

ABSTRACT
Little data are available on the overall incidence and characteristics of herpes zoster (HZ) in China, thus a community-based retrospective survey was conducted during December 2012 to March 2013 to collect HZ incident data over the past year in selected districts of Beijing, China. A total of 237 incident HZ cases were identified from 118,220 residents and majority of HZ patients (219/237, 92.4%) sought healthcare. Annual HZ incident rates were 1.90/1000 after adjusted and higher among females (2.4/1000) than males (1.7/1000). HZ rates increased with age and with a sharply rise among those aged ≥50 years particular for female. 217 cases were available for interview with 193 (88.9%) primary, 24 (11.1%) recurrent and 10 (4.6%) postherpetic neuralgia (PHN) cases respectively. No difference was shown between the primary and recurrent HZ cases in sex (P = 0.42), age (P = 0.72), times of healthcare seeking (P = 0.45), number of dermatome (P = 0.72), pain degree (P = 0.54), and hospitalization (P = 1.0). According to the survey, it can be speculated that disease burden of HZ is serious and caused at least 2.77 million cases annually in China. The recurrent HZ cases has similar characteristics to primary HZ cases. High proportion of healthcare seeking reminds that HIS records would be a feasible source for HZ surveillance to evaluate the trends and changes in China.
KEY WORDS: herpes zoster, incidence, postherpetic neuralgia, recurrent HZ
Highlights
The incidence of HZ of the whole population in China is reported for the first time and was 1.90/1000 person years which means at least 2.77 million cases in the China annually.
The HZ disease primarily attack age group is older than 50 years especially in females, the disease severities were similar between primary and recurrent HZ.
High proportion of healthcare seeking reminds that HIS records would be a feasible source for HZ surveillance to evaluate the trends and changes in China.
Introduction
Herpes zoster (HZ) is caused by reactivation of latent varicella-zoster virus (VZV) which was acquired from primary infection (varicella) and characterized as unilateral rash generally limited to single dermatome.1 Though the rash usually heals within two to four weeks, the complications from HZ can occur and the most common complication of HZ is postherpetic neuralgia (PHN). One third of individuals would develop HZ in their lifetime2" and 10% of them would develop PHN which defined as at least 90 days documented pain.3 HZ is reported to be higher among elders and females with racial differences globally.4-6 A few studies reported the incidence of HZ in regions of China among population aged≧50 years old recently,7,8 the disease burden and epidemic characteristic of the whole population are still not been reported. Shingles vaccine has not yet been licensed in China with the possibility of being introduced in the coming years, meanwhile varicella vaccine has already become available for decades and the coverage was pretty high in economically prosperous areas such as Beijing9 which may have had an impact on the incidence of HZ. Thus we conducted an a community-based retrospective survey to obtain the HZ incidence and epidemiological characteristics of the whole population of Beijing City in China.
Results
A total of 118220 residents were interviewed with little more males (52.8%, 62391/118220) than females (47.2%, 55829/118220). The age distribution of the subjects under study was 8.4%, 26.0%, 16.6%, 18.6%, 15.4%, 8.0%, 6.9% for those aged ≤14 years, 15–29 years, 30–39 years, 40–49 years,50-59 years,60-69 years, and ≥70 years old, respectively. Majority were local residents (70.9%, 83799/118220) with 29.1% (34400/118220) were migrants who were younger than the local residents (15-29 years: 46.9% vs. 17.5%, P < 0.0001) and higher proportion of male (male: 59.1% vs. 50.2%, P < 0.0001).
There were 237 incident HZ cases identified in the investigation of which 219 (92.4%) were diagnosed by healthcare and 18(7.6%) were self-diagnosis. The overall anual HZ incidence was 2.0/1000(237/118220) and 1.9/1000 after age- and sex- adjusted. Females have higher incidence than males (2.4/1000 vs. 1.7/1000, P = 0.009). The HZ incidence increased along with age, with a sharp rise among those aged ≥50 years than those aged <50 years (4.7 /1000 vs. 1.1/1000, P < 0.001). The peak point of incidence rate is 6.3/1000 person years at 60–69 years age group. The trend of increased HZ incidence with age was consistent in males and females, but the sharp increase in those aged ≥50 years was more prominent in females (Figure 1).
