

Abstract
Rationale:
According to previously published studies, treating pediatric patients with congenital pseudarthrosis of the tibia (CPT) is challenging. More effective methods are needed to treat this patient population.
Patient concerns:
A 7-year-old girl with congenital pseudarthrosis of the distal tibia, previously misdiagnosed as a fracture, underwent plate fixation. Unfortunately, the steel plate broke after 3 months, which led to ankle angle deformity.
Diagnoses:
Congenital pseudarthrosis of the tibia.
Intervention:
Treat the congenital pseudarthrosis of the tibia with Ilizarov technology.
Outcomes:
lower limb force recovery, bone union, and lower-limb-length equalization were achieved. Congenital pseudarthrosis of the tibia were cured.
Lessons:
The Ilizarov technique is a safe, effective, and practical treatment option for patients with CPT.
Keywords: congenital pseudarthrosis, Ilizarov, tibia
1. Introduction
Congenital pseudarthrosis of the tibia (CPT) is difficult to treat in pediatric patients.[1] Some patients finally undergo amputation because of improper treatment and repeated fractures.[2,3] The etiopathogenesis of the disease is unknown. In 50% of cases,[4] it is associated with neurofibromatosis. Most patients have anterolateral angulation of the bone from childhood, and spontaneous fracture occurs during growth. Despite the many treatment options, surgery remains the most effective treatment method in cases of CPT. Surgical methods include Ilizarov bone transport, intramedullary stabilization, and bone grafting. Vascularized fibular transplant and the Masquelet technique have advantages.[5] The current treatment advocates a combination of 2 or 3 types of surgeries. However, Ilizarov ring fixation has been shown to be the most effective treatment option. Every surgery should include complete removal of the lesion, correcting the deformity, promoting bone healing, and limb extension. Patients with united fracture sites often have residual deformities of the tibia and ankle, as well as shortening. Many of these patients develop progression of the deformity leading to degenerative arthritis of the ankle and knee joints. Unfortunately, surgery cannot change the natural history and pathology of the disease.[1] We believe that choosing the most appropriate surgical method can minimize patient suffering. As such, we recommend that the patient should undergo Ilizarov ring fixation.
2. Case description
The patient provided informed consent for the publication of his clinical and radiologic data. This case report was approved by Medical Ethical Committee of The First Affiliated Hospital of Nanchang University.
2.1. Preoperative conditions
A 7-year-old girl presented to our hospital with a congenital pseudarthrosis in the distal 3rd of the right tibia (Fig. 1 A, B). The patient had a history of trauma and, unfortunately, underwent plate fixation at a local hospital. After 3 months, the patient developed pain when walking and skin swelling. X-ray examination revealed broken internal fixation and tibia angular deformity (Fig. 2 A–C). Upon admission to our center, a typical presentation of CPT was confirmed during the medical examination. Fortunately, the patient did not have congenital neurofibromatosis.
Figure 1.
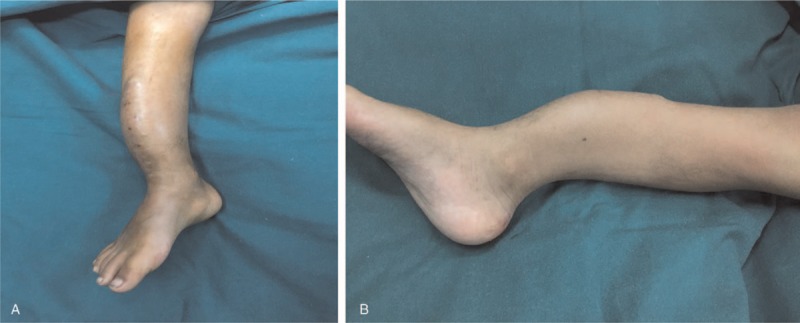
(A, B) Clinical presentation at the admission in our center.
Figure 2.

