

Abstract
Aging brings about challenges in the ability to recover balance through protective stepping, especially in the lateral direction. Previous work has suggested that lateral protective stepping during weight transfer may be affected by impaired muscle composition and performance of the hip abductors (AB) in older adults. Hence, this study investigated the influence of hip abductor-adductor (AB-AD) neuromuscular performance on the weight transfer phase of lateral protective stepping in younger and older adults. Healthy younger (n=15) and older adults (n=15) performed hip AB-AD isometric maximal voluntary contractions (IMVC). Lateral balance perturbations were applied via motorized waist-pulls. Participants were instructed to recover their balance using a single lateral step. Kinetic, kinematic and electromyographic (EMG) data were analyzed during the weight transfer phase. In the hip IMVC task, older adults showed reduced peak AB-AD torque, AB rate of torque development and AB-AD rate of EMG neuromuscular activation (RActv). During the lateral balance perturbations, older individuals had a lower incidence of lateral steps, reduced hip AB-AD RActv and delayed weight transfer. However, several outcomes were larger in the older group, such as, center of mass momentum at step onset, step-side peak rate of vertical force development, hip AB net joint torque, and power. Although older adults had greater hip muscular output during the weight transfer phase, their lateral balance recovery was still impaired. The reduced maximal hip AB-AD capacity, especially RActv, may have been a greater contributor to this impairment, as it affects the ability to generate rapid force, crucial for balance recovery.
Keywords: Aging, Lateral Balance, Hip abductors, Neuromuscular performance
1. Introduction
Falls among older adults may be considered a global epidemic. Approximately one third of individuals over 65 years of age fall every year (Hausdorff et al., 2001; WHO, 2012). When balance is perturbed, protective stepping is a common strategy used to re-establish the base of support (BoS), in order to stabilize balance and prevent falling (Barrett et al., 2012; Maki & McIlroy, 2006; Mille et al., 2013a; Pai et al., 2014; Sturnieks et al., 2013). However, this ability declines with increasing age. For example, when stationary balance is perturbed, older adults tend to use a greater number of protective steps to recover balance compared to younger individuals, which has been shown to be a potent predictor of future falls (Hilliard et al., 2008; Luchies et al., 1994; Maki et al., 1994; Mille et al., 2013b; Mille et al., 2005; Rogers & Mille, 2003).
Although loss of balance and falls can occur in all directions, postural instability with aging is especially problematic in the medio-lateral (M-L) plane (Mille et al., 2013a; Rogers & Mille, 2003). Loss of lateral balance involves unique biomechanical demands that affect the characteristics of M-L protective stepping. For example, when an external lateral balance perturbation moves the CoM relative to the BoS, the leg contralateral to the perturbation direction initially undergoes passive unloading while the ipsilateral limb undergoes passive loading. Older adults frequently use strategies involving the passively unloaded limb, such as crossover stepping (front or back) or a medial-lateral stepping sequence (Maki et al., 2000; Maki et al., 1996; Mille et al., 2005). Unloaded-limb stepping strategies allow for faster step initiation, but there are several disadvantages, such as an increased use of multiple steps, increased single-limb support time, longer and more complex foot trajectories, increased incidence of limb collisions, and reduced BoS at first-step foot landing (Bair et al., 2016; Maki et al., 2000; Mille et al., 2013a).
In contrast to older adults, younger individuals more often recover balance with a single lateral step performed by the passively loaded limb in the direction of the balance perturbation. This is normally achieved by rapidly moving the center of mass towards the passively unloaded limb during the pre-step weight transfer phase, allowing the passively loaded limb to step. This results in an increased BoS upon landing and more effective control of the CoM lateral momentum (Bair et al., 2016; Maki et al., 2000). Although this strategy may be more biomechanically stabilizing than unloaded limb stepping strategies, lateral stepping requires considerable effort to unload the passively loaded limb compared to the cross-over and medial-lateral stepping sequence strategies (Mille et al., 2005; Patton et al., 2006).
While the factors determining selection of single lateral recovery steps during M-L balance recovery by older adults are unclear, impaired hip abductor-adductor (AB-AD) muscle torque, which is important for M-L balance control and pre-stepping lateral weight shift, is often present (Addison et al., 2014; Hilliard et al., 2008; Hurt & Grabiner, 2015; Inoue et al., 2017; Robinovitch et al., 2013). With aging, the gluteal muscles of the hip are especially susceptible to adipose infiltration, reduced muscle fiber quality, and compromised hip abductor (AB) strength which limits M-L protective stepping and gait performance (Addison et al., 2016; Addison et al., 2014; Hilliard et al., 2008; Inacio et al., 2014). In addition, age-associated neuromuscular activation impairments may contribute to deficits in hip torque and power which are important during pre-step lateral weight shifting and balance recovery (Aagaard et al., 2002; Aagaard et al., 2010; Addison et al., 2016; Fujimoto et al., 2017; Kanda et al., 1996; Kido et al., 2004; Rogers & Mille, 2003). In particular, the rate of neuromuscular activation, which contributes significantly to rapid muscle force production needed for effective balance control and protective stepping, diminishes with aging (Clark et al., 2011; Clark et al., 2013; Reid et al., 2012; Yoshida et al., 2012).
Due to the predominant use by older adults of more problematic crossover and medial-lateral stepping strategies which can lead to lateral imbalance and are associated with greater fall risk, there is a need to better understand the factors that restrict the use of more stabilizing lateral protective steps. Accordingly, the purposes of this study were to compare between community living older and younger adults, the neuromuscular and biomechanical performance of the hip AB-AD musculature during: 1) isolated rapid isometric maximum voluntary contractions (IMVC); and during 2) the pre-step weight transfer phase of induced lateral stepping at different initial weight bearing distributions. Different initial stepping limb weight bearing loads were used to represent a range of challenges to weight shifting ability. Compared with younger adults, we hypothesized that older adults would demonstrate impairments in isolated neuromechanical performance with less effective lateral weight shifting and stepping performance, and that deficits in stepping would be associated with age-related limitations in maximum hip AB-AD neuromechanical performance.
2. Methods
2.1. Participants
Fifteen younger adults (29.1±1.1yrs, n=8 females) and fifteen generally healthy community dwelling older individuals (71.3±0.9yrs, n=6 females) were recruited from the Baltimore/Washington metropolitan areas (Table 1). Exclusion criteria consisted of the following: 1) cognitive impairment (Folstein Mini Mental Score Exam < 24); 2) sedative use; 3) non-ambulatory; 4) any clinically significant functional impairment related to musculoskeletal, neurological, cardiopulmonary, metabolic, or other general medical problem; 6) Centers for Epidemiological Studies Depression Survey score greater than 16; 7) BMI over 35.
Table 1.