Figure 1.
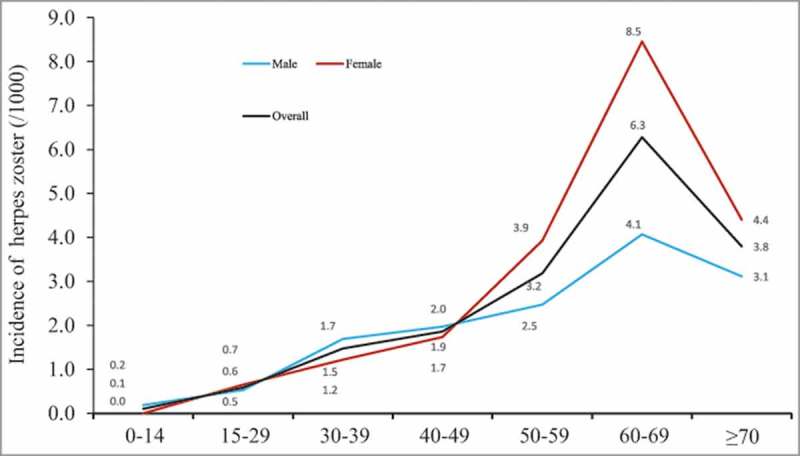
Incidence of herpes zoster by age and sex, Beijing, China.
Among 217 incident cases available for face-to-face interview, 193 cases (88.9%) were primary HZ, and 24 cases (11.1%) were recurrent HZ. Among 200 cases (92.2%, 200/217) seeking healthcare service, majority of them (158, 79.0%) sought healthcare once, and 21.0% (42/200) had doctor visit ≥2 times. 89.9% (195/217) of the cases had one dermatome affected, and 69.6% (151/217) of the cases suffered moderate /severe pain. Only 5 patients were hospitalized accounted for 2.3%. The statistic shows no difference between the primary and recurrent HZ cases in sex (P = 0.42), age (P = 0.72), times of healthcare seeking (P = 0.45), number of dermatome (P = 0.72), pain degree (P = 0.54), and hospitalization (P = 1.0) (Table 1).
Table 1.
The sociodemographic factors and disease severity between primary and recurrent herpes zoster.
| Total (%) | Primary case (%) | Recurrent case (%) | ||
|---|---|---|---|---|
| N = 217 | N = 193 | N = 24 | P value | |
| Sex | 0.42 | |||
| male | 98 (45.2) | 89(46.1) | 9(37.5) | |
| female | 119 (54.8) | 104(53.9) | 15(62.5) | |
| Age | 0.72 | |||
| <50y | 83 (38.2) | 73(37.8) | 10(41.7) | |
| ≥50y | 134 (61.8) | 120(62.2) | 14(58.3) | |
| Residency | 0.01 | |||
| local residence | 192 (88.5) | 175(90.7) | 17(70.8) | |
| migrant | 25 (11.5) | 18(9.3) | 7(29.2) | |
| Times of Healthcare seeking | 0.45 | |||
| 0 | 17 (7.8) | 15 (7.8) | 2 (8.3) | |
| 1 | 158 (72.8) | 139 (72.0) | 19 (79.2) | |
| ≥2 | 42 (19.4) | 39 (20.2) | 3 (12.5) | |
| Number of dermatome affected | 0.72 | |||
| 1 | 195 (89.9) | 174(90.2) | 21(87.5) | |
| ≥2 | 22 (10.1) | 19(9.8) | 3(12.5) | |
| Pain degree | ||||
| moderate/severe | 151 (69.6) | 133(68.9) | 18(75.0) | 0.54 |
| Mild or no pain | 66 (30.4) | 60(31.1) | 6(25.0) | |
| Hospitalization | 1.0 | |||
| Yes | 5(2.3) | 5(2.6) | 0(0) | |
| No | 212(97.7) | 188(97.4) | 24(100.0) |
There were 10 (4.6%) cases developed PHN. Majority of them (80.0%, 8/10) are older than 50 years, sought healthcare ≥ 2 times, and suffered moderate/severe pain (90.0%, 9/10). There was no significant difference between HZ with PHN and without PHN in number of dermatome, and hospitalization (P = 0.72, 1.0, respectively) (Table 2). HZ with PHN were more likely to have severe pain (90.0% vs. 29.5%, P < 0.001) and more likely to have sought healthcare ≥2 times than those without PHN (P = 0.001).