(A–C) Internal fixation broken and tibia angular deformity.
2.2. Intraoperative treatment
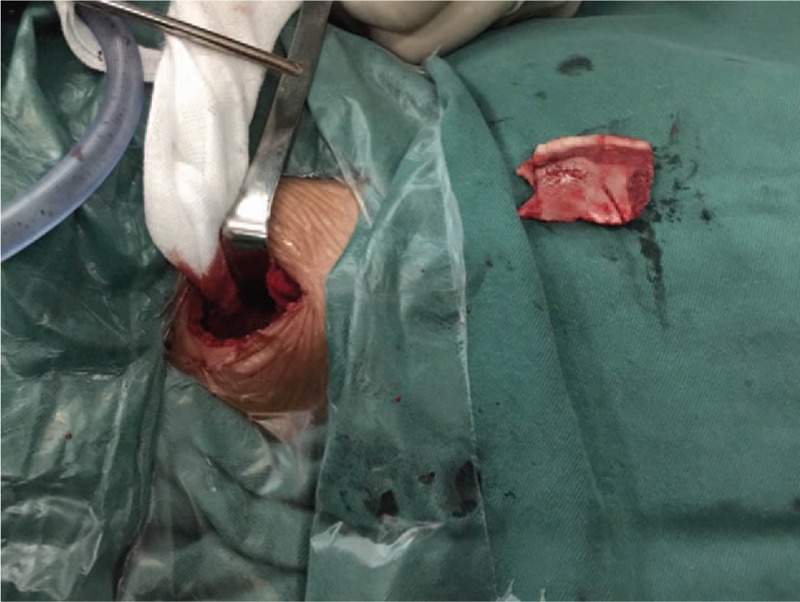
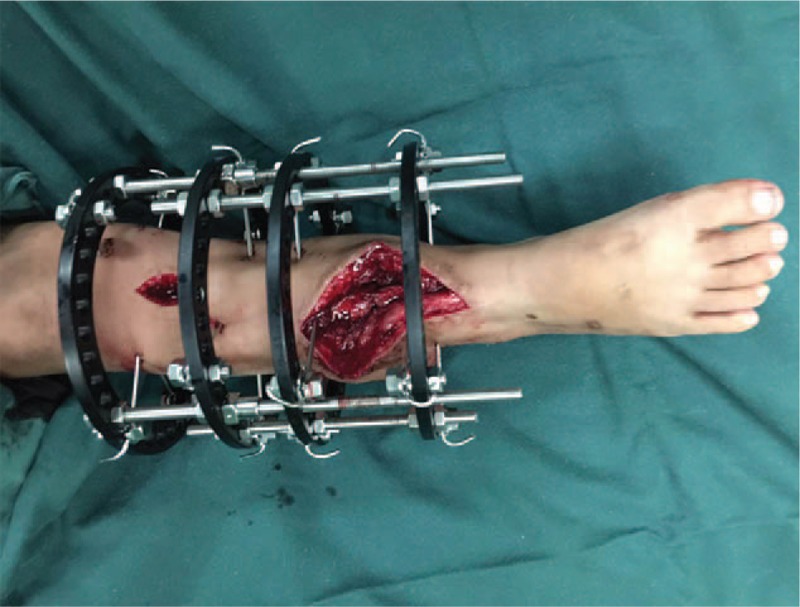
As part of the surgery, the original surgical incision was re-opened, the steel plate removed, and pseudarthrosis was exposed (Fig. 3). We performed oblique osteotomy approximately 3 cm in length on the proximal and distal ends of the fracture and radical resection of sclerotic tibial segments (Fig. 4). A longitudinal incision on the outside of the right lower leg was made, exposing the fibula. After truncation, a 3-cm-long fibula section was taken (Fig. 5). It was inserted into the medullary cavity of the tibia, after removing the soft tissue and periosteum from the surface of the fibula (Fig. 6). The assembled circular external fixator was placed at the center of the lower leg. After adjusting the position, the Kirschner wire was placed on both sides of the tibial fracture and tightened for compression fixation. The proximal tibia was exposed. The proximal end of the tibia was then cut off with a swing saw, bone knife, and electric drill. The extension ring of the external fixator was installed. Its position was confirmed by the C-arm machine. Take the right anterior superior iliac spine, cut the skin and fascia to reveal the ilium after cutting open the cortical bone, and excavate the cancellous bone (Fig. 7). The extracted cancellous bone was cut into strips (Fig. 8) and paved on both sides of the fractured end of the lower tibia and compacted (Fig. 9). The wound in the ilium was rinsed and the incision closed.
Figure 3.

The steel plate was removed and pseudarthrosis was exposed.
Figure 4.

Resection of the lesion of the congenital pseudarthrosis of the tibia.
Figure 5.

Fibula section was taken.
Figure 6.

Inserted the fibula into the medullary cavity of the tibia.
Figure 7.
Take out the medial side of the ilium.
Figure 8.

