

Abstract
Background:
Byssinosis is an acute respiratory difficulty that is caused usually following exposure to cotton and hemp dust. Occurrence of such similar acute symptoms had been reported following exposure to jute dust/fiber also. With passage of time, Jute industries have modernized themselves for increased quality and productivity, which has lessened workforce and thereby provided more working space. However, occupational health benefit due to such changes has rarely been explored. This study was initiated to understand whether this modernization can protect the health of workers.
Methodology:
This study was carried out in two jute mills manufacturing jute clothes, jute bags, and so on. Interview of the workers for their occupational and morbidity details, medical examinations, as well as pre-shift and post-shift pulmonary function tests was carried out.
Results:
It was observed that chest tightness was significantly more in the industry with old technologies. Breathlessness was also more in this industry. As far as pulmonary function status is concerned, it was noted that greater than 5% cross-shift change in forced expiratory volume in one second was more common in the industry with old technology. Obstructive feature on lung function test was also observed in workers of both industries.
Conclusion:
The study concluded that exposure to jute dust has contributed to both acute and chronic respiratory health effects in the jute industry workers. Modernized industry showed lesser prevalence of acute symptoms and changes related to byssinosis. Modernization of processes in jute industries may prove fruitful in lowering the respiratory problems of workers.
Keywords: Byssinosis, jute mill workers, modernization of industry, respiratory health
INTRODUCTION
Occurrence of byssinosis following exposure to cotton dust, hemp, and so on is already reported.[1] Epidemiological studies on jute industry workers have also reported byssinosis-like occurrences.[2] Studies have also explored etiological factors responsible for the occurrence of the disease. Endotoxins derived from gram-negative bacteria are considered to be major contributing factor. One such study showed byssinosis-like symptoms in 22.8% of workers, and acute and chronic changes of pulmonary function in 25.7% and 20.0% of workers, respectively.[2] Another study[3] noticed the evidence of byssinosis in 8.7% of workers and acute as well as chronic changes of ventilatory pulmonary function in 35.7% and 31.6% of workers, respectively. The etiological factors responsible for the occurrence of the disease in cotton textile workers is believed to be the endotoxins derived from gram-negative bacteria. It has also been found that gram-negative bacterial endotoxin is present in the jute mill dust.[4,5] Level of endotoxins of the jute mill dust[4,5,6] was almost similar to that reported in Indian cotton textile mills.[7]
The relevant studies undertaken in jute industries are almost two decades old and with passage of time such industries have modernized themselves for increased quality and productivity, which has lessened workforce and thereby provided more working space. However, occupational health benefits due to such changes have rarely been explored. Under such circumstances this study was initiated with the objective of examining workers' health with special reference to byssinosis-related symptoms and also to evaluate the pulmonary function of the workers at the pre-shift and post-shift periods.
METHODOLOGY
The study
This study is a cross-sectional epidemiological study with comparison groups.
The industries
This study was carried out in two jute mills manufacturing jute clothes, jute bags, and so on, employing about 3000 workers each. Both the mills were running in three work shifts.
Shift A: 6.00 AM to 11.00 AM and 2.00 PM to 5.00 PM (recess between 11.00 AM and 2.00 PM).
Shift B: 11.00 AM to 2.00 PM and 5.00 PM to 10.00 PM (recess between 2.00 PM and 5.00 PM).
Shift C: 10.00 PM to 6.00 AM.
The workers on shift A were included in the study due to the fact that we aimed to examine workers pre-shift and post-shift with a minimum exposure of 4 hours and it was also convenient for the management to spare workers during that time. The pulmonary function tests were carried out before the shift at 5:30 AM and then during the recess just after 11:00 AM. The main concern was to study whether the acute response of dust exposure existed or not in the jute mill workers.
This study was planned on workers from two jute mills based on the technology being adopted for jute processing. One such mill having older technology and another mill having newer, improved, and cleaner technology were selected based on the principles of random sampling. The purpose of this study is to find out workers having different grades of respiratory difficulties and ultimately help in planning for intervention strategy.