Participant demographics.
| Younger Adults (n=15) |
Older Adults (n=15) |
|
|---|---|---|
| Age (years) | 29.1±1.1 | 71.3±0.9 |
| Height (m) | 1.74±0.03 | 1.70±0.02 |
| Weight (kg) | 70.0±3.6 | 80.4±4.1 |
| BMI | 23.0±0.7 | 27.7±1.1 * |
| Induced Stepping Task Pulling Magnitude |
4.7±0.2 | 4.8±0.1 |
Data presented as Mean ± SEM.
significantly different from younger adults.
All subjects provided written informed consent. Experimental procedures were approved by the Institutional Review Board of University of Maryland, Baltimore and the Baltimore Veterans Administration Health Care System Office of Research Compliance.
2.2. Data collection
The IMVC protocol, performed on a BIODEX System 4 dynamometer (BIODEX, Shirley, NY), consisted of isometric bilateral hip AB-AD IMVCs. Participants were instructed to push as hard and fast as possible for 5 seconds, with 90s of rest between sets. Testing was performed at 30˚ of hip AB while standing in a custom stabilization frame to facilitate control of upright alignment (Johnson et al., 2004).
The induced lateral stepping protocol consisted of an initial “balance tolerance limit” (BTL) assessment (Bair et al., 2016; Yungher et al., 2012) and an induced stepping task at different initial pre-loaded weight distribution conditions. A position-controlled motorized waist-pull system was used to apply lateral balance perturbations via a pulley-cable configuration attached to rigid connections on each side of a waist-belt as described in previous studies (Pidcoe & Rogers, 1998). Participants wore a safety harness.
For the BTL assessment, subjects were instructed to react naturally and prevent themselves from falling. The BTL assessment consisted of forty waist-pulls (5 trials × 2 directions × 4 magnitudes (Appendix) randomized by direction (R or L) and magnitude. BTL was identified as the puller magnitude level where the average number of response steps, for any self-selected type of first step, exceeded 1.0 steps (Bair et al., 2016; Yungher et al., 2012).
For the induced stepping task using different initial stepping limb pre-loading conditions, participants received 30 randomly applied lateral waist-pulls in the direction of the pre-loaded limb (5 trials × 2 directions × 3 pre-loaded conditions), plus 12 catch trials (2 trials × 2 directions × 3 pre-loaded conditions) delivered to the opposite side to minimize anticipation and postural adaptation.
In order to present a range of challenges to weight transfer performance, as might be encountered during everyday activities, prior to the perturbations, participants were instructed to laterally shift their weight to distribute 50%, 65%, or 80% of their body weight onto the pre-determined stepping limb using real-time visual feedback of the vertical ground reaction forces provided by a monitor. Subjects were further instructed to respond to the waist-pull and “recover your balance with a single lateral step.” The lateral waist-pulls were triggered by computer control once the target weight distribution was maintained for more than 50ms. Perturbations were applied at one pulling-magnitude level above the previously determined BTL to ensure a stepping response on all trials.
Kinetic data were recorded by two AMTI force platforms (AMTI, Watertown, MA) at a collection frequency of 600Hz. Full body kinematic data were obtained via a motion capture system at 120Hz (VICON, Los Angeles, CA). Reflective markers were placed bilaterally on the foot (first metatarsal, hallux, fifth metatarsal and calcaneus), ankle (lateral and medial malleoli), knee (lateral and medial femoral condyles), hip (greater trochanter of the femur, PSIS and ASIS), shoulders (acromions) and head (midpoint and center of parietal bones and most lateral point of temporal bones) creating a seven-segment skeletal model (bilateral foot, shank, thigh and HAT (head+arms+trunk)).
Surface electromyographic (EMG) (NORAXON, Scottsdale, AZ) recordings of muscle activation patterns were collected during the hip AB-AD IMVC and the induced lateral stepping task at a frequency of 1500Hz. The EMG electrodes were placed in accordance with established guidelines over the gluteus medius (Gmed), tensor fasciae latae (TFL), and adductor magnus (ADD) (De Luca, 1997; Hermens et al., 2000) (Figure 1). Kinetic, kinematic and EMG data collection was synchronized by an external computer-controlled trigger.
Figure 1.
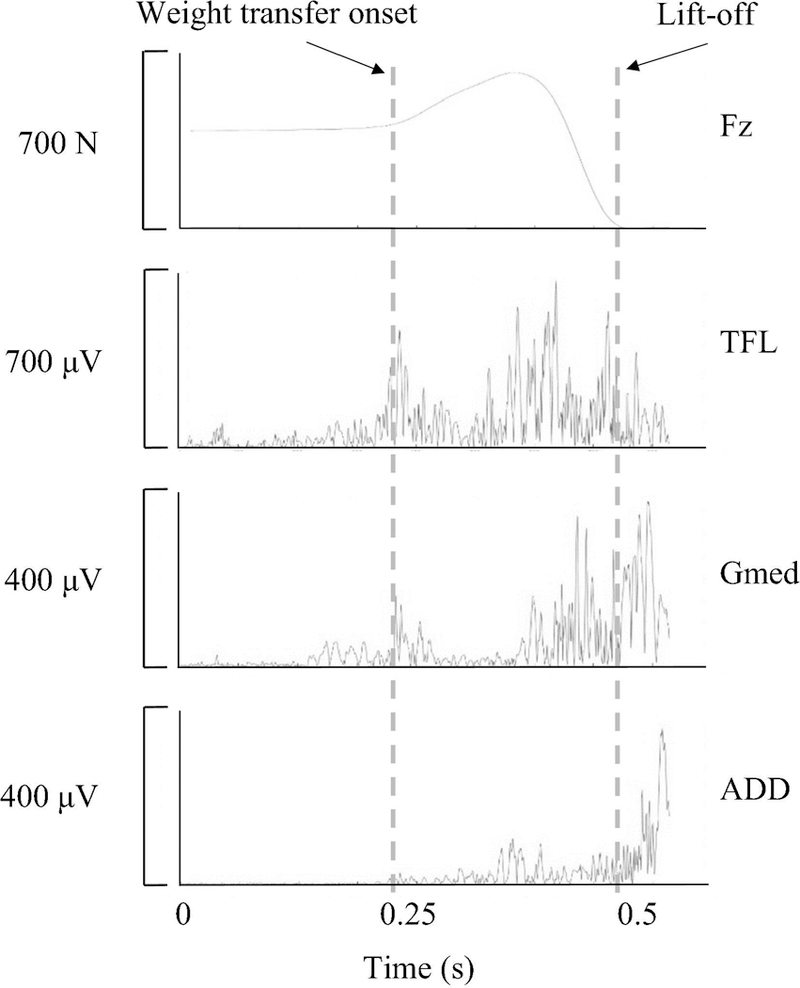
Vertical ground reaction force (Fz) and electromyography signals from the tensor fasciae latae (TFL), gluteus medius (Gmed) and adductor magnus (ADD) during a representative induced lateral stepping trial.
2.3. Data Analysis
For the IMVC task, the rate of torque development (RTD) was calculated with a custom MATLAB program as the steepest slope of the of torque-time curve between trial onset and peak torque, using the following equation:
where, ΔT- change in torque; Δxt - change in time. Peak torque was normalized to subjects’ height and weight.
