

Abstract
Autoimmune hepatitis (AIH) is a relatively rare acute or chronic liver disease of unknown etiology characterized by large heterogeneity. Its distribution is global, covering all ages, both sexes and all ethnic groups. The aim of the present Clinical Practice Guidelines (CPG) of the Hellenic Association for the Study of the Liver was to provide updated guidance and help to gastroenterologists, hepatologists, internists and general practitioners for AIH diagnosis and management. AIH diagnosis is based on clinicopathological characteristics: namely, polyclonal hypergammaglobulinemia, particularly of immunoglobulin G (IgG), circulating autoantibodies, interface hepatitis on liver histology, absence of viral hepatitis, and a favorable response to immunosuppression. Clinical manifestations at disease onset are variable, ranging from asymptomatic to the acute/severe form. Aminotransferase and bilirubin levels vary, while the presence of hepatitis at the histological level is a prerequisite for diagnosis. Autoantibodies are the hallmark for AIH diagnosis; therefore, the CPG describe the appropriate serological algorithm for their detection. AIH therapy should aim to achieve complete biochemical (normalization of IgG and aminotransferases) and histological remission. All patients who have active disease, even those with cirrhosis, should be treated with individualized and response-guided induction therapy using prednisolone in combination with azathioprine or mycophenolate mofetil as first-line therapy. Immunosuppression should be given for at least 3 years and for at least 2 years after the achievement of complete biochemical response, while a liver biopsy should be recommended before treatment discontinuation. Current CPG are also provided for several specific conditions and difficult-to-treat patients.
Keywords: Autoimmune hepatitis, autoantibodies, clinical practice guidelines, corticosteroids, azathioprine
Introduction and historical review
In 1950, Jan Waldenström was the first to describe a new type of a progressive, usually fatal, chronic hepatitis in young females with endocrine dysfunction, cutaneous striae, acne, polyarthralgias, and high γ-globulins that correlated with abundant plasma cells on liver biopsy [1]. In 1956, Cowling et al [2] introduced the term “lupoid hepatitis”, because the lupus erythematosus cell phenomenon was observed in these patients. However, 10 years later, this term was changed to “autoimmune hepatitis” (AIH), finally accepted by the International AIH Group (IAIHG) as the definite one [3,4].
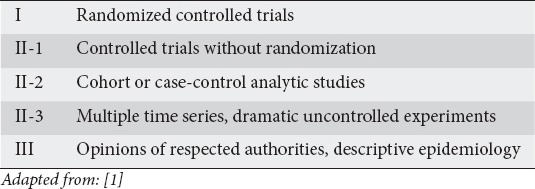
The aim of the present Clinical Practice Guidelines (CPG) of the Hellenic Association for the Study of the Liver (HASL) was to provide guidance and help to gastroenterologists, hepatologists, internists and general practitioners in the diagnosis and management of this disease, in an attempt to improve care for affected patients. The current statements and recommendations were based on the GRADE system for evidence published by Shaneyfelt et al [5] (Suppl. Table 1).
Supplementary Table 1.
Grading of recommendations
Epidemiology
AIH is an acute or more frequently chronic liver disease of unknown etiology that primarily affects females (female/male: 3-4/1) and is characterized by polyclonal hypergammaglobulinemia, particularly of immunoglobulin G (IgG), autoantibodies, interface hepatitis and favorable response to treatment [6-10].
AIH is considered relatively rare, as its prevalence is about 160-180/1,000,000 population in Europe [11-14]. Recently, a large nationwide study in Denmark showed a significant increase in AIH incidence, reaching a prevalence of 350/1,000,000 in women [15]. So far, reliable epidemiological data from Greece are not available; therefore, since 2016 HASL has started a nationwide registry for all retro- and prospective AIH cases.
AIH carries several clinical phenotypes and outcomes according to ethnicity, with patients of Hispanic, Asian or other non-European Caucasian origin demonstrating poor outcomes [16]. These differences are thought to be due to differences in genetic predisposition and triggering agents, but also to complex socioeconomic factors, such as discrepancies in healthcare delivery and failure to diagnose AIH, which finally results in delayed diagnosis [17].
STATEMENT 1.
AIH prevalence is increasing in Europe irrespective of sex, ranging from 160-180/1,000,000 inhabitants to as much as 350/1,000,000 in females (II-2)
Clinical manifestations
Clinical characteristics
AIH is a discrete clinical syndrome characterized by considerable demographic, clinical, laboratory and histological heterogeneity (Table 1). Therefore, extended differential diagnosis should be performed, considering the possibility of AIH in any acute or chronic liver disease (Tables 2, 3) [4,6-8,10,18-22]. Both sexes in all ethnic groups can be affected at any age. Disease onset has a bimodal distribution during the childhood/teenage and 4th-6th decades, but recently many patients have been diagnosed at older ages (>65 years) [6-8,11-15,23-25]. The disease may accumulate in first-degree relatives, but the absolute risk is very low. High rates of depression and anxiety have recently been recognized in AIH patients [26,27].
Table 1.
Clinical manifestations of autoimmune hepatitis (AIH)
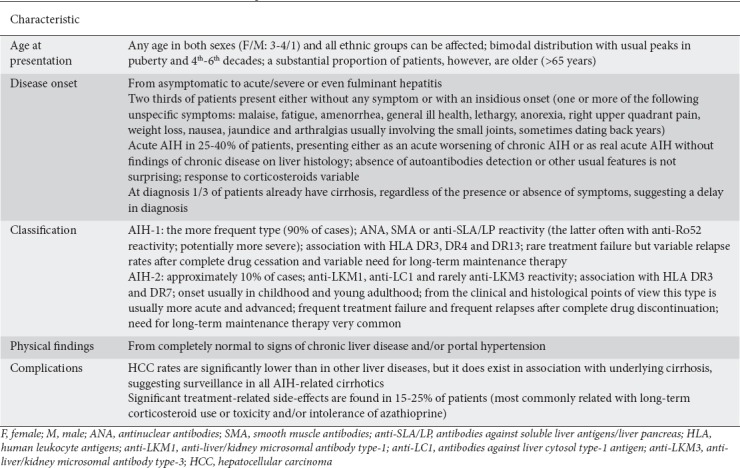
Table 2.
Differential diagnosis of autoimmune hepatitis
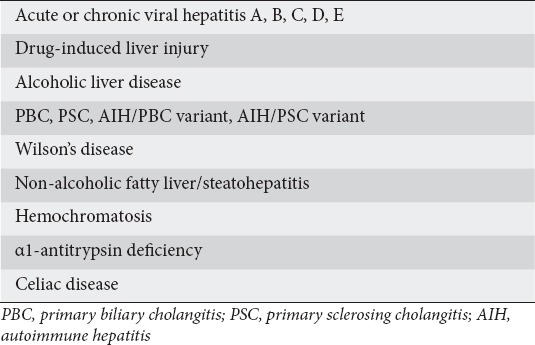
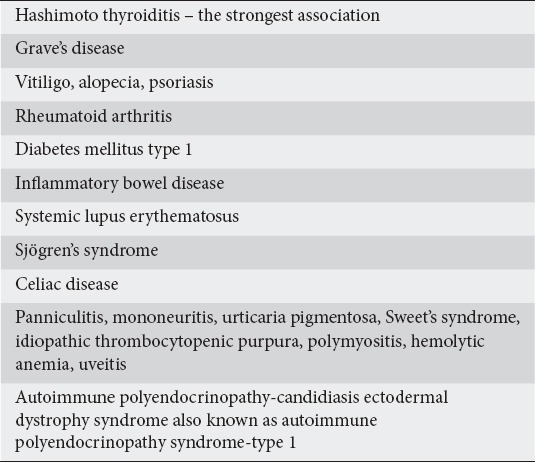
Table 3.
Common concurrent autoimmune or immune-mediated diseases in patients with autoimmune hepatitis
The manifestations are variable, ranging from asymptomatic to acute/severe or even fulminant hepatitis (Table 1) [7-9,28-30]. The acute onset accounts for 25-40% of patients and does not differ from other causes of acute hepatitis [29-31]. Two different syndromes are recognized in acute AIH: one is the acute worsening of a previously undiagnosed or misdiagnosed chronic AIH and the second is the original acute disease without chronic lesions on histology (Table 1) [28,31,32]. Interestingly, some patients with acute AIH have normal IgG levels, while 9-17% of patients have negative results at first screening for antinuclear (ANA) or smooth muscle (SMA) antibodies; consequently, physicians may not consider AIH [6-10].
Two thirds of patients present either without any symptom or with an insidious onset characterized by one or more of the general non-specific symptoms shown in Table 1 [11,14-17,23,33,34]. Physical findings vary from completely normal to signs of advanced disease with accompanied portal hypertension. Unfortunately, almost one third of adults and half of children already have cirrhosis at diagnosis [11,15,23,33-36].
According to the autoantibodies detected, a classification of AIH into two major types, AIH-1 and AIH-2, has been introduced (Table 1). AIH-1 is characterized by ANA, SMA and/or soluble liver antigens/liver pancreas antibodies (anti-SLA/LP) detection, while AIH-2 is associated with anti-liver/kidney microsomal antibody type-1 (anti-LKM1), or rarely anti-LKM-type 3 (anti-LKM3), and/or antibodies against liver cytosol type-1 antigen (anti-LC1) [6,7,10,18,19]. Apart from autoantibodies, this distinction also brings other differences helpful for clinicians (Table 1).
RECOMMENDATIONS 1-6.
AIH should be considered in any patient with acute or chronic hepatitis, particularly in the presence of high IgG levels, as it has a global distribution at any age in both sexes and in all ethnic groups (II-2)
Precise and early diagnosis is mandatory, as untreated AIH carries high morbidity and mortality rates (I)
AIH patients can be considered for screening for concurrent autoimmune diseases, especially autoimmune thyroiditis, since AIH is associated with a reduced quality of life and a broad variety of other autoimmune-mediated conditions (II-2)
Cirrhosis at diagnosis should be suspected in AIH, as almost 33% of adults and 50% of children with AIH are first diagnosed at the stage of cirrhosis, indicating that they have had subclinical disease for a long time (II-2)
-
Acute AIH can be diagnosed presenting as one of the following two clinical forms:
- -acute worsening of previously undiagnosed or misdiagnosed AIH or
- -real (original) acute onset of AIH without chronic lesions on liver histology (II-2)
AIH can be classified into two types: AIH-1, ANA, SMA and/or anti-SLA/LP positive; and AIH-2, anti-LKM1, anti-LKM3 and/or anti-LC1 positive. Apart from differences in circulating autoantibodies, other differences in the clinical substrate have become apparent that may be helpful to clinicians (II-2)
Specific features
AIH may be first diagnosed during pregnancy or more frequently after delivery (Table 4). Postpartum exacerbations may also occur in AIH patients whose condition improved during pregnancy [37-39]. Interestingly, immunosuppression has probably enabled the occurrence of pregnancy in young females with amenorrhea at presentation due to AIH.
Table 4.
Specific characteristics of autoimmune hepatitis (AIH)
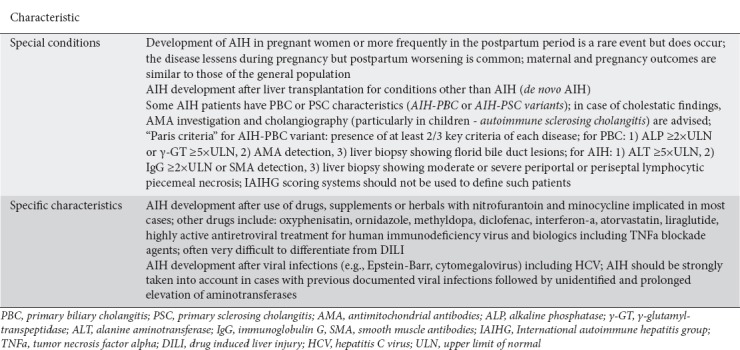
AIH may also develop after the administration of many drugs, supplements and/or herbals, with nitrofurantoin and minocycline being the best documented among diverse cases (Table 4) [40-44]. Drug-induced AIH is a complex and challenging condition characterized clinically and histologically by different phenotypes across the disease spectrum [40,45]. Therefore, the differentiation between drug-induced liver injury (DILI) and DILI-induced AIH is often difficult [46]. In such cases, the patients’ history is important, as in one third of patients with DILI the clinical features can be associated with hypersensitivity manifestations, such as fever, rash and eosinophilia [47,48]. The follow up can also help in differential diagnosis, as steroid treatment can be discontinued without relapse in DILI, in contrast to the almost universal relapse after stopping a few-month course of immunosuppressive therapy in the “true” DILI-induced AIH (Fig. 1).
Figure 1.
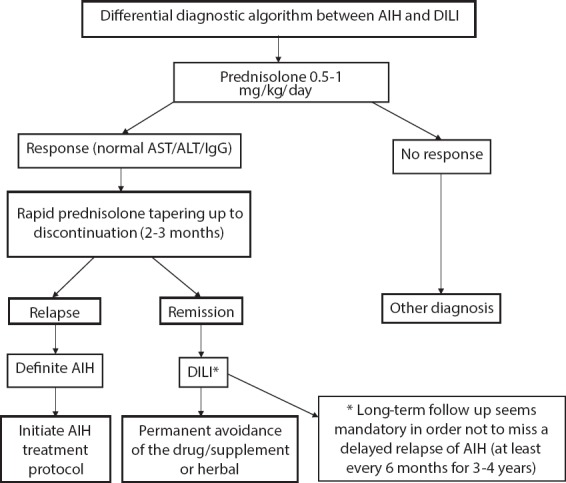
Proposed algorithm for the differential diagnosis between autoimmune hepatitis (AIH) and drug-induced liver injury (DILI) in an index case with biochemical hepatitis, positive liver autoimmune serology and hepatitis on liver histology, irrespective of the presence or absence of high IgG levels
AST, aspartate aminotransferase; ALT, alanine aminotransferase; IgG, immunoglobulin G.
AIH development has also been observed after viral infections [7,8,49,50], including hepatitis C virus (HCV) treated with interferon-a (IFNa) [51], or after liver transplantation for other liver diseases in adults and children (Table 4). This condition has been called de novo AIH and its early recognition seems helpful for avoiding another liver transplantation and improving patients’ long-term survival [52-54].
RECOMMENDATION 7.
AIH should be considered in the appropriate clinical and laboratory setting after use of drugs, supplements or herbals; viral infections; liver transplantation (de novo AIH); and rarely during pregnancy or after delivery (II-3)
Complications
As in other chronic liver diseases, cirrhosis and its consequences, including portal hypertension and hepatocellular carcinoma (HCC), may occur. Therefore, surveillance with ultrasonography every 6 months seems rational in patients with cirrhosis. HCC, however, is developed at significantly lower rates in AIH-associated cirrhosis compared with other causes (Table 1) [14,15,55-58].
RECOMMENDATION 8.
Patients with AIH-related cirrhosis should undergo ultrasonography every 6 months for early HCC detection, as in cirrhosis of other etiologies (II-2)
AIH variants
Some patients present, either concurrently or consecutively, with features of primary biliary cholangitis (PBC) or primary sclerosing cholangitis (PSC), while some PBC or PSC patients may also show AIH characteristics (Table 4) [59]. However, the previous term “overlap” used for years for these entities strongly suggests the simultaneous presence of two distinct diseases, which of course is not the case for many of these patients. Therefore, the term “variant” has recently been proposed by the European Association for the Study of the Liver (EASL), thought to be more precise for these conditions [60].
Worldwide accepted criteria defining these conditions are lacking and hence their diagnosis is usually difficult. Regarding the AIH-PBC variant, its prevalence is about 10% in adults with PBC or AIH [61]. The “Paris criteria” are even nowadays the most often used in everyday clinical practice (Table 4) [61]. Unlike several uncertainties around this issue, the recent EASL guidelines on PBC diagnosis and management recommend that liver histology is mandatory in evaluating patients with this variant of AIH [62]. In particular, liver biopsy seems crucial because of potential therapeutic implications in the PBC cases who do not respond to ursodeoxycholic acid (UDCA), having also disproportionate elevations in alanine aminotransferase (ALT) and/or IgG [62].
The AIH-PSC variant has been reported in 7-14% of mainly young patients with autoimmune liver diseases [59,63-65]. The criteria for AIH-PSC diagnosis are even less well defined than those used in AIH-PBC patients. In routine clinical practice, AIH-PSC diagnosis is based on typical cholangiographic or histological characteristics of PSC, along with AIH characteristics [66]. Interestingly, a specific and unique variant has been reported in 50% of children with AIH, characterized by both AIH and sclerosing cholangitis features; therefore, the term “autoimmune sclerosing cholangitis” was proposed [63]. Magnetic resonance cholangiopancreatography (MRCP) is advised for all children with an initial AIH diagnosis (Table 4) [63,64]. This entity is exceptionally rare in adults with AIH and thus MRCP screening is not justified [67].