Selection of subjects
An approximate number of 120 workers from each of the two selected jute mills were aimed to be included. For this purpose, 150 workers were selected randomly (taking care of non-response and lost to follow-up for post-shift examination) from both industries. After collecting the master list from the jute mill authorities, we made a list of workers who have worked for at least 5 years; random selection was made from this list using a table of random numbers. Sample size was calculated for each industry on the principles of descriptive study with population size 3000, expected frequency 9%, and allowable limit 4%–15% with a confidence interval of 95%. The calculated number was 120.
The parameters
All the subjects were investigated on the first day of the week on resuming duty after weekly holiday. They were interviewed for collecting data on details of their personal, occupational, and medical history. The emphasis was on enquiry regarding the occurrence of chest tightness, cough, sputum, and breathlessness; the day of occurrence of such symptoms; their duration; and relationship with work. The questionnaire was based on the inquiry on byssinosis.[8] Ventilatory function tests consisting of recording vital capacity (VC) and forced vital capacity (FVC) were undertaken with a Spirovit SP-10 (Switzerland) machine. Each individual performed the tests three times during pre-shift and post-shift examinations. The best of the three performances was taken into account. From the FVC curve, the forced expiratory volume in one second (FEV1) was measured. The definition–classification of changes in lung function (FEV1) due to exposure to vegetable dusts causing byssinosis-like health conditions were applied according to the standard classification.[9] The evaluation of the occurrence of byssinosis was done by clinical symptoms (work related) and the pattern of changes of pre-shift and post-shift ventilatory pulmonary function.
Statistical analysis
Initially, a descriptive analysis was carried out to obtain basic details of the study parameters. After Chi-square test, analysis of variance was used to ascertain the differences among different comparison groups in relation to different study parameters. For analysis purpose, study subjects were divided into high dust exposure group (selection, softening, carding, and preparing) and low dust exposure group (spinning, winding, beaming, weaving, and finishing).
RESULTS
Table 1 shows the distribution of jute mill workers according to age, smoking, tobacco chewing habits, work area, and job duration. The mean age of the old technology industry workers was 39.35 ± 8.7 years and mean age of the improved industry workers was 41.62 ± 8.9 years. Mean height and weight of the workers were 163.8 ± 13.8 cm and 60.1 ± 8.5 kg, respectively, for the old technology industry and 163.4 ± 5.5 cm and 58.42 ± 9.24 kg, respectively, for the improved industry. About 30% of the workers belonged to the high dust exposure group and 69.2% of the workers were in the low dust exposure group in the case of the old technology industry and about 26% of the workers belonged to the high dust exposure group and 73.9% of the workers were in the low dust exposure group in the case of the improved industry. The percentages of smokers among the old technology industry and improved industry workers were 30.1% and 32.8%, respectively. Mean job duration of old technology industry workers and improved industry workers was 15.46 ± 8.5 and 18.9 ± 9.2 years, respectively.
Table 1.
General characteristics of subjects
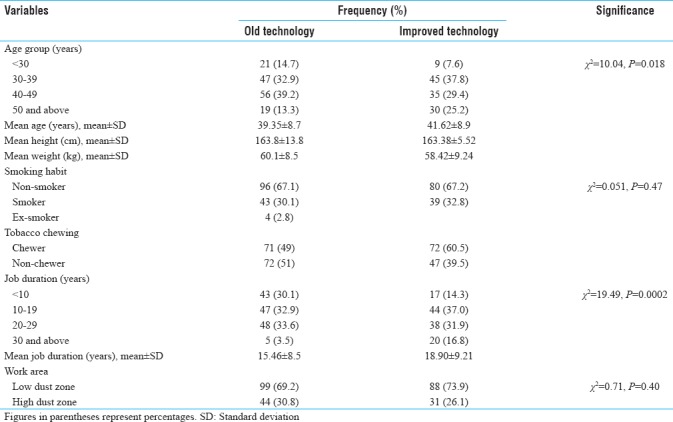
Table 2 showed the morbidity distribution of study subjects. In the case of old technology industry workers, 14 subjects (9.8%) were having chest tightness; among them 5 (3.5%) workers showed chest tightness only on the first working day of the week. Musculoskeletal pain was reported in 32.1% of the workers. In improved industry workers, 3 (2.5%) subjects were having chest tightness; among them 1 (0.8%) worker showed chest tightness only on the first working day of the week. Musculoskeletal pain and burning sensation in eyes were reported in 25.2% and 24.4% of the workers, respectively.