For the induced stepping task, analyses were performed exclusively on the stepping limb, only for trials where balance was recovered with a single lateral step, over the weight transfer phase. This was defined as the time interval between the weight transfer onset and first-step lift-off (Figure 1). Weight transfer onset was defined as the instant where the vertical ground reaction force of the stepping foot exceeded 3SD above the baseline value determined for the 100ms interval immediately prior to pull onset. First-step lift-off was defined as the time where the stepping foot’s vertical ground reaction force equaled zero.
Kinetic and kinematic data were low pass filtered at 16.5Hz (van den Bogert & de Koning, 1996). Vertical ground reaction rate of force development (RFD) was calculated as the slope of the stepping foot’s vertical ground reaction force, from the onset of the weight transfer to the peak vertical force before lift-off. Inverse dynamics was used to estimate net hip AB-AD torque and power. Calculations were performed using the Newton-Euler equations of motion (Appendix) using a bottom-up approach where the ground reaction forces functioned as the kinetic input to the lowest segment (foot) (Zatsiorsky, 2002). Torque and power values were normalized to subjects’ height and weight.
Inverse dynamics assumptions include: 1) segments are rigid bodies with uniform mass distribution and stable inertial properties; 2) all intersegmental forces pass through singular joint centers; and 3) joint friction is negligible. Segmental inertial properties were estimated using Dempster’s parameters as described by Winter (1992). Horizontal and vertical body CoM momentum was calculated by multiplying each subjects’ mass with their horizontal and vertical CoM velocity, respectively.
The raw EMG signals were band-pass filtered (25–1000Hz), full-wave rectified, and low-pass filtered (6Hz Butterworth 4th order) for smoothing purposes and normalized using the dynamic peak method (Burden, 2010; Sousa & Tavares, 2012). Rate of neuromuscular activation (RActv) was defined as the rate of rise of the normalized EMG amplitude from onset to the peak EMG activity (Clark et al., 2013). EMG activation onset was defined as the time that initiates a continuous increase in EMG amplitude leading to the peak EMG activity.
Independent samples t-tests were used to determine between-group comparisons for the incidence of single lateral steps during the stepping task. Between-group comparisons for the IMVC and induced lateral stepping performance variables were performed using a mixed effects model incorporating the groups as fixed factors and the participants as random factors. Normality was tested using the Shapiro-Wilk test. Correlation analysis was done using Spearman’s correlation (ρ). Values presented are the arithmetic mean ± standard error. Statistical analyses were performed with SPSS v.22 (IBM, Armonk, NY), with significance at p<0.05.
3. Results
For the IMVC task, normalized peak hip AB-AD torques were significantly reduced by 38% and 31% respectively in older (AB: 0.039±0.002; AD: 0.061±0.002, normalized units) compared to younger (AB: 0.063±0.001; AD: 0.088±0.002) adults (Figure 2A, p<0.05). Older adults showed a further 66% reduction in hip AB rate of torque development (RTD) (older: 73.3±6.3 Nm/s; younger: 213.7±20.5 Nm/s, p<0.05, Figure 2B). Hip AD RTD showed a similar but non-significant trend (older: 145.3±12.5 Nm/s; younger: 179.5±16.8 Nm/s, p>0.05, Figure 2B). Similarly, the EMG RActv of the TFL, Gmed and ADD were significantly lower in the older group (3.68±0.20 s−1, 3.38±0.18 s−1, 3.19±0.23 s−1, respectively) compared to younger individuals (4.44±0.24 s−1, 4.63±0.32 s−1, 6.05±0.38 s−1, respectively, Figure 2C).
Figure 2.
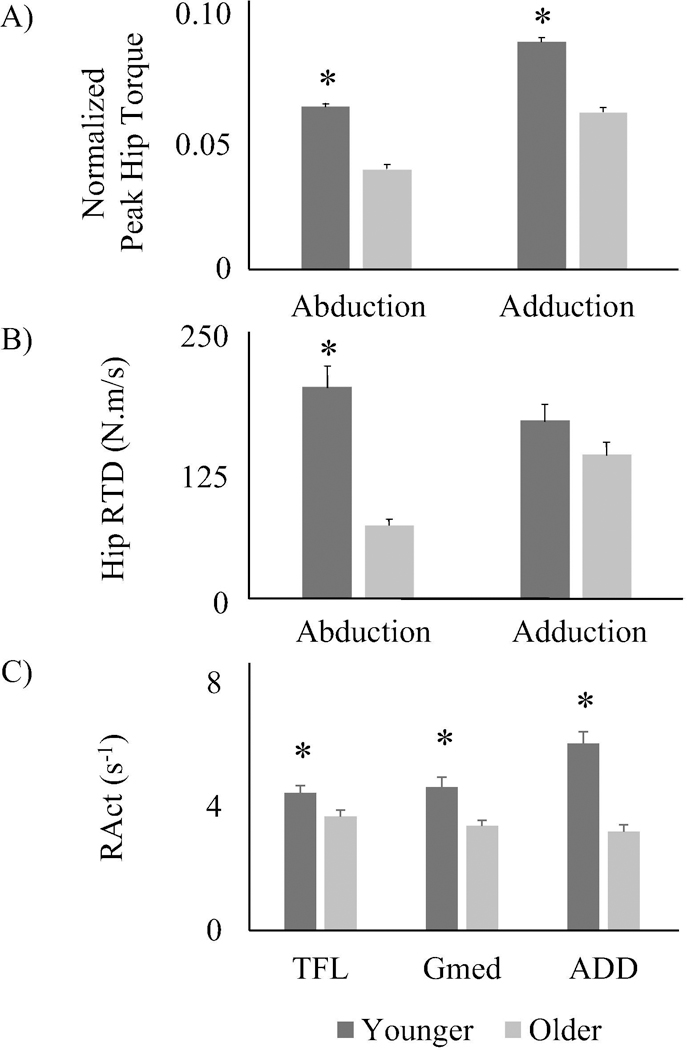
Hip abductor-adductor (AB-AD) isometric maximal voluntary contraction (IMVC) in younger and older adults. A) normalized peak hip torque; B) hip rate of torque development (RTD); C) Normalized neuromuscular rate of activation (RActv) of Tensor Fasciae Latae (TFL), Gluteus Medius (Gmed) and Adductor magnus (ADD). * significantly different from older adults (p<0.05).
In the induced stepping task, older adults demonstrated lower incidences of single lateral steps than younger adults, ranging from approximately 20% in the 50% and 65% pre-load conditions, to about 50% fewer lateral steps in the 80% condition (p<0.05, Table 2). In addition, across the pre-load conditions, the weight transfer phase was initiated later by older individuals (50%: 0.132±0.003 s; 65%: 0.134±0.003 s) than the younger group (50%: 0.096±0.002 s; 65%: 0.104±0.002 s, p<0.05, Figure 3A). Similar results were found for stepping-foot lift-off time (older, 50%: 0.494±0.006 s; 65%: 0.483±0.007 s; 80%: 0.482±0.008 s; younger: 50%: 0.416±0.005 s; 65%: 0.418±0.005 s; 80%: 0.434±0.005 s, p<0.05, Figure 3B).