STATEMENT 2.
Coexistence of AIH features and cholestatic diseases can be observed at both diagnosis and follow up, but their diagnosis may be problematic because of the lack of internationally accepted criteria (II-2)
RECOMMENDATIONS 9-11.
All children with AIH should undergo at least MRCP to exclude autoimmune sclerosing cholangitis (II-2)
Adult AIH patients should be considered for MRCP only when cholestatic laboratory manifestations are present (II-3)
AIH patients showing cholestatic features should be tested for PBC (ΙΙ-2)
Laboratory investigation
Biochemistry
Bilirubin and aminotransferase levels vary from just above the upper limits of normal (ULN) to very high levels [4,7,8,18,19]. Alkaline phosphatase (ALP) is usually normal or moderately elevated, while γ-glutamyl-transpeptidase (γ-GT) can increase variously [23,34]. Spontaneous normalization of aminotransferases and γ-GT can be observed, although there is usually evidence of continuing inflammatory activity at the histological level. This phenomenon may result in delay and/or underestimation of AIH diagnosis, as the next AIH hit can be pronounced after many months or years or may even be absolutely asymptomatic, explaining at least partially the presence of cirrhosis in one third of patients at diagnosis.
Irrespectively of the presence of cirrhosis, the majority of patients have high serum γ-globulins or IgG, a distinctive feature of AIH [19,23]. However, 25-40% of patients with acute AIH have normal IgG [29,68]. It should be noted that the range of “normal” IgG is ample, as it is impractical to have the “real normal ranges” of the respective population where an index case resides.
Liver autoimmune serology
Conventional antibodies
Autoantibodies are the hallmark for AIH diagnosis. Indirect immunofluorescence (IIF), preferably on freshly frozen rodent substrates including kidney, liver and stomach, is the technique of choice for routine screening (Fig. 2) [60]. Significant titers are ≥1:40 in adults, while ≥1:20 for ANA or SMA and ≥1:10 for anti-LKM1 are supportive of AIH diagnosis in children in association with other laboratory and clinical findings [19,60,69]. Other assays, such as ELISA or immunoblotting, are available for anti-LKM1, anti-LKM3, anti-LC1 and anti-SLA/LP testing [7,8,70].
Figure 2.
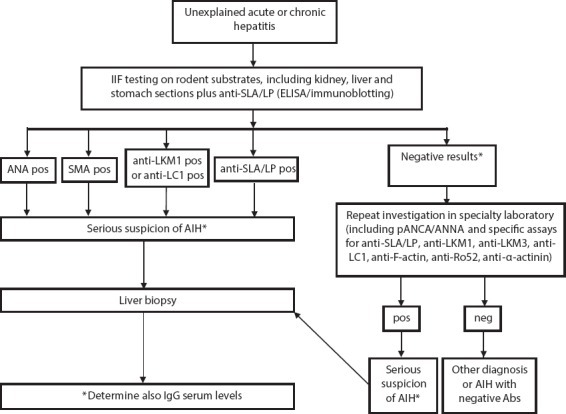
Proposed algorithm for routine autoantibody testing in cases with a suspicion of autoimmune hepatitis
Anti-SLA/LP, antibodies against soluble liver antigens/liver pancreas; ELISA, enzyme linked immunosorbent assay; Abs, autoantibodies; ANA, antinuclear antibodies; SMA, smooth muscle antibodies; anti-LKM1, anti-liver/kidney microsomal antibody type 1; anti-LC1, antibodies against liver cytosol type-1 antigen; pANCA/ANNA, perinuclear anti-neutrophil cytoplasmic antibodies/anti-nuclear neutrophil antibodies; anti-LKM3, anti-liver/kidney microsomal antibody type 3; AIH, autoimmune hepatitis.
ANA and SMA are not disease-specific and show a wide range of heterogeneity in the IIF pattern on HEp2 cells, together with varying titers [7,8,60]. However, no single ANA staining pattern on HEp2 cells is pathognomonic of AIH or seems to have any clinical and diagnostic implication in everyday practice; for these reasons their use in initial testing is not recommended. Since SMA react to cytoskeletal elements, including F-actin (the major autoantigen of SMA), testing for anti-F-actin antibodies can also be performed by ELISA [7,8,71,72]. However, IIF appears superior compared with ELISA, as testing only by ELISA may result in missing almost 20% of AIH cases [7,8,71-73].
Anti-LKM1/3 and/or anti-LC1 often coexist in AIH-2 but are not disease-specific, as they may be detected in 5-10% of HCV or hepatitis D virus (HDV) infections [7,8,23,51,70-72,74-76]. The major target-autoantigens of anti-LKM1 and anti-LKM3, first described in about 13% of HDV infections, are the cytochrome P4502D6 and family-1 of UDP-glucuronosyltransferases, respectively—although the antigenic sites differ between AIH and HCV or HDV infections; for anti-LC1 the major target-autoantigen is the formiminotransferase cyclodeaminase enzyme [7,8,60,70-72,74,76,77]. Repeated testing is advised in initially seronegative individuals, as conventional autoantibody titers vary during the course of AIH and may be detected later [18,70-72]. Autoantibody titers do not need to be monitored in adults, but should be in children, where they are considered as markers of disease activity [69]. Notably, the previous recommendation of the IAIHG for anti-LKM screening before starting IFNa-based therapies in HCV infections, as IFNa may sometimes unmask or provoke autoimmune liver reactivity and even original AIH, seems not to be rational in the new era of direct acting antivirals (DAAs) [18,51,65,78].
Non-conventional antibodies
Anti-SLA/LP has greater diagnostic value, being the only AIH-specific autoantibody. However, it is only detected in up to a third of patients, usually in strong association with anti-Ro52 antibodies (concurrence in 77-98%) [79-82]. The target-autoantigen is a synthase (S) converting O-phosphoseryl-tRNA (Sep) to selenocysteinyl-tRNA (Sec); it is therefore labeled as SepSecS, which in turn resulted in the development of reliable molecular-based assays for its detection [83,84]. Anti-SLA/LP has been associated with more aggressive disease [85], although these findings were not confirmed in recent studies [79,82].
Perinuclear pattern of anti-neutrophil cytoplasmic antibodies (pANCA), also referred to as perinuclear anti-neutrophil nuclear antibodies (p-ANNA), are detected (significant titer ≥1:20) by IIF frequently in AIH-1 patients and may act as an additional pointer towards diagnosis [18,69-72]. Anti-mitochondrial antibodies (AMA), strongly specific for PBC [86], can be detected in 8-12% of AIH patients without, however, any other evidence of chronic cholestatic disease [87-92].
Antibodies against α-actinin, which belongs to the F-actin cross-linking proteins, have been detected in autoimmune diseases such as systemic lupus erythematosus and AIH-1 [93,94]. These antibodies seem to carry particular clinical significance, as they characterize a subgroup of more severe form of AIH, specifically in association with anti-F-actin, while they might be used as predictors of treatment response [95-97]. Antibody against the asialoglycoprotein receptor is another frequently detected autoantibody, which can support diagnosis if patients have tested negative for other autoantibodies [7,8,70-72]. However, its specificity seems low and therefore its routine determination is not recommended [60].
Liver histology
The presence of hepatitis is a prerequisite for AIH diagnosis [4,6,10,18,19,60]. Ideally, liver biopsy should be performed before the initiation of treatment, as disease necroinflammatory activity and severity are not always in parallel with biochemistry [6,10,18,19]. Therefore, a pretreatment liver biopsy can provide information on prognosis but also on optimal AIH management; for instance, the potential presence of cirrhosis may influence the choice and dose of immunosuppression and suggest regular screening for complications. The typical lesions consist of interface hepatitis with portal lymphocytic/lymphoplasmacytic cells extending into lobule, hepatocyte rosetting and emperipolesis (etymology from the Greek language), which refers to the intracytoplasmic localization of one cell, usually a lymphocyte, within hepatocytes [19]. It should be noted however, that the abovementioned findings are not pathognomonic for AIH, while the absence of plasma cells observed in almost one third of AIH cases does not rule out the diagnosis [98].
Biopsies performed early in the acute disease show several signs of severe inflammatory activity, such as panlobular hepatitis with parenchymal collapse, presence of portal lymphoid follicles, inflammatory infiltrates enriched by plasma cells, central perivenulitis and pericentral, bridging or massive necrosis resembling those observed in acute DILI [18,28,68,99]. Inflammatory lymphocytic infiltrates of bile ducts have also been reported in approximately 10% of patients—without, however, any other clear manifestation of PBC [100]. At presentation, various fibrosis stages may be seen. Quantitative evaluation of inflammatory activity using the hepatitis activity index (HAI) score seems helpful during therapy and follow up.
Concerning the noninvasive methods, and in particular liver elastography, a recent study established that repeat transient elastography measurement is a reliable tool for AIH monitoring [101]. At present, however, the general belief is that the noninvasive tests are not able to replace liver biopsy at diagnosis and before treatment discontinuation [102].
Differential diagnosis and diagnostic scores
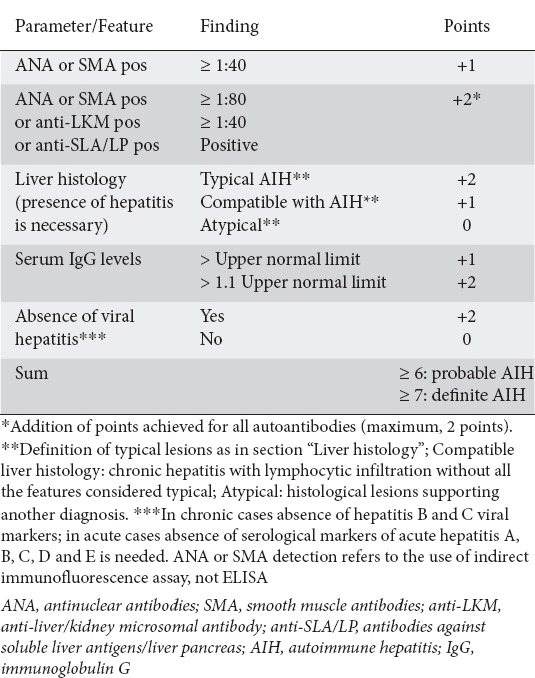
The differential diagnosis includes almost all causes of acute and chronic liver diseases as well as celiac disease [8,72,103] (Table 2). In 1999, the IAIHG published a score for AIH diagnosis [18] (Table 5). However, it proved quite complex for everyday use, while it was rather unable to safely distinguish AIH from cholestatic syndromes or AIH variants [65,104,105]. In 2008, the IAIHG proposed a simplified score for daily routine clinical practice, which is user-friendly, as it is based on autoantibody detection, IgG, liver histology, and seronegativity for viral hepatitis markers [19] (Table 6). This newer score seems to bear lower sensitivity (95% vs. 100%) but higher specificity and accuracy compared with the original revised score [106-108]. In general, however, physicians should keep in mind that any score should be used only as an aid to AIH diagnosis [109]. This is true, for example, in acute or fulminant AIH cases, AIH variants, children with AIH and DILI cases resembling AIH, as diagnosis by using the abovementioned diagnostic scores may be missed in such cases [28,29,68,99,108,110-112]. In particular, because of poor validation of the scores in the pediatric population, different scores have been suggested for child patients [69].
Table 5.
Revised scoring system for autoimmune hepatitis diagnosis (adapted from [18])
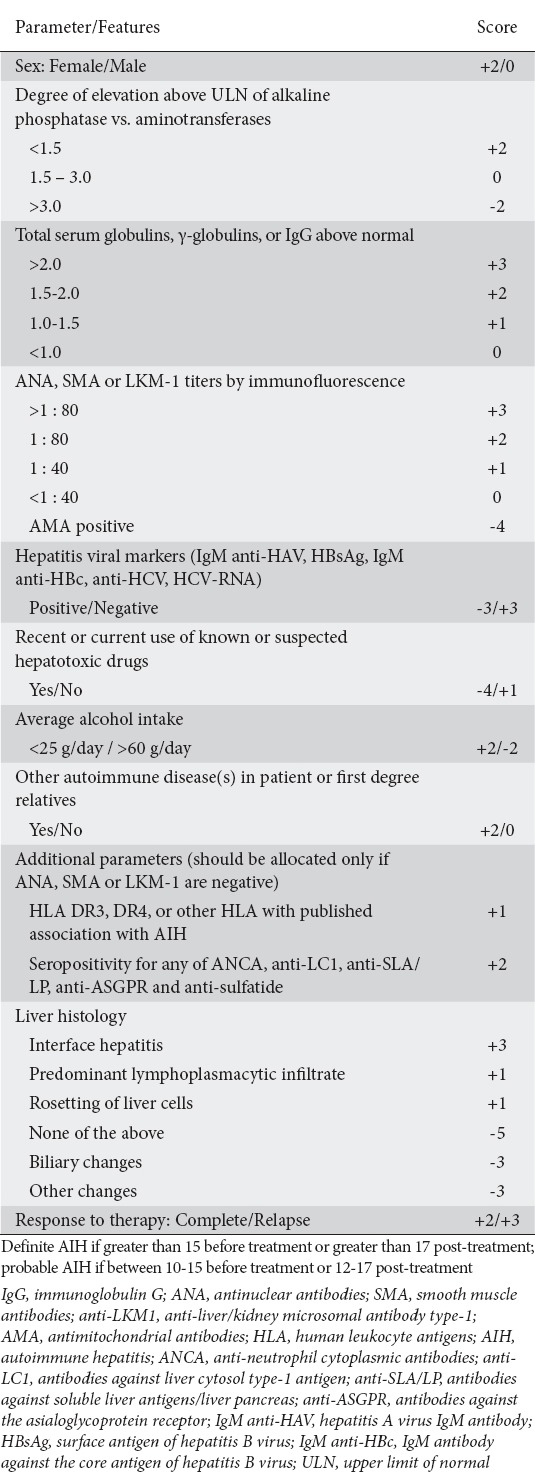
Table 6.
Simplified criteria for autoimmune hepatitis diagnosis (adapted from [19])
STATEMENTS 3-5.
AIH is a clinicopathological diagnosis and relies mainly on autoantibody detection, polyclonal hypergammaglobulinemia and supporting histology, usually in the absence of other liver disease (II-2)
Aminotransferases and bilirubin values vary in AIH (ΙΙ-2)
Presence of hepatitis at the histological level is a prerequisite for diagnosis (II-2)
RECOMMENDATIONS 12-16.
Normal IgG should not exclude the diagnosis of AIH, even though a selective high serum IgG is an important AIH characteristic (II-3)
IIF, preferably on freshly frozen rodent substrates, should be used for routine screening in the detection of most autoantibodies, while ELISA and immunoblotting should be used as the tests for anti-SLA/LP and anti-LC1 (II-3)
No anti-LKM screening is nowadays required in HCV patients before DAAs therapy (III)
Interface hepatitis, hepatocyte rosetting and emperipolesis should be considered as strongly supportive, although not pathognomonic, of AIH (II-2)
In acute AIH, several histological signs of severe inflammatory activity are observed, but they are usually indistinguishable from DILI (II-3)
RECOMMENDATIONS 17-19.
The 2008 simplified score should be used for AIH diagnosis in daily clinical practice, as it is a user-friendly clinical tool (II-2)
The previously established (1999) revised score can be helpful in diagnosing difficult AIH cases, as it includes response to treatment as an important parameter (II-2)
Diagnostic scores should not be used for the diagnosis of AIH-PBC and AIH-PSC variants. They may be used with caution for the diagnosis of AIH during childhood and for acute or fulminant disease, as they are not very well validated in these settings (II-2)
Management
All AIH patients who have active disease, even those with advanced fibrosis or cirrhosis, should receive immunosuppression in an attempt to achieve complete remission and to prevent the progression of liver disease through either maintenance therapy or a sustained remission following treatment withdrawal [6-8,10,33,60,98,113].
Indications for treatment (Fig. 3)
Figure 3.
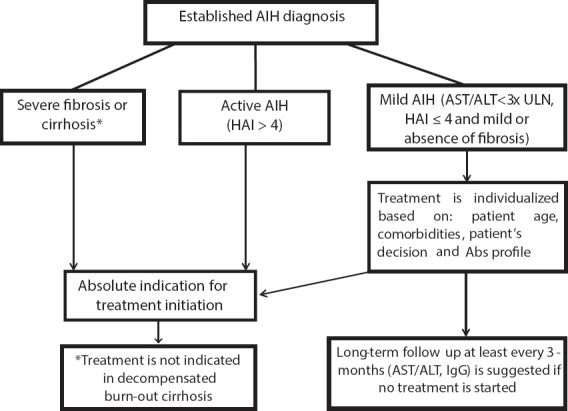
Indications for treatment initiation in defined cases of autoimmune hepatitis (AIH)
ULN, upper limit of normal; Abs, autoantibodies; HAI, histological activity index; AST, aspartate aminotransferase; ALT, alanine aminotransferase; IgG, immunoglobulin G.
