
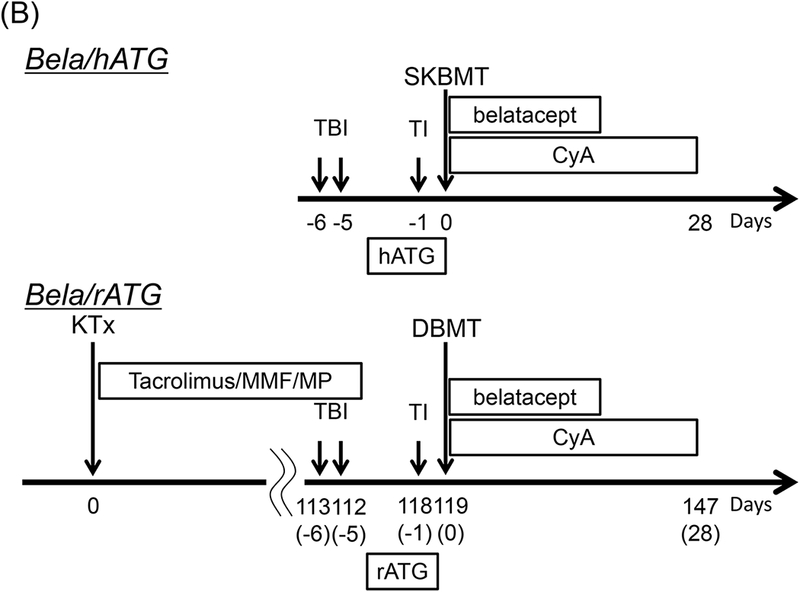
Figure 1: The DBMT conditioning regimens with or without anti-CD40 mAb.
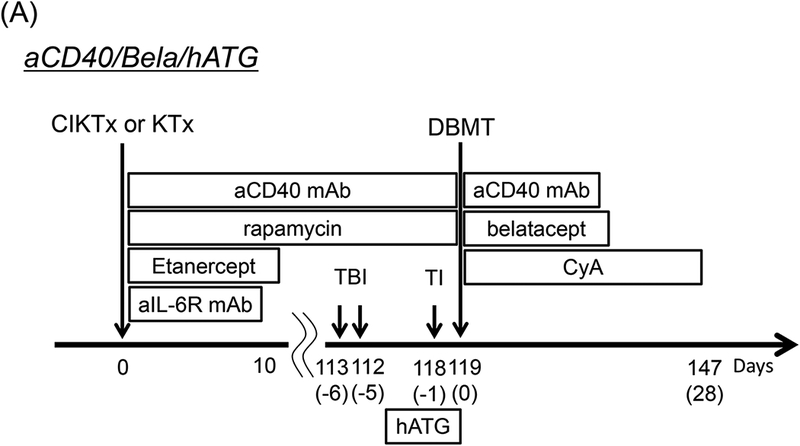
aCD40/Bela/hATG: Two to 3 weeks before combined islet and kidney transplantation (CIKTx), cynomolgus monkey recipients received streptozotocin (STZ: 75 mg/kg) for induction of diabetes. After transplantation, the CIKTx or kidney transplant (KTx)-alone recipients received the same immunosuppressive therapy with anti-CD40 mAb and rapamycin for 4 months. Anti-inflammatory therapies included anti-IL-6R mAb (10 mg/kg) and TNF-alpha receptor fusion protein (Etanercept: 25 mg) up to day 10 (A).3 At four months after transplantation, all recipients were conditioned with total body irradiation (TBI: 1.5 Gy × 2 on days −6 and −5, relative to DBMT), local thymic irradiation (TI: 7 Gy on day −1, relative to DBMT), and horse anti-thymocyte globulin (hATG: 50 mg/kg ×c 3 on days −2, −1 and 0, relative to DBMT). Following donor bone marrow transplantation (DBMT), the recipients were treated with dual costimulatory blockade (CB) with anti-CD40 mAb (20 mg/kg, on post-DBMT days 0, 2, 5, 7, 9, and 12) and belatacept (20 mg/kg, on post-DBMT days 0, 2, 5, and 15). Cyclosporine A (CyA) was administered for 28 days following DBMT, after which no immunosuppression was administered (A).
Bela/hATG: In a previous study, the conditioning regimen consisted of low-dose TBI (1.5 Gy × 2) on days −6 and −5 relative to simultaneous kidney and bone marrow transplantation (SKBMT), TI on day-1, hATG (50 mg/kg × 3 on days −2, −1, and 0) and belatacept (20 mg/kg × 4 on days 0, 2, 5, and 15). A 1-month course of CyA was administered to maintain therapeutic trough levels of 250–350 ng/ml (B).1
Bela/rATG: In the previous deceased donor study, all recipients initially underwent KTx alone with a conventional triple drug immunosuppressive regimen consisting of tacrolimus, mycophenolate mofetil, and prednisone (B). Four months after KTx alone, the recipients underwent conditioning and DBMT (delayed-DBMT). The conditioning regimen for DBMT is same as the Bela/hATG regimen, except the hATG was replaced with rATG (B).2