Table 2.
Incidence of single lateral steps in younger and older adults during the lateral induced stepping task at different initial pre-loads.
| Lateral step incidence (%) | ||
|---|---|---|
| Pre-load Conditions |
Younger Adults (n=15) |
Older Adults (n=15) |
| 50% BW | 92.5±3.2 | 73.3±8.0 * |
| 65% BW | 94.0±2.9 | 65.3±7.4 * |
| 80% BW | 85.4±4.0 | 43.4±8.6 * |
Data presented as Mean ± SEM.
significantly different from younger adults (p<0.05).
Figure 3.
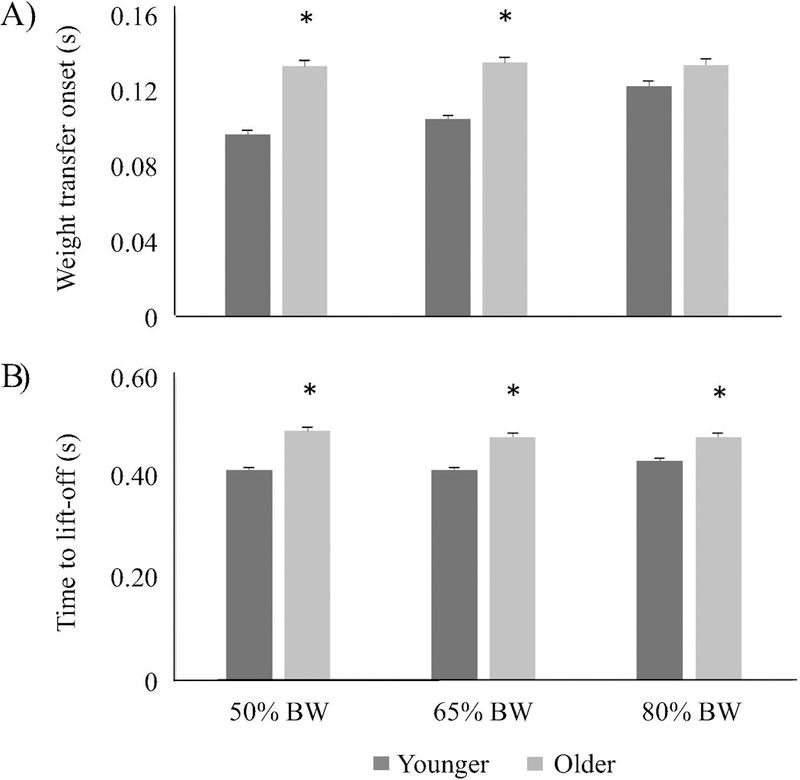
Onset of the weight transfer phase (A) and stepping foot’s time to lift-off (B) in younger and older adults during the lateral induced stepping protocol at different initial pre-loads. * significantly different from younger adults (p<0.05).
At the instant of stepping-foot lift-off, the normalized lateral momentum of the CoM was greater (p<0.05) in the older adults (58.40±1.57 s−1) than the younger adults (47.04±1.17 s−1) for the 50% pre-load condition, and marginally greater at the 65% condition (older: 58.53±1.92 s−1; younger: 47.76±1.30 s−1; p=0.06). Furthermore, at the 50% condition, the older group also had greater (p<0.05) downward CoM momentum at lift-off (10.48±0.90 s−1) than younger adults (6.60±0.53 s−1). Kinetic analysis also showed that vertical ground reaction force RFD for the older individuals (50%: 1777.3±101.4 N/s; 65%: 1598.3±106.5 N/s; 80%: 1245.7±86.8 N/s) was 70.1%−176.8% greater than that for the younger adults (50%: 642.1±38.6 N/s; 65%: 619.5±32.6 N/s; 80%: 732.6±37.1 N/s; p<0.05, Figure 4A).
Figure 4.
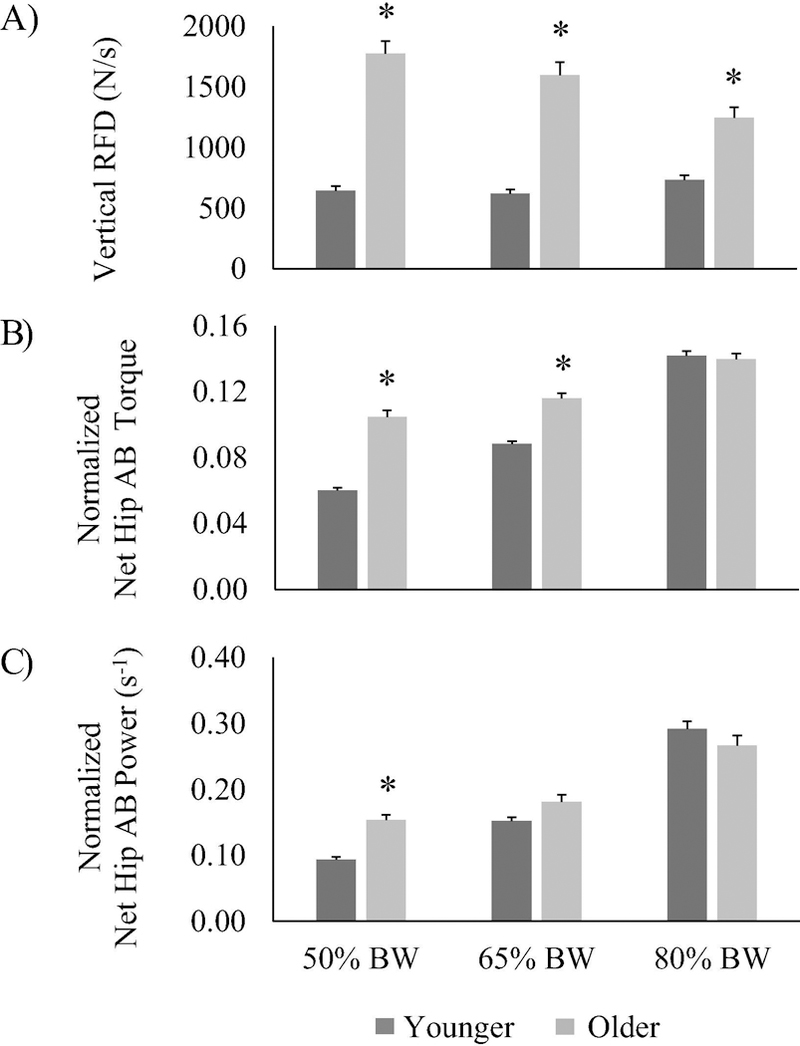
Lateral induced stepping protocol at different initial pre-loads in younger and older adults. A) vertical ground reaction rate of force development (RFD); B) normalized net hip abductor (AB) torque; C) normalized net hip AB power. * significantly different from younger adults (p<0.05).
