recovery with the intervention.
Table 1.
Previously reported cases of unilateral hemidiaphragm paralysis-induced right-to-left shunt
| No | Reference | Age/sex | Presentation and duration | Precipitating cause | CT to r/o PE | RHC | Intervention and result |
| 1 | Fabris et al, 12 | 66/F | Refractory hypoxaemia for weeks | Idiopathic unilateral phrenic nerve palsy | No PE | MRAP: 3 MPP: 12 | Successful closure |
| 2 | Benito-González et al, 13 | 75/M | Dyspnoea on exertion | Arthrodesis of thoracolumbar spine | No PE | Normal | Successful closure |
| 3 | Charbonnel et al,14 | 84/F | Severe hypoxaemia | Idiopathic unilateral phrenic nerve palsy | Small PE | – | – |
| 4 | Maholic et al, 15 | 84/F | Hypoxia | GBS 1 month earlier | No PE | PA: 22/5, RA: 5 | Successful closure |
| 5 | Darchis et al,16 | 79/F | Dyspnoea for 3 weeks | Hepatomegaly from metastasis | Small PE | MRA: 4 | Successful closure |
| 6 | Darchis et al, 16 | 61/F | Hypoxaemia | Phrenic nerve injury from CABG surgery | – | MRA: five with no right-to-left pressure gradient | Successful closure |
| 7 | Darchis et al, 16 | 84 Y/F | Dyspnoea for 3 weeks | – | Small PE | Cath done but values not mentioned | Successful closure |
| 8 | Lopez Gaston et al,17 | 75/M | Dyspnoea × 7 weeks | – | No PE | Cath done | Successful closure |
| 9 | Ghamade et al,18 | 79/F | Hypoxaemia for 6 weeks | Oophorectomy and bladder suspension | No PE | MPA: 21, MRA: seven with no gradient | Successful closure |
| 10 | Cordero et al, 19 | 57/M | Dyspnoea 1 month | Idiopathic unilateral phrenic nerve palsy | No PE | Normal pressures | Successful closure |
| 11 | Murray et al, 20 | 72/M | Dyspnoea 3 months | Idiopathic unilateral phrenic nerve palsy | No PE | Normal Pressure | Successful closure |
| 12 | Ibrahim et al,21 | 59/F | Dyspnoea | Idiopathic unilateral phrenic nerve palsy | No PE | Normal Pressure | Successful closure |
| 13 | This case | 61/M | Dyspnoea | Idiopathic unilateral phrenic nerve palsy | No PE | Normal Pressure | Successful closure |
CABG, coronary artery bypass grafting; GBS, Guillian-Barre syndrome; MPA, mean pulmonary artery; MPP, mean pulmonary pressure; MRA, mean right atrial; MRAP, mean right atrial pressure; PA, pulmonary artery; PE, pulmonary embolism; RA, right atrial; RHC, right heart catheterisation.
The mechanism of RLS in the absence of an interatrial pressure gradient was first described by Zanchetta et al as the ‘flow phenomena’.9 Right atrium can be divided into an anterior and posterior portion according to embryological development. Superior vena cava (SVC) opens in anterior portion and blood flows downward, and forward, inferior vena cava (IVC) opens up into the posterior portion, and blood flows upwards and backwards to avoid turbulence by creating a pattern of rotation. Right-sided diaphragmatic paralysis results in the shift of mediastinum, which alters the relative position of the atrial septum and IVC and the blood coming from IVC is directed towards foramen ovale creating RLS in the absence of interatrial pressure gradient. A similar mechanism has been proposed for RLS due to pneumonectomy, and aortic root enlargement.
The most common aetiology for UDP is idiopathic, but other reasons should also be considered such as cardiac surgery, cervical cord compression and pneumonia. As in our patient, detailed workup was done for the possible causes of diaphragmatic paralysis including CT of the cervical and thoracic spine and was found to be negative. An old chest X-ray from 4 years ago did not show right-sided diaphragmatic elevation. Further inquiry regarding any traumatic events in the past revealed that he did have a fall about a year ago for which a CT head and cervical cord was done and were found to be unremarkable. No chest X-ray was done at that visit, and he did not recall any respiratory problems after the fall.
