

Abstract
Purpose
If not recognized and treated promptly, nontraumatic orbital subperiosteal hemorrhage (NTSOH) can have serious sequelae including compressive optic neuropathy and permanent vision loss. The following case establishes erotic asphyxiation as a cause of NTSOH.
Observations
A 29 year-old patient presented with diplopia and periorbital edema and ecchymosis. Complete ophthalmologic exam showed no optic neuropathy. Computed tomography of the orbits revealed a subperiosteal fluid collection in the right orbit. The patient had no risk factors for NTSOH, but after detailed questioning she admitted to participating in erotic asphyxiation prior to the onset of her symptoms. She was observed and subsequently lost to follow up.
Conclusions and Importance
To the authors' knowledge, erotic asphyxiation as a cause of orbital subperiosteal hematoma has not been previously reported. Lack of knowledge about erotic asphyxiation amongst healthcare providers may contribute to hesitance to directly question patients about the practice. Clinicians should be aware of erotic asphyxiation as a potential cause of orbital subperiosteal hemorrhage.
Keywords: Erotic asphyxiation, Nontraumatic orbital subperiosteal hemorrhage, Orbital hematoma
1. Introduction
Erotic asphyxiation involves production of cerebral hypoxia for sexual pleasure. The authors report a case of nontraumatic orbital subperiosteal hemorrhage (NTSOH) following erotic asphyxiation in a patient with no other risk factors. The etiology of the hemorrhage was revealed only after thorough questioning. To the authors' knowledge, this is the first report of erotic asphyxiation as a cause of orbital subperiosteal hematoma.
2. Case report
A 29 year-old female presented with progressively worsening binocular diplopia, right-sided periorbital edema and ecchymosis, and a pressure sensation behind her right eye. There was moderate edema and ecchymosis of the right upper eyelid with associated mechanical ptosis and mild proptosis (Fig. 1). Right globe elevation was limited, and there was a small angle right hypotropia in primary gaze. Uncorrected visual acuity was 20/20 and color vision was full in both eyes. The pupils reacted normally with no relative afferent pupillary defect. Posterior segment examination revealed no optic nerve or retinal pathology.
Fig. 1.
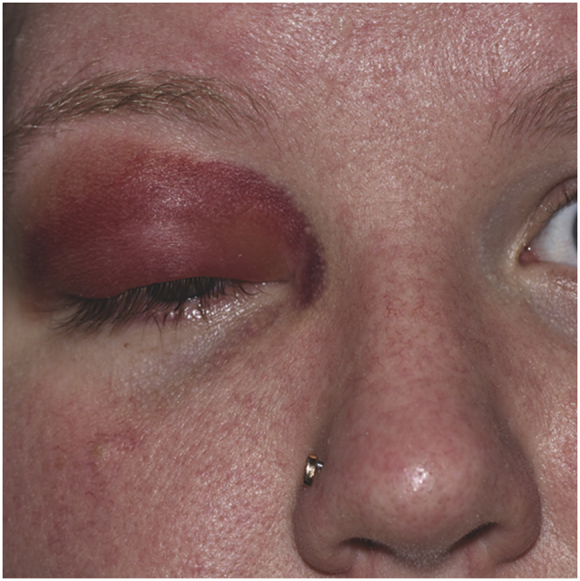
External examination showed moderate edema and ecchymosis of the right upper eyelid with associated mechanical ptosis and mild proptosis.
Computed tomography of the orbits was performed revealing a superomedial subperiosteal fluid collection in the right orbit measuring approximately 2.1 × 0.6 cm and displacing the globe inferotemporally (Fig. 2).
Fig. 2.

Computed tomography (CT) of the orbits revealed a superomedial subperiosteal fluid collection in the right orbit measuring approximately 2.1 × 0.6cm and displacing the globe inferotemporally.
The patient did not have any significant past medical history. She denied use of anticoagulants, history of periorbital trauma, recent vomiting, weightlifting, or other activities causing increased intraabdominal or cranial venous pressure. The patient eventually revealed that onset of double vision occurred during autoerotic asphyxiation by means of self-strangulation through use of digital pressure over the carotid arteries. There was no sign of trauma to the neck when she presented to the emergency department two days after the episode. She had no psychiatric history and denied current or past desire to harm herself or others.
Given the good acuity and absence of optic neuropathy, the decision was made to observe. She was subsequently lost to follow up. Consent to publish the case report was not obtained. This report does not contain any personal information that could lead to the identification of the patient.
