

Abstract
Impulsiveness has been studied as an aspect of personality and psychopathology for generations. There are longstanding disagreements about how to define it and whether it should be viewed as one construct or several. This article begins by briefly reviewing some earlier and some more recent work on impulsiveness. Several approaches have recently converged to focus on a distinction between impulsive reactions to emotion and impulsive properties that are not initiated by emotion. From this review we turn to psychopathology. It is well known that impulsiveness is related to externalizing psychopathology, but some have concluded that a similar relation does not exist for internalizing psychopathology. A recent literature is described that challenges the latter conclusion, linking impulsive reactivity to emotion to both externalizing and internalizing aspects of psychopathology. Discussion then turns to emotion-related impulsiveness and other constructs to which it is conceptually and empirically related, reexamining whether other conceptual targets should be added to the discussion. The article closes with a consideration of how important it is to continue to remain open to new conceptual perspectives.
Keywords: impulsiveness, dual process, psychopathology, internalizing, externalizing
This article has two main themes, somewhat interwoven. One is empirical, pertaining to relationships between aspects of impulsivity and psychopathology. In that context, evidence is reviewed from several research programs about the potential importance of emotionally-triggered impulsivity compared to other sorts of impulsivity. The other theme concerns issues that arise when investigating the concept of impulsivity, and by extension many other concepts. The article closes with a few words of caution about letting commitment to any given viewpoint on a construct to become so fixed that exploration elsewhere within the construct is discouraged.
Impulsivity
The concept of impulsiveness (a word that will be used interchangeably here with impulsivity) has been part of the psychological landscape for a very long time. It has been studied both as a contributor to psychopathology, and as a property of personality more generally. It is a deceptive concept, though, surprisingly difficult to pin down (Block, 2002; Eisenberg, 2002; Smith, Fischer, Cyders, Annus, Spillane, & McCarthy, 2007; Whiteside & Lynam, 2001). One widely held view says impulsivity is the tendency toward “rapid, unplanned reactions to internal or external stimuli without regard to the negative consequences of those reactions” (Moeller, Barratt, Dougherty, Schmitz, & Swann, 2001). This particular definition emphasizes lack of planning, and also the potential for negative outcomes from one’s actions. Although variations on this definition are widely used, it seems to leave some things out. For example, it doesn’t fit instances in which the action in question is unlikely to have negative consequences (and may even have positive consequences; see Dickman, 1990). It doesn’t seem to fit being easily distracted from one’s present activity to something else that is simply temporarily more appealing.
Another part of the controversy is whether to think of impulsiveness as a single construct or as a class of phenomena with different origins and dynamics that should be considered apart from one another (Depue & Collins, 1999; Sharma, Markon, & Clark, 2014; Whiteside & Lynam, 2001). Thus, for several reasons, how best to define impulsivity remains somewhat controversial.
Background
This section briefly reviews some of the background of influences on current conceptions of impulsivity. This is not a comprehensive review (see, e.g., Fischer, Smith, & Cyders, 2008; Sharma et al., 2014; Whiteside & Lynam, 2001, for more), but rather a sketch intended to give the flavor of some of the influences on contemporary thought about impulsivity. It does not review behavioral measures extensively (though it does touch on them), and it does not distinguish between impulsiveness and self-control (which can be viewed as opposites but can also be seen as having a more complex relationship).
Role of Comprehensive Trait Theories
One goal of work on impulsivity over the past several decades has been placing it (or its various aspects separately) within the framework of broader measures and conceptions of personality. As theories of traits as the structure of personality evolved, along with broad-scale measures of trait structures, so did thinking about placement of impulsivity within those theories and measures. Throughout this evolution, though, a key focus has been integrating impulsivity with contemporary thought about personality structure more generally.
An example of thought on this topic and its evolution comes from the work of the Eysencks. Early on, Eysenck and Eysenck (1968) combined measures of Impulsivity vs Restraint with Sociability to form Extraversion. However, they soon decided that impulsivity was more complex, combining Extraversion with Psychoticism. Accordingly, in the revision of their personality inventory (Eysenck & Eysenck, 1975), most impulsivity items were relocated to became part of a revised Psychoticism factor.
BIS.
Perhaps the most widely used measure of impulsiveness in contemporary psychiatric contexts is the Barratt (1965) Impulsiveness Scale (BIS), which has had many revisions over the years (now the BIS-11, Patton, Stanford, & Barratt, 1995). A main goal behind its development was to define impulsivity within the structure of broader personality constructs. The BIS-11 has 3 scales, each a second order factor combining 2 subsidiary factors. Attentional impulsiveness is having trouble focusing on the task at hand and having racing thoughts (the latter presumably interferes with the former). Motor impulsiveness is acting without thinking and behaving inconsistently over time. Nonplanning impulsiveness is acting without planning and being averse to complex thinking. Thus, the BIS addresses 3 ways in which impulsivity can be expressed—having trouble remaining focused, tending not to make plans, and changing action frequently across time. Ignored, however, are conditions that induce impulsivity.
UPPS.
A more recent attempt to capture impulsiveness within trait theory came from Whiteside and Lynam (2001). After noting that definitions of impulsiveness have a good deal of variability (even more than indicated above), they tried to address some possible sources of the variability by considering definitions of impulsivity within the context of the five-factor model of personality. This approach again frames impulsiveness within trait views of personality, but now using a trait view that has seen several decades of further thought and tinkering.
Whiteside and Lynam (2001) began by identifying facet scales of the NEO-PI-R (Costa & McCrae, 1992) that appear to capture some aspect of impulsivity. They then factor analyzed the facet scales along with several other measures. This yielded four factors, which Whiteside and Lynam (2001) termed Urgency, (Lack of) Premeditation, (Lack of) Perseverance, and Sensation seeking. Accordingly, the instrument comprising these scales is called the UPPS.
Each of these scales loaded along with one of the personality factors: Premeditation and Perseverance with all facet scales of Conscientiousness; Sensation seeking with all facet scales of Extraversion; and Urgency (defined as impulsiveness in reaction to negative affect) with all facet scales of Neuroticism (but with a relatively high secondary loading on Conscientiousness). The scales correlated only .22 with each other on average, indicating that the aspects of impulsivity were relatively distinct. Whiteside and Lynam (2001, p. 685) concluded that the scales reflect “not variations of impulsivity, but rather discrete psychological processes that lead to impulsive-like behaviors.”
Deeper into traits.
A recent meta-analysis by Sharma et al. (2014, Study 1) followed roughly the same logical path as Whiteside and Lynam (2001) but dug deeper. Sharma et al. examined published studies that incorporated “commonly used measures of trait impulsivity” and also included several broad-scale inventories of personality. The pattern of their findings generally fell in line with Whiteside and Lynam’s conclusions and extended them.
Analysis of these measures yielded 3 factors. One centered on neuroticism, one on extraversion, and one on disinhibition versus constraint (or conscientiousness). The neuroticism-like factor was mostly scales from personality inventories tapping neuroticism or its equivalent. Of freestanding impulsivity measures, only UPPS Negative Urgency loaded on that factor (.59), but it also had a substantial secondary loading on the conscientiousness-based factor (.30). The conscientiousness factor had loadings from several personality scales, plus Lack of Premeditation and Lack of Perseverance from the UPPS, as found previously by Whiteside and Lynam (2001). The extraversion-based factor loaded mostly Extraversion personality scales, but also Sensation Seeking and Venturesomeness (as in Whiteside & Lynam, 2001). These results thus generally aligned with Whiteside and Lynam (2001), but from a far larger sample and more measures.
Several conclusions from this work are of interest. Because one impulsivity scale loaded with neuroticism and two with extraversion, Sharma et al. (2014, p. 380) concluded that “many, perhaps most, types of impulsive behaviors are affect driven.” They also wrote that disinhibition is “arguably the ‘core impulsivity’ domain” (p. 378), despite a lack of clear connection from it to affect. Following Tellegen (1985), they suggested that disinhibition is not linked to a specific affect but rather applies more generally. Thus “an individual high in Negative Urgency and Disinhibition would be likely to act more readily and strongly in the context of negative emotions than would one high in Negative Urgency but low in Disinhibition” (p. 382).
Influences From Outside Comprehensive Trait Theories: Positive Urgency
The effort to consider how impulsivity fits within the structure of broader models of personality traits has remained the strongest influence on thinking about impulsivity for an extensive period. There have, however, been some other influences in recent years.