Untreated patients with moderate to severe disease (confluent necrosis on biopsy, AST/ALT >5×ULN and IgG >2×ULN) have a poor prognosis, while immunosuppression can improve symptoms and liver biochemistry, including IgG, leading to prolonged survival [114,115]. S pontaneous resolution of AIH may occur and treatment can be withheld. However, because of the fluctuating and unpredictable disease behavior, which carries a considerable risk of subclinical disease progression, these patients should be followed over the long term (3-6 monthly) in order not to miss a later clinical and/or biochemical exacerbation [33,116,117].
Induction therapy
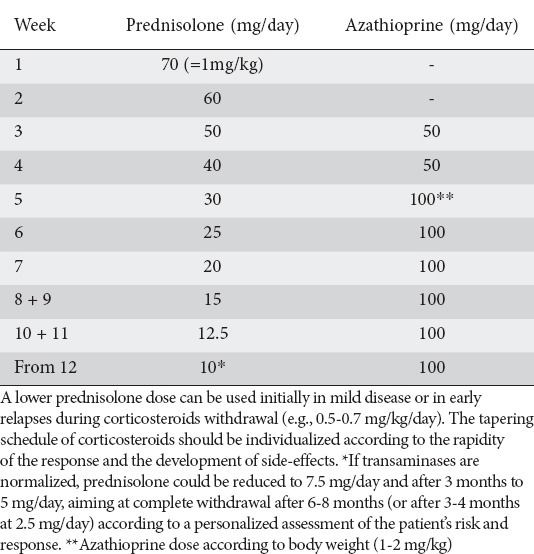
The initial first-line treatment for the induction of disease remission includes prednisolone in an individualized once-daily dose (0.5-1 mg/kg/day), followed usually after two weeks by 50 mg/day azathioprine (if bilirubin is <6 mg/dL) because this combination was associated with significantly fewer side-effects compared with prednisolone monotherapy [7,114,115,118-120]. The rationale of delaying azathioprine initiation is based firstly on resolving diagnostic uncertainties, as transaminases decrease sharply in AIH cases after prednisolone, and secondly to avoid diagnostic challenges between azathioprine hepatotoxicity and primary non-response. Azathioprine is then gradually increased according to the response or its potential toxicity up to 1-2 mg/kg/day. Azathioprine alone should not be used as induction therapy as it has been associated with high mortality rates [6-10,60,118].
STATEMENTS 6-7.
Definition of biochemical remission: Normalization of IgG, AST and ALT values (II-2)
Definition of histological remission: Absence or minimal hepatitis (HAI ≤4) (II-2)
RECOMMENDATIONS 20-22.
AIH therapy should aim to achieve complete biochemical and histological remission in an attempt to prevent potential disease progression (II-2)
All patients having active disease, even those with advanced fibrosis or cirrhosis, should be treated (I)
Treatment can be withheld in patients with spontaneous remission for whom a close long-term follow up is advised in order not to miss an AIH exacerbation (III)
The primary aim should be the achievement of complete clinical and biochemical remission at the lowest corticosteroid dose, or even complete withdrawal using a rapid manner of corticosteroid tapering (Table 7) in order to avoid corticosteroid-dependent disease and development of several significant side-effects. Azathioprine should be used with caution in pregnancy, malignancies, cytopenias and established thiopurine methyltransferase (TPMT) deficiency.
Table 7.
Suggested treatment schedule for adults with recent diagnosis of autoimmune hepatitis (e.g., 70 kg; adapted from [60,115])
Many patients (15-25%) develop side-effects or are intolerant to corticosteroid therapy alone, or in combination with azathioprine [121]. In addition, measurement of TPMT activity or genotyping, along with determination azathioprine of metabolite, are time consuming processes and are not widely available, while they neither provide convincing proof of avoidance of toxicity nor predict the treatment response [122-124]. On the other hand, in a review of 11 randomized controlled trials published from 1950-2009, which included 578 AIH patients (363 treatment-naïve), Lamers et al [115] reported a mean 43% remission rate after prednisolone with or without azathioprine treatment, much lower than those reported in the current literature (approximately 65-80%) [125], suggesting that this kind of treatment is far from ideal. In parallel, a large multicenter study in The Netherlands showed that AIH relapse is almost ubiquitous after treatment withdrawal, even though the patients were in long-term remission (>2 years), further supporting concerns regarding the conventional treatment’s lack of long-term efficacy [126].
Because of these concerns, mycophenolate mofetil (MMF) in combination with prednisolone, or budesonide in combination with azathioprine have been used as first-line induction treatment [13,34,127-134]. MMF blocks purine synthesis, inhibits DNA synthesis and has a selective antiproliferative effect on B- and T-cells. MMF has a 5-fold potent inhibitory effect on the type-II isoform of inosine-5’-monophosphate dehydrogenase, which depletes guanosine nucleotide specifically in activated T- and B-cells without affecting the type-I isoform and thus results in more powerful and selective immunosuppression with few side-effects [135]. In addition, in patients and experimental animal models, it has been shown that MMF-based immunosuppression could restore the regulatory T-cells [136-138], considered very important in AIH pathogenesis [139-141].
In this context, two uncontrolled real-world prospective studies from Greece [34,128], including the largest numbers of treatment-naïve AIH patients ever published (n=59 and n=109), showed that MMF at a dose of 1.5-2 g/day in two divided doses was safe (discontinuation in 3%) and effective as first-line treatment to induce and maintain response with a rapid steroid sparing effect (Fig. 4). In fact, initial complete response was achieved in 88% [34] and 93.6% [128] in a median time of less than 3 months (significantly shorter compared with conventional azathioprine schedules [23,142]), while on treatment complete remission was achieved in 59.3% [34] and 71.6% [128] of patients, compared with the 26% reported by Muratori et al [23,143] and 43% by Lamers et al [115]. Most importantly, a recent study by Zachou et al showed the highest rates of remission maintenance off treatment (72-75%) ever published, for at least a median of 30 months, accompanied by significant improvement in necroinflammatory activity and stable and/or improved fibrosis at second liver biopsy [128,129]. Similar findings independent of the presence of cirrhosis were reported in another retrospective study (84% response rate) in 29 AIH patients [127].
Figure 4.
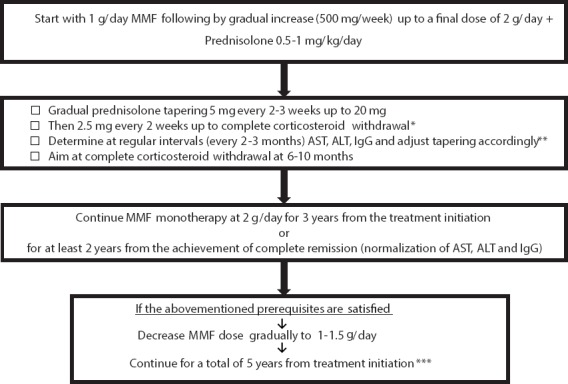
Suggested therapeutic algorithm for prednisolone in combination with mycophenolate mofetil (MMF) in treatment-naïve AIH patients. *In patients with risk factors (e.g., anti-LKM, anti-LC1, anti-α-actinin, anti-SLA/LP, cirrhosis at diagnosis) the tapering schedule could be applied every 3 weeks. **In relapses (↑AST, ALT ± IgG) prednisolone should be increased to the dose of initial complete response and then tapered, either by increasing the time interval twofold or by decreasing the dose of prednisolone tapering by half at the same time. ***In relapses after corticosteroid withdrawal restart prednisolone at the dose of initial complete response and taper according to **. MMF is given in two divided doses
AIH, autoimmune hepatitis; anti-LKM, anti-liver/kidney microsomal antibody; anti-LC1, antibodies against liver cytosol type-1 antigen; anti-SLA/LP, antibodies against soluble liver antigens/liver pancreas; AST, aspartate aminotransferase; ALT, alanine aminotransferase; IgG, immunoglobulin G.
Budesonide has also been used effectively in a randomized study (9 mg/day) in combination with azathioprine in non-cirrhotic AIH patients [130]. Biochemical remission (IgG normalization was not included in the response criteria) without the typical steroid-induced side-effects was found more frequently in budesonide-treated patients compared with the prednisone-treated group (47% vs. 18%), and side-effects were fewer (28% vs. 53%) [130]. However, response rates and side-effects in the control arm were surprisingly lower and higher, respectively, than in earlier studies, presumably because of the initial fixed-dose and fixed-dose reduction schedule in the prednisone group, whereas in the budesonide group the drug was given at a high dose until a response was achieved, thus suggesting a therapeutic bias. In addition, data on the histologic response in budesonide-treated patients are still lacking, whereas other small studies or case reports have shown either failure or exacerbation of AIH during budesonide monotherapy, making the advantages of a more expensive regimen as first-line therapy in AIH uncertain [144-146].
Maintenance therapy
Patients with mild necroinflammatory activity at initial biopsy, intolerant to azathioprine and have achieved complete biochemical response, can receive prednisolone monotherapy at the lowest dose that can maintain remission. In all other patients, the aim should be prednisolone off monotherapy with individualized adjusted azathioprine (2 mg/kg/day), or alternatively MMF doses (1.5-2 g/day) [7,34,115,119,147]. The total duration of immunosuppression should be at least 3 years, with at least the last 2 years having persistent complete biochemical response (normalization of transaminases and IgG). In patients who have received adequate induction and maintenance immunosuppression, but who have not achieved biochemical or histological remission, immunosuppression should not be stopped, as relapse will occur almost universally.
STATEMENTS 8-9.
The long-term efficacy of the conventional treatment is uncertain, as 15-25% of patients develop intolerance or side-effects (II-2)
Long-term biochemical and histological data on budesonide safety and efficacy are lacking (I)
RECOMMENDATIONS 23-27.
Induction treatment for AIH should be individualized and response-guided (II-2)
Prednisolone at one oral dose of 0.5-1 mg/kg/day in the morning, combined with azathioprine at an initial morning dose of 50 mg/dl usually after 2 weeks, if bilirubin is <6 mg/dl, should be the first-line therapy for AIH (I)
Azathioprine should then be increased up to 1-2 mg/kg/day (maintenance dose) (II-2)
In specialized AIH centers, prednisolone (0.5-1 mg/kg/day), combined with MMF (2 g/day) from the beginning of treatment if bilirubin is <6 mg/dL, may be used as first-line therapy, since real-world studies showed high rates of remission maintenance off treatment accompanied by improved liver histology (II-3)
In non-cirrhotic AIH patients, budesonide (9 mg/day) in combination with azathioprine may be used as induction treatment in those with serious comorbidities that might be exacerbated by conventional corticosteroid therapy (II-2)
Relapse of the disease
Relapse of AIH is defined as the reappearance of clinical or laboratory markers of active disease (ALT ≥2-3×ULN and/or an increase in IgG, usually preceded by ALT elevation) [60] after achievement of complete remission during the induction therapy, or during maintenance therapy and/or after complete discontinuation of treatment. In this setting, liver biopsy is usually not recommended. Relapses are particularly frequent with conventional treatment schedules and usually occur 6-12 months after therapy cessation, although a relapse episode may even present many years later [126,148,149]. Remission maintenance is usually associated with a rapid response to previous immunosuppression, with steadily normal transaminases and/or IgG, higher baseline transaminases, no residual necroinflammatory activity on liver histology before treatment withdrawal and longer treatment duration (≥4 years) [7,34,128,150-152].
RECOMMENDATIONS 28-32.
The optimal maintenance treatment should be corticosteroid-free monotherapy with azathioprine, or alternatively MMF (II-2)
Low-dose long-term prednisolone monotherapy may be used to maintain remission only in patients with mild disease and azathioprine intolerance who have achieved complete response after induction therapy (II-2)
Maintenance therapy should be adjusted to a dosage that can maintain persistent biochemical response (normalization of AST, ALT and IgG) (II-2)
Immunosuppression should be given for a total of at least 3 years, and for at least 2 years after the achievement of complete biochemical response (II-2)
Maintenance therapy should not be withdrawn without a complete biochemical or histological response (HAI>3) (II-2)
Treatment of relapses is similar to the initial treatment and is also effective in re-inducing a full response. AIH patients who suffer from multiple relapses develop more side-effects and are likely to have worse outcomes [149,153,154].
Primary treatment endpoints and discontinuation of therapy
The ideal treatment endpoints are a complete clinical, biochemical and histological response with prolonged off treatment remission [7,60,118,143,150,152,153]. In real-life, however, these endpoints are achieved in a minority of patients who discontinue therapy based on prednisolone alone or in combination with azathioprine [115,143], while data on the same issue in budesonide-treated patients are still lacking. In contrast, real-word studies showed high rates of maintained off-treatment remission accompanied by histological improvement in patients treated with prednisolone in combination with MMF as first-line therapy [34,128,129].
RECOMMENDATIONS 33-36.
Patients with AIH should remain under close long-term monitoring after treatment discontinuation, as relapses may occur most commonly in first 6-12 months but even many years later (II-2)
IgG elevation usually precedes transaminase increase in patients with AIH relapse, but liver biopsy is not recommended (II-2)
Treatment of relapses should be similar to the initial treatment schedule; it is also effective in re-inducing full remission (II-2)
Long-term, probably permanent, maintenance treatment should be recommended in AIH patients who have been treated adequately (≥4 years of immunosuppression) but relapse during drug-withdrawal or maintenance treatment (II-2)
Treatment withdrawal can be suggested only in those patients who have achieved continuous complete biochemical remission for at least the last 2 years of treatment, and especially in those with ALT below half the ULN along with IgG <1200 mg/dL [155]. In these patients, liver biopsy before treatment withdrawal is advisable [156]. However, complete treatment withdrawal is almost impossible in difficult-to-treat patients (see below), including cirrhotics and patients with AIH-2.
Follow up before and during treatment
Patients under conventional or budesonide/azathioprine schedules should be followed with baseline and weekly tests for transaminases, albumin, prothrombin time, fasting glucose and full blood count during the first month. In patients under prednisolone/MMF, the above data could be obtained at 2-3–month intervals, along with IgG determination. After corticosteroid tapering, monitoring intervals can be every 3 months and every 3-6 months during maintenance therapy.
STATEMENT 10.
Only a very small proportion of patients stay in remission without maintenance therapy with the conventional treatment regimens (II-2)
RECOMMENDATIONS 37-38.
In AIH patients who have been in persistent complete biochemical remission for at least the last 2 years of immunosuppression, a liver biopsy should be recommended before treatment discontinuation (II-2)
The decision about treatment withdrawal should be based on direct collaboration between patients and doctors (II-2)
Baseline hepatitis B (HBV) and A serology is recommended before treatment, along with the respective vaccination for those not indicating previous vaccination or virus exposure. For HBV surface antigen-positive (HBsAg) patients, preemptive therapy with either entecavir or tenofovir is strongly recommended according to the EASL and the Hellenic Center for Disease Control and Prevention (HCDCP) CPG [157,158]. Vaccination against Streptococcus pneumoniae, along with yearly influenza vaccination, should also be given to all patients.
Dual energy X-ray absorptiometry scanning assessment before treatment initiation and at 1-5-years intervals seems rational, but there are no specific data to support this assertion. Likewise, though no specific data exist concerning the use of calcium and vitamin D in patients under immunosuppression, such treatment seems reasonable, as in other diseases under corticosteroids.
Specific conditions and difficult-to-treat patients
Non-responders
Non-response includes a partial or incomplete response and treatment failure (null response), associated or not with an acute/severe form of the disease.
Partial response
A partial response means that there is some improvement in clinical, biochemical and histological parameters but without reaching complete remission despite treatment adherence. These patients have abnormal transaminases (usually below 2-3×ULN) or necroinflammatory activity on histology [6,7,10,60].
RECOMMENDATIONS 39-40.
Vaccination against hepatitis A, HBV, pneumococcus (particularly in cirrhotics) along with yearly influenza vaccination should be administered to all AIH patients (III)
Bone density determination is recommended at treatment initiation, along with vitamin D supplementation and adequate calcium intake in all patients receiving corticosteroids (II-2)
In partial responders under conventional treatment, an option is to increase azathioprine to 2 mg/kg/day in combination with prednisolone (5-10 mg/kg/day), followed by a repeat liver biopsy after 12-24 months [6,9,10,60]. In patients with a partial response after adequate treatment with budesonide-based schedules, a change to prednisolone (>20 mg/day initially) could be considered [146]. If complete biochemical and histological remission is not achieved, the aim should be either the lowest achievable biochemical activity in parallel with minimum side-effects, or the administration of alternative second-line therapeutic agents [159].
Treatment failure
Primary complete biochemical remission after adequate treatment initiation is the rule (90-95% of patients); therefore, reassessment of diagnosis and treatment adherence should be considered in non-responders. Non-response is not well-defined, but usually the absence of a transaminase decline of at least 25% from baseline after 2-3 weeks should be considered as non-response. It is also important to remember that other conditions may develop concurrently during the AIH course, such as viral infections or DILI, which if unrecognized, could be mistakenly regarded as a null response or flares [71,72,160,161].
