

Description
A 60-year-old woman presented with single episode of haematuria. An ultrasonogram was done, which was suggestive of bilateral small renal masses. Contrast-enhanced CT (CECT) scan of the abdomen confirmed the presence of right upper pole (2×2 cm) and left lower pole (2.5×2.5 cm) renal masses (figure 1). Along with these renal masses she had bilateral adrenal gland metastases (figure 2). The patient was counselled regarding his disease and the benefits versus risk of bilateral adrenalectomy that included a need for steroid replacement therapy after bilateral adrenalectomy. The patient then underwent right partial nephrectomy with adrenalectomy and enucleation of the left renal mass. The left adrenal gland was preserved to prevent adrenal insufficiency. Histopathological examination of the tumour specimens showed clear cell renal carcinoma, Fuhrman grade 3. Then systemic immunotherapy was started with tyrosine kinase inhibitor—sunitinib, at a dose of 37.5 mg with 4 weeks on and 2 weeks off schedule. The patient tolerated the drug without any significant adverse effects. Six months postsurgery, the patient is doing well and tolerating immunotherapy without any significant side effects.
Figure 1.
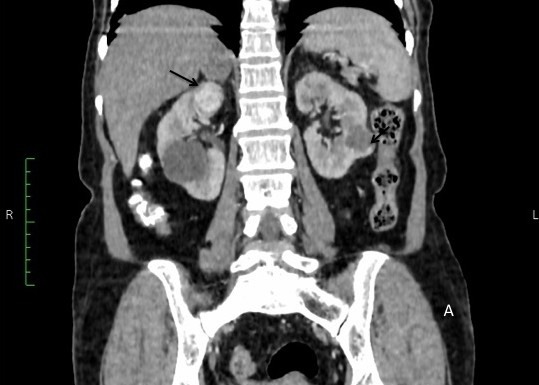
Coronal sections of contrast-enhanced CT scan showing bilateral renal masses (arrows).
Figure 2.
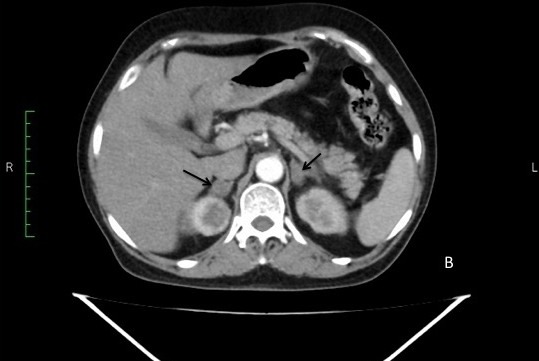
The bilateral adrenal metastases (arrows) seen on the transverse section of contrast-enhanced CT scan.
Rates of ipsilateral adrenal metastasis from renal cell carcinoma range from 6% to 29% in autopsy series.1 Metastasis to the contralateral adrenal gland is very rare and is seen in <1% of cases. Only a few cases of bilateral adrenal metastasis are reported in literature.2 Management of such cases is challenging as bilateral adrenalectomy may lead to development of iatrogenic Addison’s disease. Our case was unique as the patient had bilateral renal cell carcinoma with metastasis in bilateral adrenal glands. Such cases due to their rarity pose a therapeutic challenge for the urologist.
According to current guidelines, adrenalectomy has to be performed along with radical nephrectomy in case of detectable metastases on CECT or MRI, mass >8 cm and superior pole masses. Due to their rarity the management of bilateral adrenal metastases is not well defined with ~20 cases reported in literature. The benefits of cytoreductive nephrectomy by removing all resectable metastases have been documented in many studies. But with the results of recently concluded trials available it has been shown that with available targeted therapy the overall and cancer specific survival is similar (non-inferior) in patients with metastatic renal cell carcinoma undergoing cytoreductive nephrectomy versus those not undergoing it when both were given targeted therapy.3 Based on these results it is probably reasonable that to prevent Addison’s disease unilateral adrenalectomy followed by targeted therapy is sufficient in patients with bilateral adrenal metastases.
Learning points.
In patients with bilateral involvement of adrenal glands due to renal cell carcinoma the management options include bilateral adrenalectomy and steroid replacement therapy or unilateral adrenalectomy followed by systemic immunotherapy with tyrosine kinase inhibitors.
It is important that in such cases the patient is fully explained regarding his disease and management options, as we proceeded with unilateral adrenalectomy followed by systemic immunotherapy after patient consent.
Footnotes
Patient consent for publication: Obtained.
Contributors: SP conceived the case report. SP and TP were major contributors towards writing the manuscript. VS, AS and SP treated the patient and also interpreted the patient data. SP and TP were involved in the review. All authors read and approved the final manuscript.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Siemer S, Lehmann J, Kamradt J, et al. Adrenal metastases in 1635 patients with renal cell carcinoma: outcome and indication for adrenalectomy. J Urol 2004;171:2155–9. 10.1097/01.ju.0000125340.84492.a7 [DOI] [PubMed] [Google Scholar]
- 2. Koutalellis GE, Felekouras E, Evangelou C, et al. Renal cell carcinoma with bilateral synchronous adrenal gland metastases: a case report. Cases J 2009;2:7298 10.4076/1757-1626-2-7298 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Motzer RJ, Jonasch E, Agarwal N, et al. Kidney cancer, version 2.2017, nccn clinical practice guidelines in oncology. J Natl Compr Canc Netw 2017;15:804–34. 10.6004/jnccn.2017.0100 [DOI] [PubMed] [Google Scholar]