

Abstract
Background:
Recently, with the development of information and communication technology in the healthcare industry, the tools of this technology have different applications such as Health Smart Card in this area. The main application of health smart card in the field of ophthalmology is providing demographic and clinical information for different people. Therefore, this study was done to identify and prioritize the data elements of the ophthalmology health smart card.
Methods:
This study was a descriptive-development one that was done in 2017. A review was conducted in relevant databases including PubMed, Web of knowledge, Science direct, and Web of Science to identify appropriate related sources. In the second phase, the ophthalmology specialists and health information managers (20) in RassolAkram, Farabi and Noor Eye Hospital consulted by a questionnaire for health smart card requirements. This study carried out in Iran. Collected data were analyzed by descriptive methods in SPSS software version 19.
Results:
Two categories of demographic and clinical data requirements for health smart card were determined. Patient ID, Occupation, and National Code were the most important demographic requirements of ophthalmology health card. Furthermore, clinical data elements of the ophthalmology health smart card were identified in three categories: Corneal Tests, Retinal Tests, Glaucoma Tests, and Associated Conditions.
Conclusion:
Using the identified data elements, it is possible to design and implement an ophthalmology health smart card. Developing an ophthalmology health smart card is expected to progress of information retrieve, facilitate communication of healthcare organizations and improve healthcare quality.
Keywords: Health smart cards, Common data elements, Ophthalmology
1. INTRODUCTION
By increasing prevalence and complexity of chronic diseases, significant reorganizations necessary in the health system. In this regard various forms of health information technology have ability to facilitate and support the reorganization (1). Electronic medical records is a way to record information about people’s health which are created the possibility use of this information by clinicians, managers, researchers, quality improvement team and decision support systems. Medical record offers information about medical history, laboratory results, diagnostic tests, dosing and therapeutic intervention for the patient (2).
At three levels, we can be distinguished the primary use of electronic health records or electronic medical records (EHR or EMR). The first level any use of electronic medical records. The second level of basic electronic medical records, which include: identifying information, problem list, medication orders, lab results and reports of treatment and clinical images, third level includes warnings about interactions pharmaceutical, electronic prescribing medication, electronic transmission of data between different departments and managed applications (3).
Connecting to database of hospital information is a common practice to achieve patient information. However, in some cases, access to databases from different workstations at the same time causing performance problems due to high data rate (data rate). Also the patient information may need in an environment free from connecting to data networks such as ambulance or at the hospital where unregistered patient information is required. These problems can be solved with increase of hospital automation system capabilities by using the intelligent storage and recovery mechanisms and portable devices that can play a key role in sharing the patient information (4).
Smart card used as a portable tool with the ability to store and process information and it is common because of increase the capacity and efficiency of their use in the health system (5). Effective use of smart cards is more favorable to be answered by medical personnel with quick and easy access to patient information at different times and places to patient who has Cardholder information (6, 7). Developing the smart cards of portable personal health care records is a cost-effective system in a simple framework for storage and transfer of patient records with the technologies available to address the inefficiencies of paper records system and simultaneously can be used as a delivery system to facilitate the adoption of electronic medical records which fully employed and progressive step towards a national system of electronic medical records (8).
Use of electronic records in the field of ophthalmology can facilitate diagnostic and therapeutic processes. On the other hand, itis very important to give ophthalmology records during examination and ophthalmologists need any important medical information (9, 10). The main purpose of the present study was to identifying and prioritizing of data elements for ophthalmology health smart card.
2. AIM
Current research was a descriptive-development one to identifying and prioritizing of data elements for ophthalmology health smart card.
