

Abstract
Background:
Inpatient cardiac rehabilitation (ICR) programs provide important services to hospitalized patients by delivering risk factor education, daily ambulation, and facilitation of referral to outpatient cardiac rehabilitation. However, little is known about ICR utilization or practice patterns.
Methods:
We examined the use of ICR, between January 2007 and June 2011, in a geographically and structurally diverse sample of US hospitals (Premier, Inc.).
Results:
Among 458 hospitals, there were 1 343 537 admissions with a qualifying diagnosis for outpatient cardiac rehabilitation. Formal ICR was available at 223 (49%) of these hospitals. Overall, patient utilization of ICR was low (21.2%) and varied by indication. Utilization was highest in those undergoing cardiac surgery (43.3%) and lowest in patients with medically managed myocardial infarction (15.6%) or heart failure (10.6%). A larger bed count, the presence of cardiac interventional services, and Midwest location were associated with increased likelihood of a hospital having an ICR program. In multivariable hierarchical analysis adjusting for known hospital characteristics among hospitals that provided ICR, multiple patient factors were associated with a lower likelihood of ICR utilization, including older age, more comorbidities, female sex, and Medicare insurance, but unspecified hospital characteristics explained the vast majority of the variability.
Conclusions:
We found substantial variation in the delivery of ICR across US hospitals and by patient condition. Overall, only a minority of eligible patients ever received ICR and fewer than half of hospitals treating cardiac patients provided formal ICR services. This substantial gap in the secondary prevention of heart disease warrants further investigation and intervention.
Keywords: cardiac rehabilitation, inpatient, utilization, epidemiology, phase 1
CONDENSED ABSTRACT
The use of inpatient cardiac rehabilitation was evaluated in a sample of 458 hospitals across the United States. We found that only 21% of potentially eligible patients ever received inpatient cardiac rehabilitation and that most of this variability was due to the hospital where the patients received their care.
Each year, >2 million Americans are hospitalized for an acute cardiac condition or procedure such as acute myocardial infarction (MI), heart failure (HF), percutaneous coronary intervention (PCI), coronary artery bypass graft surgery (CABG), or heart valve surgery (HVS).1 After discharge, attending outpatient cardiac rehabilitation (CR) is a key step towards full recovery for these patients. However, despite strong evidence supporting the importance of outpatient CR,2–4 only 30–35% of patients attend outpatient CR, partly due to poor inpatient referral and weak facilitation of enrollment.5–8
As part of the initial recovery process, some hospitals provide a formal program of inpatient cardiac rehabilitation (ICR). These programs are responsible for providing patient ambulation, risk factor modification education, and motivation and encouragement to attend outpatient CR2 and are distinct from services provided during admissions to inpatient rehabilitation wards or hospitals. Prior studies reported that activities provided by ICR substantially increase participation in outpatient CR,9–11 improve patient satisfaction,12 and may reduce mortality.13 However, a prior survey suggested that ICR is not universally available,14 and based upon limited regional data from 1986 to 1997, was declining in use.15
Consequently, we sought to describe utilization of ICR in a more contemporary, large and diverse sample of US hospitals. We aimed to describe current trends in ICR utilization, services provided during an ICR visit, and the patient, hospital, and regional factors that influence the receipt of ICR. We hypothesized that, similar to outpatient CR, overall utilization of ICR would be low and that substantial variation in care would exist across the US.
METHODS
Study Design and Setting
We identified patients discharged from US hospitals that contribute to the Premier Healthcare Alliance Inpatient Database, which has been previously described.16 In brief, the database contains detailed administrative data from a geographically and structurally diverse group of more than 500 US hospitals representing approximately 15–20% of inpatient US hospitalizations. Unlike claims databases that contain only sociodemographic, diagnostic, and selected procedure codes assigned at the time of discharge, the Premier inpatient database contains date-stamped hospital service codes for all medications, procedures, diagnostic tests, and therapeutic services. Because the data are fully de-identified, the institutional review board at Baystate Medical Center determined that this study did not meet the Federal definition of research of human subjects.
Patient and Hospital Factors
We included all hospitalizations between January 2007 and June 2011 with an acute cardiac condition that, based upon Medicare insurance guidelines,17,18 were eligible to attend outpatient CR (MI, HF, CABG, HVS, PCI). Although HF was not a covered indication during the time frame of this study, we included patients with a principal diagnosis of HF as a baseline measure because CR for HF became a covered indication for CR by Medicare in February 2014 and the majority of private insurance companies now reimburse CR for patients with HF.18,19 We included patients with the following ICD-9 principal diagnosis codes: 410.x for MI and 428.x; 402.01; 402.11; 402.91; 404.03; 404.11; 404.13; 404.91; 404.94 for HF. Also included were patients with an ICD-9 procedure code (either primary or secondary) of 36.1x; 35.1x, 35.2x; or 36.06, 36.07, or 36.09 for patients with CABG, HVS, or PCI, respectively.
Because principal diagnoses and procedures are not mutually exclusive, we categorized patients into one of three mutually exclusive groups: surgical, PCI and medical. The surgical group included patients with either CABG, HVS, or combined CABG + HVS regardless of whether they had an MI or PCI. The PCI group included patients with elective PCI, urgent PCI (urgent hospital admission for PCI but without evidence for MI), or PCI + MI. The medical group included patients with medically managed MI and HF who did not have a PCI or cardiac surgery during the hospital admission. We used 3 strata (surgical, PCI, medical) for the main analysis and reporting, but also reported on the full 8 level strata (CABG, valve, CABG + valve, elective PCI, urgent PCI, PCI + MI, MI and HF) in supplemental online tables.
Demographic data was recorded including age, gender, race/ethnicity, insurance status for each admission, and computed a comorbidity score as described by Gagne.20 We calculated 29 individual comorbidity indicators based on methods developed by Elixhauser21 using software provided by Healthcare Costs and Utilization Project of the Agency for Healthcare Research and Quality. Hospital characteristics included size based on number of beds, teaching status, urban location, census region, and surgical volume.