Treatment failure can be seen either in patients with an acute/severe or even fulminant disease form, or in those without such intense severity. Data on patients with acute/severe presentation are scarce, consisting mostly of real-life non-randomized studies with a small number of patients and varying, mostly arbitrary entry criteria, because the precise definition of this form of AIH is still missing [112,162-171]. Therefore, the role and timing of corticosteroids in modifying the outcome of acute/severe AIH remains unclear, as it is ambiguous whether such patients should be given a corticosteroids trial, a priority listing for liver transplantation, or both. Potts and Verma recently reviewed five retrospective studies, each with a small number of patients, including in total 85 patients with AIH-related acute liver failure [170]. Sixty-nine patients (89.2%) received immunosuppression, mostly oral corticosteroids, and had remission rates of 8.3-50%, while 43.5% underwent or were listed for liver transplantation and 33% died. The largest recent studies in acute/severe AIH come from France (n=104) and Greece (n=42) [112,171]. In the multicenter retrospective French study, an overall survival rate of 90% was reported (median follow up: 2.3 years), although early liver transplantation was required in one third of patients. The beneficial effect of corticosteroids was observed in 66% of patients, mainly in those with low international normalized ratio (INR) at baseline and improvement in liver function during the first week of treatment [171]. In the Greek study, high-dose intravenous corticosteroids were given (prednisolone 1.5 mg/kg/day) in the early stages of acute/severe AIH, defined as an acute presentation without any sign of hepatic encephalopathy and transaminases >10×ULN, INR ≥1.5 and bilirubin ≥4 mg/dL at any time during the acute course [112]. This management appeared to prevent disease deterioration without increasing morbidity and mortality (long-term overall survival without transplantation: 95.2%; median follow up: 5.3 years).
Conclusively, despite the low level of evidence, the available data indicate that all patients with acute/severe AIH should be considered for a corticosteroid trial at the earliest opportunity (the sooner the better), using high doses of prednisolone (>1 mg/kg/day) intravenously [172]. Failure to improve within 7 days should lead to emergency listing for liver transplantation [167]. The prophylactic use of antibiotics/antifungals is not supported by the most recent studies [112,171], but they should be kept in mind and may be justified at an individualized basis.
The other form of treatment failure without intense severity is characterized by minimal, or even no improvement in the clinical and biochemical parameters after several weeks of standard regimen, despite confirmation of diagnosis and treatment adherence. In these patients, determination of active azathioprine metabolites, such as thioguanine nucleotides (TGN), could be helpful in revealing a lack of adherence to treatment or an altered azathioprine metabolism, although the therapeutic range of TGN levels is not precisely known in AIH [173]. As endorsed by EASL, AASLD and the British Society of Gastroenterology GPG [6,10,60], an increase of prednisolone for at least one month and azathioprine to the maximum doses (1 mg/kg/day and 2 mg/kg/day, respectively) seems rational. However, despite this intense treatment strategy, most patients may not respond, while they carry increased risks for drug-related side-effects. Therefore, management by expert centers should be suggested as soon as possible for these patients.
STATEMENT 11.
Definition of the acute/severe form of AIH is an urgent unmet need (I)
RECOMMENDATIONS 41-47.
In partial responders under a conventional regimen, an increase of the azathioprine dose to 2 mg/kg/day in combination with 5-10 mg/kg/day prednisolone is recommended (II-3)
In partial responders under a budesonide-based regimen, a change to prednisolone (>20 mg/day) could be considered (III)
In partial responders not able to achieve complete remission despite the above options, the goal should be the lowest achievable biochemical activity with a minimum of side-effects, or administration of alternative second-line therapeutic agents after consultation at a specialized center (II-3)
Failure of primary complete biochemical remission after adequate treatment should raise strong suspicion of misdiagnosis or non-compliance with therapy (II-2)
All AIH patients presenting with the acute/severe form of the disease should be considered for a high-dose corticosteroid trial (>1 mg/kg/day) at the earliest opportunity (the sooner the better), and preferably intravenously, but failure to improve within 7 days should lead to emergency listing for liver transplantation (II-3)
In non-responders without intense severity, prednisolone and azathioprine at the maximum dosage (1 mg/kg/day and 2 mg/kg/day, respectively) could be tried, followed by management at expert centers in the case of non-response (II-2)
Determination of TGN levels could help the redesign of treatment strategy, as undetectable TGN may indicate altered azathioprine metabolism or non-compliance, while high TGN levels may suggest toxicity (II-2)
Non-adherence
Non-adherence to treatment is an important problem during long-term follow up, particularly among children and adolescents under corticosteroids, resulting in frequent relapses or flares of AIH [174,175]. The management of non-compliance is difficult; therefore, a multidisciplinary approach is needed, including psychologists, social and youth workers, health carers, committed nurses, and pediatric and adult hepatologists in an attempt to re-motivate the young patient [176].
In addition, high rates of depression and anxiety have recently been reported in AIH patients [27] Thus, considerable attention is needed for those not appropriately followed for the psychiatry compartment, because this behavior could cause an increased frequency of non-adherence, leading to these patients erroneously being considered as non-responders and candidates for alternative therapies, with unexpected consequences [177].
RECOMMENDATIONS 48-50.
Treatment adherence should be of outmost importance for all patients and especially for children, adolescents and young adults (II-2)
The transition from childhood to adult care should be based on a multidisciplinary approach by special transition services (II-3)
Considerable attention should be given to patients with anxiety or depression in order to be sure that the psychiatric follow up and treatment are appropriate before appraising these patients as non-responders to AIH therapy (III)
Intolerance to and side-effects of treatment
Corticosteroid side-effects are numerous and develop in up to 80% of patients receiving steroid monotherapy for more than 2 years, mainly at doses >15 mg/day. However, corticosteroid discontinuation because of severe adverse events is observed in 15%. Combination with azathioprine is associated with a much lower rate of side-effects [112,147]. In non-cirrhotic prednisolone responders who nevertheless develop side-effects, even though azathioprine has been increased to the highest dose, a switch to budesonide could be suggested.
Azathioprine side-effects occur in about 25% of AIH patients, accompanied by drug withdrawal in approximately 10-15%. In patients intolerant to or with side-effects from azathioprine (bone marrow suppression, nausea, vomiting, pancreatitis, etc.), a switch to MMF (2 g/day) with subsequent prednisolone tapering appears to be an excellent alternative [178-186]. Other alternatives are steroid monotherapy in patients with mild disease, budesonide, mercaptopurine or thioguanine, tacrolimus, ciclosporin, methotrexate, cyclophosphamide, allopurinol, and biologic regimens, including tumor necrosis factor α (TNFa) blockade agents and rituximab [187-194].
RECOMMENDATIONS 51-54.
In patients intolerant to azathioprine, MMF should be the second-line treatment (II-2)
Mercaptopurine or thioguanine could also be an alternative option (III)
If adequate conventional treatment with azathioprine cannot maintain remission in corticosteroid responders who nevertheless have severe steroid side-effects, switching to budesonide may be considered (II-3)
In partial or non-responders after adequate conventional treatment, alternative therapies with ciclosporin or tacrolimus, methotrexate, cyclophosphamide, rituximab or TNFa blockade agents may be initiated only at specialized centers, although their effectiveness has not been investigated in proper clinical trials (II-3)
Non liver-related comorbidities and aging
Approximately one third of older AIH patients (>65 years) already have cirrhosis or advanced fibrosis at diagnosis, although they are more frequently asymptomatic at presentation compared to younger patients [25,27,33,195]. These patients achieve biochemical response more frequently and have a higher prevalence of concurrent autoimmune diseases compared with younger patients [25,196,197].
In asymptomatic elderly patients with mild disease, the decision about treatment initiation could be based on the presence and the severity of other comorbidities, such as uncontrolled diabetes mellitus, refractory arterial hypertension, established osteoporosis or a previous or current history of psychosis. In this context, it is better to choose a watch-and-wait strategy, but close follow up of these patients is strongly advised. Although there is no convincing data concerning the management of elderly AIH patients with mild disease and no severe comorbidities [33,116,197], it seems rational to initiate immunosuppression using a lower starting prednisolone dose (0.5 mg/kg/day), followed by a more rapid steroid de-escalation schedule in combination with azathioprine (1-2 mg/kg/day). Another attractive option for these patients without cirrhosis may be the use of budesonide (9 mg/day) plus azathioprine.
In elderly patients with at least moderate necroinflammatory activity, treatment is recommended, but again the choice of steroid therapy and the tapering schedule should be considered carefully. The same is true for all AIH patients, irrespective of age, who have concurrent severe comorbidities.
RECOMMENDATIONS 55-56.
Treatment is recommended in elderly patients with at least moderate necroinflammatory activity. In the presence of other comorbidities, the type of steroid therapy and the tapering schedule should be considered carefully in all ages (II-3)
In asymptomatic elderly patients with mild interface activity and comorbidities it is better to watch and wait, but close long-term follow up is strongly advised (II-3)
AIH variants
Although controlled trials are lacking, the recent EASL CPG for PBC have recommended adding immunosuppression to UDCA in previously well-established PBC cases if at least moderate interface hepatitis is present on liver biopsy [62,198-200]. Notably, these patients appear to respond to lower immunosuppression dosages and maintain remission after treatment withdrawal at higher rates than patients with AIH alone [198,199]. It is uncertain whether AIH patients who develop PBC features will benefit from UDCA administration, but this addition seems logical under real-life conditions, particularly in young patients, because of the potential long-term benefit of UDCA, which may subsequently protect the patients from the development of ductopenia and biliary cirrhosis during their lifetime.
Considering the AIH-PSC variant, again there are no controlled trials concerning its management. A combination treatment consisting of immunosuppression and UDCA has been suggested and response criteria have recently been published for autoimmune sclerosing cholangitis, the pediatric form of the variant [69].
However, although biochemical and histological parameters may improve, the biliary tract lesions may progress and therefore the outcome of these patients seems worse compared to those with only AIH [63,64]. The combination of UDCA and immunosuppression has also been proposed by EASL CPG for the adults with AIH-PSC variant [201], although the available but inadequate studies show that the long-term prognosis appears worse than for either AIH cases without PSC characteristics or PSC alone [66,202,203].
RECOMMENDATIONS 57-58.
In patients with the AIH-PBC variant, a combination of immunosuppression with UDCA is recommended; alternatively, if AIH is the dominant compartment, immunosuppression only should be started and UDCA could be added if remission is not achieved (III)
In patients with the AIH-PSC variant, the addition of UDCA to immunosuppressive treatment can be considered (III)
Management of AIH in pregnancy
Large series of pregnant AIH patients from the United Kingdom [37], Germany [204] and Sweden [205] have shown that the new or continued administration of azathioprine had no significant impact on the rate of live birth, termination or miscarriage, or on the gestational period. Interestingly, some unexplained adverse outcomes were found to be associated with anti-SLA/LP and anti-Ro52 detection [204], while a higher Cesarean section rate was recorded in Sweden [205], but again without higher stillbirth or fetal malformation rates compared to controls. Taken together, these findings suggest that the continuation of azathioprine in females with well-established AIH after conception appears rational and justified.
As discussed previously, AIH may also present for the first time during pregnancy or more frequently after delivery [37-39]. These cases should be treated as discussed previously for non-pregnant patients. However, as the disease during pregnancy usually has lower activity, a minimal adjustment of immunosuppression (5-10 mg/day prednisolone ± 50-75 mg/day azathioprine) in previously diagnosed patients receiving treatment seems rational. Immunosuppressive treatment should then be increased after delivery to the previous dosages, in order to minimize the risk of flare during post-partum. Complications seem to be more frequent for those patients who have not achieved complete biochemical remission at least one year before conception, while cirrhotic patients carry a high risk of adverse outcomes. Although data regarding breastfeeding in AIH females under azathioprine are limited, the drug is considered safe, despite the fact that small amounts of its metabolite can be detected in breast milk [206].
RECOMMENDATIONS 59-62.
Females with AIH in remission should be advised that they have no contraindication for pregnancy or breastfeeding (II-2)
Maintenance treatment with prednisolone with or without azathioprine should be continued in previously diagnosed females under therapy (II-2)
Mild flares can be observed during the first trimester and more frequently especially in the post-partum period, requiring an increase in immunosuppression (II-2)
MMF should be stopped at least 3 months prior to conception (either in females or males under treatment), as this drug is absolutely contraindicated in pregnancy (II-2)
Management of AIH after liver transplantation
Recurrence of AIH has been reported in 20-25% of patients [207] and is usually managed with the standard prednisolone treatment schedules in combination with azathioprine or MMF [208]. Non-responders in this setting could be aided by the use of sirolimus [209]. De novo AIH has been described in approximately 5% of subjects transplanted for reasons unrelated to AIH [53,207] and its management is identical to that suggested for recurrent AIH [210].
RECOMMENDATION 63.
AIH after liver transplantation, either recurrent or de novo, should be managed by the basic treatment principles of AIH (II-3)
Liver-related comorbidities
In countries with a moderate to high prevalence of HBV or HCV infections, the coexistence of AIH with chronic viral hepatitis is not impossible [211-213]. On the other hand, AIH patients can contract viral hepatitis. In these cases, AIH may be overlooked, as the absence of viral hepatitis markers is one of the 4 essential parameters of the simplified criteria for AIH diagnosis [19]. AIH in this situation seems to be more aggressive and carries a poorer prognosis compared to chronic viral hepatitis alone, as AIH could remain untreated in the long term because of its underdiagnosis/misdiagnosis [212]. In patients with chronic HBV infection and characteristics of AIH at diagnosis, HBV should be treated first according to the EASL and HCDCP CPG [157,158] and the need for AIH treatment should be reevaluated after viral suppression. Alternatively, in cases with moderate to severe necroinflammatory activity, immunosuppressive and antiviral treatment could be initiated in parallel. Likewise, in HCV patients with AIH features, DAAs without IFNa should be used first and initiation of immunosuppression could be started after HCV eradication if necroinflammatory activity persists.
Development of AIH has rarely been reported in human immunodeficiency virus (HIV) infection after the administration of highly active antiretroviral therapy [214,215]. Standard immunosuppression seems safe and effective in inducing remission, without significant complications or development of opportunistic infections [215]. However, as life-threatening infections can indeed be observed, treatment of AIH in this setting should be individualized.
Non-alcoholic fatty liver disease (NAFLD) has become the most common chronic liver disease in the western world (prevalence: 20-30%). Non-alcoholic steatohepatitis (NASH), with steatosis, hepatocyte ballooning and lobular inflammation, affects 3-5% of the population and can progress to severe liver fibrosis and cirrhosis [216,217]. The prevalence of NAFLD/NASH and its impact on treatment outcome and response in confirmed AIH patients are largely unknown. Obesity worsens the course and treatment response of other autoimmune diseases, such as rheumatoid arthritis, systemic lupus erythematosus, inflammatory bowel disease and psoriasis [218], and pre-existing NAFLD seems to potentiate the severity of AIH in the CYP2D6 mouse model [219]. So far, there is only one small retrospective study indicating that patients with concurrent AIH and NASH (but not simple steatosis) are more likely to present with advanced disease associated with adverse clinical outcomes and decreased survival [220]. Therefore, NAFLD/NASH in this setting should be treated strictly and intensely according to current recommendations [216,217], while efforts should be made to use the lowest effective dose of steroids [221].
RECOMMENDATIONS 64-67.
In AIH patients with concurrent chronic HBV or HCV at diagnosis, the viral infections should be treated first and AIH therapy could be offered after HBV suppression or HCV eradication if the necroinflammatory activity persists (III)
In AIH patients who contracted HBV or HCV infections during the AIH course, antiviral treatment with entecavir/tenofovir or DAAs, respectively, is recommended without stopping immunosuppression (III)
In HIV patients with AIH, treatment should be given on an individualized basis, as standard immunosuppression seems to be safe and effective but carries a risk of life threatening infections (III)
In AIH patients with NAFLD/NASH, efforts should be made to ensure strict adherence to NAFLD/NASH guidelines and the use of the lowest effective dose of steroids for AIH, although the impact of NAFLD/NASH on treatment outcome and response in AIH is unknown (III)
Concluding remarks
AIH is characterized by genetic, clinical, laboratory, histological and serological heterogeneity and therefore, it might be underestimated or unrecognized. Its diagnosis is based on the presence of polyclonal hypergammaglobulinemia, circulating autoantibodies, interface hepatitis on liver histology, absence of viral hepatitis and a favorable response to immunosuppression. In particular, autoantibodies detection and the interpretation of histological findings are considered the hallmark for a timely diagnosis. Most of the affected patients are treated very efficiently with at least near normal life expectancy and quite good quality of life. However, many patients still have experience of remarkable morbidity because of delayed or missed diagnosis, drugs intolerance and side-effects, partial treatment response or flares, poor management and poor adherence. The establishment of major centers bearing special expertise on this disease diagnosis and control will be a governing factor in improving management of patients. Also, research on AIH etiology and its underlying pathogenetic mechanisms will be the clue to improve therapy of AIH. So far, most patients need long-life immunosuppressive treatment but patients want cure, not only remission of the disease. In an attempt to achieve curative treatment, we have to work hard together with basic scientists and follow developments in immunology and autoimmunity.