Cyders, Smith, and colleagues (Cyders & Smith, 2007; Cyders, Smith, Spillane, Fischer, Annus, & Peterson, 2007) extended the work of Whiteside and Lynam (2001) by developing a scale to capture tendencies toward engaging in impulsive behavior in the presence of positive, rather than negative, emotions. Unlike the measures mentioned thus far, this was not prompted primarily by an effort to integrate the measure with trait theories. Rather, it was based on clinical evidence that some people show impulsiveness when experiencing positive emotions. Initial studies established that the resulting Positive Urgency Measure (PUM) was distinguishable (by factor analysis) from other impulsivity measures, including the UPPS Urgency scale (hereafter Negative Urgency), and that it had its own predictive validity for risk-taking, eating disorders, and problem gambling (Cyders et al., 2007; Cyders & Smith, 2007, 2008). Importantly, in light of the logic that impulsivity is triggered by emotion, Positive Urgency also predicted riskier gambling behavior and more alcohol intake after a positive mood induction than before the induction (Cyders, Zapolski, Combs, Settles, Fillmore, & Smith, 2010).
As is true of Negative Urgency, interview-based and parent-report scales to assess Positive Urgency show high correspondence with, and as strong psychometric characteristics as, self-report scales assessing those constructs (Cyders & Smith, 2007; Smith, Fischer, Cyders, Annus, Spillane, & McCarthy, 2007; Zapolski & Smith, 2013; Zapolski et al., 2010). At least some data suggest that associations with psychopathology are not just a self-report bias, in that parent report more robustly predicted aggression and attention problems than did child self-report (Zapolski & Smith, 2013). Though clearly distinguishable from Negative Urgency, Positive Urgency is also fairly correlated with it (r = .37 in Cyders et al., 2007; rs = .49 and .59 in Cyders & Smith, 2007). The most parsimonious model is one in which Positive and Negative Urgency are distinguishable facets of an overall Urgency construct (Cyders & Smith, 2007; Sperry, Lynam, & Kwapil, in press). In longitudinal research, Positive Urgency and Negative Urgency also show parallel slopes of change across adolescence (Littlefield et al., 2016). Thus, there is evidence of commonality.
Although development of the Positive Urgency measure was not prompted by a trait theory, Cyders and Smith (2008) provided evidence locating both Urgency measures in the matrix of the five-factor model, placement that agreed closely with the later analysis of Sharma et al. (2014). They reported that Negative Urgency had a substantial loading on neuroticism (.58), but also loaded on conscientiousness (−.40), and agreeableness (−.37). Positive urgency loaded on these traits in a similar pattern: conscientiousness (−.39), agreeableness (−.30), and neuroticism (.28). Neither Urgency scale loaded significantly on extraversion or openness.
As noted, this portrayal of the two aspects of Urgency was not particularly grounded in trait theory. Cyders and Smith (2008) view Urgency (both positive and negative) as representing a general predisposition to mood-based rash action. They argue that “the experience of intense emotions may lead one to focus more heavily on one’s immediate situation” (Cyders & Smith, 2008, p. 813). The reduction of cognitive resources that follows from this narrowed focus helps increase the likelihood of rash action. In effect, the greater salience and immediacy of the emotion render the person’s long-term interests less focal. This interpretation would be consistent with the associations of these scales with agreeableness and conscientiousness, both of which require taking a longer or broader view. This interpretation also resembles a position we have come to ourselves though a somewhat different path (described later), which emphasizes a lack of goal-directed cognition during states of high emotion.
Another point is also important here, regarding the two Urgency scales of the UPPS-P (as the merged measure has come to be known; Lynam, Smith, Cyders, Fischer, & Whiteside, 2007). As noted earlier, constructs and measures of impulsivity have generally given little consideration to precipitators of impulsive actions (though see Lacey & Evans, 1986, for an exception). This is not true of Negative and Positive Urgency. Both of these constructs, for their own reasons, focus in part on emotional states as triggers to the impulsive actions. They contextualize impulsiveness in a way that had not been done in most measures. This turns out to be important.
Influences Outside Trait Theories: Serotonergic Function and Dual Process Views
This section focuses mostly on our own work, which was prompted in part by interest in correlates of serotonergic function. Previous work had suggested that serotonin plays a central role in constraint over impulses, particularly emotion-related impulses (Depue, 1995; Depue & Spoont, 1986; Spoont, 1992). We were led to pursue that specific line of thought further (Carver, Johnson, & Joormann, 2008), doing so partly through the vehicle of dual process models (e.g., Bechara, 2005; Evans & Stanovich, 2013; Kahneman, 2011; Metcalfe & Mischel, 1999; Nigg, 2000; Rothbart, Ellis, Rueda, & Posner, 2003; Strack & Deutsch, 2004; Toates, 2006).
Dual process models of constraint.
Dual process models assume two modes of information processing. One is associative and quick and is sometimes referred to as reflexive. Several theorists characterize it as being especially responsive to emotions (e.g., Metcalfe & Mischel, 1999; Strack & Deutsch, 2004). This mode creates and depends on an accumulation of associations (Daw, Niv, & Dayan, 2005; Dayan, 2008; Dolan & Dayan, 2013; Otto, Gershman, Markman, & Daw, 2013; Walsh & Anderson, 2014). Functioning in this mode reflects habits (e.g., Ouellette & Wood, 1998; Wood, 2017) or responsiveness to cues of the moment that trigger automatic responses (as is true of emotions). The other mode of processing is slower; it functions by applying rules or mental models to situations as they are identified. It is often called reflective or deliberative. It bases action selection on a broader array of considerations, including intentions or plans (Ouellette & Wood, 1998; Wood, 2017). This mode requires more resources, and thus is less efficient than the reflexive mode.
Dual process models assume that both modes compete continuously to influence behavior (Buckholz, 2015; Daw et al., 2005; Dayan, 2008). Each mode has value in appropriate contexts (Block & Block, 1980; Bocanegra & Hommel, 2014; Otto, Gershman, Markman, & Daw, 2013). However, in complex social environments it is often the case that deliberative processing confers benefits, particularly with respect to the pursuit of longer-term goals.
As noted above, a conceptual element common among these theories is the idea that the reflexive mode is particularly reactive to emotions. What specific behaviors follow depends on other aspects of the person’s makeup. If your personality is such that you experience frequent intense desires, lack of deliberative influence will yield frequent expression of those desires in action. Such people can be expected to take things that don’t belong to them, seek extreme sensations, and engage in antisocial behavior, including impulsive aggression (Carver & Miller, 2006). If your approach motivation is blunted and your affect tends to be sad, lack of deliberative influence over those emotions will yield instead frequent behavioral expressions of passivity and lethargy (for detail see Carver, Johnson, & Joormann, 2008; Carver, Johnson, & Timpano, 2017).
Whereas most views of impulsiveness focus at least in part on the rashness of the action, the view pursued here focuses instead on its reflexive versus deliberative nature. Impulsiveness in this view refers to responses (cognitive or behavioral) that are relatively reflexive reactions to some condition. This view has the relatively counterintuitive implication that even inaction can be impulsive, if it is a reflexive response (Carver, Johnson, & Joormann, 2013).
Following Spoont (1992), we argued that lower serotonergic function reflects a relatively weaker influence of the deliberative system, and thus promotes impulsive reactivity to emotion. This, taken together with the idea that impulsive reactivity can yield both active and passive behavioral responses, would account for the fact that serotonergic markers have been related to behaviors with an obviously impulsive topography (e.g., impulsive aggression; Manuck, Kaplan, & Lotrich, 2006) but also to behaviors that appear at first to be the antithesis of impulsive (e.g., the passivity common in depression; Uher & McGuffin, 2010). Following the lead of Depue and Spoont (1986), we argued that both are impulsive because both are reflexive. Both reflect a lack of control over responses to the respective triggering emotions (i.e., anger and sadness).
This focus on poor constraint over underlying emotions resembles somewhat a suggestion by Sharma et al. (2014), described earlier regarding Disinhibition and Negative Urgency. There is, however, this difference: Our view does not assume that Negative Urgency creates the affect. Rather, it is posited here that negative affect stems from neuroticism. Negative Urgency in this view is a tendency toward impulsive reactivity to the emotions created by neuroticism, whereas to Sharma et al., reactivity comes from disinhibition. Our position here is closer to that of Cyders and Smith (2008), who argued that among persons with high levels of Urgency, presence of emotions diminishes the cognitive resources available to constrain responses to the emotions.