During the weight transfer phase, inverse dynamics analysis for the stepping limb indicated that older adults generated significantly greater relative net peak AB hip torque than the younger group at 50% and 65% pre-load conditions (older: 0.105±0.004 and 0.116±0.003; younger: 0.060±0.002 and 0.088±0.002; p<0.05, Figure 4B), and greater net peak AB power at the 50% condition (older: 0.153±0.008 s−1; younger: 0.093±0.004 s−1; p<0.05, Figure 4C). In contrast, the EMG activation patterns indicated that RActv of all analyzed muscles was diminished in the older population. Specifically, TFL RActv of older individuals (50%: 5.88±0.25 s−1; 65%: 5.10±0.22 s−1; 80%: 5.09±0.29 s−1; p<0.05, Figure 5) was reduced compared to younger adults (50%: 7.17±0.28 s−1; 65%: 7.63±0.24 s−1; 80%: 7.09±0.27 s−1; p<0.05, Figure 5). Gmed RActv showed similar differences between older (50%: 5.64±0.25 s−1; 65%: 5.93±0.22 s−1; 80%: 6.37±0.23 s−1; p<0.05, Figure 5) and younger individuals (50%: 7.50±0.25 s−1; 65%: 7.96±0.28 s−1; 80%: 7.75±0.23 s−1; p<0.05, Figure 5). ADD RActv was also impaired in older adults (50%: 6.43±0.26 s−1; 65%: 6.05±0.28 s−1; 80%: 6.62±0.29 s−1; p<0.05, Figure 5) compared to the younger group (50%: 8.23±0.33 s−1; 65%: 8.19±0.28 s−1; 80%: 7.66±0.25 s−1; p<0.05, Figure 5).
Figure 5.
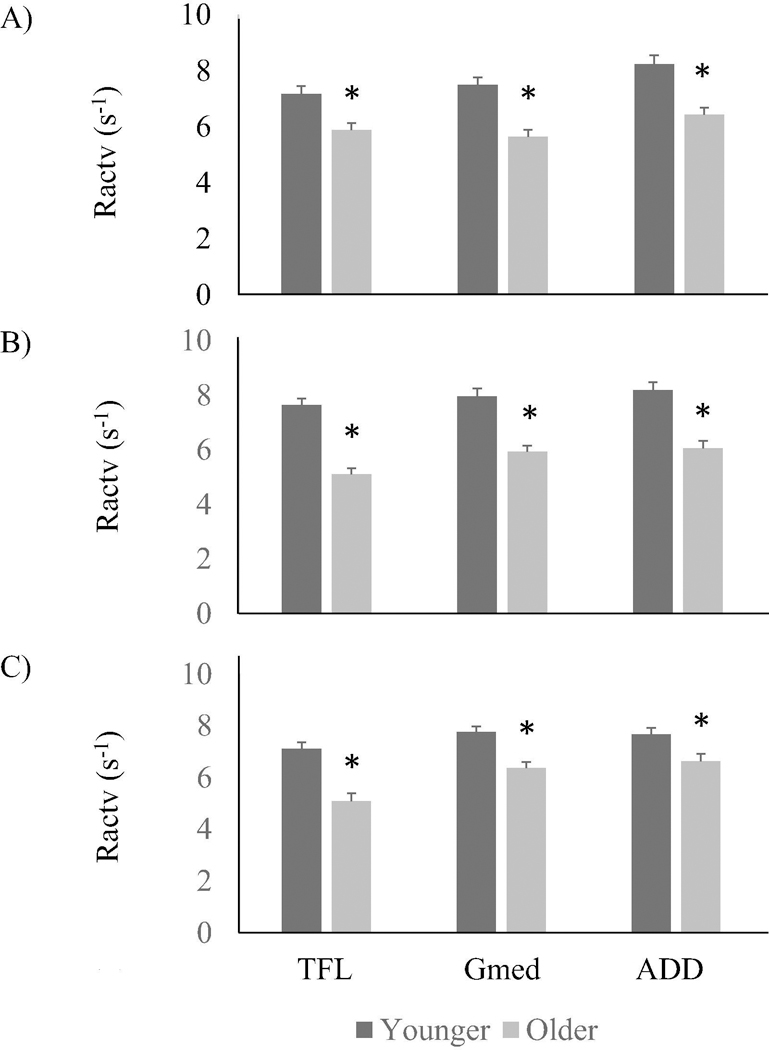
Normalized neuromuscular rate of activation (RActv) of Tensor Fasciae Latae (TFL), Gluteus Medius (Gmed) and Adductor magnus (ADD), in younger and older adults during the lateral induced stepping protocol at 50% (A), 65% (B) and 80% (C) initial pre-loads. * significantly different from younger adults (p<0.05).
Correlation analyses revealed significant moderate positive correlations between the IMVC hip AB-AD peak torque (PT) and the incidence of lateral steps at 65% and 80% pre-load conditions (p<0.05, Table 3). IMVC hip AB RTD was also positively correlated with the incidence of lateral steps, independent of the weight distribution condition (p<0.05, Table 3). Furthermore, TFL, Gmed, and ADD RActv showed moderate correlations with the incidence of lateral steps for all pre-load conditions (p<0.05, Table 3).
Table 3.
Correlations between the incidence of single lateral steps at the different initial pre-loads and hip abductor-adductor (AB-AD) isometric maximal voluntary contraction (IMVC) peak torque (PT), rate of torque development (RTD), and Tensor Fasciae Latae (TFL), Gluteus Medius (Gmed) and Adductor magnus (ADD) rate of neuromuscular activation (RActv).
| IMVC AB PT |
IMVC AB RTD |
IMVC AD PT |
IMVC AD RTD |
TFL RAct |
Gmed RAct |
ADD RAct |
||
|---|---|---|---|---|---|---|---|---|
| Incidence of Lat. Steps at: |
50% BW |
0.30 | 0.48* | 0.19 | 0.21 | 0.48* | 0.50* | 0.42* |
| 65% BW |
0.53* | 0.67* | 0.65* | 0.31 | 0.81* | 0.76* | 0.79* | |
| 80% BW |
0.60* | 0.67* | 0.58* | 0.27 | 0.75* | 0.71* | 0.71* |
Data presented as Spearman correlation coefficients (r).
represents significant correlation (p<0.05).
4. Discussion
The results of this study provide new information about age-related changes in hip neuromuscular and biomechanical contributions to medio-lateral balance control during the weight transfer phase of perturbation-induced lateral protective stepping.