In patients with severe hypoxia unresponsive to oxygen therapy and with normal lung parenchyma, intracardiac shunt should always be a consideration and workup should include transthoracic ECHO with bubble study, and if PFO is found it should be followed by TOE. TOE helps to measure the accurate anatomy of PFO, for example, size, length and also helps exclude other possible causes of shunt such as eustachian valve and atrial septal aneurysm.10 11 Cardiac catheterisation should follow TOE as it helps to rule out increased right-sided cardiac pressure as the cause of RLS. A step down in oxygen saturation from pulmonary veins into left atrium is also another clue for RLS, and which is due to deoxygenated blood coming in from the IVC and SVC mixing with oxygenated blood coming in from pulmonary veins in the left atrium. The diagnosis can be further consolidated by the occlusion test of the atrial defect with the help of the balloon tip catheter which brings up the oxygen saturation in the left atrium to normal.4 In such circumstances, closure of PFO through percutaneous transcatheter intervention is an indication and hypoxia generally improves after closure. There have been calls to address the diaphragmatic paralysis as it is the underlying cause for the decompensation in patients who had asymptomatic PFO for decades.
Recurrence of RLS is uncommon after closure, and the procedure is generally tolerated well. Our patient’s oxygenation improved after the closure of PFO.
Learning points.
Right-to-left shunt via patent foramen ovale (PFO) can occur due to various causes that either increase the right atrial pressure, reduce the left atrial pressure or facilitate the inferior vena cava flow to be directed to the PFO.
In rare instances, new diaphragmatic paralysis in the background of asymptomatic PFO can cause significant hypoxaemia which poses a diagnostic challenge due to the novelty of this condition.
Pulmonologists and cardiologists need to be aware of this rare phenomena as the condition can be life threatening if not diagnosed on time but if managed appropriately has a good prognosis.
Footnotes
Contributors: WU did critical review and manuscript writing, ARG and PD modified and improved the case presentation and MH did literature search.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Meissner I, Whisnant JP, Khandheria BK, et al. Prevalence of potential risk factors for stroke assessed by transesophageal echocardiography and carotid ultrasonography: the SPARC study. Stroke prevention: assessment of risk in a community. Mayo Clin Proc 1999;74:862–9. [DOI] [PubMed] [Google Scholar]
- 2. Elefteriades J, Singh M, Tang P, et al. Unilateral diaphragm paralysis: etiology, impact, and natural history. J Cardiovasc Surg 2008;49:289–95. [PubMed] [Google Scholar]
- 3. Hagen PT, Scholz DG, Edwards WD. Incidence and size of patent foramen ovale during the first 10 decades of life: an autopsy study of 965 normal hearts. Mayo Clin Proc 1984;59:17–20. 10.1016/S0025-6196(12)60336-X [DOI] [PubMed] [Google Scholar]
- 4. Godart F, Rey C, Prat A, et al. Atrial right-to-left shunting causing severe hypoxaemia despite normal right-sided pressures. Report of 11 consecutive cases corrected by percutaneous closure. Eur Heart J 2000;21:483–9. 10.1053/euhj.1999.1944 [DOI] [PubMed] [Google Scholar]
- 5. Fisher DC, Fisher EA, Budd JH, et al. The incidence of patent foramen ovale in 1,000 consecutive patients. A contrast transesophageal echocardiography study. Chest 1995;107:1504–9. [DOI] [PubMed] [Google Scholar]