Outcome Measures
Our primary outcome was the presence of ≥1 inpatient service code for any kind of ICR which we grouped by their content, differentiating them by CR exercise, CR education, and CR other (SDC Table 1). We also recorded the first hospitalization day in which a patient received ICR, the total number of days with ICR, and the proportion of total hospital days (days of ICR/hospital length of stay) that had a code for ICR. In cases where patients had multiple service codes, we counted only 1 code for ICR each day. Notably, the primary role of these codes is for tracking internal hospital process of care that influence hospital costs rather than for external billing or insurance claims. As such, these codes represent professionally delivered and tracked ICR associated with formal services, rather than informal education or ambulation offered by a nurse, physician or other non-CR professional.
Recognizing that physical therapy (PT) sometimes partially fills the role of ICR at some hospitals, especially at hospitals without an ICR program, we separately assessed all patients for ≥1 inpatient service code(s) for PT. We included only codes that seemed likely to have some component of exercise, ambulation, or risk-factor education and selected 52 of 236 available PT codes (SDC Table 1). We noted the type, timing, and dose of PT deliverer and reported this separately and distinctly from ICR utilization.
Statistical Analysis
We considered a hospital to provide ICR if 1 or more eligible patients received ICR service codes at the hospital. Similarly, hospital capability for cardiac surgery and PCI were determined by the presence of any patients with these procedures. Characteristics of patients and hospitals with and without ICR were compared using chi-square tests for categorical factors and Kruskal-Wallis tests for continuous factors. Restricting focus to patients receiving ICR, we then described the variation in type (education/evaluation/exercise), timing, and dose of ICR across patient strata (surgical, PCI, medical).
To assess trends in use of ICR, we restricted our analysis to hospitals that participated in the database during the entire 4.5-y study period and computed proportion of patients receiving ICR during each 6-mo interval of the study period. Temporal trends of ICR were assessed with the Cochran-Armitage trend test for overall group and within each stratum. To identify patient characteristics associated with use of ICR, we restricted analysis to hospitals that provided ICR, defined as having at least 1 patient with ICR within each 6-mo interval. We developed a hierarchical generalized linear model with a random hospital effect, using a logit link, that included patient demographics, the Gagne comorbidity score,20 selected comorbidities, and hospital characteristics. Age, race, and sex were forced into all models; all other factors with P > .05 were removed. Finally, intraclass correlation coefficients (ICC) were used to compare variation in ICR use across hospitals, taking into account patient characteristics in surgical, PCI and medical groups.22 All analyses were performed using SAS version 9.3 (SAS Institute).
RESULTS
During the study period, 1 343 537 patient admissions met inclusion criteria. Of these, 209 932 (15.6%) had a cardiac surgical procedure; 370 324 had a PCI (27.6%); 171 729, had MI without PCI (12.8%), and almost half of the total number of admissions 592 551 (44.1%) were for HF. Within each patient stratum, patient characteristics varied significantly by the receipt of ICR (Table 1). In general, patients with ICR were younger, had fewer comorbidities, were more often male, and were more likely to have non-Medicare insurance. Results for the full 8-stratum analysis are provided in SDC Table 2.
Table 1. Patient Characteristics by Group and by Receipt of Inpatient Cardiac Rehabilitationa.
| Surgical |
PCI |
Medical |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| No ICR | ICR | P Valueb | No ICR | ICR | P Valueb | No ICR | ICR | P Valueb | |
| Number of patients, n (%) | 119 100 (56.7) | 90 832 (43.3) | 271 607 (73.3) | 98 717 (26.7) | 674 102 (88.3) | 89 179 (11.7) | |||
| Age, yc | 67 (58 – 75) |
66 (58 – 74) |
<.001 | 65 (56 – 74) |
64 (55 – 74) |
<.001 | 76 (63 – 84) |
73 (61 – 83) |
<.001 |
| Female sex | 32.0 | 30.9 | <.001 | 34.5 | 34.5 | .89 | 50.2 | 48.0 | <.001 |
| Race/ethnicity | |||||||||
| White | 70.0 | 76.0 | <.001 | 68.8 | 73.5 | <.001 | 62.6 | 63.7 | <.001 |
| Black | 7.0 | 5.9 | 8.2 | 7.0 | 16.8 | 19.6 | |||
| Hispanic | 3.6 | 3.1 | 4.1 | 3.8 | 4.7 | 4.6 | |||
| Other | 19.5 | 15.0 | 18.9 | 15.7 | 15.8 | 12.1 | |||
| Marital status | |||||||||
| Married | 56.9 | 58.1 | <.001 | 53.9 | 54.7 | <.001 | 36.9 | 39.5 | <.001 |
| Single | 33.0 | 31.5 | 34.8 | 34.8 | 51.2 | 52.0 | |||
| Other | 10.1 | 10.3 | 11.3 | 10.5 | 11.8 | 8.5 | |||