Hip AB-AD Isometric Maximal Voluntary Contractions (IMVC)
As expected, younger individuals showed greater isolated maximum hip neuromuscular performance than older adults (Johnson et al., 2004; Kim et al., 2011; Korff et al., 2014). Although the aging impairments in hip AB-AD peak torque production were relatively large, the observed deficits in maximum RActv and hip AB RTD, important for muscle power generation, were even greater (Aagaard et al., 2002). Similar to previous reports for other lower limb muscles, these findings indicated that the RTD and RActv may be impaired to a greater extent than maximum strength/torque production (Clark et al., 2013; Melzer et al., 2010; Metter et al., 1997). Considering that the most mechanically stable stepping strategy (lateral stepping) requires rapid force generation to advance the passively loaded limb through pre-step weight transfer, these findings provide further insight about the neuromechanical mechanisms of age-related impairment in M-L balance control and increased risk of falls (Orr et al., 2006; Suetta et al., 2004).
Induced lateral stepping
In contrast to what was hypothesized, older individuals recovered balance with a lateral step while performing greater relative vertical RFD and hip AB torque and power production. Nonetheless, younger adults were more successful than older individuals in their ability to use the lateral stepping strategy to recover balance, as reflected in their greater incidence of successful recovery steps. Furthermore, older adults demonstrated a timing delay in the initiation of weight transfer and in the time taken to achieve the stepping foot lift-off. These timing deficits in pre-step weight transfer resulted in overall increased time to initiate a step after the onset of the balance perturbation, and likely contributed to the greater lateral and downward CoM momentum at lift-off (50% pre-load condition) for the older group.
The hip muscle activation patterns during the stepping task also differed substantially between younger and older individuals. Older adults showed reduced hip AB-AD RActv in all pre-load conditions. Considering that neuromuscular RActv is a fundamental component for muscle power generation, this age-related neuromuscular impairment is likely an important contributor to the difficulties with lateral balance recovery and may have contributed to the delayed timing of the weight transfer phase observed for the older adults (Aagaard et al., 2002).
Although older adults attempted to counteract the weight transfer timing deficits by increasing their maximum hip AB torque, power, and vertical rate of force generation, they were still limited by their reduced rate of neuromuscular activation. This greater kinetic performance during the weight transfer phase likely approached their maximum capacity and may represent a saturation point or neuromechanical performance limit. In this regard, previous reports of impaired mobility function in older individuals have identified a similar “over taxation” of the neuromuscular system during activities of daily living (Hortobagyi et al., 2003; Reeves et al., 2009). Furthermore, the observed discrepancy between the greater relative stepping kinetic performance and limited neuromuscular RActv in the older adults may, at least in part, be explained by fact that the RActv is based on the surface EMG from solely the hip AB-AD musculature, while the RFD is calculated from the vertical ground reaction force involving musculature throughout the leg and body and other mechanical factors not captured in the focal neuromuscular recording. While the present focus is on the contributions of the hip AB-AD musculature, the RActv from hip, knee and ankle extensors and multi-segmental kinematics would need to be accounted for to further address this issue.
Associations between IMVC and lateral stepping performance
The association between the incidence of lateral steps and hip AB-AD absolute maximum performance indicated that the greater the maximum peak torque and AB RTD, the greater the incidence of recovering balance with a single lateral step. This was particularly the case when the lateral perturbations were applied with the CoM presumably closer to the limits of the BoS during the 65% and 80% pre-load conditions. Moreover, the hip AB-AD RActv appeared to be of even greater importance for successful lateral stepping than maximal muscular performance, as it consistently showed moderately higher positive associations with the lateral step incidence in all pre-load conditions. Altogether, these associations highlight the increased importance of the rate of neuromuscular activation for successful balance recovery through lateral stepping as it affects the ability to generate rapid force, i.e. muscular power (Aagaard et al., 2002; Clark et al., 2013).
Among the limitations of this study, was that the older group had a higher proportion of male participants. However, gender appeared not to affect the findings as the outcomes were similar in both groups. Although this study did not directly compare the responses between the different pre-loads, it was evident that the 80% pre-load condition was the most challenging for balance recovery as would be expected considering that the CoM was closest to the BoS boundary limit, resulting in less time to perform the weight transfer preceding the lateral step during an evolving perturbation. Hence, in general, the weight transfer phase in the 80% pre-load condition similarly influenced the performance in both groups and represented a comparably challenging condition possibly related to the available capacity limits of neuromechanical performance.
Lastly, these results suggest that the age-associated impairments in hip AB-AD rate of neuromuscular activation and power generation during the pre-step weight transfer phase are important contributing factors affecting the use of more mechanically stable and potentially safer protective stepping strategies. Compared with younger adults, older individuals generally show a lower incidence of taking lateral protective steps which requires stepping with the passively loaded limb. In contrast, older individuals more frequently use cross-over stepping or a medial-lateral stepping sequence that involve stepping with the passively unloaded limb (Addison et al., 2016). Although balance may be successfully recovered using passively unloaded-limb stepping, the consequences for using these strategies are reduced margins of stability at first step landing, multiple recovery steps, longer and more complex stepping trajectories, and increased collisions between the limbs (Bair et al., 2016; Maki et al., 2000; Mille et al., 2013a). Moreover, the predominant use of unloaded-limb stepping patterns has been linked with a greater risk of falls (Mille et al., 2005). Furthermore, the results demonstrate that progressively increasing pre-step limb load demands reduces the incidence of lateral steps leading to balance recovery, especially for the older group. It is conceivable that alleviating these weight transfer neuromechanical deficits in older individuals through intervention training could lead to improved weight transfer function and an increased incidence of lateral stepping.
In conclusion, this study identified new insights on how age-related impairments in maximum hip AB-AD neuromuscular and mechanical performance limit the ability to perform lateral stepping, through deficits in response timing, kinetic performance, and especially rate of neuromuscular activation during the pre-step weight transfer phase. These findings support the need for advancing hip abductor-adductor muscle resistance power training interventions that have been shown to improve the rates of neuromuscular activation and force production, as well as muscular power (Bottaro et al., 2007; Lopes et al., 2016; Nogueira et al., 2009).
Supplementary Material
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Conflict of Interest
We wish to confirm that there are no known conflicts of interest associated with this publication and there has been no significant financial support for this work that could have influenced its outcome.