An implication of the dual process view is that weakness of the reflective mode could lead to unconstrained responses to a broad range of motivational and emotional states. To further explore this view, several measures of impulsiveness were gathered (Carver et al., 2011), with an emphasis on measures that reflect cognitive or behavioral reactivity to emotional or motivational stimuli. Included were Negative Urgency, Positive Urgency, and a new item set measuring reflexive behavioral reactivity to emotions-in-general. Also included were measures suggesting cognitive over-reactivity to emotions (e.g., overgeneralization from a bad outcome to one’s entire self) and a reflexive passivity in the face of emotion (inclusion of these measures was prompted in part by manifestations of depression in the context of depressed affect). Also included were measures that do not imply reaction to emotions. Some participants were also genotyped on the serotonin transporter polymorphism.
The self-reports formed 3 factors, which have since been labelled the Three-Factor index. Two concerned reflexive responses to emotions. One (Feelings Trigger Action) loaded Negative Urgency, Positive Urgency, and the new measure of reflexive behavioral responses to emotions-in-general. The other (Pervasive Influence of Feelings) loaded measures of cognitive and deenergization reactions to mostly negative emotions. A third factor (Lack of Follow-Through) loaded measures of carry-through of intentions versus impulsively being distracted from them, but with no mention of emotion as a trigger. The two emotion-reactivity factors related in the predicted way to the serotonin transporter polymorphism; the other factor did not. This supports a role for serotonin in emotion-related impulsivity, but not in forms of impulsivity that are not tied to emotional triggers.
Emotion-Related Impulsivity and Response Inhibition
Emotion-related impulsivity has been discussed thus far as a self-report (or parent-report or interview) variable. Does this verbal report also relate to behavioral or neural mechanisms involved in failures of constraint? A construct that is closely related conceptually to it is called response inhibition, the overriding of prepotent responses. The literature on this construct focuses on creating prepotency by creating a habit on some task. The construct is rarely applied to emotion-driven responses (this literature largely ignores emotion). To the extent that emotion also shapes prepotency, however, poor response inhibition should also yield impulsive responses to emotion.
There is some information on the relation between emotion-related impulsiveness and impaired response inhibition. Some studies have found direct associations (i.e., with no manipulation of affect during the response inhibition task) between Urgency and response inhibition: in go/no-go tasks (Gay et al., 2008), the go-stop task (Bagge, Littlefield, Rosellini, & Coffey, 2013; Gay et al., 2008; Wilbertz et al., 2014), and the antisaccade task (Roberts, Fillmore, & Milich, 2011). A recent meta-analysis found that direct relations of Negative Urgency with impaired response inhibition behavior were robust in clinical samples but very small in student and community samples (Johnson, Tharp et al., 2016). This may reflect a restricted range of emotion-related impulsivity in the student and community samples, which were recruited without regard to psychological disturbance.
Another recent study (Peckham & Johnson, 2018) found that 6 sessions of training (compared to a wait list control group) on the go/no-go task, a response inhibition task, led to a decrease in self-reports of emotion-related impulsivity. This suggests a link between response inhibition and emotion-related impulsivity. In another study, higher Negative Urgency related to both poorer performance and less neural activation in the interior frontal gyrus and anterior insula during a response inhibition task (Wilbertz et al., 2014).
To the extent a link between Negative Urgency and impaired response inhibition is supported, it appears relatively specific. That is, (a) Negative Urgency relates more to impaired response inhibition than do other aspects of impulsivity (Cyders & Coskunpinar, 2011), and (b) Negative Urgency does not relate much to other behavioral indicators of impulsivity, including delay discounting, resistance to cognitive distractors, proactive interference, shifting, inattention, or other indices of impulsive decision-making (Cyders & Coskunpinar, 2011; Sharma et al., 2014).
The preceding are all direct associations of cold cognitive measures of response inhibition to self-rated emotional impulsivity. The logic behind impulsive reactivity to emotion, however, is that its effects should depend on the presence of an emotion. The studies just described did not involve emotions. Indeed, very few studies have assessed response inhibition tasks in emotional contexts. Two recent studies successfully induced moods, then tested response inhibition. In both, Negative and Positive Urgency had curvilinear relations to response inhibition, with deficits only at Urgency’s higher levels (as main effects; no interaction with mood; Dekker & Johnson, 2018; Johnson et al., 2016). In a third study (Gunn & Finn, 2015) the mood induction failed, preventing a test of the hypothesis. Taken together, what evidence there is suggests that impaired response inhibition is linked to emotion-related impulsivity, but that emotion need not be part of the context for effects on response inhibition to emerge.
Impulsivity and Psychopathology
We turn now to literature on the involvement of emotion-related impulsivity in psychopathology. It has long been known that impulsiveness is related to a wide range of externalizing disorders (cf. Beauchaine, Zisner, & Sauder, 2017; Venables, Foell, Yancey, Kane, Engle, & Patrick, 2018). Evidence of an association with internalizing psychopathology has been more sparse (but see Granö, Keltikangas-Järvinen, Kouvonen, et al., 2007; Patton, Standform, & Barratt, 1995; Schalling & Edman, 1987), leading some to conclude that no such relation exists (e.g., Krueger & Markon, 2006). Recent research is beginning to change that picture, however.
In particular, many studies have by now examined how the two Urgency measures link to psychopathology. Much of this work, of course, focuses on externalizing. In one meta-analysis of 115 studies involving more than 40,000 participants, Negative Urgency was more closely tied to alcohol and substance problems, aggression, borderline personality disorder symptoms, and disordered eating (r = .34) than were the other forms of impulsivity measured by the UPPS (rs .08 to .14; Berg, Latzman, Bliwise, & Lilienfeld, 2015). In a separate meta-analysis of 50 articles, Negative Urgency was more closely tied to bulimia nervosa (r = .38) than were other forms of impulsivity (rs = .08 to .20; Fischer, Smith, & Cyders, 2008). In longitudinal research, Negative Urgency predicts a worse course of many facets of externalizing psychopathology, including early onset of alcohol use, alcohol dependence, and difficulty with smoking cessation (cf. Hooper & Carver, 2016; Riley, Rukavina, & Smith, 2016; Stojek & Fischer, 2013). This pattern fits with the broader literature linking impulsivity with externalizing syndromes.
Some of this work, however, has also examined relations between Urgency and internalizing. Several studies have found that depressive symptoms are correlated with higher Negative Urgency scores (d’Acremont & Van der Linden, 2007; Karyadi & King, 2011; Miller, Flory, Lynam, & Leukefeld, 2003; Pang, Farrahi, Glazier, Sussman, & Leventhal, 2014). In the Berg et al. (2015) meta-analysis, effects of Negative Urgency on depressive symptoms (r = .45) were larger than those for other dimensions of the UPPS (rs = −.04 to .11). In sum, evidence supports the role of Negative Urgency in internalizing as well as externalizing syndromes. What differentiates these may be the dimension of incentive sensitivity, which is generally low among internalizing problems and high among externalizing problems (Figure 1).
Figure 1.
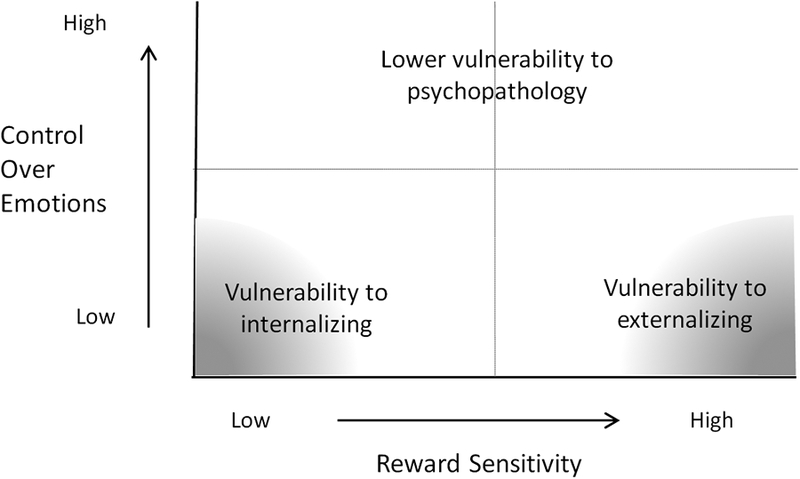
A dimension of incentive sensitivity crossed by a dimension of control over emotions versus reflexive reacting to emotions. Vulnerability to internalizing symptoms such as sadness and lethargy emerges from the combination of low incentive sensitivity (and thus blunted approach) and low control over emotions. Vulnerability to externalizing symptoms emerges from the combination of high incentive sensitivity (and thus strong desires) and low control over emotions. (A dimension of threat sensitivity is also clearly relevant, but is omitted for clarity.) From Carver, Johnson, & Timpano, 2017.
