

Abstract
Rationale:
Urinary tract infections (UTIs) are common infectious diseases in women. The management of patients with UTI after menopause is commonly combined with antibiotics and external application of estrogen, which could also cause drug resistance and result in poor curative effect. This study reports a case of UTI with pain of episiotomy scar inflammation for 10 years, which was successfully cured under traditional Chinese medicine (TCM) and showed no recurrence for 5 years.
Patient concerns:
A female patient, aged 71 years, experienced UTIs with pain of episiotomy scar inflammation for 10 years. Under antibiotics and external application of estrogen therapy, the patient still had no significant curative effect. Therefore, he was admitted to treatment with TCM for complementary therapy.
Diagnosis:
UTIs with pain of episiotomy scar inflammation.
Interventions
: This patient was treated with Chinese herbal medicine (CHM) treatment 2 times a day for 1 year. After 1 month of CHM treatment, the patient could tolerate pain of episiotomy scar inflammation.
Outcomes:
After 2 months of CHM treatment, the follow-up urinalysis leukocyte, red blood cell, and pH showed great improvements in examination. Late follow-up was continued to November 2017, and the patient recovered stable condition without recurrence.
Lessons:
In this case, successful treatment by only applying the prescription of CHM is achieved in 1 elderly woman with UTI and pain of episiotomy scar inflammation in 1 year. It is suggested that the CHM formula has a potential effect on UTI and pain from episiotomy scar inflammation when usage of antibiotics and hormones meets with poor response.
Keywords: Chinese herbal medicine, episiotomy scar, geriatrics, urinary tract infections
1. Introduction
Urinary tract infections (UTIs) are common infectious diseases in women. In elderly women, the decrease of estrogen level after menopause may induce the weakened protective effect of urinary tract, and the increased possibility of recurrent infection accordingly.[1] UTIs are common in postmenopausal women that occupies 30% of the incidence of UTI, and 15% of the patients had recurrent symptoms of infection.[2,3] After menopause, the level of estrogen in women is reduced, accompanied by thinned urinary tract mucosa, decreased local antibacterial ability, and increased pH value in the vagina, which leads to the disorder of vaginal flora, so postmenopausal women are prone to develop UTI.[4,5] The management of UTI is commonly combined with antibiotics and external application of estrogen.[6,7] But the abidingly usage of antibiotics and estrogen replacement therapy could also cause drug resistance, resulting in poor curative effect.
Here we reported a case of UTI with pain of episiotomy scar inflammation, treated with traditional Chinese medicine (TCM). The patient had no response to antibiotics, laser excision, and physiotherapy in the early stages. The case was successfully cured under TCM and showed no recurrence for 5 years.
2. Case report
A female patient, aged 71 years, was admitted to the Department of TCM in General Hospital of the PLA due to frequent urination and odynuria over 10 years on December 7, 2011. Since the autumn of 2001, the patient complained of frequent urination with no obvious cause. The number of urination during the day was 3 to 4 times per hour (averaging 15–20 minutes), and up to 18 times at night, which had a great negative influence on the quality of sleep in the patient. Subsequently, the patient had odynuria and pain at the site of episiotomy scar. The patient visited the clinic of the work unit for intravenous injection of antibiotics drugs, without obvious effect. A few months later, the patient visited the Department of Urology in Beijing. A polyp was observed during urethra examination, which was then treated by laser excision. The symptoms were still not improved after several courses of physical therapy. In November 2002, an operation was carried out at the site of episiotomy scar, and it was found to be inflammation of muscle tissues at wound site after opening. The patient was given antibiotics and external application of estrogen postoperatively. One month after operation, the patient perceived aggravated pain and restless that affected physical activity. Consequently, the patient visited the Pain Department and was provided with acesodyne to relieve pain. However, the symptom of pain was still not totally relieved. Accordingly, the patient sought medical advices even from folk prescription for years, but was not cured. On September 30, 2011, the patient was admitted to the Department of Urology in Beijing. A routine urine test was performed, and white blood cells were found throughout the visual field under the microscope. Simultaneously the patient still took antibiotics and estrogen after the examination, but had no obvious curative effect for 3 to 4 months. On December 7, 2011, the patient sought TCM treatment in TCM Department of General Hospital of the PLA.
On TCM observation, the patient had burning pain in the urethra, lower abdominal pain, and occasional lumbago. Routine urine test was conducted and revealed that leukocytes were found throughout the visual field. Tongue diagnosis revealed pale red tongue, thick white tongue fur and pulse string. Diagnosis of TCM was Stranguria, deficiency of kidney Qi, and evil heat depressed internally. Rules of treatment: Invigorating Qi and tonifying the kidney, as well as clearing away damp-heat material. The Chinese medicines (Table 1) were decocted in water for oral dose, 1 dose each day and 2 times a day.
Table 1.
Ingredient and function of traditional Chinese herbal formulas.