Extracted cancellous bone was cut into strips.
Figure 9.
The extracted cancellous bone was paved on both sides of the fractured end of the lower tibia.
2.3. Postoperative treatment
In the postoperative examination, we found that the deformity of the lower limbs was corrected and the line of force was restored (Fig. 10). Patient with external fixation began extending her affected extremity after 1 week, and continued pressure was applied to maintain the stability of the stub and force line. The bones were extended by 1 mm per day. The rod was screwed 4 times a day and 90° each time for the 1/4 turn. The knee and ankle were moved simultaneously to acquire strength. The patient was seen monthly for the 1st follow-up year. X-rays were obtained to determine bone quality. After 9 months, we removed the external fixator (Fig. 11 A, B). Three months after its removal, the patient started to practice partial weight-bearing exercises because the new bone was fragile, avoided strenuous exercise for the near joints, and gradually transitioned to full weight-bearing walking. One year postoperatively, we found that the lower limb force line was normal, and lower limb shortening eliminated. The knee joint was not stiff, but ankle dorsiflexion was mildly limited. We believe this is related to the formation of mild forward angled deformities in the lower tibia. The patient can perform full weight-bearing walking without pain (Fig. 12). However, the most important issue that we care about is whether a refracture will occur.
Figure 10.

X-rays after the operation and application of Ilizarov ring fixation.
Figure 11.

(A, B) After removing the Ilizarov ring fixation.
Figure 12.