References
- Aagaard P, Simonsen EB, Andersen JL, Magnusson P, & Dyhre-Poulsen P (2002). Increased rate of force development and neural drive of human skeletal muscle following resistance training. J Appl Physiol, 93(4), 1318–1326. 10.1152/japplphysiol.00283.2002 [DOI] [PubMed] [Google Scholar]
- Aagaard P, Suetta C, Caserotti P, Magnusson SP, & Kjaer M (2010). Role of the nervous system in sarcopenia and muscle atrophy with aging: strength training as a countermeasure. Scand J Med Sci Sports, 20(1), 49–64. 10.1111/j.1600-0838.2009.01084.xSMS1084 [pii] [DOI] [PubMed] [Google Scholar]
- Addison O, Inacio M, Bair WN, Beamer BA, Ryan AS, & Rogers MW (2016). Role of Hip Abductor Muscle Composition and Torque in Protective Stepping for Lateral Balance Recovery in Older Adults. Arch Phys Med Rehabil 10.1016/j.apmr.2016.10.009 [DOI] [PMC free article] [PubMed]
- Addison O, Young P, Inacio M, Bair WN, Prettyman MG, Beamer BA, … Rogers MW (2014). Hip but not thigh intramuscular adipose tissue is associated with poor balance and increased temporal gait variability in older adults. Curr Aging Sci, 7(2), 137–143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bair WN, Prettyman MG, Beamer BA, & Rogers MW (2016). Kinematic and behavioral analyses of protective stepping strategies and risk for falls among community living older adults. Clin Biomech, 36, 74–82. 10.1016/j.clinbiomech.2016.04.015 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barrett RS, Cronin NJ, Lichtwark GA, Mills PM, & Carty CP (2012). Adaptive recovery responses to repeated forward loss of balance in older adults. J Biomech, 45(1), 183–187. 10.1016/j.jbiomech.2011.10.005 [DOI] [PubMed] [Google Scholar]
- Bottaro M, Machado SN, Nogueira W, Scales R, & Veloso J (2007). Effect of high versus low-velocity resistance training on muscular fitness and functional performance in older men. Eur J Appl Physiol, 99(3), 257–264. 10.1007/s00421-006-0343-1 [DOI] [PubMed] [Google Scholar]
- Burden A (2010). How should we normalize electromyograms obtained from healthy participants? What we have learned from over 25 years of research. J Electromyogr Kinesiol, 20(6), 1023–1035. 10.1016/j.jelekin.2010.07.004S1050-6411(10)00100-8 [pii] [DOI] [PubMed] [Google Scholar]
- Clark DJ, Patten C, Reid KF, Carabello RJ, Phillips EM, & Fielding RA (2011). Muscle performance and physical function are associated with voluntary rate of neuromuscular activation in older adults. J Gerontol A Biol Sci Med Sci, 66(1), 115–121. 10.1093/gerona/glq153glq153 [pii] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark DJ, Pojednic RM, Reid KF, Patten C, Pasha EP, Phillips EM, & Fielding RA (2013). Longitudinal Decline of Neuromuscular Activation and Power in Healthy Older Adults. J Gerontol A Biol Sci Med Sci 10.1093/gerona/glt036 [DOI] [PMC free article] [PubMed]
- De Luca CJ (1997). The use of surface electromyography in biomechanics. Journal of Applied Biomechanics, 13(2), 135–163. [Google Scholar]
- Fujimoto M, Bair WN, & Rogers MW (2017). Single and multiple step balance recovery responses can be different at first step lift-off following lateral waist-pull perturbations in older adults. J Biomech, 55, 41–47. 10.1016/j.jbiomech.2017.02.014 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hausdorff JM, Rios DA, & Edelberg HK (2001). Gait variability and fall risk in community-living older adults: a 1-year prospective study. Arch Phys Med Rehabil, 82(8), 1050–1056. [DOI] [PubMed] [Google Scholar]
- Hermens HJ, Freriks B, Disselhorst-Klug C, & Rau G (2000). Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol, 10(5), 361–374. doi: S1050-6411(00)00027-4[pii] [DOI] [PubMed] [Google Scholar]
- Hilliard MJ, Martinez KM, Janssen I, Edwards B, Mille ML, Zhang Y, & Rogers MW (2008). Lateral balance factors predict future falls in community-living older adults. Arch Phys Med Rehabil, 89(9), 1708–1713. 10.1016/j.apmr.2008.01.023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hortobagyi T, Mizelle C, Beam S, & DeVita P (2003). Old adults perform activities of daily living near their maximal capabilities. J Gerontol A Biol Sci Med Sci, 58(5), M453–460. [DOI] [PubMed] [Google Scholar]
- Hurt CP, & Grabiner MD (2015). Age-related differences in the maintenance of frontal plane dynamic stability while stepping to targets. J Biomech, 48(4), 592–597. 10.1016/j.jbiomech.2015.01.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Inacio M, Ryan AS, Bair WN, Prettyman M, Beamer BA, & Rogers MW (2014). Gluteal muscle composition differentiates fallers from non-fallers in community dwelling older adults. BMC Geriatr, 14, 37 10.1186/1471-2318-14-37 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Inoue W, Ikezoe T, Tsuboyama T, Sato I, Malinowska KB, Kawaguchi T, … Ichihashi N (2017). Are there different factors affecting walking speed and gait cycle variability between men and women in community-dwelling older adults? Aging Clin Exp Res, 29(2), 215–221. 10.1007/s40520-016-0568-8 [DOI] [PubMed] [Google Scholar]
- Johnson ME, Mille ML, Martinez KM, Crombie G, & Rogers MW (2004). Age-related changes in hip abductor and adductor joint torques. Arch Phys Med Rehabil, 85(4), 593–597. doi: S0003999303010669 [pii] [DOI] [PubMed] [Google Scholar]
- Kanda K, Hashizume K, Miwa T, & Miwa Y (1996). Overloading a muscle does not alter the rate of motoneuronal loss in aged rats. Neurobiol Aging, 17(4), 613–617. doi: S0197458096000048 [pii] [DOI] [PubMed] [Google Scholar]
- Kido A, Tanaka N, & Stein RB (2004). Spinal excitation and inhibition decrease as humans age. Can J Physiol Pharmacol, 82(4), 238–248. 10.1139/y04-017y04-017 [pii] [DOI] [PubMed] [Google Scholar]
- Kim JW, Kwon Y, Chung HY, Eom GM, Jun JH, Chung JS, & Park BK (2011). Age-sex differences in the hip abductor muscle properties. Geriatr Gerontol Int, 11(3), 333–340. 10.1111/j.1447-0594.2011.00693.x [DOI] [PubMed] [Google Scholar]
- Korff T, Newstead AH, van Zandwijk R, & Jensen JL (2014). Age- and activity-related differences in the mechanisms underlying maximal power production in young and older adults. J Appl Biomech, 30(1), 12–20. 10.1123/jab.2013-0037 [DOI] [PubMed] [Google Scholar]
- Lopes PB, Pereira G, Lodovico A, Bento PC, & Rodacki AL (2016). Strength and Power Training Effects on Lower Limb Force, Functional Capacity, and Static and Dynamic Balance in Older Female Adults. Rejuvenation Res 10.1089/rej.2015.1764 [DOI] [PubMed]
- Luchies CW, Alexander NB, Schultz AB, & Ashton-Miller J (1994). Stepping responses of young and old adults to postural disturbances: kinematics. J Am Geriatr Soc, 42(5), 506–512. [DOI] [PubMed] [Google Scholar]