| Insurance payor | |||||||||
| Medicare | 55.4 | 54.7 | <.001 | 51.1 | 49.5 | <.001 | 75.1 | 72.5 | <.001 |
| Medicaid | 5.6 | 4.8 | 6.1 | 4.7 | 6.7 | 6.1 | |||
| Managed care/Commercial Indemnity | 32.5 | 33.2 | 34.2 | 35.6 | 12.8 | 15.0 | |||
| Self-pay/Other | 6.5 | 7.3 | 8.7 | 10.2 | 5.4 | 6.4 | |||
| Gagne comorbidity scorec | 1 (0, 3) | 2 (0, 3) | <.001 | 0 (−1, 2) | 0 (−1, 2) | <.001 | 4 (3, 6) | 4 (2, 6) | <.001 |
| Selected comorbiditiesd | |||||||||
| Hypertension | 73.1 | 75.3 | <.001 | 70.4 | 68.0 | <.001 | 69.2 | 69.8 | .001 |
| Tobacco abuse disorder | <.001 | <.001 | <.001 | ||||||
| Former smoker | 20.9 | 20.7 | 14.9 | 13.5 | 14.9 | 15.2 | |||
| Current smoker | 18.0 | 20.9 | 23.5 | 26.0 | 12.3 | 15.4 | |||
| Nonsmoker | 61.1 | 58.4 | 61.5 | 60.4 | 72.8 | 69.4 | |||
| Diabetes | 38.1 | 38.5 | .09 | 33.9 | 31.6 | <.001 | 44.0 | 43.1 | <.001 |
| Atrial fibrillation | 34.2 | 32.5 | <.001 | 9.6 | 9.9 | .03 | 34.6 | 32.7 | <.001 |
| Congestive heart failure | 26.0 | 22.6 | <.001 | 14.8 | 14.4 | .003 | 51.9 | 54.9 | <.001 |
| Chronic pulmonary disease | 22.7 | 25.7 | <.001 | 15.7 | 15.8 | .33 | 34.8 | 33.1 | <.001 |
| Deficiency anemias | 20.7 | 22.0 | <.001 | 9.1 | 9.9 | <.001 | 30.0 | 27.6 | <.001 |
| Valvular disease | 20.5 | 19.9 | .01 | 9.2 | 9.7 | <.001 | 27.3 | 28.1 | <.001 |
| Obesity | 18.0 | 19.5 | <.001 | 13.1 | 14.0 | <.001 | 14.4 | 15.9 | <.001 |
| Peripheral vascular disease | 15.9 | 16.0 | .66 | 10.9 | 9.9 | <.001 | 13.5 | 13.9 | .001 |
| Acute kidney injury | 14.2 | 13.0 | <.001 | 5.2 | 5.4 | .08 | 18.0 | 19.0 | <.001 |
| Renal failure | 13.8 | 13.5 | .08 | 10.5 | 10.1 | <.001 | 37.9 | 36.7 | <.001 |
| Hypothyroidism | 10.0 | 10.2 | .35 | 8.2 | 8.5 | .003 | 16.2 | 14.7 | <.001 |
| Pulmonary circulation disease | 8.1 | 8.0 | .54 | 3.0 | 3.2 | <.001 | 15.6 | 16.3 | <.001 |
| Obstructive sleep apnea | 8.0 | 9.3 | <.001 | 4.9 | 5.9 | <.001 | 9.7 | 10.9 | <.001 |
| Depression | 6.7 | 7.7 | <.001 | 5.6 | 6.3 | <.001 | 9.6 | 9.3 | <.001 |
Abbreviations: ICR, inpatient cardiac rehabilitation; PCI, percutaneous coronary intervention.
Data reported as percentage or median (interquartile range), unless otherwise noted.
P values calculated using Chi-square test.
P values calculated using Kruskal-Wallis test.
Comorbidities with ≥5% prevalence.
Overall, patient level utilization of ICR at all hospitals was 20.8%, but this varied greatly by indication, ranging from 43.3% (surgical patients) to 11.7% (medically treated MI and HF) (Table 2). Between 2007 and 2011, utilization of ICR decreased, but only slightly, from 21.2% to 19.1%, P < .001. There was a more sizable, but still small, decline in ICR among surgical patients from 45.1% to 42.0%, P < .001. (SDC Figure 1).
Table 2. Utilization, Timing, and Dose of Inpatient Cardiac Rehabilitation and/or Physical Therapya.
| Total | Surgical | PCI | Medical | |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | n (%) | |
| 1 343 537 (100) | 209 932 (15.6) | 370 324 (27.6) | 763 281 (56.8) | |
| ICR utilization among all patients | 278 728 (20.8) | 90 832 (43.3) | 98 717 (26.7) | 89 179 (11.7) |
| Among patients with ICR | ||||
| Dose and timing of ICR | ||||
| ICR dose, d | 1 (1–2) | 3 (1–4) | 1 (1–2) | 1 (1–2) |
| LOS, d | 4 (2–7) | 8 (6–11) | 2 (1–4) | 4 (3–7) |
| Proportion of hospital days coveredb | 0.33 (0.18–0.50) | 0.28 (0.14–0.50) | 0.33 (0.25–0.50) | 0.25 (0.17–0.40) |
| First day of ICR service, hospital day | 3 (2–4) | 4 (2–7) | 2 (2–3) | 2 (2–4) |
| Proportional timing of ICRc | 0.60 (0.33–0.83) | 0.50 (0.28–0.71) | 0.75 (0.50–1.00) | 0.50 (0.33–0.75) |
| Components of ICR | ||||
| Evaluation | 75 503 (27.1) | 24 400 (26.9) | 25 552 (25.9) | 25 551 (28.7) |
| Education | 57 949 (20.8) | 16 001 (17.6) | 22 027 (22.3) | 19 921 (22.3) |
| Exercise | 172 147 (61.8) | 65 698 (72.3) | 62 997 (63.8) | 43 452 (48.7) |
| Other | 53 451 (19.2) | 16 255 (17.9) | 16 360 (16.6) | 20 836 (23.4) |
| PT utilization among all patients | 462 553 (34.4) | 123 816 (59.0) | 41 552 (11.2) | 297 185 (38.9) |
| Among patients with PT only | ||||
| PT dose, d | 2 (1–4) | 3 (2–5) | 2 (1–4) | 2 (1–3) |
| Components of PT | ||||
| Evaluation | 437 174 (94.5) | 116 325 (94.0) | 37 424 (90.1) | 283 425 (95.4) |
| Education | 3909 (0.9) | 1569 (1.3) | 290 (0.7) | 2050 (0.7) |
| Exercise | 351 492 (76.0) | 109 294 (88.3) | 28 597 (68.8) | 213 601 (71.9) |
| Other | 118 471 (25.6) | 311 54 (25.2) | 9839 (23.7) | 77 478 (26.1) |
| Both PT and ICR among all patients | 88 983 (6.6) | 43 176 (20.6) | 18 848 (8.3) | 34 857 (4.6) |
| Neither ICR nor PT among all patients | 691 239 (51.5) | 38 460 (18.3) | 241 005 (65.1) | 411 774 (54.0) |
Abbreviations: ICR, inpatient cardiac rehabilitation; IQR, interquartile range; PT, physical therapy, LOS, length of stay; PCI, percutaneous coronary intervention
Data reported as number (%) or median (IQR).