Another important outcome is suicidality. Among the UPPS impulsivity dimensions, the greatest link to suicidality is from Negative Urgency (Berg et al., 2015). In other research, emotion-related impulsivity related to suicidal ideation and suicidal action (Auerbach, Stewart, & Johnson, 2016). Negative Urgency at age 10 has predicted suicide attempt by age 25 (Kasen, Cohen, & Chen, 2011), and Negative Urgency at entrance to college predicted initiation of non-suicidal self-injury during college (Riley, Combs, Jordan, & Smith, 2015).
Intriguingly, Negative Urgency has also been found to be elevated among persons with psychotic disorders, including bipolar disorder in remission (Muhtadie, Johnson, Carver, & Gotlib, 2014) and schizophrenia, a condition not tied to emotional extremes (Hoptman, 2014).
Positive Urgency.
The studies just reviewed examined Negative Urgency. If impulsive reactivity to emotions generalizes across emotional valence, similar associations should appear for Positive Urgency. Although less research has examined Positive than Negative Urgency, similar associations have emerged. Berg and colleagues (2015) found the effect size of Positive Urgency on psychopathology to be roughly comparable to the effect size for Negative Urgency (r = .30). Positive Urgency has also been found to be elevated among persons with remitted bipolar I disorder as compared to well-matched controls (Muhtadie et al., 2014).
In prospective research, Positive Urgency has been tied to the onset and course of externalizing symptoms, including illegal drug use (Zapolski, Cyders, & Smith, 2009), as well as greater use of alcohol among college students (Kaiser, Bonsu, Charnigo, Milich, & Lynam, 2016), adolescents (Lopez-Vergara, Spillane, Merrill, & Jackson, 2016) and middle school students (Settles, Zapolski, & Smith, 2014). Indeed, Positive and Negative Urgency appear to have comparable effects on the onset of drinking among youth between 6th and 9th grade (Riley, Rukavina, & Smith, 2016). The literature thus supports the importance of impulsive responses to both negative and positive emotion states as relevant to externalizing syndromes.
One particular body of findings is especially striking here. It is not surprising to find that depression is correlated with reactivity to negative emotion. Growing evidence, however, relates depression to impulsive reactivity to positive emotions as well. Negative and Positive Urgency both have been tied to current depressive symptoms among children (Marmorstein, 2013) and undergraduates (Karyadi & King, 2011). Lifetime major depressive disorder has been correlated with Positive Urgency, but not with non-emotional impulsivity (Carver et al., 2013; Dekker & Johnson, 2018). This does not appear to be an artifact of current symptoms, as the link remains when current depressive symptoms are controlled (Carver et al., 2013). In longitudinal research, a blend of positive and negative urgency predicted increased depressive symptoms from 5th to 6th grade in a sample of 1,906 children (Smith, Guller, & Zapolski, 2013).
The counterintuitive finding that depression is related to impulsive reactions to positive as well as negative emotions has important implications for the conceptualization of emotion-related impulsivity. The fact that a disorder typified by negative emotional experiences should also be characterized by elevation in Positive Urgency is a strong source of evidence suggesting the existence of a more general reflexive response system that contributes to depression.
In discussing the emerging evidence linking emotion-related impulsivity to internalizing as well as externalizing problems, one more recent article deserves brief mention. In Gustavson et al. (2017) an index of impulsivity was related to externalizing but not internalizing. However, the index was a combination of Positive and Negative Urgency, along with two scales that are not strongly related to Urgency: Lack of Premeditation (from the UPPS), and the Self-Control Scale (Tangney, Baumeister, & Boone, 2004). When the data were reanalyzed using only the Urgency scales (thus being specific to emotion-triggered impulsivity), significant relations to both internalizing and externalizing emerged (Gustavson, personal communication, 2017). This illustrates how results can differ for different aspects of impulsivity.
Section Summary and Implications
This section presented evidence that emotion-related impulsivity is linked to internalizing, externalizing, and psychotic symptoms, and that both longitudinal and cross-sectional research supports these links. We believe that the association of emotion-related impulsivity with diverse indices of psychopathology is an important development in the effort to characterize psychopathology dimensionally. Indeed, we have suggested that emotion-related impulsivity may play a role in what has been called the p factor in psychopathology (Caspi et al., 2014). This is a factor that appears to transcend distinctions among internalizing, externalizing, and psychotic aspects of psychopathology. Carver et al. (2017) have suggested that emotion-related impulsivity may be a key to understanding the p factor.
This suggestion rests on several observations. First is the evidence that emotion-related impulsivity is a correlate of internalizing, externalizing, and psychosis syndromes. Second, some have suggested that the p factor might reflect functional impairment—difficulties in management of key life roles, and tendencies toward problems such as aggression and suicidality—more than specific symptom profiles that were considered above (Caspi et al., 2014). Fitting that, one meta-analysis found that Negative Urgency was a strong correlate of problematic behaviors in daily life, including aggression, gambling, and sex (Sharma et al., 2014). Third, a large number of findings link internalizing, externalizing, and psychosis syndromes with deficits in response inhibition (Bora, Yucel, & Pantelis, 2009; Snyder, 2013; Young, Friedman, Miyake, 2009; Wright et al., 2014), which have been related to emotion-related impulsivity. Taken together, substantial evidence indicates that emotion-related impulsivity is a good candidate in the hunt for explanations of general vulnerability to psychopathology.
Indeed, we have very recently collected a sample of over 500 participants to explore this reasoning further (Pearlstein, Johnson, Timpano, & Carver, 2018). We measured internalizing, externalizing, thought problems, and emotion-related impulsivity. Preliminary analyses yielded a p factor with loadings on the latent variables underlying the three sets of symptom measures. Further, the latent variable from the three-factor scale (Feeling Trigger Action) that loaded scales assessing emotion-related behavioral impulsivity (Carver et al., 2011) was significantly related to the p factor, consistent with our reasoning.
Status Quo and Moving Forward
Psychopathology is gradually moving to a dimensional view, in which liabilities are conferred by being extreme on one or more dimension of variability. These dimensions are presumed to reflect basic functions, which are thought to operate transdiagnostically. This reasoning is embodied in the Research Domain Operating Criteria (RDoC; Cuthbert, 2015; Cuthbert & Insel, 2013). Given the broad array of outcomes predicted by emotion-related impulsivity, from internalizing, externalizing, and psychotic disorders, to dimensions of functional impairment, this concept would seem to fit with the emphasis on transdiagnostic mechanisms.
More concretely, RDoC is organized around a matrix of candidate dimensions expected to contribute to psychopathologies. RDoC thus specifies a preliminary set of domains for research: negative valence, positive valence, cognitive systems (including difficulty overriding prepotent responses), social processes, and arousal/regulatory systems. Indeed, there are even lists of measures recommended as choices for operationalization (National Institute of Mental Health, 2016). NIMH funding prioritizes these domains, and applicants and reviewers are instructed to attend to the recommended choices for both domains and operationalization.
We raise this in order to point out that emotion-related impulsivity per se is not easily accommodated by the RDOC matrix. Response inhibition is a construct that RDoC prioritizes. But to the extent that emotion drives failures in response inhibition, the role of the precipitator is not well captured by that construct.
Continued Reexamination
We just implicitly criticized RDoC on the grounds that it may focus too much on constructs that have been studied extensively and potentially impede novel approaches. In light of the second theme of this article (how the targets of our investigations may evolve or shift over time), we should also question whether emotion-related impulsivity (the target now under discussion here) is as important as we have been asserting it is.