3. MATERIAL AND METHODS
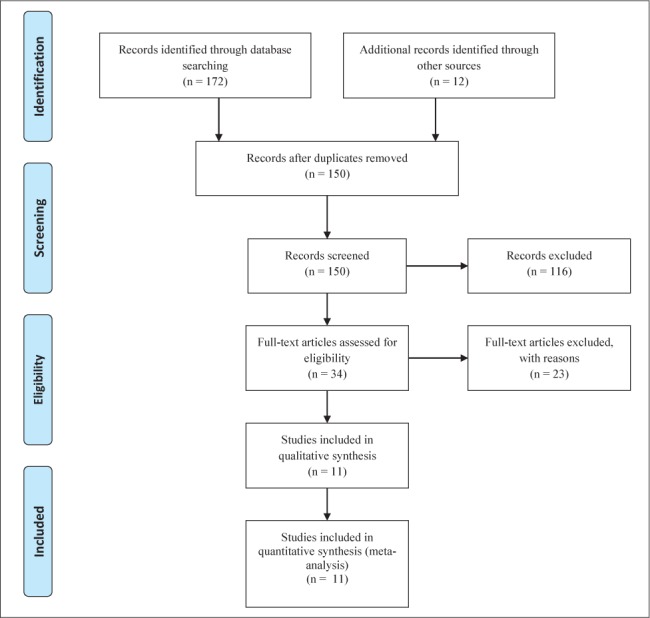
In the first phase of this study, a review was conducted in relevant databases including PubMed, Web of knowledge, Science direct, and Web of Science to identify appropriate related sources. Keywords that used to search for sources of information include the following: data elements, minimum data set, health smart card, health card, and ophthalmology. Articles that were published between 2000 and 2017 were selected. Our inclusion criteria were: Full text papers with the keywords in the title or abstracts, studies that published in 2000 to November 29, 2017, and studies published in English language. We excluded resources such as reports, editorial letters, newspapers, and abstracts. We also excluded studies that addressed the broader field of health smart card, which isn’t applicable in the field of ophthalmology. Using the search strategies, 184 records were retrieved and 11 papers were comprehensively surveyed (Figure 1). At this stage, by reviewing of related papers (5, 7, 8, 11-18), the data elements for ophthalmology health smart card were identified. A questionnaire was designed based on information obtained from similar articles and review of ophthalmology forms approved by the Ministry of Health. The questionnaire consisted of five sections and 37 questions, including demographic data elements (11 questions), clinical data elements including: Corneal Tests (7 questions), Retinal Tests (6 questions), Glaucoma Tests (7 questions), and Associated Conditions (6 questions) that were based on the 5-point Likert scale (strongly agree, Agree, Don’t have any idea, Disagree, and Completely disagree). The questionnaire reliability was calculated through Cronbach’s 0.85 alpha calculations and its validity was evaluated and verified by 5 ophthalmology specialists and 4 health information management specialists. In order to data collection and increase the number of participants in this research in-person method was used.
Figure 1. Search results from different databases.
In the second phase, ophthalmology and health information management specialists (n=20) were consulted for health smart card requirements. The statistical population was all of ophthalmology and health information management specialists (n=20) in Rassol Akram, Farabi and Noor Eye Hospital that due to the limitations of community members, all individuals were included to study. Collected data were analyzed by using SPSS version 19 (SPSS Inc., Chicago, Illinois, USA), descriptive statistics and frequency distribution report. In this way the questionnaire items were scored from 1 to 5 (Strongly agree=5, Agree=4, Don’t have any idea=3, Disagree=2, and Completely disagree=1) and each of the data items that had got at least a mean score of 2.5 or more was measured as selected data elements from perspective of ophthalmology specialists.
4. RESULTS
Based on the findings of the first phase of this study, no study was conducted on the design or survey of the requirements for ophthalmology health smart cards. Therefore, the demographic data requirements were obtained by review of related articles, but the clinical data requirements were obtained by studying the ophthalmology forms approved by the Ministry of Health. Different stages of reviewing articles are showed in PRISMA flow diagram. Figure 1 shows the resources that were recovered but did not meet inclusion criteria and were excluded from this study.
The findings of the first phase showed that, 37 data elements were identified for ophthalmology health smart card. Moreover, the findings of the second phase of the present study showed that 7 data elements for demographic requirements and 21 data elements for clinical requirements were selected. Patient ID, Occupation, and National Code were the most important demographic requirements of ophthalmology health smart card (Table 1).