The patient can have full weight bearing and be free of pain.
3. Discussion
The CPT remains challenging for orthopedic physicians because it is difficult to obtain and maintain a solid union.[6,7] In this present study, the healing rate with follow-up until many years after reaching skeletal maturity was 60%. In a multicenter study, Ohnishi et al observed that the most acceptable method for treating patients with CPT was with Ilizarov technology and vascularized fibular graft.[8] However, those methods do not always guarantee a solid union. Authors have stressed the importance of fixing the fibula and think that the nonunion of the fibula favors valgus deformities.[9,10] However, we have taken different surgical methods. In our patients, we truncate the fibula and transplant it to the tibia. The upper and lower ends of the fibula are not fixed, and the fibula is nonunited. However, there is no valgus deformity at the lower end of the tibia.
Surgical treatment seeks to achieve bone union of the pseudarthrosis while restoring alignment in the leg to prevent the risk of recurrent fracture and preserve function and bone growth in the leg.[11] Based on to our experience, using the Ilizarov technique is very beneficial when other surgeries fail, or refracture occurs. In addition, all other conventional treatments are still possible if this technique fails. Cortical bone grafts have been used as anabolic stimuli to promote repair. Therefore, we use the fibula for bone transplantation and the bone repairs quickly. Generally, the adjoining joints are stiff because of prolonged immobilization, but this patient's knee and ankle joints were not. This might be related to the child's activities.
It is presented as CPT usually associated with characteristic anterolateral bowing.[9,12] It is often misdiagnosed, because the initial symptoms are very similar to those of fractures. In this case, the patient was initially fixed with a plate because of the apparent history of trauma which led to a misdiagnosis. Managing CPT using steel plates is taboo in this patient population. It must be corrected with a second operation compared with traditional surgery (through osteotomy surgery to correct the lower limb angulation). After the osteotomy is healed, the lower limbs are lengthened to correct the inequality. We believe that it is possible to address lower extremity angulation and shortened deformity simultaneously during 1 operation. It can shorten hospitalization time and reduce hospitalization cost.
Although the cure rate for CPT is gradually increasing, other concerns, such as leg-length discrepancy, refracture, axial deformity, progressive malalignment, and ankle valgus, usually influence the final outcome.[13–15] One of the main issues is refracture. Any stress on weight-bearing will pass through the weakest point in the link. The united bone is often of inferior biologic and mechanical quality, such as a small docking site, tibial valgus or rotation deformity, and sclerotic bone with no medullary cavity, therefore a protective brace is recommended.[16,17]
4. Conclusion
The Ilizarov technique is a safe, effective, and practical treatment option for patients with CPT. Compared with other treatment options, it can achieve several goals such as ankle stabilization, osteosynthesis, and leg-length equalization. Patients’ condition is also stable postoperatively. If the patient has mastered how to adjust the tractor, he or she can go home with external fixation. This can shorten hospitalization time and reduce hospitalization cost. However, the impact of surgery also requires continuous follow-up. We hope that future research will uncover the etiopathogenesis of CPT and that a new technique can be developed.
Acknowledgment
The authors thank the patient for agreeing to use her image and clinical data.
Author contributions
Conceptualization: Ling Dong Kong.
Formal analysis: Han Xiong Cheng.
Project administration: Tao Nie.
Writing – original draft: Ling Dong Kong.
Footnotes
Abbreviation: CPT = congenital pseudarthrosis of the tibia.
This research was supported by the Science and Technology Foundation of Jiangxi Province (20161BBG70174).
The authors have no conflicts of interest to disclose.
References
- [1].Ghanem I, Damsin JP, Carlioz H. Ilizarov technique in the treatment of congenital pseudarthrosis of the tibia. J Pediatr Orthop 1997;17:685–90. [DOI] [PubMed] [Google Scholar]
- [2].Joseph B, Mathew G. Management of congenital pseudarthrosis of the tibia by excision of the pseudarthrosis, onlay grafting, and intramedullary nailing. J Pediatr Orthop B 2000;9:16–23. [DOI] [PubMed] [Google Scholar]
- [3].Su YP, Wang MN, Chang WN. Successful treatment of congenital pseudarthrosis of the tibia with long segment fibular allografting in a young child. J Formos Med Assoc 2007;106:S44–9. [DOI] [PubMed] [Google Scholar]
- [4].Oetgen ME, Richards BS. Complications associated with the use of bone morphogenetic protein in pediatric patients. J Pediatr Orthop 2010;30:192–8. [DOI] [PubMed] [Google Scholar]
- [5].Vanderstappen J, Lammens J, Berger P, et al. Ilizarov bone transport as a treatment of congenital pseudarthrosis of the tibia: a long-term follow-up study. J Child Orthop 2015;9:319–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Ippolito E, Corsi A, Grill F, et al. Pathology of bone lesions associated with congenital pseudarthrosis of the leg. J Pediatr Orthop B 2000;9:3–10. [DOI] [PubMed] [Google Scholar]
- [7].Kristiansen LP, Steen H, Terjesen T. Residual challenges after healing of congenital pseudarthrosis in the tibia. Clin Orthop Relat Res 2003;414:228–37. [DOI] [PubMed] [Google Scholar]
- [8].Ohnishi I, Sato W, Matsuyama J, et al. Treatment of congenital pseudarthrosis of the tibia—a multicenter study in Japan. J Pediatr Orthop 2005;25:219–24. [DOI] [PubMed] [Google Scholar]
- [9].Shah H, Rousset M, Canavese F. Congenital pseudarthrosis of the tibia: management and complications. Indian J Orthop 2012;46:616–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Mathieu L, Vialle R, Thevenin-Lemoine C, et al. Association of Ili-zarov's technique and intramedullary rodding in the treatment of congenital pseudarthrosis of the tibia. J Child Orthop 2008;2:449–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Joseph B, Somaraju VV, Shetty SK. Management of congenital pseudarthrosis of the tibia in children under 3 years of age: effect of early surgery on union of the pseudarthrosis and growth of the limb. J Pediatr Orthop 2003;23:740–6. [DOI] [PubMed] [Google Scholar]
- [12].Bhowmick KVD. Varghese retrograde intramedullary nailing for recurrent fracture in congenital pseudarthrosis of the tibia. J Foot Ankle Surg 2016;55:1287–91. [DOI] [PubMed] [Google Scholar]
- [13].Choi IH, Cho TJ, Moon HJ. Ilizarov treatment of congenital pseudarthrosis of the tibia: a multi-targeted approach using the Ilizarov technique. Clin Orthop Surg 2011;3:1–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [14].Pannier S. Congenital pseudarthrosis of the tibia. Orthop Traumatol Surg Res 1978;97:750–61. [DOI] [PubMed] [Google Scholar]
- [15].Tudisco C, Bollini G, Dungl P, et al. Functional results at the end of skeletal growth in 30 patients affected by congenital pseudarthrosis of the tibia. J Pediatr Orthop B 2000;9:94–102. [DOI] [PubMed] [Google Scholar]
- [16].Cho TJ, Choi IH, Lee SM, et al. Refracture after Ilizarov osteosynthesis in atrophic-type congenital pseudarthrosis of the tibia. J Bone Joint Surg Br 2008;90:488–93. [DOI] [PubMed] [Google Scholar]
- [17].Romanus B, Bollini G, Dungl P, et al. Free vascular fibular transfer in congenital pseudoarthrosis of the tibia: results of the EPOS multicenter study. J Pediatr Orthop 2000;9:90–3. [DOI] [PubMed] [Google Scholar]