Table 2.
Morbidity distribution of study subjects

The distribution of chest tightness according to work area and job duration was presented in Table 3. In old technology industry, chest tightness was present in 5 (5.1%) and 9 (20.5%) workers in the low and high dust zone, respectively. Chest tightness has increased as the duration of work increased. Chest tightness showed significantly higher prevalence in the high dust exposure group. In improved industry workers, chest tightness was present in 1 (3.2%) worker in the high dust zone and 2 (2.3%) workers in the low dust zone, respectively.
Table 3.
Distribution of chest tightness according to work area and job duration
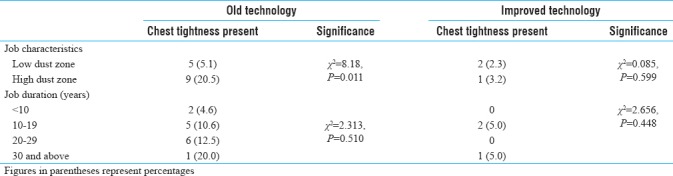
Table 4 depicts the comparison of mean of age, duration of exposure, and ventilatory function test results according to the dust exposure group as low and high dust zone. Slow vital capacity, FVC, and FEV1 were significantly lower in the high dust exposure group in comparison to the low dust exposure group. FEV1%, FEF200–1200 ml, FEF25%–75%, FEF75%–85%, and PEFR also showed lower mean values in the high dust exposure group than the low dust exposure group, where FEF represents forced expiratory flow and PEFR represents peak expiratory flow rate. Such changes were more prominent among the workers of old technology industry.
Table 4.
Distribution of worker and pulmonary function characteristics according to the work area of the subjects
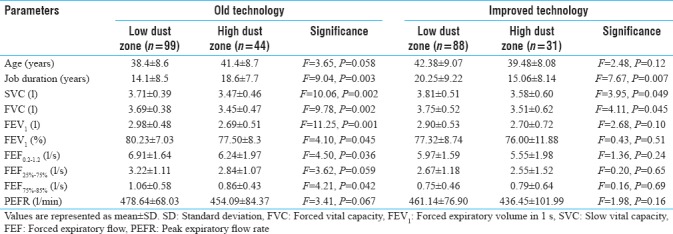
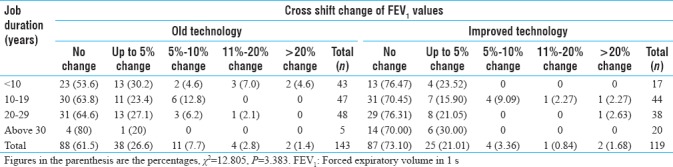
Table 5 showed acute changes in FEV1 in jute mill workers according to the duration of job. On the first working day of the week, change in FEV1 was measured across the shift. Eighty-eight (61.5%) workers of the old technology industry and 87 (73.1%) workers of the improved technology industry had no change in FEV1. Similarly, up to 5% change was found in 26.6% and 21.01% of the workers, respectively. FEV1 decreased by 5%–10% in 11 (7.7%) and 4 (3.36%) workers, respectively, and 11%–20% decrease in FEV1 was seen in 4 (2.8%) and 1 (0.84%) of old technology industry and improved technology industry workers, respectively. Similarly, FEV1 decrease of more than 20% was observed among 2 (1.4%) and 2 (1.68%) workers, respectively.
Table 5.