Biography
Institute of Internal Medicine and Hepatology, Larissa; University Hospital of Larissa; National and Kapodistrian University of Athens, “Hippokratio” General Hospital of Athens, Athens; Medical School of National and Kapodistrian University of Athens, “Laiko” General Hospital of Athens, Athens, Greece
Footnotes
Conflict of Interest: None.
References
- 1.Waldenström J. Leber. Blutproteine und Nahrungseiweiss. Deutsch Z Verdau Stoffwechselkr. 1950;15:113–119. [PubMed] [Google Scholar]
- 2.Cowling DC, Mackay IR, Taft LI. Lupoid hepatitis. Lancet. 1956;268:1323–1326. doi: 10.1016/s0140-6736(56)91483-0. [DOI] [PubMed] [Google Scholar]
- 3.Mackay IR, Weiden S, Hasker J. Autoimmune hepatitis. Ann NY Acad Sci. 1965;124:767–780. doi: 10.1111/j.1749-6632.1965.tb19000.x. [DOI] [PubMed] [Google Scholar]
- 4.Johnson PJ, McFarlane IG. Meeting report:International Autoimmune Hepatitis Group. Hepatology. 1993;18:998–1005. doi: 10.1002/hep.1840180435. [DOI] [PubMed] [Google Scholar]
- 5.Shaneyfelt TM, Mayo-Smith MF, Rothwangl J. Are guidelines following guidelines?The methodological quality of clinical practice guidelines in the peer-reviewed medical literature. JAMA. 1999;281:1900–1905. doi: 10.1001/jama.281.20.1900. [DOI] [PubMed] [Google Scholar]
- 6.Manns MP, Czaja AJ, Gorham JD, et al. American Association for the Study of Liver Diseases. Diagnosis and management of autoimmune hepatitis. Hepatology. 2010;51:2193–2213. doi: 10.1002/hep.23584. [DOI] [PubMed] [Google Scholar]
- 7.Zachou K, Muratori P, Koukoulis GK, et al. Review article:autoimmune hepatitis —current management and challenges. Aliment Pharmacol Ther. 2013;38:887–913. doi: 10.1111/apt.12470. [DOI] [PubMed] [Google Scholar]
- 8.Gatselis NK, Zachou K, Koukoulis GK, Dalekos GN. Autoimmune hepatitis, one disease with many faces:etiopathogenetic, clinico-laboratory and histological characteristics. World J Gastroenterol. 2015;21:60–83. doi: 10.3748/wjg.v21.i1.60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gleeson D, Heneghan MA British Society of Gastroenterology. British Society of Gastroenterology (BSG) guidelines for management of autoimmune hepatitis. Gut. 2011;60:1611–1629. doi: 10.1136/gut.2010.235259. [DOI] [PubMed] [Google Scholar]
- 10.Mieli-Vergani G, Vergani D, Czaja AJ, et al. Autoimmune hepatitis. Nat Rev Dis Primers. 2018;4:18017. doi: 10.1038/nrdp.2018.17. [DOI] [PubMed] [Google Scholar]
- 11.Werner M, Prytz H, Ohlsson B, et al. Epidemiology and the initial presentation of autoimmune hepatitis in Sweden:a nationwide study. Scand J Gastroenterol. 2008;43:1232–1240. doi: 10.1080/00365520802130183. [DOI] [PubMed] [Google Scholar]
- 12.Ngu JH, Bechly K, Chapman BA, et al. Population-based epidemiology study of autoimmune hepatitis:a disease of older women? J Gastroenterol Hepatol. 2010;25:1681–1686. doi: 10.1111/j.1440-1746.2010.06384.x. [DOI] [PubMed] [Google Scholar]
- 13.Delgado JS, Vodonos A, Malnick S, et al. Autoimmune hepatitis in southern Israel:a 15-year multicenter study. J Dig Dis. 2013;14:611–618. doi: 10.1111/1751-2980.12085. [DOI] [PubMed] [Google Scholar]
- 14.van Gerven NM, Verwer BJ, Witte BI, et al. Dutch Autoimmune hepatitis STUDY group. The epidemiology and clinical characteristics of autoimmune hepatitis in the Netherlands. Scand J Gastroenterol. 2014;49:1245–1254. doi: 10.3109/00365521.2014.946083. [DOI] [PubMed] [Google Scholar]
- 15.Grønbæk L, Vilstrup H, Jepsen P. Autoimmune hepatitis in Denmark:incidence, prevalence, prognosis, and causes of death. A nationwide registry-based cohort study. J Hepatol. 2014;60:612–617. doi: 10.1016/j.jhep.2013.10.020. [DOI] [PubMed] [Google Scholar]
- 16.Wong RJ, Gish R, Frederick T, Bzowej N, Frenette C. The impact of race/ethnicity on the clinical epidemiology of autoimmune hepatitis. J Clin Gastroenterol. 2012;46:155–161. doi: 10.1097/MCG.0b013e318228b781. [DOI] [PubMed] [Google Scholar]
- 17.Czaja AJ. Autoimmune hepatitis in diverse ethnic populations and geographical regions. Expert Rev Gastroenterol Hepatol. 2013;7:365–385. doi: 10.1586/egh.13.21. [DOI] [PubMed] [Google Scholar]
- 18.Alvarez F, Berg PA, Bianchi FB, et al. International Autoimmune Hepatitis Group Report:review of criteria for diagnosis of autoimmune hepatitis. J Hepatol. 1999;31:929–938. doi: 10.1016/s0168-8278(99)80297-9. [DOI] [PubMed] [Google Scholar]
- 19.Hennes EM, Zeniya M, Czaja AJ, et al. International Autoimmune Hepatitis Group. Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology. 2008;48:169–176. doi: 10.1002/hep.22322. [DOI] [PubMed] [Google Scholar]
- 20.Rigopoulou EI, Dalekos G, Bogdanos DP. How common are connective tissue disorders in patients with autoimmune hepatitis? Semin Arthritis Rheum. 2007;36:332. doi: 10.1016/j.semarthrit.2006.11.005. [DOI] [PubMed] [Google Scholar]
- 21.Teufel A, Weinmann A, Kahaly GJ, et al. Concurrent autoimmune diseases in patients with autoimmune hepatitis. J Clin Gastroenterol. 2010;44:208–213. doi: 10.1097/MCG.0b013e3181c74e0d. [DOI] [PubMed] [Google Scholar]
- 22.Obermayer-Straub P, Perheentupa J, Braun S, et al. Hepatic autoantigens in patients with autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. Gastroenterology. 2001;121:668–677. doi: 10.1053/gast.2001.27103. [DOI] [PubMed] [Google Scholar]
- 23.Muratori P, Granito A, Quarneti C, et al. Autoimmune hepatitis in Italy:the Bologna experience. J Hepatol. 2009;50:1210–1218. doi: 10.1016/j.jhep.2009.01.020. [DOI] [PubMed] [Google Scholar]
- 24.Peng M, Li Y, Zhang M, et al. Clinical features in different age groups of patients with autoimmune hepatitis. Exp Ther Med. 2014;7:145–148. doi: 10.3892/etm.2013.1363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Al-Chalabi T, Boccato S, Portmann BC, McFarlane IG, Heneghan MA. Autoimmune hepatitis (AIH) in the elderly:a systematic retrospective analysis of a large group of consecutive patients with definite AIH followed at a tertiary referral centre. J Hepatol. 2006;45:575–583. doi: 10.1016/j.jhep.2006.04.007. [DOI] [PubMed] [Google Scholar]
- 26.Grønbæk L, Vilstrup H, Pedersen L, Christensen K, Jepsen P. Family occurrence of autoimmune hepatitis:A Danish nationwide registry-based cohort study. J Hepatol. 2018;69:873–877. doi: 10.1016/j.jhep.2018.05.035. [DOI] [PubMed] [Google Scholar]
- 27.Schramm C, Wahl I, Weiler-Normann C, et al. Health-related quality of life, depression, and anxiety in patients with autoimmune hepatitis. J Hepatol. 2014;60:618–624. doi: 10.1016/j.jhep.2013.10.035. [DOI] [PubMed] [Google Scholar]
- 28.Stravitz RT, Lefkowitch JH, Fontana RJ, et al. Acute Liver Failure Study Group. Autoimmune acute liver failure:proposed clinical and histological criteria. Hepatology. 2011;53:517–526. doi: 10.1002/hep.24080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Muratori P, Carbone M, Stangos G, et al. Clinical and prognostic implications of acute onset of autoimmune hepatitis:An Italian multicentre study. Dig Liver Dis. 2018;50:698–702. doi: 10.1016/j.dld.2018.02.015. [DOI] [PubMed] [Google Scholar]
- 30.Joshita S, Yoshizawa K, Umemura T, et al. Japan Autoimmune Hepatitis Study Group (JAIHSG) Clinical features of autoimmune hepatitis with acute presentation:a Japanese nationwide survey. J Gastroenterol. 2018;53:1079–1088. doi: 10.1007/s00535-018-1444-4. [DOI] [PubMed] [Google Scholar]
- 31.Takahashi H, Zeniya M. Acute presentation of autoimmune hepatitis:Does it exist?A published work review. Hepatol Res. 2011;41:498–504. doi: 10.1111/j.1872-034X.2011.00808.x. [DOI] [PubMed] [Google Scholar]
- 32.Karkhanis J, Verna EC, Chang MS, et al. Acute Liver Failure Study Group. Steroid use in acute liver failure. Hepatology. 2014;59:612–621. doi: 10.1002/hep.26678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Feld JJ, Dinh H, Arenovich T, Marcus VA, Wanless IR, Heathcote EJ. Autoimmune hepatitis:effect of symptoms and cirrhosis on natural history and outcome. Hepatology. 2005;42:53–62. doi: 10.1002/hep.20732. [DOI] [PubMed] [Google Scholar]
- 34.Zachou K, Gatselis N, Papadamou G, Rigopoulou EI, Dalekos GN. Mycophenolate for the treatment of autoimmune hepatitis:prospective assessment of its efficacy and safety for induction and maintenance of remission in a large cohort of treatment-naïve patients. J Hepatol. 2011;55:636–646. doi: 10.1016/j.jhep.2010.12.032. [DOI] [PubMed] [Google Scholar]
- 35.Landeira G, Morise S, Fassio E, et al. Effect of cirrhosis at baseline on the outcome of type 1 autoimmune hepatitis. Ann Hepatol. 2012;11:100–106. [PubMed] [Google Scholar]
- 36.Ngu JH, Gearry RB, Frampton CM, Stedman CA. Predictors of poor outcome in patients with autoimmune hepatitis:a population-based study. Hepatology. 2013;57:2399–2406. doi: 10.1002/hep.26290. [DOI] [PubMed] [Google Scholar]
- 37.Westbrook RH, Yeoman AD, Kriese S, Heneghan MA. Outcomes of pregnancy in women with autoimmune hepatitis. J Autoimmun. 2012;38:J239–J244. doi: 10.1016/j.jaut.2011.12.002. [DOI] [PubMed] [Google Scholar]
- 38.Terrabuio DR, Abrantes-Lemos CP, Carrilho FJ, Cançado EL. Follow-up of pregnant women with autoimmune hepatitis:the disease behavior along with maternal and fetal outcomes. J Clin Gastroenterol. 2009;43:350–356. doi: 10.1097/MCG.0b013e318176b8c5. [DOI] [PubMed] [Google Scholar]
- 39.Danielsson Borssén, Wallerstedt S, Nyhlin N, et al. Pregnancy and childbirth in women with autoimmune hepatitis is safe, even in compensated cirrhosis. Scand J Gastroenterol. 2016;51:479–485. doi: 10.3109/00365521.2015.1115893. [DOI] [PubMed] [Google Scholar]
- 40.Castiella A, Zapata E, Lucena MI, Andrade RJ. Drug-induced autoimmune liver disease:a diagnostic dilemma of an increasingly reported disease. World J Hepatol. 2014;6:160–168. doi: 10.4254/wjh.v6.i4.160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Appleyard S, Saraswati R, Gorard DA. Autoimmune hepatitis triggered by nitrofurantoin:a case series. J Med Case Rep. 2010;4:311. doi: 10.1186/1752-1947-4-311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Saitis A, Gatselis N, Zachou K, Dalekos GN. Use of TNFαantagonists in refractory AIH:revealing the unforeseen. J Hepatol. 2013;59:197–198. doi: 10.1016/j.jhep.2013.02.029. [DOI] [PubMed] [Google Scholar]
- 43.Kern E, VanWagner LB, Yang GY, Rinella ME. Liraglutide-induced autoimmune hepatitis. JAMA Intern Med. 2014;174:984–987. doi: 10.1001/jamainternmed.2014.674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Arvaniti P, Zachou K, Koukoulis GK, Dalekos GN. Postinfantile giant cell hepatitis with features of acute severe autoimmune hepatitis probably triggered by diclofenac in a patient with primary myelofibrosis. Case Reports Hepatol. 2018;2018:9793868. doi: 10.1155/2018/9793868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Suzuki A, Brunt EM, Kleiner DE, et al. The use of liver biopsy evaluation in discrimination of idiopathic autoimmune hepatitis versus drug-induced liver injury. Hepatology. 2011;54:931–939. doi: 10.1002/hep.24481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Fontana RJ, Seeff LB, Andrade RJ, et al. Standardization of nomenclature and causality assessment in drug-induced liver injury:summary of a clinical research workshop. Hepatology. 2010;52:730–742. doi: 10.1002/hep.23696. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Björnsson E, Talwalkar J, Treeprasertsuk S, et al. Drug-induced autoimmune hepatitis:clinical characteristics and prognosis. Hepatology. 2010;51:2040–2048. doi: 10.1002/hep.23588. [DOI] [PubMed] [Google Scholar]
- 48.Chalasani N, Fontana RJ, Bonkovsky HL, et al. Drug Induced Liver Injury Network (DILIN) Causes, clinical features, and outcomes from a prospective study of drug-induced liver injury in the United States. Gastroenterology. 2008;135:1924-1934–1934.e1-e4. doi: 10.1053/j.gastro.2008.09.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Vento S, Cainelli F. Is there a role for viruses in triggering autoimmune hepatitis? Autoimmun Rev. 2004;3:61–69. doi: 10.1016/S1568-9972(03)00053-3. [DOI] [PubMed] [Google Scholar]
- 50.Zellos A, Spoulou V, Roma-Giannikou E, Karentzou O, Dalekos GN, Theodoridou M. Autoimmune hepatitis type-2 and Epstein-Barr virus infection in a toddler:Art of facts or an artifact? Ann Hepatol. 2013;12:147–151. [PubMed] [Google Scholar]
- 51.Dalekos GN, Wedemeyer H, Obermayer-Straub P, et al. Epitope mapping of cytochrome P4502D6 autoantigen in patients with chronic hepatitis C during alpha-interferon treatment. J Hepatol. 1999;30:366–375. doi: 10.1016/s0168-8278(99)80092-0. [DOI] [PubMed] [Google Scholar]
- 52.Mieli-Vergani G, Vergani D. De novo autoimmune hepatitis after liver transplantation. J Hepatol. 2004;40:3–7. doi: 10.1016/j.jhep.2003.10.022. [DOI] [PubMed] [Google Scholar]
- 53.Montano-Loza AJ, Vargas-Vorackova F, Ma M, et al. Incidence and risk factors associated with de novo autoimmune hepatitis after liver transplantation. Liver Int. 2012;32:1426–1433. doi: 10.1111/j.1478-3231.2012.02832.x. [DOI] [PubMed] [Google Scholar]
- 54.Kwon JH, Hanouneh IA, Allende D, et al. De novo autoimmune hepatitis following liver transplantation. Transplant Proc. 2018;50:1451–1456. doi: 10.1016/j.transproceed.2018.02.066. [DOI] [PubMed] [Google Scholar]
- 55.Teufel A, Weinmann A, Centner C, et al. Hepatocellular carcinoma in patients with autoimmune hepatitis. World J Gastroenterol. 2009;15:578–582. doi: 10.3748/wjg.15.578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Yeoman AD, Al-Chalabi T, Karani JB, et al. Evaluation of risk factors in the development of hepatocellular carcinoma in autoimmune hepatitis:implications for follow-up and screening. Hepatology. 2008;48:863–870. doi: 10.1002/hep.22432. [DOI] [PubMed] [Google Scholar]
- 57.Ngu JH, Gearry RB, Frampton CM, Stedman CA. Mortality and the risk of malignancy in autoimmune liver diseases:a population-based study in Canterbury, New Zealand. Hepatology. 2012;55:522–529. doi: 10.1002/hep.24743. [DOI] [PubMed] [Google Scholar]