Table 1. Identified and selected demographic data elements of ophthalmology health smart card. *Selected Items.
| N | Demographic | |
|---|---|---|
| Data element | Value | |
| 1 | Patient ID* | 4.9 |
| 2 | First name and last name* | 3.8 |
| 3 | National Code* | 4.5 |
| 4 | Age* | 3.8 |
| 5 | Father’s name* | 3.6 |
| 6 | Religion | 2.0 |
| 7 | Place of Issue | 1.9 |
| 8 | Phone number* | 2.8 |
| 9 | Address | 2.2 |
| 10 | Occupation* | 4.7 |
| 11 | Postal code | 2.3 |
Furthermore, clinical data elements of ophthalmology health smart card were identified in three categories: Corneal Tests, Retinal Tests, Glaucoma Tests, and Associated Conditions. Identified and selected clinical data elements of ophthalmology health smart card are shown in Table 2.
Table 2. Identified and selected clinical data elements for demographic of ophthalmology health smart card. *Selected Items.
| N | Clinical | ||
|---|---|---|---|
| Data element | Value | ||
| 1 | Corneal Tests | Pachymetry* | 4.9 |
| Aberrometry* | 3.8 | ||
| Pentacam* | 3.5 | ||
| Blink reflex* | 4.0 | ||
| Orbscan* | 4.1 | ||
| Enhanced Corneal Compensation (ECC) * | 3.9 | ||
| Variable Corneal Compensation (VCC) * | 4.2 | ||
| 2 | Retinal Tests | Diagnostic B-scan* | 3.8 |
| Diagnostic A-Scan* | 3.7 | ||
| Fluorescein Angiography* | 4.2 | ||
| Indocyanine Green Angiography (ICG) * | 2.9 | ||
| Visual field test* | 3.0 | ||
| Optical coherence tomography (OCT) * | 3.8 | ||
| 3 | Glaucoma Tests | Heidelberg Retina Tomograph 3 (HRT3) * | 4.5 |
| The Ocular Response Analyzer (ORA) * | 4.5 | ||
| Electrooculography (EOG) * | 3.8 | ||
| Visual Evoked Potential (VEP) | 4.0 | ||
| Electroretinography (ERG) * | 4.2 | ||
| Selective Laser Trabeculoplasty (SLT) * | 3.6 | ||
| The Intraocular Lens Master (IOLM) * | 3.2 | ||
| 4 | Associated Conditions | Kidney diseases | 2.1 |
| Liver disease | 1.8 | ||
| Neurological diseases | 2.4 | ||
| Diabetes* | 3.5 | ||
| Allergies | 1.0 | ||
| History of surgery | 2.3 |
5. DISCUSSION
This study was examined the requirements for creating a health card in Eye Hospitals, and after doing research, health card was designed, created and ready for use. So far, many studies have been conducted in line with the actual use of smart cards which reflects the positive impact on improving the quality of health cards and electronic health records and is a step towards reaching the infrastructure (12).
According to the findings, 11 data elements for demographic requirements and 26 data elements for clinical data elements were identified. Mehraeen et al. in a related study by full-text reviewing of 9 related articles, the identified elements were justified in three main categories and 37 subcategories including: clinical data elements, technical capabilities and demographic data elements. According to the findings of this similar study, among the clinical category, 11 data elements and six data elements were selected as the demographic category by the statistical population (19). Navato et al., in a developmental study, identified requirements of an intelligent system for tracking the care of patients in six categories: data acquisition requirements, telecommunications cost, privacy and data security, text message content, communication, and system scalability. The findings of this similar study showed that using this system could improve quality of healthcare and facilitate communication of healthcare organizations (20).