Calculated by dividing ICR dose by LOS. This represents the fraction of hospital days that included a visit from ICR. For example, if a patient was hospitalized for 3 d and was visited once by ICR on the day of discharge, this would be a proportion of 0.33, or 1/3 of the d covered.
Calculated by dividing first day of ICR by LOS. This represents the time point during the hospitalization that a patient was first evaluated by ICR. For example, if a patient with PCI was hospitalized for 4 d and the first day of ICR was day 3, this would a proportional timing of 0.75, having occurred about three-fourths of way through the hospitalization.
Among patients who received ICR, the median number (interquartile range [IQR]) of days with ICR services per admission was 1 (1–2), ranging from 3 (1– 4) sessions for surgical patients to 1 (1–2) sessions per PCI admission (Table 2). For surgical admissions, the initial evaluation by ICR typically occurred on hospital day 4, which was about half-way through the hospitalization. For all other admissions, ICR occurred during the latter half of the hospital stay. Exercise was the most common modality of treatment by ICR (61.8%); education and evaluation services accounted for 20.8% and 27.1% of services rendered, respectively. Although 87.7% of surgical patients were treated with either ICR and/or PT, most of all patients (51.5%) did not have a service code for either ICR or PT. Results for the full 8-stratum analysis are provided in SDC Table 3.
Of the 458 hospitals, 223 (49%) had at least 1 hospital admission with an ICR code, suggesting the availability of ICR at these hospitals. Several hospital characteristics were associated with the presence of an ICR program. Hospitals that were located in urban areas (52.3 vs 47.7%, P = .01) and those that offered cardiac surgery (67.1 vs. 32.9%, P < .001) or PCI services (63.3 vs. 36.7%, P < .001) were significantly more likely to offer ICR (Table 3). Hospitals located in the Midwest and particularly the west north central region of the Midwest (Missouri, Kansas, Iowa, Minnesota, Nebraska, and North and South Dakota) were most likely to provide ICR.
Table 3. Characteristics of Hospitals Treating Cardiac Patients With and Without ICR Programsa.
| All Hospitals n = 458 | Hospitals without ICR n = 235 | Hospitals with ICR n = 223 | P Valueb | |
|---|---|---|---|---|
| Urban | 342 (74.7) | 163 (47.7) | 179 (52.3) | .01 |
| Teaching | 118 (25.8) | 49 (41.5) | 69 (58.5) | .01 |
| Hospital size | <.001 | |||
| ≤200 beds | 184 (40.2) | 133 (72.3) | 51 (27.7) | |
| 201-400 beds | 166 (36.2) | 70 (42.2) | 96 (57.8) | |
| ≥401 beds | 108 (23.6) | 32 (29.6) | 76 (70.4) | |
| US regional divisions | <.001 | |||
| Midwest | ||||
| East north centrald | 62 (13.5) | 28 (45.2) | 34 (54.8) | |
| West north centrale | 38 (8.3) | 7 (18.4) | 31 (81.6) | |
| Northeast | ||||
| Middle Atlantic | 55 (12.0) | 34 (61.8) | 21 (38.2) | |
| New England | 13 (2.8) | 8 (61.5) | 5 (38.5) | |
| South | ||||
| East south centralf | 31 (6.8) | 16 (51.6) | 15 (48.4) | |
| South Atlantic | 123 (26.9) | 55 (44.7) | 68 (55.3) | |
| West south centralg | 45 (9.8) | 27 (60.0) | 18 (40.0) | |
| West | ||||
| Mountain | 17 (3.7) | 7 (41.2) | 10 (58.8) | |
| Pacific | 74 (16.2) | 53 (71.6) | 21 (28.4) | |
| Surgical services | 225 (49.1) | 74 (32.9) | 151 (67.1) | <.001 |
| PCI services | 297 (64.9) | 109 (36.7) | 188 (63.3) | <.001 |
| Proportion of patients receiving physical therapy | 36.7 ± 14.5 | 37.5 ± 15.7 | 36.0 ± 13.0 | .10c |
Abbreviations: ICR, inpatient cardiac rehabilitation; PCI, percutaneous coronary intervention, US, United States.
Data reported as n (%) or mean ± standard deviation
Calculated using Kruskal-Wallis test.
Calculated using Chi-square test.
Includes Illinois, Indiana, Michigan, Ohio, and Wisconsin
Includes Iowa, Kansas, Minnesota, Missouri, Nebraska, North Dakota, and South Dakota
Includes Alabama, Kentucky, Mississippi, and Tennessee
Includes Arkansas, Louisiana, Texas, Oklahoma
Results at Hospitals with ICR Programs
When the analysis was restricted to hospitals that provided ICR, 30.6% of patients received ICR and hospital median utilization was 18.8% [IQR 0.3%-51.9%]. Use of ICR varied substantially by indication, and was highest among surgical patients (median [IQR] = 86%, [45%-96%]) and lowest among patients with heart failure or medically managed MI (7%, [0.45–30%]). Use of ICR among patients who had undergone PCI showed the greatest variation between hospitals (mean = 48%, range = 4.0% to 83%) (Figure). The presence of a surgical program with high ICR utilization rates was strongly associated with use of ICR among other patient groups (SDC Figure 2).
Figure.