Table 2.
The sociodemagraphic factors and disease severity between Herpes Zoster with and without PHN.
| With PHN (%) | Without PHN (%) | ||
|---|---|---|---|
| N = 10 | N = 207 | P value | |
| Times of Healthcare seeking | 0.001 | ||
| 0 | 0(0) | 17(8.2) | |
| 1 | 3(30.0) | 144(69.6) | |
| ≥2 | 7(70.0) | 46(22.2) | |
| Number of dermatome affected | 0.07 | ||
| 1 | 7(70.0) | 188(90.8) | |
| ≥2 | 3(30.0) | 19(9.2) | |
| Pain degree | 0.29 | ||
| moderate/severe | 9(90.0) | 142(68.6) | |
| Mild or no pain | 1(10.0) | 65(31.4) | |
| Hospitalization | 0.21 | ||
| Yes | 1(10.0) | 4(1.9) | |
| No | 9(90.0) | 203(98.1) |
Discussion
Compared with previous studies,7-8 our study firstly reported HZ incidence of whole population in mainland China region by a community-based retrospective survey. The incidence of HZ of all ages and sexes was firstly described. Moreover, the rate of healthcare seeking, as well as the characteristics of primary and recurrent, non PHN and PHN cases were further described and compared.
Our study shows nearly two-thirds of the patients (61.8%) are older than 50 years old. Similar incidence trends by age and sex could be found in studies from other countries.3-6 The adjusted overall incidence rate of our study is lower compared with a systematic review which present the incidence of HZ in multiple countries or regions.10 Most of the studies adopted retrospective survey and usually acquired information from insurance data or electronic medical records or administrative data, and case ascertainment were from screening medical records by ICD code, or a few applied with prospective survey method. Different study design and case ascertainment may cause difference on incidence estimation. However, since China is not yet able to use medical insurance data as a developed country, a retrospective survey could be a feasible method, even if it may have methodological imperfection.
We compared with previous studies from China mainland merely reported incidence of elders aged≥50 years, one reported that the incidence was 3.4-5.5/1000 in Guangdong province7" and another was 3.43/1000 in selected districts of several provinces,8 which are similar to our study (4.7/1000). Compared with other countries or regions,10 it was found that the most of the age group in our study had a comparable or slightly lower incidence, as particularly in 50–59 and 60–69 age group. However, the incidence of 0–19 and 70- age group were significantly lower than other countries or regions. It is presumed that this two age group's information were often provided by guardian or caretaker in household survey, which may cause the reporting bias to underestimate the incidence.
It has been confirmed that the risk of HZ is associated with age and sex, however, there is no sufficient epidemiological evidence to support this association with recurrent HZ. Similar to our research, it have found the trend of increased HZ incidence with age, particularly the sharp increase in those aged ≥50 years was more prominent in females, but for recurrent HZ, this association is not obvious.11 Our study found that the recurrent HZ cases has similar characteristics to primary HZ cases. By now there has not been reported PHN incidence in China, the risk of PHN in HZ patients of our study (4.6%) is lower than some other studies which also use the same definition. All these studies results were varied from 10% to 30.0% with different study designs.10 It is generally believed that the occurrence of PHN is related to age and sex,12 our study did not find this might be due to small number of PHN cases.