- Maki BE, Edmondstone MA, & McIlroy WE (2000). Age-related differences in laterally directed compensatory stepping behavior. J Gerontol A Biol Sci Med Sci, 55(5), M270–277. [DOI] [PubMed] [Google Scholar]
- Maki BE, Holliday PJ, & Topper AK (1994). A prospective study of postural balance and risk of falling in an ambulatory and independent elderly population. J Gerontol, 49(2), M72–84. [DOI] [PubMed] [Google Scholar]
- Maki BE, & McIlroy WE (2006). Control of rapid limb movements for balance recovery: age-related changes and implications for fall prevention. Age Ageing, 35 Suppl 2, ii12–ii18. 10.1093/ageing/afl078 [DOI] [PubMed] [Google Scholar]
- Maki BE, McIlroy WE, & Perry SD (1996). Influence of lateral destabilization on compensatory stepping responses. J Biomech, 29(3), 343–353. [DOI] [PubMed] [Google Scholar]
- Melzer I, Krasovsky T, Oddsson LI, & Liebermann DG (2010). Age-related differences in lower-limb force-time relation during the push-off in rapid voluntary stepping. Clin Biomech (Bristol, Avon), 25(10), 989–994. 10.1016/j.clinbiomech.2010.07.009 [DOI] [PubMed] [Google Scholar]
- Metter EJ, Conwit R, Tobin J, & Fozard JL (1997). Age-associated loss of power and strength in the upper extremities in women and men. J Gerontol A Biol Sci Med Sci, 52(5), B267–276. [DOI] [PubMed] [Google Scholar]
- Mille ML, Johnson-Hilliard M, Martinez KM, Zhang Y, Edwards BJ, & Rogers MW (2013a). One step, two steps, three steps more … Directional vulnerability to falls in community-dwelling older people. J Gerontol A Biol Sci Med Sci, 68(12), 1540–1548. 10.1093/gerona/glt062 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mille ML, Johnson-Hilliard M, Martinez KM, Zhang Y, Edwards BJ, & Rogers MW (2013b). One Step, Two Steps, Three Steps More … Directional Vulnerability to Falls in Community-Dwelling Older People. J Gerontol A Biol Sci Med Sci doi: glt062 [pii] 10.1093/gerona/glt062 [DOI] [PMC free article] [PubMed]
- Mille ML, Johnson ME, Martinez KM, & Rogers MW (2005). Age-dependent differences in lateral balance recovery through protective stepping. Clin Biomech, 20(6), 607–616. 10.1016/j.clinbiomech.2005.03.004 [DOI] [PubMed] [Google Scholar]
- Nogueira W, Gentil P, Mello SN, Oliveira RJ, Bezerra AJ, & Bottaro M (2009). Effects of power training on muscle thickness of older men. Int J Sports Med, 30(3), 200–204. 10.1055/s-0028-1104584 [DOI] [PubMed] [Google Scholar]
- Orr R, de Vos NJ, Singh NA, Ross DA, Stavrinos TM, & Fiatarone-Singh MA (2006). Power training improves balance in healthy older adults. J Gerontol A Biol Sci Med Sci, 61(1), 78–85. doi: 61/1/78 [pii] [DOI] [PubMed] [Google Scholar]
- Pai YC, Bhatt T, Yang F, & Wang E (2014). Perturbation training can reduce community-dwelling older adults’ annual fall risk: a randomized controlled trial. J Gerontol A Biol Sci Med Sci, 69(12), 1586–1594. 10.1093/gerona/glu087 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patton JL, Hilliard MJ, Martinez K, Mille ML, & Rogers MW (2006). A simple model of stability limits applied to sidestepping in young, elderly and elderly fallers. Conf Proc IEEE Eng Med Biol Soc, 1, 3305–3308. 10.1109/IEMBS.2006.260199 [DOI] [PubMed] [Google Scholar]
- Pidcoe PE, & Rogers MW (1998). A closed-loop stepper motor waist-pull system for inducing protective stepping in humans. J Biomech, 31(4), 377–381. [DOI] [PubMed] [Google Scholar]
- Reeves ND, Spanjaard M, Mohagheghi AA, Baltzopoulos V, & Maganaris CN (2009). Older adults employ alternative strategies to operate within their maximum capabilities when ascending stairs. J Electromyogr Kinesiol, 19(2), e57–68. 10.1016/j.jelekin.2007.09.009 [DOI] [PubMed] [Google Scholar]
- Reid KF, Doros G, Clark DJ, Patten C, Carabello RJ, Cloutier GJ, … Fielding RA (2012). Muscle power failure in mobility-limited older adults: preserved single fiber function despite lower whole muscle size, quality and rate of neuromuscular activation. Eur Appl Physiol, 112(6), 2289–2301. 10.1007/s00421-011-2200-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Robinovitch SN, Feldman F, Yang Y, Schonnop R, Leung PM, Sarraf T, … Loughin M (2013). Video capture of the circumstances of falls in elderly people residing in long-term care: an observational study. Lancet, 381(9860), 47–54. 10.1016/S0140-6736(12)61263-XS0140-6736(12)61263-X [pii] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogers MW, & Mille ML (2003). Lateral stability and falls in older people. Exerc Sport Sci Rev, 31(4), 182–187. [DOI] [PubMed] [Google Scholar]
- Sousa A, & Tavares J (2012). Surface electromyographic amplitude normalization methods: A review Electromyography: New Developments, Procedures and Applications (pp. pp. 85–102): Nova Science Publishers, Inc. [Google Scholar]
- Sturnieks DL, Menant J, Delbaere K, Vanrenterghem J, Rogers MW, Fitzpatrick C, & Lord SR (2013). Force-controlled balance perturbations associated with falls in older people: a prospective cohort study. PLoS One, 8(8), e70981 10.1371/journal.pone.0070981 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suetta C, Aagaard P, Rosted A, Jakobsen AK, Duus B, Kjaer M, & Magnusson SP (2004). Training-induced changes in muscle CSA, muscle strength, EMG, and rate of force development in elderly subjects after long-term unilateral disuse. J Appl Physiol, 97(5), 1954–1961. 10.1152/japplphysiol.01307.200301307.2003 [pii] [DOI] [PubMed] [Google Scholar]
- van den Bogert AJ, & de Koning JJ (1996). ON OPTIMAL FILTERING FOR INVERSE DYNAMICS ANALYSIS. Proceedings of the IXth Biennial Conference of the Canadian Society for Biomechanics, 214–215. [Google Scholar]
- WHO, W. H. O. (2012). Falls Retrieved 2012, 2012, from http://www.who.int/violence_injury_prevention/other_injury/falls/en/index.html
- Winter DA (1992). Biomechanics and Motor Control of Human Movements (2nd ed.).Waterloo, Canada: University of Waterloo Press. [Google Scholar]
- Yoshida Y, Marcus RL, & Lastayo PC (2012). Intramuscular adipose tissue and central activation in older adults. Muscle Nerve, 46(5), 813–816. 10.1002/mus.23506 [DOI] [PubMed] [Google Scholar]
- Yungher DA, Morgia J, Bair WN, Inacio M, Beamer BA, Prettyman MG, & Rogers MW (2012). Short-term changes in protective stepping for lateral balance recovery in older adults. Clin Biomech, 27(2), 151–157. 10.1016/j.clinbiomech.2011.09.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zatsiorsky V (2002). Kinetics of Human Motion Champaign, IL, USA. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.