- 58.Migita K, Watanabe Y, Jiuchi Y, et al. Japanese NHO-Liver-network study group. Hepatocellular carcinoma and survival in patients with autoimmune hepatitis (Japanese National Hospital Organization-autoimmune hepatitis prospective study) Liver Int. 2012;32:837–844. doi: 10.1111/j.1478-3231.2011.02734.x. [DOI] [PubMed] [Google Scholar]
- 59.Boberg KM, Chapman RW, Hirschfield GM, Lohse AW, Manns MP, Schrumpf E International Autoimmune Hepatitis Group. Overlap syndromes:the International Autoimmune Hepatitis Group (IAIHG) position statement on a controversial issue. J Hepatol. 2011;54:374–385. doi: 10.1016/j.jhep.2010.09.002. [DOI] [PubMed] [Google Scholar]
- 60.European Association for the Study of the Liver. EASL Clinical Practice Guidelines:Autoimmune hepatitis. J Hepatol. 2015;63:971–1004. doi: 10.1016/j.jhep.2015.06.030. [DOI] [PubMed] [Google Scholar]
- 61.Chazouillères O, Wendum D, Serfaty L, Montembault S, Rosmorduc O, Poupon R. Primary biliary cirrhosis-autoimmune hepatitis overlap syndrome:clinical features and response to therapy. Hepatology. 1998;28:296–301. doi: 10.1002/hep.510280203. [DOI] [PubMed] [Google Scholar]
- 62.European Association for the Study of the Liver. EASL Clinical Practice Guidelines:The diagnosis and management of patients with primary biliary cholangitis. J Hepatol. 2017;67:145–172. doi: 10.1016/j.jhep.2017.03.022. [DOI] [PubMed] [Google Scholar]
- 63.Gregorio GV, Portmann B, Karani J, et al. Autoimmune hepatitis/sclerosing cholangitis overlap syndrome in childhood:a 16-year prospective study. Hepatology. 2001;33:544–553. doi: 10.1053/jhep.2001.22131. [DOI] [PubMed] [Google Scholar]
- 64.Rojas CP, Bodicharla R, Campuzano-Zuluaga G, Hernandez L, Rodriguez MM. Autoimmune hepatitis and primary sclerosing cholangitis in children and adolescents. Fetal Pediatr Pathol. 2014;33:202–209. doi: 10.3109/15513815.2014.898721. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Papamichalis PA, Zachou K, Koukoulis GK, et al. The revised international autoimmune hepatitis score in chronic liver diseases including autoimmune hepatitis/overlap syndromes and autoimmune hepatitis with concurrent other liver disorders. J Autoimmune Dis. 2007;4:3. doi: 10.1186/1740-2557-4-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Lüth S, Kanzler S, Frenzel C, et al. Characteristics and long-term prognosis of the autoimmune hepatitis/primary sclerosing cholangitis overlap syndrome. J Clin Gastroenterol. 2009;43:75–80. doi: 10.1097/MCG.0b013e318157c614. [DOI] [PubMed] [Google Scholar]
- 67.Lewin M, Vilgrain V, Ozenne V, et al. Prevalence of sclerosing cholangitis in adults with autoimmune hepatitis:a prospective magnetic resonance imaging and histological study. Hepatology. 2009;50:528–537. doi: 10.1002/hep.23024. [DOI] [PubMed] [Google Scholar]
- 68.Yasui S, Fujiwara K, Yonemitsu Y, Oda S, Nakano M, Yokosuka O. Clinicopathological features of severe and fulminant forms of autoimmune hepatitis. J Gastroenterol. 2011;46:378–390. doi: 10.1007/s00535-010-0316-3. [DOI] [PubMed] [Google Scholar]
- 69.Mieli-Vergani G, Vergani D, Baumann U, et al. Diagnosis and management of pediatric autoimmune liver disease:ESPGHAN hepatology committee position statement. J Pediatr Gastroenterol Nutr. 2018;66:345–360. doi: 10.1097/MPG.0000000000001801. [DOI] [PubMed] [Google Scholar]
- 70.Terziroli Beretta-Piccoli B, Mieli-Vergani G, Vergani D. Serology in autoimmune hepatitis:A clinical-practice approach. Eur J Intern Med. 2018;48:35–43. doi: 10.1016/j.ejim.2017.10.006. [DOI] [PubMed] [Google Scholar]
- 71.Dalekos GN, Zachou K, Liaskos C, Gatselis N. Autoantibodies and defined target autoantigens in autoimmune hepatitis:an overview. Eur J Intern Med. 2002;13:293–303. doi: 10.1016/s0953-6205(02)00089-4. [DOI] [PubMed] [Google Scholar]
- 72.Zachou K, Rigopoulou E, Dalekos GN. Autoantibodies and autoantigens in autoimmune hepatitis:important tools in clinical practice and to study pathogenesis of the disease. J Autoimmune Dis. 2004;1:2. doi: 10.1186/1740-2557-1-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Liaskos C, Bogdanos DP, Davies ET, Dalekos GN. Diagnostic relevance of anti-filamentous actin antibodies in autoimmune hepatitis. J Clin Pathol. 2007;60:107–108. doi: 10.1136/jcp.2006.039404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Dalekos GN, Makri E, Loges S, et al. Increased incidence of anti-LKM autoantibodies in a consecutive cohort of hepatitis C patients from central Greece. Eur J Gastroenterol Hepatol. 2002;14:35–42. doi: 10.1097/00042737-200201000-00007. [DOI] [PubMed] [Google Scholar]
- 75.Ferri S, Muratori L, Quarneti C, et al. Clinical features and effect of antiviral therapy on anti-liver/kidney microsomal antibody type 1 positive chronic hepatitis C. J Hepatol. 2009;50:1093–1101. doi: 10.1016/j.jhep.2009.02.020. [DOI] [PubMed] [Google Scholar]
- 76.Crivelli O, Lavarini C, Chiaberge E, et al. Microsomal autoantibodies in chronic infection with the HBsAg associated delta (delta) agent. Clin Exp Immunol. 1983;54:232–238. [PMC free article] [PubMed] [Google Scholar]
- 77.Fabien N, Desbos A, Bienvenu J, Magdalou J. Autoantibodies directed against the UDP-glucuronosyltransferases in human autoimmune hepatitis. Autoimmun Rev. 2004;3:1–9. doi: 10.1016/S1568-9972(03)00051-X. [DOI] [PubMed] [Google Scholar]
- 78.European Association for the Study of the Liver. EASL Recommendations on Treatment of Hepatitis C 2018. J Hepatol. 2018;69:461–511. doi: 10.1016/j.jhep.2018.03.026. [DOI] [PubMed] [Google Scholar]
- 79.Zachou K, Gampeta S, Gatselis NK, et al. Anti-SLA/LP alone or in combination with anti-Ro52 and fine specificity of anti-Ro52 antibodies in patients with autoimmune hepatitis. Liver Int. 2015;35:660–672. doi: 10.1111/liv.12658. [DOI] [PubMed] [Google Scholar]
- 80.Liaskos C, Bogdanos DP, Rigopoulou EI, et al. Antibody responses specific for soluble liver antigen co-occur with Ro-52 autoantibodies in patients with autoimmune hepatitis. J Hepatol. 2007;46:S250. [Google Scholar]
- 81.Eyraud V, Chazouilleres O, Ballot E, Corpechot C, Poupon R, Johanet C. Significance of antibodies to soluble liver antigen/liver pancreas:a large French study. Liver Int. 2009;29:857–864. doi: 10.1111/j.1478-3231.2009.01986.x. [DOI] [PubMed] [Google Scholar]
- 82.Montano-Loza AJ, Shums Z, Norman GL, Czaja AJ. Prognostic implications of antibodies to Ro/SSA and soluble liver antigen in type 1 autoimmune hepatitis. Liver Int. 2012;32:85–92. doi: 10.1111/j.1478-3231.2011.02502.x. [DOI] [PubMed] [Google Scholar]
- 83.Wies I, Brunner S, Henninger J, et al. Identification of target antigen for SLA/LP autoantibodies in autoimmune hepatitis. Lancet. 2000;355:1510–1515. doi: 10.1016/s0140-6736(00)02166-8. [DOI] [PubMed] [Google Scholar]
- 84.Palioura S, Sherrer RL, Steitz TA, Söll D, Simonovic M. The human SepSecS-tRNASec complex reveals the mechanism of selenocysteine formation. Science. 2009;325:321–325. doi: 10.1126/science.1173755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Ma Y, Okamoto M, Thomas MG, et al. Antibodies to conformational epitopes of soluble liver antigen define a severe form of autoimmune liver disease. Hepatology. 2002;35:658–664. doi: 10.1053/jhep.2002.32092. [DOI] [PubMed] [Google Scholar]
- 86.Gatselis NK, Dalekos GN. Molecular diagnostic testing for primary biliary cholangitis. Expert Rev Mol Diagn. 2016;16:1001–1010. doi: 10.1080/14737159.2016.1217159. [DOI] [PubMed] [Google Scholar]
- 87.O'Brien C, Joshi S, Feld JJ, Guindi M, Dienes HP, Heathcote EJ. Long-term follow-up of antimitochondrial antibody-positive autoimmune hepatitis. Hepatology. 2008;48:550–556. doi: 10.1002/hep.22380. [DOI] [PubMed] [Google Scholar]
- 88.Montano-Loza AJ, Carpenter HA, Czaja AJ. Frequency, behavior, and prognostic implications of antimitochondrial antibodies in type 1 autoimmune hepatitis. J Clin Gastroenterol. 2008;42:1047–1053. doi: 10.1097/MCG.0b013e3181587d18. [DOI] [PubMed] [Google Scholar]
- 89.Nezu S, Tanaka A, Yasui H, et al. Presence of antimitochondrial autoantibodies in patients with autoimmune hepatitis. J Gastroenterol Hepatol. 2006;21:1448–1454. doi: 10.1111/j.1440-1746.2006.04434.x. [DOI] [PubMed] [Google Scholar]
- 90.Muratori P, Efe C, Muratori L, et al. Clinical implications of antimitochondrial antibody seropositivity in autoimmune hepatitis:a multicentre study. Eur J Gastroenterol Hepatol. 2017;29:777–780. doi: 10.1097/MEG.0000000000000870. [DOI] [PubMed] [Google Scholar]
- 91.Liaskos C, Bogdanos DP, Rigopoulou EI, Dalekos GN. Development of antimitochondrial antibodies in patients with autoimmune hepatitis:art of facts or an artifact? J Gastroenterol Hepatol. 2007;22:454–455. doi: 10.1111/j.1440-1746.2006.04751.x. [DOI] [PubMed] [Google Scholar]
- 92.Dinani AM, Fischer SE, Mosko J, Guindi M, Hirschfield GM. Patients with autoimmune hepatitis who have antimitochondrial antibodies need long-term follow-up to detect late development of primary biliary cirrhosis. Clin Gastroenterol Hepatol. 2012;10:682–684. doi: 10.1016/j.cgh.2012.02.010. [DOI] [PubMed] [Google Scholar]
- 93.Renaudineau Y, Deocharan B, Jousse S, Renaudineau E, Putterman C, Youinou P. Anti-alpha-actinin antibodies:a new marker of lupus nephritis. Autoimmun Rev. 2007;6:464–468. doi: 10.1016/j.autrev.2007.02.001. [DOI] [PubMed] [Google Scholar]
- 94.Oikonomou KG, Zachou K, Dalekos GN. Alpha-actinin:a multidisciplinary protein with important role in B-cell driven autoimmunity. Autoimmun Rev. 2011;10:389–396. doi: 10.1016/j.autrev.2010.12.009. [DOI] [PubMed] [Google Scholar]
- 95.Guéguen P, Dalekos G, Nousbaum JB, et al. Double reactivity against actin and alpha-actinin defines a severe form of autoimmune hepatitis type 1. J Clin Immunol. 2006;26:495–505. doi: 10.1007/s10875-006-9045-z. [DOI] [PubMed] [Google Scholar]
- 96.Renaudineau Y, Dalekos GN, Guéguen P, Zachou K, Youinou P. Anti-alpha-actinin antibodies cross-react with anti-ssDNA antibodies in active autoimmune hepatitis. Clin Rev Allergy Immunol. 2008;34:321–325. doi: 10.1007/s12016-007-8050-1. [DOI] [PubMed] [Google Scholar]
- 97.Zachou K, Oikonomou K, Renaudineau Y, et al. Anti-αactinin antibodies as new predictors of response to treatment in autoimmune hepatitis type 1. Aliment Pharmacol Ther. 2012;35:116–125. doi: 10.1111/j.1365-2036.2011.04908.x. [DOI] [PubMed] [Google Scholar]
- 98.Dienes HP, Erberich H, Dries V, Schirmacher P, Lohse A. Autoimmune hepatitis and overlap syndromes. Clin Liver Dis. 2002;6:349–362, vi. doi: 10.1016/s1089-3261(02)00007-7. [DOI] [PubMed] [Google Scholar]
- 99.Zen Y, Notsumata K, Tanaka N, Nakanuma Y. Hepatic centrilobular zonal necrosis with positive antinuclear antibody:a unique subtype or early disease of autoimmune hepatitis? Hum Pathol. 2007;38:1669–1675. doi: 10.1016/j.humpath.2007.03.019. [DOI] [PubMed] [Google Scholar]
- 100.Czaja AJ, Muratori P, Muratori L, Carpenter HA, Bianchi FB. Diagnostic and therapeutic implications of bile duct injury in autoimmune hepatitis. Liver Int. 2004;24:322–329. doi: 10.1111/j.1478-3231.2004.0924.x. [DOI] [PubMed] [Google Scholar]
- 101.Hartl J, Ehlken H, Sebode M, et al. Usefulness of biochemical remission and transient elastography in monitoring disease course in autoimmune hepatitis. J Hepatol. 2018;68:754–763. doi: 10.1016/j.jhep.2017.11.020. [DOI] [PubMed] [Google Scholar]
- 102.Gutkowski K, Hartleb M, Kacperek-Hartleb T, et al. Laboratory-based scoring system for prediction of hepatic inflammatory activity in patients with autoimmune hepatitis. Liver Int. 2013;33:1370–1377. doi: 10.1111/liv.12198. [DOI] [PubMed] [Google Scholar]
- 103.Dalekos GN, Bogdanos DP, Neuberger J. Celiac disease-related autoantibodies in end-stage autoimmune liver diseases:what is the message? Liver Int. 2008;28:426–428. doi: 10.1111/j.1478-3231.2008.01708.x. [DOI] [PubMed] [Google Scholar]
- 104.Kaya M, Angulo P, Lindor KD. Overlap of autoimmune hepatitis and primary sclerosing cholangitis:an evaluation of a modified scoring system. J Hepatol. 2000;33:537–542. doi: 10.1034/j.1600-0641.2000.033004537.x. [DOI] [PubMed] [Google Scholar]
- 105.Talwalkar JA, Keach JC, Angulo P, Lindor KD. Overlap of autoimmune hepatitis and primary biliary cirrhosis:an evaluation of a modified scoring system. Am J Gastroenterol. 2002;97:1191–1197. doi: 10.1111/j.1572-0241.2002.05703.x. [DOI] [PubMed] [Google Scholar]
- 106.Gatselis N, Zachou K, Papamichalis P, et al. Comparison of simplified score with the revised original score for the diagnosis of autoimmune hepatitis:a new or a complementary diagnostic score? Dig Liver Dis. 2010;42:807–812. doi: 10.1016/j.dld.2010.03.005. [DOI] [PubMed] [Google Scholar]
- 107.Qiu D, Wang Q, Wang H, et al. Validation of the simplified criteria for diagnosis of autoimmune hepatitis in Chinese patients. J Hepatol. 2011;54:340–347. doi: 10.1016/j.jhep.2010.06.032. [DOI] [PubMed] [Google Scholar]
- 108.Yeoman AD, Westbrook RH, Al-Chalabi T, et al. Diagnostic value and utility of the simplified International Autoimmune Hepatitis Group (IAIHG) criteria in acute and chronic liver disease. Hepatology. 2009;50:538–545. doi: 10.1002/hep.23042. [DOI] [PubMed] [Google Scholar]
- 109.Lohse AW. Recognizing autoimmune hepatitis:scores help, but no more. J Hepatol. 2011;54:193–194. doi: 10.1016/j.jhep.2010.07.013. [DOI] [PubMed] [Google Scholar]
- 110.Yamamoto K, Miyake Y, Ohira H, et al. Intractable Liver and Biliary Diseases Study Group of Japan. Prognosis of autoimmune hepatitis showing acute presentation. Hepatol Res. 2013;43:630–638. doi: 10.1111/j.1872-034X.2012.01109.x. [DOI] [PubMed] [Google Scholar]
- 111.Fujiwara K, Yasui S, Tawada A, Fukuda Y, Nakano M, Yokosuka O. Diagnostic value and utility of the simplified International Autoimmune Hepatitis Group criteria in acute-onset autoimmune hepatitis. Liver Int. 2011;31:1013–1020. doi: 10.1111/j.1478-3231.2011.02524.x. [DOI] [PubMed] [Google Scholar]