Taking into account the huge population, the disease burden of HZ in China will be massive using our data to speculate. According to the Beijing city13 and China population census14 in 2014, there could be at least 0.055 million cases in Beijing city and 2.77 million cases in the whole China annually. Chinese government should begin to pay attention on the prevention and control of HZ, and take action to work on related research and evaluation early, such as establishing monitoring system and supporting HZ vaccine developing or introducing.
The healthcare utilization patterns related study of HZ patients is rare in China. In our study, vast majority patients seek healthcare at least once (92.2%). The high level of proportion prompts that using medical records is a good source to surveillance HZ for the trend changing, which would be a cost-effective, time-saving monitoring method compared with the field investigation in communities. This monitoring method is particularly suitable for regions has commendable HIS in public medical institutions such as Beijing.
Several limitations should be considered in interpretation the results in current study. There may be recall bias in retrospective survey which may underestimate the overall incidence. The information of Children, adolescents and elders aged≥70 years were probably provided by guardian or caretaker may cause the reporting bias to underestimate the incidence of these age groups. Less patients may conceal their illnesses because of privacy protection, which may lead to an little underestimated incidence. Medical records have the most reliable information, but it is very time-consuming to review it.
In summary, we found HZ is a serious disease burden in China before the introduction of herpes zoster vaccine, which may cause at least 2.77 million cases annually and was more severe in the elderly older than 50 years. The survey also found that the recurrent HZ cases has similar characteristics to primary HZ. High proportion of healthcare seeking and multiple times for healthcare seeking in HZ cases remind that, HIS records would be a feasible source for HZ surveillance to evaluate the trends and changes in China.
Material and method
This investigation has been authorized by the ethics committee of Beijing CDC. From December 2012 to March 2013, a community-based retrospective survey was launched in three districts of Beijing (Xicheng, Changping, and Miyun, respectively) with a two-step sampling algorithm to select eight cities first, and one/community per city in the 2nd step. The 3 districts selected were located in the urban, suburb, rural regions of Beijing. In each district, all cities/towns was categorized according to varicella incidence of past five years into three groups (high, medium, and low), with a similar number of cities/towns falling within each group. One city/town was randomly sampled from each group and a total of nine cities/towns were brought in, and eight agreed to participate. Within each city/town, one community/village was randomly selected. All residents who had lived in the selected community/village for at least six months during December 1, 2011 to November 30, 2012 were eligible to be study participants and were interviewed until the target of 15,000 participants per community/village was reached. The adjacent community/village would be enrolled if the first selected community/village had failed to reach the target participants. A total of 52 communities / villages were investigated from the cities/towns included.
A Herpes zoster incident case was defined as 1) a diagnosis of HZ by a medical provider, medical record is not necessary; 2) the onset date is between December 1 2011 and November 30, 2012; 3) if care was not sought, self-diagnosis of HZ based on the presence of cluster blisters one dermatome with pain, itch. A HZ primary case was defined as it is the first time of suffering the disease. A HZ recurrent case was defined as suffered more than once before the investigation time. PHN was defined as pain persisting 90 days or more after HZ rash healed.3
The trained investigators filled in socio-demographic information for all the members by a standard questionnaire through main family after entering house, then through face-to-face or telephone to contact each family member to ascertain them suffer from an HZ. For the ascertained cases, a face-to-face interview was conducted after getting the consent letter. The detail characteristics were collected such as time onset, dermatome involved, pain degree, healthcare seeking, hospitalization, and so on.
The overall incidence and incidences by sociodemographic factors were calculated as the proportion of the number of HZ cases over the number of study participants wherever appropriate. Overall incidence was age- and sex- adjusted to the 2013 Beijing city population. Comparisons of characteristics between cases of primary HZ and recurrent HZ, and between cases with and without PHN were performed by Pearson Chi-square test or Fisher exact test with SPSS version 19.0 (Chicago, IL).
Funding Statement
The study was supported and completed by the work budget of Beijing CDC. No funds were received for field investigation, the data analysis, interpretation, or writing manuscript from other agency.