After 1 month of Chinese herbal medicine (CHM) treatment, relevant symptoms were reduced gradually, and there was no obvious abnormality in routine urine test, but the patient still complained of pain in the urethra, urinary stammering and frequent urination. Tongue diagnosis was pink tongue, yellow coating of the tongue fur, and pulse string. Syndrome differentiation of TCM and rules of treatment were similar to those before. Prescription for promoting Qi circulation to relieve pain was added to the original prescription, with the addition of 15 g Corydalis Yanhusuo.
After that, the patient visited the outpatient department for re-examination every 2 weeks. Until in November 2012, the patient reported the disappearance of frequent urination and odynuria, and the condition remained stable except the occurrence of poor digestion. TCM syndrome differentiation indicated diet stagnation, indigestion, and anorexia. Therefore, 15 g processed Massa Medicata Fermentata and Endothelium Corneum Gigeriae Galli was supplemented in the original prescription. The series of urinalysis leukocyte, red blood cell, and pH before and after TCM treatment is summarized on Figure 1. The patient was ordered to pay attention to diet, regular daily life, and avoid anxiety. Late follow-up was continued to November 2017, and the patient recovered and was in stable condition without recurrence.
Figure 1.
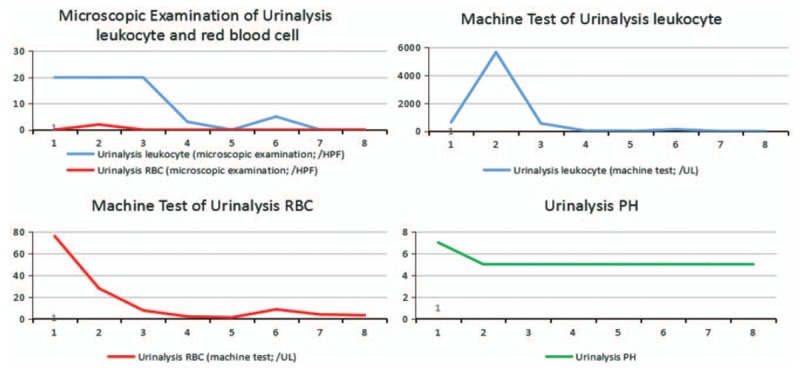
The series of urinalysis leukocyte, red blood cell, and pH before and after traditional Chinese medicine treatment. 1 represents 2011-9-30, 2 represents 2011-11-16, 3 represents 2011-12-7, 4 represents 2011-12-21, 5 represents 2012-1-4, 6 represents 2012-1-18, 7 represents 2012-2-8, and 8 represents 2015-7-30.
3. Discussion
It is quite rare regarding the successful treatment of patients with UTI with chief complaint of recurrent odynuria for 10 years by applying Chinese medicines for 2 years. The reported 71-year-old female patient suffered from UTI with symptoms of burning pain in episiotomy scar and urethra, frequent urination, and unobstructed urination between 2001 and 2011. The patient received antibiotics, laser ablation, physical therapy, and other methods, but clinical symptoms and laboratory indicators had not been significantly improved. In this regard, the patient chose TCM treatment and achieved satisfied curative effect. No recurrence occurred in the patient within 5 years of follow-up.
The UTI is mainly manifested as urgent urination, dysuria, and urination discomfort, which is commonly treated by antibiotics at present. However, antibiotic treatment alone often fails to achieve satisfactory results according to clinical observation. At the same time, with the extensive application of antibiotics, immunosuppressive agents, and hormones, the bacterial spectrum of pathogenic bacteria of UTI is gradually changing, and its drug resistance is also increasing.[8,9] Simultaneously, in the elderly women, the decreased estrogen level and reduced sugar content of the vaginal epithelium may contribute to the transformation of vaginal microflora from glycogen-dependent lactic acid bacteria to Escherichia coli, leading to the increase in potential risk of UTI.[10] In such way, the reduced bladder compliance, the decreased detrusor contractility and residual urine in the bladder >10 mL are beneficial to the growth and reproduction of bacteria. With respect to the above, these physiologic changes may lead to an upward trend in the incidence of UTI in elderly women with age.[11]
The CHMs are a major complementary medicine treatment for UTIs in China, which could regulate the increase of renal blood flow, improve the glomerular filtration rate, increase urine output, promote bacterial excretion in urinary tract, and improve the blood circulation in the inflammatory region of the urinary tract.[12] And under estrogen-like effects, epithelial cells of the vaginal mucosa secrete glycogen, which is converted into lactic acid by Lactobacillus and prevents the growth of other bacteria.