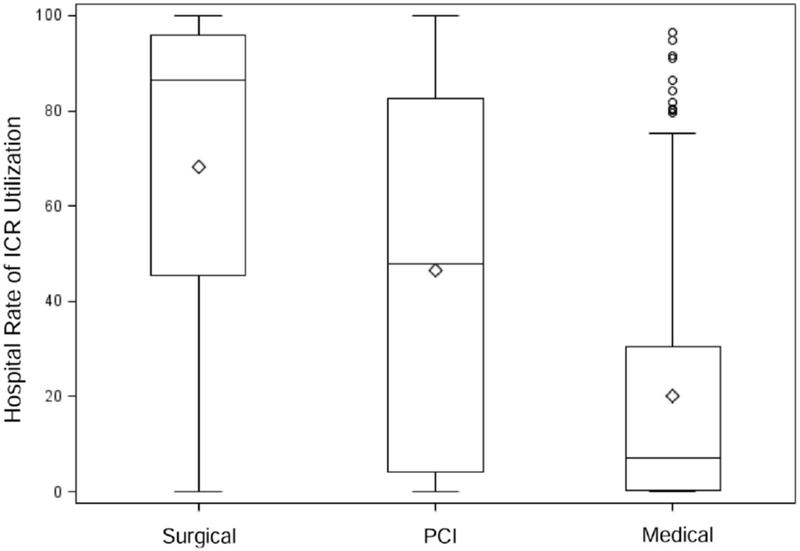
Variation in utilization rate ICR at hospitals with ICR services. The hospital utilization rate rangeg from 0% to 100% in nearly all patient groups, demonstrating the wide variations in care seen across US hospitals in delivery of ICR. The middle line in the boxes represents the median value, the upper and lower lines of the boxes are the interquartile ranges, and the whiskers represent the maximum and minimum observation within 1.5 times the interquartile range. The diamond inside the boxes is the mean value and the open circles are oulier value. Abbreviations: ICR, inpatient cardiac rehabilitation; PCI, percutaneous coronary intervention
Multivariable hierarchical modeling revealed several patient factors associated with lower likelihood of ICR utilization (Table 4). Among surgical patients, older age (OR = 0.88; 95% CI, I0.81-0.96) for 80+ y old vs 55–64 y old; “other” racial category (OR = 0.88; 95% CI, 0.81–0.94) vs whites; and female sex (OR = 0.91; 95% CI, 0.87–0.95). Medicare insurance and higher comorbidity burden were independently associated with lower odds of receiving ICR. Results were similar among patients with PCI procedures or medically managed MI or HF. Tobacco abuse was the only factor examined that was consistently associated with significantly greater ICR utilization (OR range across conditions was 1.07–1.14). In general, PT use was associated with lower ICR use (OR range across conditions was 0.51–0.98) (Table 4).
Table 4. Patient Characteristics Associated with Receipt of Inpatient Cardiac Rehabilitationa.
| Surgical | PCI | Medical | ||||
|---|---|---|---|---|---|---|
| OR (LL - UL) | P Value | OR (LL - UL) | P Value | OR (LL - UL) | P Value | |
| Patient subgroups | ||||||
| CABG | Referent | |||||
| CABG + HVS | 0.82 (0.77–0.87) | <.0001 | ||||
| HVS | 0.84 (0.79–0.89) | <.0001 | ||||
| Urgent PCI | Referent | |||||
| Elective PCI | 1.08 (1.04–1.12) | <.0001 | ||||
| MI + PCI | 1.60 (1.56–1.65) | <.0001 | ||||
| Heart failure | Referent | |||||
| Myocardial infarction | 2.1 (2.05–2.15) | <.0001 | ||||
| Age groups | ||||||
| <55 y | 0.96 (0.90–1.02) | .1847 | 1.02 (0.98–1.06) | .2712 | 0.98 (0.94–1.02) | .2645 |
| 55–64 y | Referent | Referent | Referent | |||
| 65–79 y | 1.00 (0.94–1.06) | .9703 | 1.06 (1.02–1.11) | .0029 | 1 (0.96–1.03) | .9106 |
| 80+ y | 0.88 (0.81–0.96) | .003 | 0.99 (0.94–1.04) | .6337 | 0.75 (0.72–0.78) | <.0001 |
| Female | 0.91 (0.87–0.95) | <.001 | 1.00 (0.97–1.02) | .7641 | 0.86 (0.84–0.88) | <.0001 |
| Race/Ethnicity | ||||||
| White | Referent | Referent | Referent | |||
| Black | 0.98 (0.90–1.07) | .7143 | 0.99 (0.94–1.04) | .6518 | 0.99 (0.96–1.02) | .5504 |
| Hispanic | 0.90 (0.79–1.02) | .0881 | 1.02 (0.94–1.11) | .5891 | 0.96 (0.9–1.01) | .1015 |
| Other | 0.88 (0.81–0.94) | .0006 | 0.94 (0.90–0.99) | .0148 | 0.82 (0.79–0.86) | <.0001 |
| Insurance payors | ||||||
| Medicare | Referent | Referent | Referent | |||
| Medicaid | 1.11 (1–1.23) | .0441 | 0.93 (0.87–1) | .0401 | 1.1 (1.05–1.15) | .0002 |
| Managed care/community indemnity | 1.15 (1.08–1.22) | <.001 | 1.1 (1.05–1.14) | <.0001 | 1.33 (1.28–1.38) | <.0001 |
| Self-pay/ Other | 1.08 (0.99–1.19) | .0843 | 1.08 (1.03–1.14) | .0039 | 1.24(1.18–1.3) | <.0001 |
| Gagne comorbidity score | ||||||
| Tertile 1 | Referent | Referent | Referent | |||
| Tertile 2 | 1.03 (0.97–1.09) | .3025 | 1.01 (0.98–1.05) | .378 | 0.77 (0.75–0.79) | <.0001 |
| Tertile 3 | 0.83 (0.77–0.89) | <.0001 | 0.86 (0.82–0.91) | <.0001 | 0.7 (0.67–0.72) | <.0001 |
| LOS tertiles | ||||||
| Tertile 1 | Referent | Referent | Referent | |||
| Tertile 2 | 1.71 (1.63–1.81) | <.001 | 1.6 (1.55–1.66) | <.0001 | 1.88 (1.83–1.93) | <.0001 |
| Tertile 3 | 1.31 (1.23- .39) | <.001 | 2.29 (2.19–2.38) | <.0001 | 2.31 (2.24–2.38) | <.0001 |
| Comorbidities | ||||||
| Congestive heart failure | 0.88 (0.83–0.93) | <.001 | 0.95 (0.91–0.99) | .0149 | ||
| Valvular disease | 0.95 (0.9–1) | .042 | 1.04 (0.99–1.08) | .1153 | 1.14 (1.12–1.17) | <.0001 |
| Pulmonary circulation disease | 0.89 (0.83–0.96) | .0035 | 1 (0.93–1.08) | .924 | 1.09 (1.06–1.12) | <.0001 |
| Peripheral vascular disease | 0.91 (0.86–0.96) | .0008 | 0.94 (0.9–0.98) | .0045 | 1.06 (1.03–1.09) | .0002 |
| Chronic lung disease | 0.99 (0.94–1.04) | .7595 | 0.94 (0.91–0.98) | .0015 | 0.93 (0.91–0.95) | <.0001 |
| Diabetes | 1.09 (1.04–1.13) | .0001 | 0.99 (0.96–1.02) | .5244 | 0.98 (0.96–1.00) | .0655 |
| Renal failure | 0.81 (0.76–0.87) | <.0001 | 0.9 (0.85–0.94) | <.0001 | 1.02 (0.99–1.06) | .1261 |
| Atrial fibrillation | 1.09 (1.04–1.15) | .0002 | 0.94 (0.9–0.98) | .0039 | 1.02 (0.99–1.04) | .1396 |
| Obstructive sleep apnea | 1.00 (0.93–1.07) | .9309 | 1.11 (1.05–1.17) | .0004 | 1.01 (0.98–1.05) | .514 |
| Tobacco abuse disorder | ||||||
| Nonsmoker | Referent | Referent | Referent | |||
| Former smoker | 1.07 (1.02–1.13) | .0114 | 1.06 (1.02–1.09) | .0039 | 1.11 (1.07–1.14) | <.0001 |
| Current smoker | 1.06 (1–1.12) | .0492 | 1.07 (1.04–1.11) | <.0001 | 1.21 (1.17–1.25) | <.0001 |
| Use of physical therapy | 0.51 (0.48–0.53) | <.0001 | 0.81 (0.70.85) | <.0001 | 0.98 (0.9–1.01) | .1726 |