One major concern is that the mechanisms behind emotion-related impulsivity are under-studied. As noted earlier, links from emotion-related impulsivity to behavioral response inhibition (its closest relative among related constructs) emerge most reliably in clinical samples, suggesting that the connection may be facilitated among persons with some level of disturbance. There is a need to examine variables that may induce lapses in control over emotion, including—given that emotions of both valences can drive this form of impulsivity—the role of arousal per se, distinct from valence (there is some evidence for the latter: Pearlstein, Johnson, Modavi, Peckham, & Carver, in press).
To the extent that temporary deficits in cognitive resources help explain effects of emotion-related impulsivity, this has consequences for treatment development. Interventions that rely heavily on strategies requiring cognitive control in response to emotions (e.g., reappraisal) are correspondingly unlikely to be effective. We are now gathering data on an intervention for persons high in emotion-related impulsivity that relies on preplanning and behavioral strategies that are not cognitively demanding when called for. On the other hand, as noted earlier, we are also testing cognitive remediation that is aimed at improving response inhibition per se (Peckham & Johnson, 2018).
Disentangling Urgencies from Related Constructs
A related issue follows from the origins of our own interest in this topic. We got here partly via an interest in dual process models, in which reactivity to emotion plays a role. However, this is not the only feature of such models. A reasonable question is whether the true vulnerability factor is instead a bias toward reactive-mode functioning more generally—to behave in a way that is dictated heavily by habit (Gillan et al., 2011; Gillan & Robbins, 2014; Gillan et al., 2016; Morris et al., 2016; Ouellette & Wood, 1998; Watson, Wiers, Hommel, & de Wit, 2014; Wood, 2017; Wood & Neal, 2007; Wood & Rünger, 2016; Worbe, Savulich, de Wit, Fernandez-Egea, & Robbins, 2015). Habitual responses are often linked to particular emotions, but, in principle, they need not be.
Arguing for a more general influence of the reactive mode (not reactivity to emotions per se) would seem to be nearly the same as arguing that impaired response inhibition is really the phenomenon of interest. Several findings are at least consistent with the view that excessive reliance on habit (reactive mode) may be the real culprit. As noted in an earlier section, there are a number of studies linking disorder to impaired response inhibition per se (which is about overriding habit). Another source of information is associations of the serotonin transporter polymorphism with other variables. As noted earlier, this gene has been linked to emotion-related impulsivity (Carver et al., 2011). However, other research has linked serotonergic deficits to a more general bias toward habit-based responding (Sanchez, Bishop, Herpetz, Gaber, Kuhn, Hood, & Zepf, 2015; Worbe et al., 2015) and reflexive (automatic) processing (Maddox et al., 2017). More information on whether reactions to emotion per se are critical to the phenomena of greatest interest (i.e., vulnerability to psychopathology) is obviously needed.
It is also important to acknowledge that even apart from impaired response inhibition, emotion-related impulsivity shares overlap, conceptual and empirical, with other variables that are known risk factors for psychopathology. These include emotionality per se (neuroticism, negative affectivity), and variables tied to both emotionality and cognitive control, such as rumination and impaired emotion regulation (Wray, Simons, Dvorak, & Gather, 2012; Fossati Gratz, Maffei, & Borroni, 2014; Valderrama & Miranda, 2017). This overlap is not trivial, given the extensive work relating these other constructs to psychopathology (Aldao et al., 2010; Joormann & Gotlib, 2010; Kotov et al., 2010; Sheppes et al., 2015; Watkins, 2008).
Several lines of work suggest that impulsive responses to emotion can be differentiated from the intensity of the emotion itself. First, as noted earlier, most variance in Negative Urgency is not explained by neuroticism (Cyders & Smith, 2008). Second, persons with emotion-related impulsivity do not have elevated subjective affective or psychophysiological responses to standardized stimuli (Cyders, Coskunpinar, & Lehman, 2012; Cyders et al., 2010; Johnson et al., 2016). Third, there is evidence that impulsive responses to emotion predict psychopathology above and beyond neuroticism or similar tendencies (Cyders & Coskunpinar, 2010; Kaiser, Milich, Lynam, & Charnigo, 2012; Peterson, Davis-Becker, & Fischer, 2014; Riley, Rukavina, & Smith, 2016), and that the effects of emotion-related impulsivity are more powerful than are tendencies to be emotional per se (Kaiser et al., 2012; Settles, Fischer, Cyders, et al., 2012).
Perhaps the domains of greatest overlap with emotion-related impulsivity are variables that involve both emotion and cognitive control in some fashion, such as emotion regulation problems (Buhle et al., 2014) and rumination (Joormann & Gotlib, 2010). Despite the conceptual similarities, research thus far suggests that Negative Urgency is related to psychopathology above and beyond effects of rumination (Valderrama & Miranda, 2017). Negative Urgency has also been found to amplify the effects of poor emotion regulation on psychopathology rather than being redundant with it (Dir et al., 2016). Despite the evidence for unique contributions of emotion-related impulsivity, disentangling various manifestations of poor control over emotion, and their combined role in predicting psychopathology, remains an important goal.
Can all of these constructs be folded into a view in which deficits pertaining to constraint over emotion are one reflection of a broader process with multiple manifestations? Perhaps one of the manifestations will prove to be more reliable as a “core” driver of psychopathology than others. Perhaps there is an element shared among these variables that is the real quality of importance, which is not captured perfectly by any of these variables.
What criteria should be used in evaluating the constructs? At a minimum, relevant criteria would seem to include clinical utility in guiding diagnosis and treatment, and the extent to which a target variable merges into a broader view of personality or organismic functioning. As these broader views wax and wane, the angles from which we evaluate the constructs will also shift.
Constructs and Operationalizations
A well-known and important foundational goal of psychological research is to improve operationalizations of the constructs we use. Less emphasized, but equally important, is continuing to reexamine the constructs themselves, and sometimes refining them. The impetus for reexamining the construct can come from many places, and theorists should be open to considering as many of them as we can. Study of impulsivity as a psychological construct has benefited from views of people from several areas: personality, affective science, cognitive science, and psychopathology. Perhaps most importantly, knowledge from those various corners of science might not have received the attention it did receive were it not for a willingness of people in this area of work to approach these conceptual questions with fresh eyes, along with a collaborative and open approach to what emerged.
Acknowledgments
Work on this article was supported by National Institute of Mental Health grant 1R01MH110477.
Footnotes
Editor’s note. Janice K. Kiecolt-Glaser received a 2018 APA Award for Distinguished Scientific Contributions. This article is based on an invited presentation at the 126th Annual Convention of the American Psychological Association, held August 9–12, 2018, San Francisco, California.