Distribution of cross shift change of forced expiratory volume in 1 s according to job duration
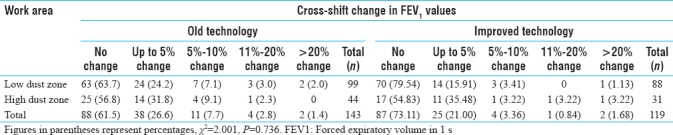
An acute change in FEV1 according to work area characteristics was presented in Table 6. In the low dust zone, no change was found in 63.7% and 79.5% of the workers of the old technology industry and improved technology industry, respectively. Up to 5% change in 24.2% of the workers of the old technology industry and in 15.9% of the workers of the improved technology industry was noted. Cross-shift change of 5%–10% was found in 7.1% and 3.4% of the old technology industry and improved technology industry workers. The corresponding figures in the high dust zone were 56.8% and 54.8% with no change, 31.8% and 35.5% with up to 5% change, and 9.1% and 3.2% with 5%–10% change in the old technology industry and improved technology industry workers, respectively.
Table 6.
Distribution of cross-shift change in forced expiratory volume in 1 s, according to work area characteristic
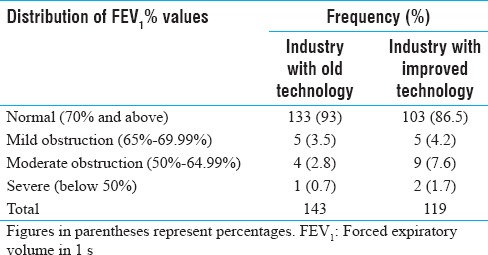
The chronic change in FEV1 values among workers (represented by FEV1% values with respect to FVC values) was presented in Table 7. Among the study subjects, 133 (93%) of old technology industry workers and 103 (86.5%) of improved technology industry workers had values more than or equal to 70%. Mild, moderate, and severe obstruction was present in 5 (3.5%), 4 (2.8%), and 1 (0.7%) of old technology industry worker and 5 (4.2%), 9 (7.6%), and 2 (1.7%) of improved industry workers, respectively.
Table 7.
Distribution of forced expiratory volume in 1 s percentage values among study subjects
Distribution of cross-shift change in FEV1 according to the presence of symptom of chest tightness is presented in Table 8. There were some subjects with cross-shift change of FEV1 values; however, they had no symptom of chest tightness. Among the workers with no chest tightness, no change in FEV1 was found in 80 (62%) workers of the old technology industry and 87 (73.1%) workers of the improved technology industry. Among the workers having chest tightness, no change in FEV1 was found in 8 (57.2%) workers and 3 (100%) workers in the old technology industry and improved technology industry workers, respectively.
Table 8.
Distribution of cross-shift change in forced expiratory volume in 1 s according to the presence of symptoms of chest tightness
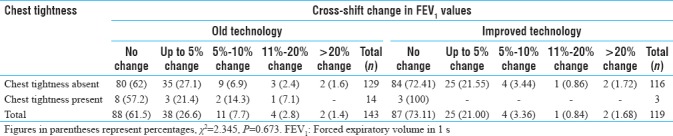
Table 9 presented the prevalence of byssinosis-like symptoms (chest tightness) and ventilatory function changes among study subjects. Byssinosis-like symptoms are present and cross-shift changes in FEV1 of more than 5% was found in 3 (2.09%) old technology industry workers making them typical byssinotic subjects. Such worker was not observed in improved technology industry. In 11 (7.69%) workers of the old technology industry, work-related symptoms were present; however, they had no change or up to 5% change in FEV1 values. The number of such workers was 2.5% among the improved technology industry. In 14 (9.79%) old technology industry workers, no symptoms of byssinosis were reported but more than 5% cross-shift changes in FEV1 was noticed. The number of similar workers was 7 (5.88%) in the improved technology industry.
Table 9.
Prevalence of byssinosis-like symptoms and ventilatory function changes among jute industry workers

Table 10 summarizes the acute and chronic changes in pulmonary function observed in both types of industries. Obstructive change (FEV1% values <70%) was more in the industry with improved technology; however, greater than 5% cross-shift changes in FEV1 values were more in the industry with old technology.