- 112.Zachou K, Arvaniti P, Azariadis K, et al. Prompt initiation of high-dose i.v. corticosteroids seems to prevent progression to liver failure in patients with original acute severe autoimmune hepatitis. Hepatol Res. 2018 Sep 24; doi: 10.1111/hepr.13252. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 113.Kalafateli M, Triantos C, Tsamandas A, Dalekos GN. Spontaneous cirrhosis regression in an IFN-beta-induced AIH-like syndrome following drug withdrawal:art of facts or artifacts? Eur J Case Rep Intern Med. 2016:3. doi: 10.12890/2016_000396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Kirk AP, Jain S, Pocock S, Thomas HC, Sherlock S. Late results of the Royal Free Hospital prospective controlled trial of prednisolone therapy in hepatitis B surface antigen negative chronic active hepatitis. Gut. 1980;21:78–83. doi: 10.1136/gut.21.1.78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Lamers MM, van Oijen MG, Pronk M, Drenth JP. Treatment options for autoimmune hepatitis:a systematic review of randomized controlled trials. J Hepatol. 2010;53:191–198. doi: 10.1016/j.jhep.2010.01.037. [DOI] [PubMed] [Google Scholar]
- 116.Dufour JF, Zimmermann M, Reichen J. Severe autoimmune hepatitis in patients with previous spontaneous recovery of a flare. J Hepatol. 2002;37:748–752. doi: 10.1016/s0168-8278(02)00329-x. [DOI] [PubMed] [Google Scholar]
- 117.Czaja AJ. Features and consequences of untreated type 1 autoimmune hepatitis. Liver Int. 2009;29:816–823. doi: 10.1111/j.1478-3231.2008.01904.x. [DOI] [PubMed] [Google Scholar]
- 118.Lohse AW, Mieli-Vergani G. Autoimmune hepatitis. J Hepatol. 2011;55:171–182. doi: 10.1016/j.jhep.2010.12.012. [DOI] [PubMed] [Google Scholar]
- 119.Schramm C, Weiler-Normann C, Wiegard C, Hellweg S, Müller S, Lohse AW. Treatment response in patients with autoimmune hepatitis. Hepatology. 2010;52:2247–2248. doi: 10.1002/hep.23840. [DOI] [PubMed] [Google Scholar]
- 120.Wang Q, Qiu D, Ma X. Early normalisation of aminotransferase predicts complete biochemical remission in autoimmune hepatitis patients. Aliment Pharmacol Ther. 2011;34:107–109. doi: 10.1111/j.1365-2036.2011.04690.x. [DOI] [PubMed] [Google Scholar]
- 121.Czaja AJ. Safety issues in the management of autoimmune hepatitis. Expert Opin Drug Saf. 2008;7:319–333. doi: 10.1517/14740338.7.3.319. [DOI] [PubMed] [Google Scholar]
- 122.Heneghan MA, Allan ML, Bornstein JD, Muir AJ, Tendler DA. Utility of thiopurine methyltransferase genotyping and phenotyping, and measurement of azathioprine metabolites in the management of patients with autoimmune hepatitis. J Hepatol. 2006;45:584–591. doi: 10.1016/j.jhep.2006.05.011. [DOI] [PubMed] [Google Scholar]
- 123.Czaja AJ, Carpenter HA. Thiopurine methyltransferase deficiency and azathioprine intolerance in autoimmune hepatitis. Dig Dis Sci. 2006;51:968–975. doi: 10.1007/s10620-006-9336-5. [DOI] [PubMed] [Google Scholar]
- 124.Hindorf U, Jahed K, Bergquist A, et al. Characterisation and utility of thiopurine methyltransferase and thiopurine metabolite measurements in autoimmune hepatitis. J Hepatol. 2010;52:106–111. doi: 10.1016/j.jhep.2009.10.004. [DOI] [PubMed] [Google Scholar]
- 125.Czaja AJ. Current and prospective pharmacotherapy for autoimmune hepatitis. Expert Opin Pharmacother. 2014;15:1715–1736. doi: 10.1517/14656566.2014.931938. [DOI] [PubMed] [Google Scholar]
- 126.van Gerven NM, Verwer BJ, Witte BI, et al. Dutch Autoimmune Hepatitis Working Group. Relapse is almost universal after withdrawal of immunosuppressive medication in patients with autoimmune hepatitis in remission. J Hepatol. 2013;58:141–147. doi: 10.1016/j.jhep.2012.09.009. [DOI] [PubMed] [Google Scholar]
- 127.Hlivko JT, Shiffman ML, Stravitz RT, et al. A single center review of the use of mycophenolate mofetil in the treatment of autoimmune hepatitis. Clin Gastroenterol Hepatol. 2008;6:1036–1040. doi: 10.1016/j.cgh.2008.04.006. [DOI] [PubMed] [Google Scholar]
- 128.Zachou K, Gatselis NK, Arvaniti P, et al. A real-world study focused on the long-term efficacy of mycophenolate mofetil as first-line treatment of autoimmune hepatitis. Aliment Pharmacol Ther. 2016;43:1035–1047. doi: 10.1111/apt.13584. [DOI] [PubMed] [Google Scholar]
- 129.Dalekos GN, Zachou K. Editorial:autoimmune hepatitis-identifying options for treatment. Authors'reply. Aliment Pharmacol Ther. 2016;43:1237–1238. doi: 10.1111/apt.13626. [DOI] [PubMed] [Google Scholar]
- 130.Manns MP, Woynarowski M, Kreisel W, et al. European AIH-BUC-Study Group. Budesonide induces remission more effectively than prednisone in a controlled trial of patients with autoimmune hepatitis. Gastroenterology. 2010;139:1198–1206. doi: 10.1053/j.gastro.2010.06.046. [DOI] [PubMed] [Google Scholar]
- 131.Liberal R, de Boer YS, Andrade RJ, et al. International Autoimmune Hepatitis Group (IAIHG) Expert clinical management of autoimmune hepatitis in the real world. Aliment Pharmacol Ther. 2017;45:723–732. doi: 10.1111/apt.13907. [DOI] [PubMed] [Google Scholar]
- 132.Wiegand J, Schüler A, Kanzler S, et al. Budesonide in previously untreated autoimmune hepatitis. Liver Int. 2005;25:927–934. doi: 10.1111/j.1478-3231.2005.01122.x. [DOI] [PubMed] [Google Scholar]
- 133.Efe C, Ozaslan E, Kav T, et al. Liver fibrosis may reduce the efficacy of budesonide in the treatment of autoimmune hepatitis and overlap syndrome. Autoimmun Rev. 2012;11:330–334. doi: 10.1016/j.autrev.2011.09.006. [DOI] [PubMed] [Google Scholar]
- 134.Woynarowski M, Nemeth A, Baruch Y, et al. European Autoimmune Hepatitis-Budesonide Study Group. Budesonide versus prednisone with azathioprine for the treatment of autoimmune hepatitis in children and adolescents. J Pediatr. 2013;163:1347–1353.e1. doi: 10.1016/j.jpeds.2013.05.042. [DOI] [PubMed] [Google Scholar]
- 135.Allison AC. Mechanisms of action of mycophenolate mofetil. Lupus. 2005;14(Suppl 1):s2–s8. doi: 10.1191/0961203305lu2109oa. [DOI] [PubMed] [Google Scholar]
- 136.Demirkiran A, Sewgobind VD, van der Weijde J, et al. Conversion from calcineurin inhibitor to mycophenolate mofetil-based immunosuppression changes the frequency and phenotype of CD4+FOXP3+regulatory T cells. Transplantation. 2009;87:1062–1068. doi: 10.1097/TP.0b013e31819d2032. [DOI] [PubMed] [Google Scholar]
- 137.Miroux C, Morales O, Ouaguia L, et al. Corticosteroids do not reverse the inhibitory effect of cyclosporine on regulatory T-cell activity in contrast to mycophenolate mofetil. Transplant Proc. 2012;44:2834–2839. doi: 10.1016/j.transproceed.2012.09.091. [DOI] [PubMed] [Google Scholar]
- 138.Lee J, Kim MS, Kim EY, et al. Mycophenolate mofetil promotes down-regulation of expanded B cells and production of TNF-alpha in an experimental murine model of colitis. Cytokine. 2008;44:49–56. doi: 10.1016/j.cyto.2008.06.006. [DOI] [PubMed] [Google Scholar]
- 139.Taubert R, Hardtke-Wolenski M, Noyan F, et al. Intrahepatic regulatory T cells in autoimmune hepatitis are associated with treatment response and depleted with current therapies. J Hepatol. 2014;61:1106–1114. doi: 10.1016/j.jhep.2014.05.034. [DOI] [PubMed] [Google Scholar]
- 140.Chen YY, Jeffery HC, Hunter S, et al. Human intrahepatic regulatory T cells are functional, require IL-2 from effector cells for survival, and are susceptible to Fas ligand-mediated apoptosis. Hepatology. 2016;64:138–150. doi: 10.1002/hep.28517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141.Diestelhorst J, Junge N, Schlue J, et al. Pediatric autoimmune hepatitis shows a disproportionate decline of regulatory T cells in the liver and of IL-2 in the blood of patients undergoing therapy. PLoS One. 2017;12:e0181107. doi: 10.1371/journal.pone.0181107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 142.Czaja AJ. Rapidity of treatment response and outcome in type 1 autoimmune hepatitis. J Hepatol. 2009;51:161–167. doi: 10.1016/j.jhep.2009.02.026. [DOI] [PubMed] [Google Scholar]
- 143.Muratori P, Granito A, Pappas G, Muratori L. Validation of simplified diagnostic criteria for autoimmune hepatitis in Italian patients. Hepatology. 2009;49:1782–1783. doi: 10.1002/hep.22825. author reply 1783. [DOI] [PubMed] [Google Scholar]
- 144.Manns MP, Jaeckel E, Taubert R. Budesoinide in autoimmune hepatitis:The right drug at the right time for the right patient. Clin Gastroenterol Hepatol. 2018;16:186–189. doi: 10.1016/j.cgh.2017.11.003. [DOI] [PubMed] [Google Scholar]
- 145.Czaja AJ, Lindor KD. Failure of budesonide in a pilot study of treatment-dependent autoimmune hepatitis. Gastroenterology. 2000;119:1312–1316. doi: 10.1053/gast.2000.0010000001. [DOI] [PubMed] [Google Scholar]
- 146.Lohse AW, Gil H. Reactivation of autoimmune hepatitis during budesonide monotherapy, and response to standard treatment. J Hepatol. 2011;54:837–839. doi: 10.1016/j.jhep.2010.09.017. [DOI] [PubMed] [Google Scholar]
- 147.Johnson PJ, McFarlane IG, Williams R. Azathioprine for long-term maintenance of remission in autoimmune hepatitis. N Engl J Med. 1995;333:958–963. doi: 10.1056/NEJM199510123331502. [DOI] [PubMed] [Google Scholar]
- 148.Czaja AJ, Ludwig J, Baggenstoss AH, Wolf A. Corticosteroid-treated chronic active hepatitis in remission:uncertain prognosis of chronic persistent hepatitis. N Engl J Med. 1981;304:5–9. doi: 10.1056/NEJM198101013040102. [DOI] [PubMed] [Google Scholar]
- 149.Czaja AJ, Menon KV, Carpenter HA. Sustained remission after corticosteroid therapy for type 1 autoimmune hepatitis:a retrospective analysis. Hepatology. 2002;35:890–897. doi: 10.1053/jhep.2002.32485. [DOI] [PubMed] [Google Scholar]
- 150.Verma S, Gunuwan B, Mendler M, Govindrajan S, Redeker A. Factors predicting relapse and poor outcome in type I autoimmune hepatitis:role of cirrhosis development, patterns of transaminases during remission and plasma cell activity in the liver biopsy. Am J Gastroenterol. 2004;99:1510–1516. doi: 10.1111/j.1572-0241.2004.30457.x. [DOI] [PubMed] [Google Scholar]
- 151.Kanzler S, Gerken G, Löhr H, Galle PR, Meyer zum Büschenfelde KH, Lohse AW. Duration of immunosuppressive therapy in autoimmune hepatitis. J Hepatol. 2001;34:354–355. doi: 10.1016/s0168-8278(00)00095-7. [DOI] [PubMed] [Google Scholar]
- 152.Montano-Loza AJ, Carpenter HA, Czaja AJ. Improving the end point of corticosteroid therapy in type 1 autoimmune hepatitis to reduce the frequency of relapse. Am J Gastroenterol. 2007;102:1005–1012. doi: 10.1111/j.1572-0241.2007.01153.x. [DOI] [PubMed] [Google Scholar]
- 153.Hoeroldt B, McFarlane E, Dube A, et al. Long-term outcomes of patients with autoimmune hepatitis managed at a nontransplant center. Gastroenterology. 2011;140:1980–1989. doi: 10.1053/j.gastro.2011.02.065. [DOI] [PubMed] [Google Scholar]
- 154.Montano-Loza AJ, Carpenter HA, Czaja AJ. Consequences of treatment withdrawal in type 1 autoimmune hepatitis. Liver Int. 2007;27:507–515. doi: 10.1111/j.1478-3231.2007.01444.x. [DOI] [PubMed] [Google Scholar]
- 155.Hartl J, Ehlken H, Weiler-Normann C, et al. Patient selection based on treatment duration and liver biochemistry increases success rates after treatment withdrawal in autoimmune hepatitis. J Hepatol. 2015;62:642–646. doi: 10.1016/j.jhep.2014.10.018. [DOI] [PubMed] [Google Scholar]
- 156.Lüth S, Herkel J, Kanzler S, et al. Serologic markers compared with liver biopsy for monitoring disease activity in autoimmune hepatitis. J Clin Gastroenterol. 2008;42:926–930. doi: 10.1097/MCG.0b013e318154af74. [DOI] [PubMed] [Google Scholar]
- 157.European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;67:370–398. doi: 10.1016/j.jhep.2017.03.021. [DOI] [PubMed] [Google Scholar]
- 158.Dalekos GN, Goulis I, Manolakopoulos S, Papaevangelou V, Papatheodoridis G. Clinical Practice Guidelines for the Management of Hepatitis B Virus Infection. Hellenic Center for Disease Control and Prevention, Hellenic Ministry of Health, Athens, December 2017 (online edition, www.keelpno.gr) [Google Scholar]
- 159.Selvarajah V, Montano-Loza AJ, Czaja AJ. Systematic review:managing suboptimal treatment responses in autoimmune hepatitis with conventional and nonstandard drugs. Aliment Pharmacol Ther. 2012;36:691–707. doi: 10.1111/apt.12042. [DOI] [PubMed] [Google Scholar]
- 160.Deutsch M, Emmanuel T, Koskinas J. Autoimmune hepatitis or Wilson's disease, a clinical dilemma. Hepat Mon. 2013;13:e7872. doi: 10.5812/hepatmon.7872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 161.Azariadi K, Arvaniti P, Gatselis NK, Koukoulis GK, Dalekos GN, Zachou K. Severe acute non-A, non-B, non-C hepatitis with autoimmune features:Consider acute hepatitis E virus (HEV) infection not just autoimmune hepatitis (AIH) 9thInternational Congress of Internal Medicine, Athens, March 9-11, 2017, Abstract Book. :23. [Google Scholar]
- 162.Ichai P, Duclos-Vallee JC, Guettier C, et al. Usefulness of corticosteroids for the treatment of severe and fulminant forms of autoimmune hepatitis. Liver Transpl. 2007;13:996–1003. doi: 10.1002/lt.21036. [DOI] [PubMed] [Google Scholar]
- 163.Yeoman AD, Westbrook RH, Zen Y, et al. Prognosis of acute severe autoimmune hepatitis (AS-AIH):the role of corticosteroids in modifying outcome. J Hepatol. 2014;61:876–882. doi: 10.1016/j.jhep.2014.05.021. [DOI] [PubMed] [Google Scholar]
- 164.Verma S, Maheshwari A, Thuluvath P. Liver failure as initial presentation of autoimmune hepatitis:clinical characteristics, predictors of response to steroid therapy, and outcomes. Hepatology. 2009;49:1396–1397. doi: 10.1002/hep.22894. [DOI] [PubMed] [Google Scholar]
- 165.Wendon J, Cordoba J, Dhawan A, et al. EASL Governing Board representative. EASL Clinical Practical Guidelines on the management of acute (fulminant) liver failure. J Hepatol. 2017;66:1047–1081. doi: 10.1016/j.jhep.2016.12.003. [DOI] [PubMed] [Google Scholar]