| Model characteristics | ||||||
| Full model C-statistic | 0.92 | 0.90 | 0.90 | |||
| Intraclass correlation | ||||||
| Hospital effect, % | 83.2 | 79.7 | 69.7 | |||
| Including patient characteristics, % | 83.5 | 80.2 | 70.8 | |||
Abbreviations: CABG, coronary artery bypass graft surgery; HVS, heart valve surgery; MI, myocardial infarction; PCI, percutaneous coronary intervention; LOS, length of stay; OR, odds ratio; UL, upper limit; LL, lower limit.
Analysis used hierarchical general linear models adjusted for hospital characteristics.
Model discrimination was excellent with C-statistics for all patient strata ranging from 0.90 to 0.92. (Table 4). In models including a hospital random effect, there was substantial variation in ICR use associated with the hospital only, 83.2%, 79.7% and 69.7% for surgical, PCI and medical groups, respectively. Addition of patient characteristics to these models accounted for a nominal addition to the explained variation (Table 4).
DISCUSSION
Using a large, detailed, national database of more than 450 hospitals and 1.3 million admissions, we found that 21% of eligible patients received formal ICR before hospital discharge and that the percentage of patients receiving ICR gradually declined over time. Additionally, fewer than half of hospitals treating cardiac patients offered formal ICR, and, among the hospitals that offered ICR, fewer than one-third of patients received ICR services. We also found that only approximately 60% of hospitals that perform cardiac surgery offer formal ICR and, overall, fewer than 50% of CABG patients received ICR. Given the important role both inpatient and outpatient CR plays in recovery from an acute cardiac condition, our findings suggest there is a large opportunity to increase hospital-initiated, lifestyle-focused efforts in the secondary prevention of heart disease.
Including PT as an ICR surrogate improved rates of use particularly among the surgical population. However, even when considering both of these services together, both PT and ICR still did not reach even half of the potentially eligible population. Moreover, there are often substantial differences between the goals and purposes of ICR and PT, so it is unclear if PT can really be consider a full surrogate for ICR.
Although we found that older patients, females, those with more comorbidities, and non-Medicare insurance were less likely to receive ICR, these factors were dwarfed by the much larger role of the hospital in predicting use of ICR. This is not necessarily surprising because, unlike outpatient CR, hospitalized patients do not actively decide to participate in ICR and hospital protocols and policies likely play a stronger role than physician referral patterns. However, this pattern of ICR use strongly suggests that any initiatives seeking to improve either ICR or outpatient CR will be more successful if they focus on hospital-level interventions rather than on patient or physician interventions.
Although the exact reason for low ICR utilization is unknown, 2 key factors are probably at play. First, declining hospital length of stay23,24 over the past few decades has made some cardiac hospitalizations so brief (1–2 days in this PCI group) that it is now difficult to assure that every patient receives ICR. Second, because ICR has not been a billable service since the 1980s, hospitals have had no direct financial incentive to retain these prevention-focused programs. As a result, it is understandable that such programs might be inadequately staffed, poorly supported, never initiated, or have been discontinued after initial implementation. However, because ongoing healthcare reforms are increasingly using bundled payments and population risk management, we suspect that ICR will become more appealing to hospital executives as a mechanism to improve outpatient CR rates and thereby improve both financial and patient outcomes.4,25,26
Although ideal secondary prevention and referral to outpatient CR can be accomplished in the outpatient setting, there are several reasons why the inpatient setting is an optimal place and time to initiate CR. First, prior research has suggested that only 1 in 4 eligible hospitalized cardiac patients receives ideal care, composed of outpatient CR referral, smoking cessation advice, lifestyle counseling, and proper medications prior to discharge.27 As ICR should be providing at least 2 of these 4 services, a robust ICR program could help decrease this gap and potentially decrease mortality.13 Second, counseling hospitalized patients on lifestyle issues improves patient experience12 and substantially increases the chance that important lifestyle and behavior counseling will occur.15 Third, inpatient liaison-facilitated CR referral is an effective tool to increase outpatient CR participation rates.10 Fourth, making an appointment for CR prior to hospital discharge hastens enrollment into outpatient CR and improves CR participation.25 As the vast majority of patients are hospitalized prior to commencing outpatient CR, improving ICR utilization is likely to increase outpatient CR participation and improve secondary prevention care.