Table 10.
Pulmonary function of the study subjects (acute and chronic changes)

DISCUSSION
The results indicate the presence of symptoms and cross-shift ventilatory function changes like byssinosis in jute industry workers. This is in agreement with earlier findings of eight cases of byssinosis in jute mill workers[2] and similar observation of cases of byssinosis in jute industry workers of Calcutta, India.[10] Studies from India and China[11,12] reported higher prevalence of chest tightness and cough in jute mill workers than in controls. Bacterial endotoxins which are thought to beassociated with byssinosis in cotton workers[4] may play a similar role in jute workers also. Retting of jute is a process by which the embedded fiber is separated from the stem through partial rotting by immersion in water. Heavy bacterial contamination during retting may lead to high levels of bacterial endotoxins. Besides this, one more special step in jute processing may cause microorganism contamination in jute fiber. In the softening process, oil and water are added to the jute fiber which is then kept in a warm house (25°C) for 48 hours. Bacteria and endotoxins may be produced in the jute fiber during this time.[8] The hot and humid Indian climate is quite favorable for bacterial growth. The jute processing procedures in both the jute industries mentioned in this study have been similar.
Chest tightness was observed to be significantly more in the old technology industry. It was also significantly more in the high dust zone as well as among the workers with job duration of 10 or more years. Pulmonary function values mostly were significantly lower in the high dust zone compared to the low dust zone. Cross-shift FEV1 change was more in the old technology industry; however, this difference was more prominent in low dust zone. High dust zone of both industries showed similarity in decrement of FEV1 values across the shift. When cross-shift change in FEV1 was combined with symptoms of chest tightness, it was observed that those old technology industry workers were showing greater change in FEV1 values irrespective of the suffering of chest tightness. Typical byssinotic features of chest tightness combined with more than 5% FEV1 change (cross shift) was observed in 2% of the old technology industry workers, no such subject was found in the improved technology industry. Although cross-shift change in FEV1 value (more than 5%) was more in the old technology industry, obstructive changes (FEV1 value less than 70%) was more in the improved technology industry.
The decrease in FEV1 during the shift on the first working day of the week was found in 24 jute mill workers. This decrease in FEV1 was observed among the jute mill workers with or without symptoms of byssinosis. These findings are in agreement with earlier reports.[6] The temporary decrease in FEV1 in non-byssinotic workers indicates the effect of jute dust on the smooth muscles of the airways resulting in their constriction.[4] The finding of chronic effects in jute mill workers confirms earlier findings[13] which reported that low FEV1 values in jute workers were attributed to the exposure of jute fibers. The study also reported a decrease in FVC and FEV1 in a longitudinal examination of jute mill workers.[14] This study results also showed that the chronic obstructive effect was observed after jute dust exposure. This study concluded that byssinosis symptom does exist in jute mill workers particularly those who are exposed to higher level jute dust for a longer time. The exposure of jute dust leads to fall in FEV1 on the first working day of the week and this fall may occur in jute workers in the absence of symptoms of byssinosis. The etiological factors for the occurrence of the disease in such workers may be gram-negative bacterial endotoxin.
On comparing the data of two industries, it was found that subjects with higher age and job experience were more in the industry with improved technology. However, distribution of workers according to the smoking habit and working area showed no significant difference. While comparing morbidity, it was observed that chest tightness was significantly more in the industry with old technology. On the contrary, irritation/watering in eye during working time was higher in the industry with improved technology. Musculoskeletal pain was a problem in both industries, relatively more in the industry with old technology. As far as pulmonary function status is concerned, it was noted that greater than 5% cross-shift changes in FEV1 were more in the industry with old technology. Obstructive features, however, were more among the workers of the industry with improved technology. This comparative study showed that the acute symptoms and functional changes related to byssinosis were more associated with the industry with old technology, whereas chronic changes (obstructive features) were found to be more associated with the industry with improved technology. Finding of more number of chronic changes in the industry with improved technology may also be due to the fact that workers with higher work experience were more in this industry.