According to results of this study, seven data elements for demographic requirements and 21 data elements for clinical requirements were selected. Structured and accessible clinical data set is a prerequisite for optimum information management and efficient clinical procedures in every healthcare organization (21). In a similar study, to design of Taiwan health care system were studied and finally profile system designed were provided according to the requirements and specifications native Taiwanese access systems, and it became clear that indigenous people identifying information should be carefully considered for the design of the health card (22).Kardaset al. in a similar study that was related to design and application of smart cards in health information systems, two smart card software modules was used to identify personnel and the transfer of data between systems, in addition to identifying information, general information about the patient’s health was embedded in the card design fields (5).
Patient ID, Occupation, and National Code were the most important demographic requirements of ophthalmology health smart card. Furthermore, clinical data elements of ophthalmology health smart card were identified in three categories: Corneal Tests, Retinal Tests, Glaucoma Tests, and Associated Conditions. Similar studies refers to principle and efficacy of smart cards with specific patients manage drug effect of using smart cards medication management of patients with specific reference to the importance of clinical information in the design of smart card, although it is not much time goes on deployment of smart cards in the healthcare system, especially in the health insurance organization in charge of the country, but use of health cart improves management of drug use in certain patients and other patients (14, 23-25).
6. CONCLUSIONS
Developing an ophthalmology health smart card is expected to progress of information retrieve, facilitate communication of healthcare organizations and improve of healthcare quality. A cohort study to identify the additional necessities such as technical and strategically requirements of a ophthalmology health smart card can be done as future research on this topic.
Acknowledgments:
This manuscript was based on some results of the Master’s Degree dissertation in Health Information Technology at the Tehran University of Medical Sciences. The authors extend thanks to ophthalmology specialists of RassolAkram, Farabi and Noor Eye Hospital.
Author contribution:
Conception and design of study: Safdari R, Ghazi-saeedi M. Acquisition of data: Noori T, Shamsabadi A, Mehraeen E.Analysis and/or interpretation of data: Noori T, Shamsabadi A, Mehraeen E. Drafting the manuscript: Shamsabadi A, Mehraeen E. Revising the manuscript critically for important intellectual content: Mehraeen E.
Financial support and sponsorship:
None.
Conflict of interest:
There are no conflict of interest.
REFERENCES
- 1.Herrin J, Graca B, Nicewander D, Fullerton C, Aponte P, Stanek G. The effectiveness of implementing an electronic health record on diabetes care and outcomes. Health services research. 2012;47(4):1522–1540. doi: 10.1111/j.1475-6773.2011.01370.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Hussain F, Qamar U. Identification and Correction of Misspelled Drugs’ Names in Electronic Medical Records (EMR) 2016 [Google Scholar]
- 3.Lehmann CU, O’Connor KG, Shorte VA, Johnson TD. Use of electronic health record systems by office-based pediatricians. Pediatrics. 2014:1115. doi: 10.1542/peds.2014-1115. [DOI] [PubMed] [Google Scholar]
- 4.Liu CT, Yang PT, Yeh YT, Wang BL. The impacts of smart cards on hospital information systems - An investigation of the first phase of the national health insurance smart card project in Taiwan. International Journal of Medical Informatics. 2006 Feb 1;75(2):173–181. doi: 10.1016/j.ijmedinf.2005.07.022. [DOI] [PubMed] [Google Scholar]
- 5.Kardas G, Tunali ET. Design and implementation of a smart card based healthcare information system. Computer methods and programs in biomedicine. 2006;81(1):66–78. doi: 10.1016/j.cmpb.2005.10.006. [DOI] [PubMed] [Google Scholar]
- 6.Grogan D. Smart Cards In Healthcare: A Logical Evolution. Smart Card Association. 2007.