3. Discussion
Autoerotic asphyxiation is the practice of producing cerebral hypoxia for the purpose of attaining or enhancing solitary sexual pleasure.1, 2, 3 Strangulation, suffocation, chest or neck compression, and inhalation of volatile solvents are methods used to induce hypoxia.1, 2, 3 Although the prevalence of autoerotic asphyxiation is difficult to quantify due to its secretive nature, the incidence of autoerotic deaths in Western countries is estimated to be 0.5 deaths per million people per year.2 Of these, 70–80% are due to autoerotic asphyxia by hanging and an additional 10–30% are related to asphyxia by use of plastic bags or chemicals.2 The actual prevalence of autoerotic asphyxiation is likely much higher than these statistics suggest as they do not include the incidents that evade death or the autoerotic deaths that are mistakenly labeled as suicide.1,3,4
Autoerotic practices have been documented for over 200 years, and the vast majority of individuals involved in North America are young, white men.4,5 Further questioning or examination may reveal accompanying practices used to enhance sexual pleasure including cross-dressing and rectal or genital foreign body insertion.1,3,4 Sexual asphyxia must not be overlooked as a mechanism of injury in other demographics as cases have been reported across all age groups and socioeconomic classes and regardless of marital status.3,4
NTSOH has been reported in a number of situations. The most common etiology is related to a sudden increase in cranial venous pressure, which occurs in situations such as vomiting, childbirth, or strangulation.5, 6, 7 Other predisposing factors include bleeding disorders, sinus infections, or the use of general anesthesia.5, 6, 7 A case of a NTSOH in a young, healthy patient after a yoga headstand maneuver has also been reported.8 The bleeding in NTSOH is thought to originate from small veins coursing across the subperiosteal space between the orbital bones and periorbital.5, 6, 7 Common presenting symptoms include proptosis, globe displacement, eyelid edema, periorbital pain, nausea and vomiting, and diplopia.5,6 If not recognized and treated promptly, an orbital subperiosteal hematoma can cause compressive optic neuropathy and permanent vision loss. Surgical drainage is indicated for patients with acute optic nerve compression or to confirm an uncertain diagnosis.5
Although orbital subperiosteal hematomas have been attributed to other non-traumatic causes, to our knowledge, erotic asphyxiation as a cause of orbital subperiosteal hematoma has not been previously reported. Our patient was a young female who presented to the emergency department with diplopia, periorbital ecchymosis, and pain and was found to have an orbital subperiosteal hematoma in the absence of trauma or obvious non-traumatic risk factors. Upon further questioning, the patient revealed that she had participated in autoerotic asphyxiation by means of strangulation two days prior to her presentation, around the time of onset of her symptoms.
4. Conclusions
Many healthcare professionals lack knowledge of the unusual, secretive practice of erotic asphyxiation and its prevalence. This contributes to hesitance to directly question patients and in turn may delay recognition and treatment of complications resulting from the practice. This case report establishes erotic asphyxiation as a cause of orbital subperiosteal hemorrhage.
Patient consent
Written consent to publish this case has not been obtained. This report does not contain any personal identifying information.
Acknowledgements and disclosures
Funding
No finding or grant support.
Conflicts of interest
The following authors have no financial disclosures: CH, ARH, TB, AM.
Authorship
All authors attest that they meet the current ICMJE criteria for Authorship.
Acknowledgements
None.
References
- 1.Yacobi Y., Tsivian A., Sidi A.A. Emergent and surgical interventions for injuries associated with eroticism: a review. J Trauma Inj Infect Crit Care. 2007;62:1522–1530. doi: 10.1097/TA.0b013e3180341f8f. [DOI] [PubMed] [Google Scholar]
- 2.Sauvageau A. Current reports on autoerotic deaths – five persistent myths. Curr Psychiatr Rep. 2014;16:430. doi: 10.1007/s11920-013-0430-z. [DOI] [PubMed] [Google Scholar]
- 3.Gosink P.D., Jumbelic M.I. Autoerotic asphyxiation in a female. Am J Forensic Med Pathol. 2000;21:114–118. doi: 10.1097/00000433-200006000-00004. [DOI] [PubMed] [Google Scholar]
- 4.Byard R.W. Autoerotic death: a rare but recurrent entity. Forensic Sci Med Pathol. 2012;8:349–350. doi: 10.1007/s12024-012-9319-0. [DOI] [PubMed] [Google Scholar]
- 5.Atalla M.L., Mcnab A.A., Sullivan T.J., Sloan B. Nontraumatic subperiosteal orbital hemorrhage. Ophthalmology. 2001;108:183–189. doi: 10.1016/s0161-6420(00)00482-6. [DOI] [PubMed] [Google Scholar]
- 6.Mcnab A.A. Nontraumatic orbital hemorrhage. Surv Ophthalmol. 2014;59:166–184. doi: 10.1016/j.survophthal.2013.07.002. [DOI] [PubMed] [Google Scholar]
- 7.Subiras X., Koch K.R., Schrittenlocher S. Spontaneous unilateral subperiosteal hematoma in the orbit due to self-induced asphyxia: unusual cause of unilateral exophthalmos. Case Rep. Ophthalmol. 2017;8:232–236. doi: 10.1159/000469701. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Richards A., Wijesinghe N. Non-traumatic subperiosteal orbital haematoma following yoga. J Clin Exp Ophthalmol. 2014;5:339. [Google Scholar]