The study concluded that exposure to jute dust has contributed to both acute and chronic respiratory health effects in the jute industry workers. Industry with improved technology showed lesser prevalence of acute symptoms and changes related with byssinosis. This study recommends that the modernization of processes in jute industries may prove fruitful in lowering the respiratory problems of workers. Adoption of proper work postures and knowledge of correct working methods based on ergonomic principles may be useful in controlling the high prevalence of musculoskeletal pain.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Annual Report. India: National Institute of Occupational Health; National Institute of Occupational Health. 1985-86, 1986-87, 1987-88. [Google Scholar]
- 2.Chattopadhyay BP, Alam J, Bandyopadhyay B, Gangopadhyay PK. Study to evaluate the occurrence of byssinosis among jute mill workers by clinical history and acute and chronic changes of forced expiratory volume. Indian J Environ Prot. 1993;13:903–8. [Google Scholar]
- 3.Chattopadhyay BP, Saiyed HN, Alam J, Roy SK, Thakur S, Dasgupta TK. Inquiry into occurrence of Byssinosis in jute mill workers. J Occup Health. 1999;41:225–31. [Google Scholar]
- 4.Zhou C, Liu ZL, Ho CS, Lou JZ. Respiratory symptoms and lung function in jute processing workers: A primary investigation. Arch Environ Health. 1989;44:370–4. doi: 10.1080/00039896.1989.9935909. [DOI] [PubMed] [Google Scholar]
- 5.Chattopadhyay BP, Dipali S, Satipati C. Pulmonary function tests and the jute mill workers. Indian J Occup Health. 1994;37:1–10. [Google Scholar]
- 6.Rylander R, Morey P. Airborne endotoxin in industries processing vegetable fibers. Am Ind Hyg Assoc J. 1982;43:811–2. doi: 10.1080/15298668291410611. [DOI] [PubMed] [Google Scholar]
- 7.Gokani VN, Doctor PB, Ghosh SK. Isolation and identification of gram negative bacteria from raw baled cotton and synthetic textile fibers with special reference to environmental GNB and endotoxin concentrations of textile mill. Am Ind Hyg Assoc J. 1987;48:511–4. doi: 10.1080/15298668791385138. [DOI] [PubMed] [Google Scholar]
- 8.Schilling R. Worldwide problems of byssinosis. Chest. 1981;79:3S–5S. doi: 10.1378/chest.79.4_supplement.3s. [DOI] [PubMed] [Google Scholar]
- 9.Chatterjee S, Saha D, Chatterjee BP. Pulmonary function studies in healthy non-smoking men of Calcutta. Ann Hum Biol. 1988;15:365–74. doi: 10.1080/03014468800009841. [DOI] [PubMed] [Google Scholar]
- 10.Report of WHO. Vegetable dust. Dust causing Byssinosis. WHO Task Group meeting held at Copenhagen. Environ Health Crit. 1983;81:1–19. [Google Scholar]
- 11.Roy B. Prevalence of chest diseases in different working environments among jute mill workers. Bengal Tuberc Assoc. 1985;48:101–5. [Google Scholar]
- 12.Chattopadhyay BP, Saiyed HN, Mukherjee AK. Byssinosis among jute mill workers. Ind Health. 2003;41:265–72. doi: 10.2486/indhealth.41.265. [DOI] [PubMed] [Google Scholar]
- 13.Chattopadhyay BP, Alams J, Gangopadhyay PK, Saiyed HN. Effect of jute dust exposure on ventilatory function and the pertinence of cough and smoking to the response. J UOEH. 1995;17:91–104. doi: 10.7888/juoeh.17.91. [DOI] [PubMed] [Google Scholar]
- 14.Liu Z, Zhou C, Lou J. A longitudinal study of lung function in jute processing workers. Arch Environ Health. 1992;47:218–22. doi: 10.1080/00039896.1992.9938352. [DOI] [PubMed] [Google Scholar]