Notably, several features of ICR are similar to the findings of prior publications concerning the epidemiology and utilization of outpatient CR. First, our finding of overall low ICR utilization is consistent with data from the 1995–2005 era which show low national utilization of outpatient CR.5,7 Second, patients undergoing procedures were more likely to receive ICR and this is consistent with prior studies which demonstrated that patients with CABG or PCI were more likely to be referred to and attend outpatient CR than patients with MI.7,28,29 Third, we found the highest utilization of ICR in the Midwest (specifically the West-North-Central areas), consistent with prior publications where outpatient CR utilization was highest in Nebraska and other North-Central states.7, 30 Fourth, we found that active smoking was associated with increased ICR utilization, consistent with a prior publication showing that smokers are more likely to be referred for CR.31
Several study limitations deserve to be mentioned. First, it is possible our reported ICR utilization rate is artificially low because of incomplete ascertainment of ICR. However, given that ICR is usually provided by trained professionals in hospital service lines where productivity is monitored and reported, we believe that our database captures the vast majority of formal ICR delivered in these hospitals. Additionally, prior studies have reported very high correlations between treatment rate estimates produced using the Premier database and those obtained through chart review.32,33 Second, physicians, nurses, or other non-ICR staff members at hospitals without ICR programs may provide at least some ICR equivalent services to patients without such efforts being recorded in the database. Depending on how frequently this occurred, efforts at CR referral and secondary prevention of heart disease at hospitals without ICR programs might be substantially higher than suggested by our data. However, the size of the national CR referral gap8,29 and other known secondary prevention quality gaps27,34 suggests that current US hospital-based efforts in the secondary prevention of heart disease are suboptimal. Third, although national ICR guidelines recommend that each patient be ambulated, educated, and referred to outpatient CR,2 we cannot verify which of these 3 activities were performed as part of the database-recorded ICR visit. Consequently, this limits our ability to know if a patient was referred to outpatient CR, but this limitation seems unlikely to affect whether or not they actually had an ICR visit.
Conclusion
In summary, we found that most patients did not receive formal ICR during a hospitalization for a cardiac condition that would make them eligible for outpatient CR. We also found wide variations in care across diagnoses, procedures, and a host of additional patient and hospital level factors. These findings highlight the large opportunity hospitals and providers have to use ICR programs to optimize the care provided to their patients in the secondary prevention of heart disease.
Supplementary Material
SDC Figure 1. ICR utilization trends 2007–2011 at hospitals with ICR programs. Note the gradual decrease in overall rates during the study period, with a somewhat larger decline among surgical patients. Abbreviations: ICR, inpatient cardiac rehabilitation; PCI, percutaneous coronary intervention.
SDC Figure 2. Hospital rate of ICR stratified by the presence of a surgical program and by tertiles of ICR use by surgical programs. The presence of a surgical program with high ICR utilization was strongly associated with increased utilization of ICR by other patient groups. Abbreviations: ICR, inpatient cardiac rehabilitation; PCI, percutaneous coronary intervention.
Acknowledgements
This work was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health, award number KL2TR001063. Dr Lagu and Dr Lindenauer were supported by the National Heart, Lung and Blood Institute of the National Institutes of Health (NIH), under award numbers K01HL114745 and 1K24HL132008, respectively. Dr Ades was supported by the Vermont Center for Behavior and Health (NIH-NIGMS P20GM103644). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Footnotes
Conflict of interest: All authors declare no conflicts of interest.
All authors have read and approved the manuscript.
REFERENCES
- 1.Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart disease and stroke statistics-2017 update: a report from the American Heart Association. Circulation. 2017;135(10):e146–e603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.American Association of Cardiovascular and Pulmonary Rehabilitation. Guidelines for Cardiac Rehabilitation and Secondary Prevention Programs. 5th ed. Champaign, IL: Human Kinetics, 2013. [Google Scholar]
- 3.Ades PA. Cardiac rehabilitation and secondary prevention of coronary heart disease. N Engl J Med. 2001;345(12):892–902. [DOI] [PubMed] [Google Scholar]
- 4.Heran BS, Chen JM, Ebrahim S, et al. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev. 2011(7):CD001800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Receipt of outpatient cardiac rehabilitation among heart attack survivors--United States, 2005. MMWR. February 1 2008;57(4):89–94. [PubMed] [Google Scholar]
- 6.Receipt of cardiac rehabilitation services among heart attack survivors--19 states and the District of Columbia, 2001. MMWR. November 7 2003;52(44):1072–1075. [PubMed] [Google Scholar]
- 7.Suaya JA, Shepard DS, Normand SL, Ades PA, Prottas J, Stason WB. Use of cardiac rehabilitation by Medicare beneficiaries after myocardial infarction or coronary bypass surgery. Circulation. 2007;116(15):1653–1662. [DOI] [PubMed] [Google Scholar]
- 8.Aragam KG, Dai D, Neely ML, et al. Gaps in referral to cardiac rehabilitation of patients undergoing percutaneous coronary intervention in the United States. J Am Coll Cardiol. 2015;65(19):2079–2088. [DOI] [PubMed] [Google Scholar]
- 9.Grace SL, Leung YW, Reid R, et al. The role of systematic inpatient cardiac rehabilitation referral in increasing equitable access and utilization. J Cardiopulm Rehabil Prev. 2012;32(1):41–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Grace SL, Russell KL, Reid RD, et al. Effect of cardiac rehabilitation referral strategies on utilization rates: a prospective, controlled study. Arch Intern Med. 2011;171(3):235–241. [DOI] [PubMed] [Google Scholar]