Contributor Information
Charles S. Carver, University of Miami
Sheri L. Johnson, University of California, Berkeley
References
- Aldao A, Nolen-Hoeksema S, & Schweizer S, (2010). Emotion-regulation strategies across psychopathology: A meta-analytic review. Clinical Psychology Review, 30, 217–237. [DOI] [PubMed] [Google Scholar]
- Auerbach RP, Stewart JG, & Johnson SL (2016). Impulsivity and suicidality in adolescent inpatients. Journal of Abnormal Child Psychology, 1–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bagge CL, Littlefield AK, Rosellini AJ, & Coffey SF (2013). Relations among behavioral and questionnaire measures of impulsivity in a sample of suicide attempters. Suicide & Life-Threatening Behavior, 43, 460–467. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barratt ES (1965). Factor analysis of some psychometric measures of impulsiveness and anxiety. Psychological Reports, 16, 541–554. [DOI] [PubMed] [Google Scholar]
- Beauchaine TP, Zisner AR, & Sauder CL (2017). Trait impulsivity and the externalizing spectrum. Annual Review of Clinical Psychology, 13, 343–368. [DOI] [PubMed] [Google Scholar]
- Bechara A (2005). Decision making, impulse control and loss of will-power to resist drugs: A neurocognitive perspective. Nature Neuroscience, 8, 1458–1463. [DOI] [PubMed] [Google Scholar]
- Bechara A, & Van der Linden M (2005). Decision-making and impulse control after frontal lobe injuries. Current Opinion in Neurology, 18(6), 734–739. [DOI] [PubMed] [Google Scholar]
- Berg JM, Latzman RD, Bliwise NG, & Lilienfeld SO (2015). Parsing the heterogeneity of impulsivity: A meta-analytic review of the behavioral implications of the UPPS for psychopathology. Psychological Assessment, 27, 1129–1146. [DOI] [PubMed] [Google Scholar]
- Block J (2002). Personality as an affect-processing system: Toward an integrative theory. Mahwah, NJ: Erlbaum. [Google Scholar]
- Block JH, & Block J (1980). The role of ego-control and ego-resiliency in the organization of behavior In Collins WA (Ed.), Development of cognition, affect, and social relations (Minnesota symposia on child psychology, Vol. 13, pp. 39–101). Hillsdale, NJ: Erlbaum. [Google Scholar]
- Bocanegra BR, & Hommel B (2014). When cognitive control is not adaptive. Psychological Science, 25, 1249–1255. [DOI] [PubMed] [Google Scholar]
- Bora E, Yucel M & Pantelis C (2009). Cognitive endophenotypes of bipolar disorder: A meta-analysis of neuropsychological deficits in euthymic patients and their first-degree relatives. Journal of Affective Disorders, 113, 1–20. [DOI] [PubMed] [Google Scholar]
- Buckholz JW (2015). Social norms, self-control, and the value of antisocial behavior. Current Opinion in Behavioral Sciences, 3, 122–129. [Google Scholar]
- Buhle JT, Silvers JA, Wager TD, Lopez R, Onyemekwu C, Kober H, et al. (2014). Cognitive reappraisal of emotion: A meta-analysis of human neuroimaging studies. Cerebral Cortex, 24, 2981–2990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carver CS, Johnson SL, & Joormann J (2008). Serotonergic function, two-mode models of self-regulation, and vulnerability to depression: What depression has in common with impulsive aggression. Psychological Bulletin, 134, 912–943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carver CS, Johnson SL, & Joormann J (2013). Major depressive disorder and impulsive reactivity to emotion: Toward a dual process view of depression. British Journal of Clinical Psychology, 52, 285–299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carver CS, Johnson SL, Joormann J, Kim Y, & Nam JY (2011). Serotonin transporter polymorphism interacts with childhood adversity to predict aspects of impulsivity. Psychological Science, 22, 589–595. [DOI] [PubMed] [Google Scholar]
- Carver CS, Johnson SL, & Timpano KR (2017). Toward a functional view of the p factor in psychopathology. Clinical Psychological Science, 5, 880–889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carver CS, & Miller CJ (2006). Relations of serotonin function to personality: Current views and a key methodological issue. Psychiatry Research, 144, 1–15. [DOI] [PubMed] [Google Scholar]
- Caspi A, Houts RM, Belsky DW, Goldman-Mellor SJ, Harrington H, Israel S, et al. (2014). The P-factor: One general psychopathology factor in the structure of psychiatric disorders? Clinical Psychological Science, 2, 119–137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chester DS, Lynam DR, Milich R, Powell DK, Andersen AH, & Dewall CN (2016). How do negative emotions impair self-control? A neural model of negative urgency. NeuroImage, 132, 43–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Costa PT Jr., & McCrae RR (1992). NEO-PI–R professional manual. Odessa, FL: Psychological Assessment Resources. [Google Scholar]
- Cuthbert BN (2015). Research domain criteria: Toward future psychiatric nosologies. Dialogues in Clinical Neuroscience, 17, 89–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cuthbert BN & Insel TR (2013). Toward the future of psychiatric diagnosis: The seven pillars of RDoC. BMC Medicine, 11, 1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cyders MA, & Coskunpinar A (2010). Is urgency emotionality? Separating urgent behaviors from effects of emotional experiences. Personality & Individual Differences, 48, 839–844. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cyders MA, & Coskunpinar A (2011). Measurement of constructs using self-report and behavioral lab tasks: Is there overlap in nomothetic span and construct representation for impulsivity? Clinical Psychology, 31, 965–982. [DOI] [PubMed] [Google Scholar]
- Cyders MA, Coskunpinar A, & Lehman ZA (2012). Difficulties and advancements in the assessment and induction of emotion-based impulsivity: Development of the Three-Task Procedure In Cyders MA (Ed.), Psychology of impulsivity (pp. 237–258). Nova Science Publishers. [Google Scholar]
- Cyders MA, Zapolski TCB, Combs JL, Settles RF, Fillmore MT, & Smith GT (2010). Experimental effect of positive urgency on negative outcomes from risk taking and on increased alcohol consumption. Psychology of Addictive Behaviors, 24, 367–375. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cyders MA, & Smith GT (2007). Mood-based rash action and its components: Positive and negative urgency. Personality and Individual Differences, 43(4), 839–850. [Google Scholar]
- Cyders MA, & Smith GT (2008). Emotion-based dispositions to rash action: Positive and negative urgency. Psychological Bulletin, 134, 807–828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cyders MA, Smith GT, Spillane NS, Fischer S, Annus AM, & Peterson C (2007). Integration of impulsivity and positive mood to predict risky behavior: Development and validation of a measure of positive urgency. Psychological Assessment, 19, 107–118. [DOI] [PubMed] [Google Scholar]
- d’Acremont M, & Van der Linden M (2007). How is impulsivity related to depression in adolescence? Evidence from a French validation of the cognitive emotion regulation questionnaire. Journal of Adolescence, 30, 271–282. [DOI] [PubMed] [Google Scholar]
- Daw ND, Niv Y, & Dayan P (2005). Uncertainty-based competition between prefrontal and dorsolateral striatal systems for behavioral control. Nature Neuroscience, 8, 1704–1711. [DOI] [PubMed] [Google Scholar]
- Dayan P (2008). Simple substrates for complex cognition. Frontiers in Neuroscience, 2, 255–263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dekker MR, & Johnson SL (2018). Major depressive disorder and emotion-related impulsivity: Are both related to cognitive inhibition? Cognitive Therapy and Research, 42, 398–407. [Google Scholar]
- Depue RA (1995). Neurobiological factors in personality and depression. European Journal of Personality, 9, 413–439. [Google Scholar]
- Depue RA, & Collins PF (1999). Neurobiology of the structure of personality: Dopamine, facilitation of incentive motivation, and extraversion. Behavioral and Brain Sciences, 22, 491–569. [DOI] [PubMed] [Google Scholar]
- Depue RA, & Spoont MR (1986). Conceptualizing a serotonin trait: A behavioral dimension of constraint. Annals of the New York Academy of Sciences, 487, 47–62. [DOI] [PubMed] [Google Scholar]
- Dickman SJ (1990). Functional and dysfunctional impulsivity: Personality and cognitive correlates. Journal of Personality and Social Psychology, 58, 95–102. [DOI] [PubMed] [Google Scholar]
- Dir AL, Banks DE, Zapolski TCB, McIntyre E, & Hulvershorn LA (2016). Negative urgency and emotion regulation predict positive smoking expectancies in non-smoking youth. Additive Behaviors, 58, 47–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dolan RJ, & Dayan P (2013). Goals and habits in the brain. Neuron, 80, 312–325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eisenberg N (2002). Emotion-related regulation and its relation to quality of social functioning, In Hartup WW & Weinberg RA (Eds.), Child psychology in retrospect and prospect: The Minnesota symposium on child psychology (Vol. 32, pp. 133–171). Mahwah, NJ: Erlbaum. [Google Scholar]
- Evans J. St. B. T., & Stanovich KE (2013). Dual-process theories of higher cognition: Advancing the debate. Perspectives on Psychological Science, 8, 223–241. [DOI] [PubMed] [Google Scholar]
- Eysenck HJ, & Eysenck SBG (1968). Manual of the Eysenck Personality Inventory. London, England: University of London Press. [Google Scholar]
- Eysenck SBG, & Eysenck HJ (1975). Manual of the Eysenck Personality Questionnaire. London, England: Hodder & Stoughton. [Google Scholar]
- Fischer S, Smith GT, & Cyders MA (2008). Another look at impulsivity: A meta analytic review of trait impulsivity and its association with bulimic symptoms. Clinical Psychology Review, 28, 1413–1425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fossati A, Gratz KL, Maffei C, & Borroni S (2014). Impulsivity dimensions, emotions dysregulation, and borderline personality disorder features among Italian nonclinical adolescents. Borderline Personality Disorder and Emotional Dysregulation, 5, 1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gay P, Rochat L, Billieux J, d’Acremont M, & Van der Linden M (2008). Heterogeneous inhibition processes involved in different facets of self-reported impulsivity: Evidence from a community sample. Acta Psychologica, 129, 332–339. [DOI] [PubMed] [Google Scholar]
- Gillan CM, Kosinski M, Whelan R, Phelps EA, & Daw ND (2016). Characterizing a psychiatric symptom dimension related to deficits in goals-directed control. E-Life, 5, e11305, 1–24 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gillan CM, & Robbins TW (2014). Goal-directed learning and obsessive compulsive disorder. Philosophical Transactions of the Royal Society B, 369, 1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Granö N, Keltikangas-Järvinen L, Kouvonen A, Virtanen M, Elovainio M, Vahtera J & Kivimäki M (2007). Impulsivity as a predictor of newly diagnosed depression. Scandinavian Journal of Psychology, 48, 173–179. [DOI] [PubMed] [Google Scholar]
- Gunn RL, & Finn PR (2015). Applying a dual process model of self-regulation: The association between executive working memory capacity, negative urgency, and negative mood induction on pre-potent response inhibition. Personality & Individual Differences, 75, 210–215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gustavson DE. (personal communication, October 24, 2017).