- 7.Masoudi Asl I, Nasiripour A, Esmaeillou Y. Relationship of using smart card and drug consumption management of MS specific patients. Journal of Military Medicine. 2012;13(4):229–233. [Google Scholar]
- 8.Xiao C, Yu A. Medical Smart Card System for Patient Record Management. Molecular and Cell Biology University of California–Berkeley. 2009:12. [Google Scholar]
- 9.Hashemi H, Rezvan F, Khabazkhoob M, Gilasi H, Etemad K, Mahdavi A, Asgari S. Trend in cataract surgical rate in Iran provinces. Iranian journal of public health. 2014 Jul;43(7):961. [PMC free article] [PubMed] [Google Scholar]
- 10.Kirkwood BJ, Pesudovs K, Loh RS, Coster DJ. Implementation and evaluation of an ophthalmic nurse practitioner emergency eye clinic. Clinical & experimental ophthalmology. 2005 Dec;33(6):593–597. doi: 10.1111/j.1442-9071.2005.01101.x. [DOI] [PubMed] [Google Scholar]
- 11.Shelfer KM, Procaccino JD. Smart card evolution. Communications of the ACM. 2002;45(7):83–88. [Google Scholar]
- 12.Liu CT, Yang PT, Yeh YT, Wang BL. The impacts of smart cards on hospital information systems - An investigation of the first phase of the national health insurance smart card project in Taiwan. International Journal of Medical Informatics. 2006;75(2):173–181. doi: 10.1016/j.ijmedinf.2005.07.022. [DOI] [PubMed] [Google Scholar]
- 13.Latha NA, Murthy BR, Sunitha U. Smart Card Based Integrated Electronic Health. Record System for Clinical Practice. Editorial Preface. 2012;3(10) [Google Scholar]
- 14.Hsu MH, Yen JC, Chiu WT, Tsai SL, Liu CT, Li YC. Using health smart cards to check drug allergy history: The perspective from Taiwan’s experiences. Journal of medical systems. 2011;35(4):555–558. doi: 10.1007/s10916-009-9391-5. [DOI] [PubMed] [Google Scholar]
- 15.Kumari S, Chaudhry SA, Wu F, Li X, Farash MS, Khan MK. An improved smart card based authentication scheme for session initiation protocol. Peer-to-Peer Networking and Applications. 2017 Jan 1;10(1):92–105. [Google Scholar]
- 16.Mayes K. An introduction to smart cards. InSmart Cards, Tokens, Security and Applications. 2017:1–29. [Google Scholar]
- 17.Islam SK. Design and analysis of an improved smartcard-based remote user password authentication scheme. International Journal of Communication Systems. 2016 Jul 25;29(11):1708–1719. [Google Scholar]
- 18.Bona JK, Cox MA. inventors; X-Card Holdings, Llc, assignee. Secure smart card system. 2015 Sep 8. United States patent US 9, 129, 28.
- 19.Mehraeen E, Safdari R, SeyedAlinaghi SA, Mohammadzadeh N, Mohraz M. Common elements and features of a mobile-based self-management system for people living with HIV. Electronic Physician. 2018;10(4):6655–6662. doi: 10.19082/6655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mehraeen E, Safdari R, Mohammadzadeh N, Seyedalinaghi S, Forootan S, Mohraz M. Mobile-Based Applications and Functionalities for Self-Management of People Living with HIV. Studies in health technology and informatics. 2018;248:172–179. [PubMed] [Google Scholar]
- 21.Pakgaohar A, Sadegi Kia A. Analysis of accident data by decision trees. Traffic Manage Study. 2009;3(8):27–47. [Google Scholar]
- 22.Wu TY, Majeed A, Kuo KN. An overview of the healthcare system in Taiwan. London journal of primary care. 2010 Dec 1;3(2):115–119. doi: 10.1080/17571472.2010.11493315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Tavakoli A. MM, Khajenasir R. Second International Conference on Electronics City. Tehran: 2009. The provision of Iran health cards, from dream to reality: a first step. [Google Scholar]
- 24.Ferraiolo D, Cugini J, Kuhn DR. Role-based access control (RBAC): Features and motivations. Proceedings of 11th annual computer security application conference. 1995 [Google Scholar]
- 25.Ferraiolo DF, Kuhn DR. Role-based access controls. arXiv preprint arXiv:09032171. 2009 [Google Scholar]