- 11.Gurewich D, Prottas J, Bhalotra S, Suaya JA, Shepard DS. System-level factors and use of cardiac rehabilitation. J Cardiopulm Rehabil Prev. 2008;28(6):380–385. [DOI] [PubMed] [Google Scholar]
- 12.Jackson EA, Krishnan S, Meccone N, Ockene IS, Rubenfire M. Perceived quality of care and lifestyle counseling among patients with heart disease. Clin Cardiol. 2010;33(12):765–769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Auer R, Gaume J, Rodondi N, Cornuz J, Ghali WA. Efficacy of in-hospital multidimensional interventions of secondary prevention after acute coronary syndrome: a systematic review and meta-analysis. Circulation. 2008;117(24):3109–3117. [DOI] [PubMed] [Google Scholar]
- 14.Pack QR, Squires RW, Lopez-Jimenez F, et al. Participation rates, process monitoring, and quality improvement among cardiac rehabilitation programs in the United States: a national survey. J Cardiopulm Rehabil Prev. 2015;35(3):173–180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Spencer FA, Salami B, Yarzebski J, Lessard D, Gore JM, Goldberg RJ. Temporal trends and associated factors of inpatient cardiac rehabilitation in patients with acute myocardial infarction: a community-wide perspective. J Cardiopulm Rehabil. 2001;21(6):377–384. [DOI] [PubMed] [Google Scholar]
- 16.Lindenauer PK, Pekow P, Gao S, Crawford AS, Gutierrez B, Benjamin EM. Quality of care for patients hospitalized for acute exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 2006;144(12):894–903. [DOI] [PubMed] [Google Scholar]
- 17.Decision Memo for Cardiac Rehabilitation Programs (CAG-00089R). Baltimore, MD: Centers for Medicare and Medicaid Services; 2006. [Google Scholar]
- 18.Centers for Medicare and Medicaid Services. Proposed Decision Memo for Cardiac Rehabilitation (CR) Programs - Chronic Heart Failure (CAG-00437N). 2013
- 19.Thirapatarapong W, Thomas RJ, Pack Q, Sharma S, Squires RW. Commercial insurance coverage for outpatient cardiac rehabilitation in patients with heart failure in the United States. J Cardiopulm Rehabil Prev. 2014;34(6):386–389. [DOI] [PubMed] [Google Scholar]
- 20.Gagne JJ, Glynn RJ, Avorn J, Levin R, Schneeweiss S. A combined comorbidity score predicted mortality in elderly patients better than existing scores. J Clin Epidemiol. 2011;64(7):749–759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8–27. [DOI] [PubMed] [Google Scholar]
- 22.Larsen K, Petersen JH, Budtz-Jorgensen E, Endahl L. Interpreting parameters in the logistic regression model with random effects. Biometrics. 2000;56(3):909–914. [DOI] [PubMed] [Google Scholar]
- 23.Berger AK, Duval S, Jacobs DR Jr, et al. Relation of length of hospital stay in acute myocardial infarction to postdischarge mortality. Am J Cardiol. 2008;101(4):428–434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Chin CT, Weintraub WS, Dai D, et al. Trends and predictors of length of stay after primary percutaneous coronary intervention: a report from the CathPCI registry. Am Heart J. 2011;162(6):1052–1061. [DOI] [PubMed] [Google Scholar]
- 25.Dunlay SMZVN; Pack QR; Thomas RJ; Roger V Attendance at cardiac rehabilitation is associated with decreased re-hospitalization following an acute myocardial infarction. Circ Cardiovasc Qual Outcomes 2013(6):A70 [Google Scholar]
- 26.Wong WP, Feng J, Pwee KH, Lim J. A systematic review of economic evaluations of cardiac rehabilitation. BMC Health Serv Res 2012;12:243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Redfern J, Hyun K, Chew DP, et al. Prescription of secondary prevention medications, lifestyle advice, and referral to rehabilitation among acute coronary syndrome inpatients: results from a large prospective audit in Australia and New Zealand. Heart. 2014;100(16):1281–1288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Thomas RJ, Miller NH, Lamendola C, et al. National survey on gender differences in cardiac rehabilitation programs. Patient characteristics and enrollment patterns. J Cardiopulm Rehabil. 1996;16(6):402–412. [DOI] [PubMed] [Google Scholar]
- 29.Brown TM, Hernandez AF, Bittner V, et al. Predictors of cardiac rehabilitation referral in coronary artery disease patients: findings from the American Heart Association’s Get With The Guidelines Program. J Am Coll Cardiol. 2009;54(6):515–521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Curnier DY, Savage PD, Ades PA. Geographic distribution of cardiac rehabilitation programs in the United States. J Cardiopulm Rehabil. 2005;25(2):80–84. [DOI] [PubMed] [Google Scholar]
- 31.Gaalema DE, Cutler AY, Higgins ST, Ades PA. Smoking and cardiac rehabilitation participation: associations with referral, attendance and adherence. Prev Med. 2015;80:67–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Rothberg MB, Lahti M, Pekow PS, Lindenauer PK. Venous thromboembolism prophylaxis among medical patients at US hospitals. J Gen Intern Med. 2010;25(6):489–494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Jennings LA, Auerbach AD, Maselli J, Pekow PS, Lindenauer PK, Lee SJ. Missed opportunities for osteoporosis treatment in patients hospitalized for hip fracture. J Am Geriatr Soc. 2010;58(4):650–657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Tang L, Patao C, Chuang J, Wong ND. Cardiovascular risk factor control and adherence to recommended lifestyle and medical therapies in persons with coronary heart disease (from the National Health and Nutrition Examination Survey 2007–2010). Am J Cardiol. 2013;112(8):1126–1132. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
SDC Figure 1. ICR utilization trends 2007–2011 at hospitals with ICR programs. Note the gradual decrease in overall rates during the study period, with a somewhat larger decline among surgical patients. Abbreviations: ICR, inpatient cardiac rehabilitation; PCI, percutaneous coronary intervention.
SDC Figure 2. Hospital rate of ICR stratified by the presence of a surgical program and by tertiles of ICR use by surgical programs. The presence of a surgical program with high ICR utilization was strongly associated with increased utilization of ICR by other patient groups. Abbreviations: ICR, inpatient cardiac rehabilitation; PCI, percutaneous coronary intervention.