- 166.Moenne-Loccoz R, Severac F, Baumert TF, Habersetzer F. Usefulness of corticosteroids as first-line therapy in patients with acute severe autoimmune hepatitis. J Hepatol. 2016;65:444–446. doi: 10.1016/j.jhep.2016.03.023. [DOI] [PubMed] [Google Scholar]
- 167.Yeoman AD, Westbrook RH, Zen Y, et al. Early predictors of corticosteroid treatment failure in icteric presentations of autoimmune hepatitis. Hepatology. 2011;53:926–934. doi: 10.1002/hep.24141. [DOI] [PubMed] [Google Scholar]
- 168.Montano-Loza AJ, Carpenter HA, Czaja AJ. Features associated with treatment failure in type 1 autoimmune hepatitis and predictive value of the model of end-stage liver disease. Hepatology. 2007;46:1138–1145. doi: 10.1002/hep.21787. [DOI] [PubMed] [Google Scholar]
- 169.Sonthalia N, Rathi M, Jain S, et al. Natural history and treatment outcomes of severe autoimmune hepatitis. J Clin Gastroenterol. 2017;51:548–556. doi: 10.1097/MCG.0000000000000805. [DOI] [PubMed] [Google Scholar]
- 170.Potts JR, Verma S. Optimizing management in autoimmune hepatitis with liver failure at initial presentation. World J Gastroenterol. 2011;17:2070–2075. doi: 10.3748/wjg.v17.i16.2070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 171.De M E, Coilly A, Houssel-Debry P, et al. Treatment and prognosis of acute severe autoimmune hepatitis. J Hepatol. 2017;66(Suppl 1):S4. [Abstract] [Google Scholar]
- 172.Weiler-Normann C, Lohse AW. Acute autoimmune hepatitis:many open questions. J Hepatol. 2014;61:727–729. doi: 10.1016/j.jhep.2014.06.030. [DOI] [PubMed] [Google Scholar]
- 173.Dhaliwal HK, Anderson R, Thornhill EL, et al. Clinical significance of azathioprine metabolites for the maintenance of remission in autoimmune hepatitis. Hepatology. 2012;56:1401–1408. doi: 10.1002/hep.25760. [DOI] [PubMed] [Google Scholar]
- 174.Floreani A, Liberal R, Vergani D, Mieli-Vergani G. Autoimmune hepatitis:Contrasts and comparisons in children and adults - a comprehensive review. J Autoimmun. 2013;46:7–16. doi: 10.1016/j.jaut.2013.08.004. [DOI] [PubMed] [Google Scholar]
- 175.Kerkar N, Annunziato RA, Foley L, et al. Prospective analysis of nonadherence in autoimmune hepatitis:a common problem. J Pediatr Gastroenterol Nutr. 2006;43:629–634. doi: 10.1097/01.mpg.0000239735.87111.ba. [DOI] [PubMed] [Google Scholar]
- 176.Kelly D. Theory to reality:the role of the transition nurse coordinator. Br J Nurs. 2014;23:888. doi: 10.12968/bjon.2014.23.16.888. 890, 892-894. [DOI] [PubMed] [Google Scholar]
- 177.Sockalingam S, Blank D, Abdelhamid N, Abbey SE, Hirschfield GM. Identifying opportunities to improve management of autoimmune hepatitis:evaluation of drug adherence and psychosocial factors. J Hepatol. 2012;57:1299–1304. doi: 10.1016/j.jhep.2012.07.032. [DOI] [PubMed] [Google Scholar]
- 178.Chatur N, Ramji A, Bain VG, et al. Transplant immunosuppressive agents in non-transplant chronic autoimmune hepatitis:the Canadian association for the study of liver (CASL) experience with mycophenolate mofetil and tacrolimus. Liver Int. 2005;25:723–727. doi: 10.1111/j.1478-3231.2005.01107.x. [DOI] [PubMed] [Google Scholar]
- 179.Inductivo-Yu I, Adams A, Gish RG, et al. Mycophenolate mofetil in autoimmune hepatitis patients not responsive or intolerant to standard immunosuppressive therapy. Clin Gastroenterol Hepatol. 2007;5:799–802. doi: 10.1016/j.cgh.2007.02.030. [DOI] [PubMed] [Google Scholar]
- 180.Aw MM, Dhawan A, Samyn M, Bargiota A, Mieli-Vergani G. Mycophenolate mofetil as rescue treatment for autoimmune liver disease in children:a 5-year follow-up. J Hepatol. 2009;51:156–160. doi: 10.1016/j.jhep.2009.02.024. [DOI] [PubMed] [Google Scholar]
- 181.Wolf DC, Bojito L, Facciuto M, Lebovics E. Mycophenolate mofetil for autoimmune hepatitis:a single practice experience. Dig Dis Sci. 2009;54:2519–2522. doi: 10.1007/s10620-008-0632-0. [DOI] [PubMed] [Google Scholar]
- 182.Czaja AJ, Carpenter HA. Empiric therapy of autoimmune hepatitis with mycophenolate mofetil:comparison with conventional treatment for refractory disease. J Clin Gastroenterol. 2005;39:819–825. doi: 10.1097/01.mcg.0000177260.72692.e8. [DOI] [PubMed] [Google Scholar]
- 183.Hennes EM, Oo YH, Schramm C, et al. Mycophenolate mofetil as second line therapy in autoimmune hepatitis? Am J Gastroenterol. 2008;103:3063–3070. doi: 10.1111/j.1572-0241.2008.02180.x. [DOI] [PubMed] [Google Scholar]
- 184.Sharzehi K, Huang MA, Schreibman IR, Brown KA. Mycophenolate mofetil for the treatment of autoimmune hepatitis in patients refractory or intolerant to conventional therapy. Can J Gastroenterol. 2010;24:588–592. doi: 10.1155/2010/891252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 185.Baven-Pronk AM, Coenraad MJ, van Buuren HR, et al. The role of mycophenolate mofetil in the management of autoimmune hepatitis and overlap syndromes. Aliment Pharmacol Ther. 2011;34:335–343. doi: 10.1111/j.1365-2036.2011.04727.x. [DOI] [PubMed] [Google Scholar]
- 186.Roberts SK, Lim R, Strasser S, et al. ALA Clinical Research Network. Efficacy and safety of mycophenolate mofetil in patients with autoimmune hepatitis and suboptimal outcomes after standard therapy. Clin Gastroenterol Hepatol. 2018;16:268–277. doi: 10.1016/j.cgh.2017.09.063. [DOI] [PubMed] [Google Scholar]
- 187.Efe C, Hagström H, Ytting H, et al. Efficacy and safety of mycophenolate mofetil and tacrolimus as second-line therapy for patients with autoimmune hepatitis. Clin Gastroenterol Hepatol. 2017;15:1950–1956. doi: 10.1016/j.cgh.2017.06.001. [DOI] [PubMed] [Google Scholar]
- 188.Peiseler M, Liebscher T, Sebode M, et al. Efficacy and limitations of budesonide as a second-line treatment for patients with autoimmune hepatitis. Clin Gastroenterol Hepatol. 2018;16:260–267. doi: 10.1016/j.cgh.2016.12.040. [DOI] [PubMed] [Google Scholar]
- 189.Legué C, Legros L, Kammerer-Jacquet S, et al. Safety and efficacy of 6-thioguanine as a second-line treatment for autoimmune hepatitis. Clin Gastroenterol Hepatol. 2018;16:290–291. doi: 10.1016/j.cgh.2017.07.032. [DOI] [PubMed] [Google Scholar]
- 190.Haridy J, Nicoll A, Sood S. Methotrexate therapy for autoimmune hepatitis. Clin Gastroenterol Hepatol. 2018;16:288–289. doi: 10.1016/j.cgh.2017.07.003. [DOI] [PubMed] [Google Scholar]
- 191.Sciveres M, Caprai S, Palla G, Ughi C, Maggiore G. Effectiveness and safety of ciclosporin as therapy for autoimmune diseases of the liver in children and adolescents. Aliment Pharmacol Ther. 2004;19:209–217. doi: 10.1046/j.1365-2036.2003.01754.x. [DOI] [PubMed] [Google Scholar]
- 192.de Boer YS, van Gerven NM, de Boer NK, Mulder CJ, Bouma G, van Nieuwkerk CM. Allopurinol safely and effectively optimises thiopurine metabolites in patients with autoimmune hepatitis. Aliment Pharmacol Ther. 2013;37:640–646. doi: 10.1111/apt.12223. [DOI] [PubMed] [Google Scholar]
- 193.Burak KW, Swain MG, Santodomingo-Garzon T, et al. Rituximab for the treatment of patients with autoimmune hepatitis who are refractory or intolerant to standard therapy. Can J Gastroenterol. 2013;27:273–280. doi: 10.1155/2013/512624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 194.Weiler-Normann C, Schramm C, Quaas A, et al. Infliximab as a rescue treatment in difficult-to-treat autoimmune hepatitis. J Hepatol. 2013;58:529–534. doi: 10.1016/j.jhep.2012.11.010. [DOI] [PubMed] [Google Scholar]
- 195.Chen J, Eslick GD, Weltman M. Systematic review with meta-analysis:clinical manifestations and management of autoimmune hepatitis in the elderly. Aliment Pharmacol Ther. 2014;39:117–124. doi: 10.1111/apt.12563. [DOI] [PubMed] [Google Scholar]
- 196.Miyake Y, Iwasaki Y, Takaki A, Kobashi H, Sakaguchi K, Shiratori Y. Clinical features of Japanese elderly patients with type 1 autoimmune hepatitis. Intern Med. 2007;46:1945–1949. doi: 10.2169/internalmedicine.46.0420. [DOI] [PubMed] [Google Scholar]
- 197.Azariadi K, Arvaniti P, Zachou K, Saitis AI, Dalekos GN, Gatselis N. Autoimmune hepatitis:Impact of age at disease onset on disease severity, outcome and response to treatment. Hepatology. 2016;64:820A. [Abstract] [Google Scholar]
- 198.Chazouillères O, Wendum D, Serfaty L, Rosmorduc O, Poupon R. Long term outcome and response to therapy of primary biliary cirrhosis-autoimmune hepatitis overlap syndrome. J Hepatol. 2006;44:400–406. doi: 10.1016/j.jhep.2005.10.017. [DOI] [PubMed] [Google Scholar]
- 199.Ozaslan E, Efe C, Heurgué-Berlot A, et al. Factors associated with response to therapy and outcome of patients with primary biliary cirrhosis with features of autoimmune hepatitis. Clin Gastroenterol Hepatol. 2014;12:863–869. doi: 10.1016/j.cgh.2013.09.021. [DOI] [PubMed] [Google Scholar]
- 200.Poupon R, Chazouilleres O, Corpechot C, Chrétien Y. Development of autoimmune hepatitis in patients with typical primary biliary cirrhosis. Hepatology. 2006;44:85–90. doi: 10.1002/hep.21229. [DOI] [PubMed] [Google Scholar]
- 201.European Association for the Study of the Liver. EASL Clinical Practice Guidelines:management of cholestatic liver diseases. J Hepatol. 2009;51:237–267. doi: 10.1016/j.jhep.2009.04.009. [DOI] [PubMed] [Google Scholar]
- 202.Floreani A, Rizzotto ER, Ferrara F, et al. Clinical course and outcome of autoimmune hepatitis/primary sclerosing cholangitis overlap syndrome. Am J Gastroenterol. 2005;100:1516–1522. doi: 10.1111/j.1572-0241.2005.41841.x. [DOI] [PubMed] [Google Scholar]
- 203.Zenouzi R, Lohse AW. Long-term outcome in PSC/AIH “overlap syndrome”:does immunosuppression also treat the PSC component? J Hepatol. 2014;61:1189–1191. doi: 10.1016/j.jhep.2014.08.002. [DOI] [PubMed] [Google Scholar]
- 204.Schramm C, Herkel J, Beuers U, Kanzler S, Galle PR, Lohse AW. Pregnancy in autoimmune hepatitis:outcome and risk factors. Am J Gastroenterol. 2006;101:556–560. doi: 10.1111/j.1572-0241.2006.00479.x. [DOI] [PubMed] [Google Scholar]
- 205.Werner M, Björnsson E, Prytz H, et al. Autoimmune hepatitis among fertile women:strategies during pregnancy and breastfeeding? Scand J Gastroenterol. 2007;42:986–991. doi: 10.1080/00365520601155266. [DOI] [PubMed] [Google Scholar]
- 206.Angelberger S, Reinisch W, Messerschmidt A, et al. Long-term follow-up of babies exposed to azathioprine in utero and via breastfeeding. J Crohns Colitis. 2011;5:95–100. doi: 10.1016/j.crohns.2010.10.005. [DOI] [PubMed] [Google Scholar]
- 207.Carbone M, Neuberger JM. Autoimmune liver disease, autoimmunity and liver transplantation. J Hepatol. 2014;60:210–223. doi: 10.1016/j.jhep.2013.09.020. [DOI] [PubMed] [Google Scholar]
- 208.González-Koch A, Czaja AJ, Carpenter HA, et al. Recurrent autoimmune hepatitis after orthotopic liver transplantation. Liver Transpl. 2001;7:302–310. doi: 10.1053/jlts.2001.21449. [DOI] [PubMed] [Google Scholar]
- 209.Chatrath H, Allen L, Boyer TD. Use of sirolimus in the treatment of refractory autoimmune hepatitis. Am J Med. 2014;127:1128–1131. doi: 10.1016/j.amjmed.2014.06.016. [DOI] [PubMed] [Google Scholar]
- 210.Salcedo M, Vaquero J, Bañares R, et al. Response to steroids in de novo autoimmune hepatitis after liver transplantation. Hepatology. 2002;35:349–356. doi: 10.1053/jhep.2002.31167. [DOI] [PubMed] [Google Scholar]
- 211.Georgiadou SP, Zachou K, Liaskos C, Gabeta S, Rigopoulou EI, Dalekos GN. Occult hepatitis B virus infection in Greek patients with autoimmune liver diseases. Liver Int 2009. 29:434–442. doi: 10.1111/j.1478-3231.2008.01851.x. [DOI] [PubMed] [Google Scholar]
- 212.Rigopoulou EI, Zachou K, Gatselis N, Koukoulis GK, Dalekos GN. Autoimmune hepatitis in patients with chronic HBV and HCV infections:patterns of clinical characteristics, disease progression and outcome. Ann Hepatol. 2014;13:127–135. [PubMed] [Google Scholar]
- 213.Azhar A, Niazi MA, Tufail K, Malek AH, Balasubramanian M, Araya V. A new approach for treatment of hepatitis C in hepatitis C-autoimmune hepatitis overlap syndrome. Gastroenterol Hepatol (N Y) 2010;6:233–236. [PMC free article] [PubMed] [Google Scholar]
- 214.Ofori E, Ramai D, Ona MA, Reddy M. Autoimmune hepatitis in the setting of human immunodeficiency virus infection:A case series. World J Hepatol. 2017;9:1367–1371. doi: 10.4254/wjh.v9.i36.1367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 215.Kia L, Beattie A, Green RM. Autoimmune hepatitis in patients with human immunodeficiency virus (HIV):Case reports of a rare, but important diagnosis with therapeutic implications. Medicine (Baltimore) 2017;96:e6011. doi: 10.1097/MD.0000000000006011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 216.European Association for the Study of Obesity (EASO) EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J Hepatol. 2016;64:1388–1402. doi: 10.1016/j.jhep.2015.11.004. [DOI] [PubMed] [Google Scholar]
- 217.Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67:358–380. doi: 10.1002/hep.29086. [DOI] [PubMed] [Google Scholar]
- 218.Versini M, Jeandel PY, Rosenthal E, Shoenfeld Y. Obesity in autoimmune diseases:not a passive bystander. Autoimmun Rev. 2014;13:981–1000. doi: 10.1016/j.autrev.2014.07.001. [DOI] [PubMed] [Google Scholar]
- 219.Müller P, Messmer M, Bayer M, Pfeilschifter JM, Hintermann E, Christen U. Non-alcoholic fatty liver disease (NAFLD) potentiates autoimmune hepatitis in the CYP2D6 mouse model. J Autoimmun. 2016;69:51–58. doi: 10.1016/j.jaut.2016.02.007. [DOI] [PubMed] [Google Scholar]
- 220.De Luca-Johnson J, Wangensteen KJ, Hanson J, Krawitt E, Wilcox R. Natural history of patients presenting with autoimmune hepatitis and coincident nonalcoholic fatty liver disease. Dig Dis Sci. 2016;61:2710–2720. doi: 10.1007/s10620-016-4213-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 221.Weiler-Normann C, Lohse AW. Nonalcoholic fatty liver disease in patients with autoimmune hepatitis:Further reason for teeth GNASHing? Dig Dis Sci. 2016;61:2462–2464. doi: 10.1007/s10620-016-4258-3. [DOI] [PubMed] [Google Scholar]