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Acknowledgments
We thank the participants of our study and are indebted to the staff of Xicheng, Changping, and Miyun District CDCs for their coordination and field work and also highly appreciate the help from Dr. Chengbin Wang from Centers for Disease Control and Prevention, Atlanta, Georgia, USA.
References
- 1.Cohen JI. Herpes zoster. N Engl J Med. 2013;369(3):255–63. doi: 10.1056/NEJMcp1302674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Harpaz R, Ortega-Sanchez IR, Seward JF. Prevention of herpes zoster: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2008;57(RR-5):1–30. [PubMed] [Google Scholar]
- 3.Yawn BP, Saddier P, Wollan PC, St Sauver JL, Kurland MJ, Sy LS. A population-based study of the incidence and complication rates of herpes zoster before zoster vaccine introduction. Mayo Clin Proc. 2007;82(11):1341–9. [DOI] [PubMed] [Google Scholar]
- 4.Gauthier A, Breuer J, Carrington D, Martin M, Rémy V. Epidemiology and cost of herpes zoster and post-herpetic neuralgia in the United Kingdom. Epidemiol Infect. 2009;137(1):38–47. doi: 10.1017/S0950268808000678. [DOI] [PubMed] [Google Scholar]
- 5.Coplan P, Black S, Rojas C, Shinefield H, Ray P, Lewis E, Guess H. Incidence and hospitalization rates of varicella and herpes zoster before varicella vaccine introduction: a baseline assessment of the shifting epidemiology of varicella disease. Pediatr Infect Dis J. 2001;20(7):641–5. [DOI] [PubMed] [Google Scholar]
- 6.Gonzalez Chiappe S, Sarazin M, Turbelin C, Lasserre A, Pelat C, Bonmarin I, Chosidow O, Blanchon T, Hanslik T. Herpes zoster: burden of disease in France. Vaccine. 2010;28(50):7933–8. doi: 10.1016/j.vaccine.2010.09.074. [DOI] [PubMed] [Google Scholar]
- 7.Zhu Q, Zheng H, Qu H, Deng H, Zhang J, Ma W, Lin Y, Xie X, Qiu Q, Huang Z. Epidemiology of herpes zoster among adults aged 50 and above in Guangdong, China. Hum Vaccin Immunother. 2015;11(8):2113–8. doi: 10.1080/21645515.2015.1016672. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Li Y, An Z, Yin D, Liu Y, Huang Z, Xu J, Ma Y, Tu Q, Li Q, Wang H. Disease Burden Due to Herpes Zoster among Population Aged ≥50 Years Old in China: A Community Based Retrospective Survey. PLoS One. 2016;11(4):e0152660. doi: 10.1371/journal.pone.0152660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lu L, Wang C, Suo L, Li J, Liu W, Pang X, Seward JF. Varicella disease in beijing in the era of voluntary vaccination, 2007–2010. Pediatr Infect Dis J. 2013;32(8):e314–8. doi: 10.1097/INF.0b013e31828d948b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kawai K, Gebremeskel BG, Acosta CJ. Systematic review of incidence and complications of herpes zoster: towards a global perspective. BMJ Open. 2014;4(6):e004833. doi: 10.1136/bmjopen-2014-004833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Shiraki K, Toyama N, Daikoku T, Yajima M. Herpes zoster and recurrent herpes zoster. Open Forum Infect Dis. 2017;4(1):ofx007. doi: 10.1093/ofid/ofx007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Choo PW, Galil K, Donahue JG, Walker AM, Spiegelman D, Platt R. Risk factors for postherpetic neuralgia. Arch Intern Med. 1997;157(11):1217–24. [PubMed] [Google Scholar]
- 13.Beijing Municipal Bureau of Statistics NBS Survey in Beijing(2014) Available at:http://tjj.beijing.gov.cn/nj/main/2014_tjnj/index.htm
- 14.National Bureau of Statistics of the People's Republic of China China statistical yearbook(2015) Available at: http://data.stats.gov.cn/easyquery.htm?cn = C01