- 6. van Rossum P, Plokker HW, Ascoop CA. Breathlessness and hypoxaemia in the upright position after right pneumonectomy. Eur Heart J 1988;9:1230–3. 10.1093/oxfordjournals.eurheartj.a062434 [DOI] [PubMed] [Google Scholar]
- 7. Faller M, Kessler R, Chaouat A, et al. Platypnea-orthodeoxia syndrome related to an aortic aneurysm combined with an aneurysm of the atrial septum. Chest 2000;118:553–7. 10.1378/chest.118.2.553 [DOI] [PubMed] [Google Scholar]
- 8. Perkins LA, Costa SM, Boethel CD, et al. Hypoxemia secondary to right-to-left interatrial shunt through a patent foramen ovale in a patient with an elevated right hemidiaphragm. Respir Care 2008;53:462–5. [PubMed] [Google Scholar]
- 9. Zanchetta M, Rigatelli G, Ho SY. A mystery featuring right-to-left shunting despite normal intracardiac pressure. Chest 2005;128:998–1002. 10.1378/chest.128.2.998 [DOI] [PubMed] [Google Scholar]
- 10. Bashour T, Kabbani S, Saalouke M, et al. Persistent Eustachian valve causing severe cyanosis in atrial septal defect with normal right heart pressures. Angiology 1983;34:79–83. 10.1177/000331978303400201 [DOI] [PubMed] [Google Scholar]
- 11. Chidambaram M, Mink S, Sharma S. Atrial septal aneurysm with right-to-left interatrial shunting. Tex Heart Inst J 2003;30:68–70. [PMC free article] [PubMed] [Google Scholar]
- 12. Fabris T, Buja P, Cucchini U, et al. Right-to-left interatrial shunt secondary to right hemidiaphragmatic paralysis: an unusual scenario for urgent percutaneous closure of patent foramen ovale. Heart Lung Circ 2015;24:e56–9. 10.1016/j.hlc.2014.11.003 [DOI] [PubMed] [Google Scholar]
- 13. Benito-González T, Díez-Fernández F, Pérez de Prado A. Respiratory failure associated with diaphragmatic paralysis: just a ventilation/perfusion problem? Arch Bronconeumol 2016;52:566–7. 10.1016/j.arbr.2016.09.001 [DOI] [PubMed] [Google Scholar]
- 14. Charbonnel C, Ennezat PV, Darchis J, et al. [Pulmonary embolism and right diaphragmatic paralysis: “one train can hide another”]. Arch Mal Coeur Vaiss 2007;100:61–3. [PubMed] [Google Scholar]
- 15. Maholic R, Lasorda D. Successful percutaneous closure of a patent foramen ovale causing hypoxia in the setting of an elevated hemidiaphragm due to Guillian-Barre syndrome. J Invasive Cardiol 2006;18:434. [PubMed] [Google Scholar]
- 16. Darchis JS, Ennezat PV, Charbonnel C, et al. Hemidiaphragmatic paralysis: an underestimated etiology of right-to-left shunt through patent foramen ovale? Eur J Echocardiogr 2007;8:259–64. 10.1016/j.euje.2006.05.003 [DOI] [PubMed] [Google Scholar]
- 17. Lopez Gaston OD, Calnevaro O, Gallego C, et al. [Platypnea-orthodeoxia syndrome, atrial septal aneurysm and right hemidiaphragmatic elevation with a right-to-left shunt through a patent foramen ovale]. Medicina 2005;65:252–4. [PubMed] [Google Scholar]
- 18. Ghamande S, Ramsey R, Rhodes JF, et al. Right hemidiaphragmatic elevation with a right-to-left interatrial shunt through a patent foramen ovale: a case report and literature review. Chest 2001;120:2094–6. [DOI] [PubMed] [Google Scholar]
- 19. Cordero PJ, Morales P, Mora V, et al. Transient right-to-left shunting through a patent foramen ovale secondary to unilateral diaphragmatic paralysis. Thorax 1994;49:933–4. 10.1136/thx.49.9.933 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Murray KD, Kalanges LK, Weiland JE, et al. Platypnea-orthodeoxia: an unusual indication for surgical closure of a patent foramen ovale. J Card Surg 1991;6:62–7. 10.1111/j.1540-8191.1991.tb00565.x [DOI] [PubMed] [Google Scholar]
- 21. Ibrahim H, Khan A, Nishi SP, et al. Symptomatic patent foramen ovale with hemidiaphragm paralysis. Case Rep Pulmonol 2017;2017:1–4. 10.1155/2017/9848696 [DOI] [PMC free article] [PubMed] [Google Scholar]