- Gustavson DE, du Pont A, Hatoum AS, Rhee SH, Kremen WS, Hewitt JK, & P.Friedman NP, (2017). Genetic and environmental associations between procrastination and internalizing/externalizing psychopathology. Clinical Psychological Science, 5, 798–815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hooper MW, & Carver CS (2016). Reflexive reaction to feelings predicts failed smoking cessation better than does lack of general self-control. Journal of Consulting and Clinical Psychology, 84, 612–618. [DOI] [PubMed] [Google Scholar]
- Hoptman MJ, Antonius D, Mauro CJ, Parker EM, & Javitt DC (2014). Cortical thinning, functional connectivity, and mood-related impulsivity in schizophrenia: Relationship to aggressive attitudes and behavior. American Journal of Psychiatry, 171, 939–948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson SL, Tharp JA, Peckham AD, Sanchez AH, Carver C (2016). Positive urgency is related to difficulty inhibiting prepotent responses. Emotion, 16, 750–758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Joormann J & Gotlib IH (2010). Emotion regulation in depression: Relation to cognitive inhibition. Cognition and Emotion, 24, 281–298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kahneman D (2011). Thinking, fast and slow. New York, NY: Farrar, Straus and Giroux. [Google Scholar]
- Kaiser A, Bonsu JA, Charnigo RJ, Milich R, & Lynam DR (2016). Impulsive personality and alcohol use: Bidirectional relations over one year. Journal of Studies on Alcohol and Drugs, 77, 473–482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaiser AJ, Milich R, Lynam DR, & Charnigo RJ (2012). Negative urgency, distress tolerance, and substance abuse among college students. Addictive Behaviors, 37, 1075–1083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Karyadi KA, & King K (2011). Urgency and negative emotions: Evidence for moderation on negative alcohol consequences. Personality and Individual Differences, 51, 635–640. [Google Scholar]
- Kasen S, Cohen P, & Chen H (2011). Developmental course of impulsivity and capability from age 10 to age 25 as related to trajectory of suicide attempt in a community cohort. Suicide and Life-threatening Behavior, 41, 180–192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kotov R, Gamez W, Schmidt F, & Watson D (2010). Linking “big” personality traits to anxiety, depressive, and substance use disorders: a meta-analysis. Psychological Bulletin, 136, 768–821. [DOI] [PubMed] [Google Scholar]
- Krueger RF, & Markon KE (2006). Reinterpreting comorbidity: A model-based approach to understanding and classifying psychopathology. Annual Review of Clinical Psychology, 2, 111–133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lacey JH, & Evans CDH (1986). The impulsivist: A multi-impulsive personality disorder. British Journal of Addiction, 81, 64–649. [DOI] [PubMed] [Google Scholar]
- Littlefield AK, Stevens AK, Ellingson JM, King KM, & Jackson KM (2016). Changes in negative urgency, positive urgency, and sensation seeking across adolescence. Personality and Individual Differences, 90, 332–337. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lopez-Vergara H, Spillane NS, Merrill JE, & Jackson KM (2016). Developmental trends in alcohol use initiation and escalation from early to middle adolescence: Prediction by urgency and trait affect. Psychology of Addictive Behaviors, 30, 578–587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lynam D, Smith GT, Cyders MA, Fischer S, & Whiteside SA (2007). The UPPS-P: A multidimensional measure of risk for impulsive behavior (Technical report). West Lafayette, IN: Purdue University. [Google Scholar]
- Maddox WT, Gorlick MA, Koslov S, McGeary JE, Knopik VS, & Beevers CG (2017). Serotonin transporter genetic variation is differentially associated with reflexive- and reflective-optimal learning. Cerebral Cortex, 27, 1182–1192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Manuck SB, Kaplan JR, & Lotrich FE (2006). Brain serotonin and aggressive disposition in humans and nonhuman primates In Nelson RJ (Ed.) Biology of Aggression (pp. 65–102). New York: Oxford University Press. [Google Scholar]
- Marmorstein NR (2013). Associations between dispositions to rash action and internalizing and externalizing symptoms in children. Journal of Clinical Child and Adolescent Psychology, 42, 131–138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Metcalfe J, & Mischel W (1999). A hot/cool-system analysis of delay of gratification: Dynamics of willpower. Psychological Review, 106, 3–19. [DOI] [PubMed] [Google Scholar]
- Miller J, Flory K, Lynam D, & Leukefeld C (2003). A test of the four-factor model of impulsivity-related traits. Personality and Individual Differences, 34, 1403–1418. [Google Scholar]
- Moeller FG, Barratt ES, Dougherty DM, Schmitz JM, & Swann AC (2001). Psychiatric aspects of impulsivity. American Journal of Psychiatry, 158, 1783–1793. [DOI] [PubMed] [Google Scholar]
- Morris LS, Kundu P, Irvine MA, Harrison NA, Robbins TW, Daw N, et al. (2016). Latent substrates of compulsivity and behavioral flexibility. European Neuropsychopharmacology, 26, 892–893. [Google Scholar]
- Muhtadie L, Johnson SL, Carver CS, & Gotlib IH (2014). A profile approach to impulsivity in bipolar disorder: The key role of strong emotions. Acta Psychiatrica Scandinavica, 129, 100–108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Institute of Mental Health (2016). Behavioral assessment methods for RDoC Constructs. A report by the National Advisory Mental health council workgroup on tasks and measures for research domain criterial (RDoC) 1–161. https://www.nimh.nih.gov/about/advisory-boards-and-groups/namhc/reports/rdoc_council_workgroup_report_153440.pdf [Google Scholar]
- Nigg JT (2000). On inhibition/disinhibition in developmental pychopathology: Views from cognitive and personality psychology and a working inhibition taxonomy. Psychological Bulletin, 126, 220–246. [DOI] [PubMed] [Google Scholar]
- Otto AR, Gershman SJ, Markman AB, & Daw ND (2013). The curse of planning: Dissecting multiple reinforcement learning systems by taxing the central executive. Psychological Science, 24, 751–761. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ouellette JA, & Wood W (1998). Habit and intention in everyday life: The multiple processes by which past behavior predicts future behavior. Psychological Bulletin, 124, 54–74. [Google Scholar]
- Pang RD, Farrahi L, Glazier S, Sussman S, & Leventhal AM (2014). Depressive symptoms, negative urgency, and substance use initiation in adolescents. Drug and Alcohol Dependence,144, 225–230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patton JH, Stanford MS, & Barratt ES (1995). Factor structure of the Barratt Impulsiveness Scale. Journal of Clinical Psychology, 51, 768–774. [DOI] [PubMed] [Google Scholar]
- Pearlstein J, Johnson SL, Modavi K, Peckham A & Carver CS (in press). Neurocognitive Mechanisms of Emotion-Related Impulsivity: The Role of Arousal. Psychophysiology. Pending minor revisions. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pearlstein JG, Johnson SL, Timpano KR, Carver CS, (2018). Emotion-related impulsivity and the general psychopathology factor. Manuscript in preparation. [DOI] [PubMed]
- Peckham AD & Johnson SL (2018). Cognitive control training for emotion-relevant impulsivity. Behaviour Resarch and Therapy, 105, 17–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peterson CM, Davis-Becker K, & Fischer S (2014). Interactive role of depression, distress tolerance and negative urgency on non-suicidal self-injury. Personal Mental Health, 8, 151–160. [DOI] [PubMed] [Google Scholar]
- Quinn ME, & Joormann J (2015). Stress-induced changes in executive control are associated with depression symptoms: Examining the role of rumination. Clinical Psychological Science, 3, 628–636. [Google Scholar]
- Riley EN, Combs JL, Jordan CE, & Smith GT (2015). Negative urgency and lack of perseverance: Identification of differential pathways of onset and maintenance risk in the longitudinal prediction of nonsuicidal self-injury. Behavior Therapy, 46, 439–448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Riley EN, Rukavina M, & Smith GT (2016). The reciprocal predictive relationship between high-risk personality and drinking: An 8-wave longitudinal study in early adolescents. Journal of Abnormal Psychology, 125, 798–804. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roberts W, Fillmore MT, & Milich R (2011). Linking impulsivity and inhibitory control using manual and oculomotor response inhibition tasks. Acta Psychologica, 138, 419–428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rothbart MK, Ellis LK, Rueda MR, & Posner MI (2003). Developing mechanisms of temperamental effortful control. Journal of Personality, 71, 1113–1143. [DOI] [PubMed] [Google Scholar]
- Schalling D, & Edman G (1987). Personality and vulnerability to psychopathology: The development of the Karolinska Scales of Personality (KSP). Stockholm: Karolinska Institute. [Google Scholar]
- Settles R, Fischer S, Cyders MA, Combs JL, Gunn RL, & Smith GT (2012). Urgency: A personality predictor of externalizing behavior characterized by neuroticism, low conscientiousness, and disagreeableness. Journal of Abnormal Psychology, 121, 160–172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Settles RE, Zapolski TCB, & Smith GT (2014). Longitudinal test of a developmental model of the transition to early drinking. Journal of Abnormal Psychology, 123, 141–151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sharma L, Markon K, & Clark LA (2014). Toward a theory of distinct types of “impulsive” behaviors: A meta-analysis of self-report and behavioral measures. Psychological Bulletin, 140, 374–408. [DOI] [PubMed] [Google Scholar]
- Sheppes G, Suri G, & Gross JJ, (2015). Emotion regulation and psychopathology. Annual Review of Clinical Psychology, 11, 379–405. [DOI] [PubMed] [Google Scholar]
- Smith GT, Fischer S, Cyders MA, Annus AM, Spillane NS, & McCarthy DM (2007). On the validity and utility of discriminating among impulsivity-like traits. Assessment, 14,155–170. [DOI] [PubMed] [Google Scholar]
- Smith GT, Guller L, & Zapolski TC (2013). A comparison of two models of urgency: Urgency predicts both rash action and depression in youth. Clinical Psychological Science, 1, 266–275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Snyder HR (2013). Major depressive disorder is associated with broad impairments on neuropsychological measures of executive function: A meta-analysis and review. Psychological Bulletin, 139, 81–132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sperry SH, Lynam DP, & Kwapil TR, (in press). The convergence and divergence of impulsivity facets in daily life. Journal of Personality. [DOI] [PubMed] [Google Scholar]
- Spoont MR (1992). Modulatory role of serotonin in neural information processing: Implications for human psychopathology. Psychological Bulletin, 112, 330–350. [DOI] [PubMed] [Google Scholar]
- Stojek M, & Fischer S (2013). Impulsivity and motivations to consume alcohol: A prospective study on risk of dependence in young adult women. Alcoholism: Clinical and Experimental Research, 37, 292–299. [DOI] [PubMed] [Google Scholar]
- Strack F, & Deutsch R (2004). Reflective and impulsive determinants of social behavior. Personality and Social Psychology Review, 8, 220–247. [DOI] [PubMed] [Google Scholar]
- Tangney JP, Baumeister RF, & Boone AL (2004). High self-control predicts good adjustment, less pathology, better grades, and interpersonal success. Journal of Personality, 72, 271–324. [DOI] [PubMed] [Google Scholar]
- Tellegen A (1985). Structures of mood and personality and their relevance to assessing anxiety, with an emphasis on self-report In Tuma AH & Maser JD (Eds.), Anxiety and the anxiety disorders (pp. 681–706). Hillsdale, NJ: Erlbaum. [Google Scholar]
- Toates F (2006). A model of the hierarchy of behaviour, cognition, and consciousness. Consciousness and Cognition: An International Journal, 15, 75–118. [DOI] [PubMed] [Google Scholar]
- Uher R, & McGuffin P (2010). The moderation by the serotonin transporter gene of environmental adversity in the aetiology of depression: 2009 update. Molecular Psychiatry, 15, 18–22. [DOI] [PubMed] [Google Scholar]
- Valderrama J, & Miranda R (2017). Early life stress predicts negative urgency through brooding, depending on 5-HTTLPR genotype: A pilot study with 6-month follow-up examining suicide ideation. Psychiatry Research, 258, 481–487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Venables NC, Foell J, Yancey JR, Kane MJ, Engle RW, & Patrick CJ (2018). Quantifying inhibitory control as externalizing proneness: A cross-domain model. Clinical Psychological Science, in press. [Google Scholar]
- Walsh MM, & Anderson JR (2014). Navigating complex decision spaces: Problems and paradigms in sequential choice. Psychological Bulletin, 140, 466–486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watkins ER (2008). Constructive and unconstructive repetitive. thought. Psychological Bulletin, 134, 163–206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson P, Wiers RW, Hommel B, & de Wit S (2014). Working for food you don’t desire. Cues interfere with goal-directed food-seeking. Appetite, 79, 139–148. [DOI] [PubMed] [Google Scholar]
- Whiteside SP, & Lynam DR (2001). The five factor model and impulsivity: Using a structural model of personality to understand impulsivity. Personality and Individual Differences, 30, 669–689. [Google Scholar]
- Wilbertz T, Deserno L, Horstmann A, Neumann J, Villringer A, Heinze HJ, et al. (2014). Response inhibition and its relation to multidimensional impulsivity. NeuroImage, 103, 241–248. [DOI] [PubMed] [Google Scholar]
- Wood W (2017). Habit in personality and social psychology. Personality and Social Psychology Review, 21, 389–403. [DOI] [PubMed] [Google Scholar]
- Wood W, & Neal DT (2007). A new look at habits and the habit–goal interface. Psychological Review, 114, 843–863. [DOI] [PubMed] [Google Scholar]
- Wood W, & Rünger D (2016). Psychology of habit. Annual Review of Psychology, 67, 289–314. [DOI] [PubMed] [Google Scholar]
- Worbe Y, Savulich G, de Wit S, Fernandez-Egea E, & Robbins TW (2015). Tryptophan depletion promotes habitual over goal-directed control of appetitive responding in humans. International Journal of Neuropsychopharmacology, 18: pyv013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wray TB, Simons JS, Dvorak RD, & Gaher, (2012), Trait-based affective processes in alcohol-involved “risk behaviors.” Addictive Behavior, 37, 1230–1239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wright L, Lipszyc J, Thayapararajah SW, & Schachar R (2014). Response inhibition and psychopathology: A meta-analysis of go/no-go task performance. Journal of Abnormal Psychology, 123, 429–439. [DOI] [PubMed] [Google Scholar]
- Young SE, Friedman NP, Miyake A, Willcutt EG, Corley RP, Haberstick BC, & Hewitt JK (2009). Behavioral disinhibition: Liability for externalizing spectrum disorders and its genetic and environmental relation to response inhibition across adolescence. Journal of Abnormal Psychology, 118, 117–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zapolski TCB, Cyders MA, & Smith GT (2009). Positive urgency predicts illegal drug use and risky sexual behavior. Psychology of Addictive Behaviors, 23, 348–354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zapolski TCB, Stairs AM, Settles RF, Combs JL, & Smith GT (2010). The measurement of dispositions to rash action in children. Assessment, 17, 116–125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zapolski TCB, Smith GT, (2013). Comparison of parent versus child-report of child impulsivity traits and prediction of outcome variables. Journal of Psychopathology and Behavioral Assessment, 35, 301–313. [DOI] [PMC free article] [PubMed] [Google Scholar]