In accordance with the above characteristics, TCM theory holds the opinion that the TCM syndrome differentiation of UTI is not only predominated by damp-heat syndrome, but also has the syndrome of kidney deficiency. Therefore, treatment rules of invigorating Qi and tonifying the kidney, as well as clearing away damp-heat material were put forward in our study. The therapy and prescription had been applied to those elderly women with UTI for a long period of time and had achieved remarkable results.[13]
In the prescription, Astragalus Membranaceus, Chinese Yam, Dipsacaceae, and Achyranthes Bidentata could exert roles of invigorating the kidney and replenishing Qi, which might result in the securing and containing of the body fluid, thereby achieving radical results. Processed Radix Aconiti Lateralis and Lindera Strychnifolia could contribute to warmly invigorating kidney yang, promoting Qi circulation to relieve pain. Flos Lonicerae and Forsythia Suspensa could clear away damp-heat material to scavenge the residual heat of the bladder. In addition, Sargentodoxa Cuneata, Patrinia Scabiosaefolia, and Lophantherum Gracilewere conducive to inducing diuresis for treating strangurtia, thereby relieving burning pain in urethra.
Previous evidence has demonstrated that medicine of tonifying the kidney and replenishing Qi can improve the immunity and other functions, and can effectively improve the symptoms of UTI in the elderly by adjusting the hormone level in the body.[12,13] According to pharmacologic effects, Radix Aconiti Lateralis, Dipsacaceae, and Achyranthes Bidentata play a hormone-like role. While Astragalus Membranaceus, Lindera Strychnifolia, Chinese Yam, Flos Lonicerae, and Forsythia Suspensa could effectively inhibit the inflammation of the urethra.
Radix Aconiti Lateralis has immunomodulatory properties, which plays an important role in the anti-inflammatory process and inhibits the development of major symptoms such as inflammation, inflammatory exudation, pain, and fever.[14] Recent studies found that aconitine significantly decreased PGE2, interleukin (IL)-17a, IL-6, and the elevated blood leukocyte counts in mice with systemic lupus erythematosus.[15] Achyranthes Bidentata possesses anti-inflammatory properties, Achyranthes bidentate saponins. The saponins are the main bioactive principles that produce protective effects on inflammation, and the therapeutic effect relies on suppressed IL-1β-induced apoptosis by suppressing the activation of caspase-3, inhibiting levels of proapoptotic proteins Bax and Bad, decreasing p53 protein phosphorylation, and promoting the expression of antiapoptotic protein Bcl-xL and inhibit IL-1β-induced nuclear factor κB activation.[16] Chinese Yam has estrogen-like effects, with 2 main compounds, adenosine and arbutin. The estrogen-like effects of Chinese Yam was mainly mediated by the estrogen receptors ERα, ERβ, and GPR30, while the adenosine effects was mainly mediated by estrogen receptors ERβ and GPR30.[17] And evidence showed that Flos Lonicerae extract (FLE) significantly suppressed the production of NO, PGE2, and tumor necrosis factor-α (TNF-α) in the culture medium as well as the expression of iNOS and COX-2 by lipopolysaccharide (LPS)-stimulated RAW264.7 cells in a dose-dependent fashion, which suggests that FLE attenuates the degree of inflammation by inhibiting the nuclear factor-κB (NF-κB)-dependent signaling pathway and the subsequent production of proinflammatory mediators.[18] Forsythia Suspensa also could inhibit LPS-induced inflammatory responses in BV2 microglia cells and primary microglia cells through inhibition of NF-κB activation and activation of Nrf2/HO-1 signaling pathway.[19] An experiment of Patrinia Scabiosaefolia on pelvic inflammation rats showed that the serum levels of IL-6, IL-8, and TNF-α in PV and DEX group were all significantly lower than those of the CON group, and the serum levels of IL-6 and IL-8 in PV group were significantly lower than those of the DEX group. Thus Patrinia Scabiosaefolia possesses strong anti-inflammatory and anti-nociceptive effects on pelvic inflammation and the pain associated.[20]
The treatment principles remained unchanged while prescriptions were adjusted slightly according to patient's conditions changes in this case. After 11 months of treatment, the patient returned to hospital on November 7, 2011, without frequent micturition and odynuria disappeared. During the follow-up period, the patient's condition was stable. Nevertheless the study of this UTI with pain of episiotomy scar inflammation case is inseparable from the patient's high degree of cooperation.
4. Conclusion
Successful treatment by only applying the prescription of CHM is achieved in the geriatric woman with UTI and pain of episiotomy scar inflammation in 1 year. Though direct mechanism of CHM remains unidentified in this disease, the authors believe that potential effect of TCM therapy, tonifying the kidney, and replenishing Qi as well as clearing away damp-heat material, has played a role in the treatment of UTI. When usage of antibiotics and hormones meets with poor response, Chinese herbal formula may be an alternative choice in such diseases.
Author contributions
Conceptualization: Zhan-Qi Tong.
Data curation: Zhan-Qi Tong.
Formal analysis: Zhan-Qi Tong.
Funding acquisition: Zhan-Qi Tong.
Investigation: Chen Zhang.
Methodology: Chen Zhang, Zhan-Qi Tong.
Resources: Mingjun Chen.
Software: Mingjun Chen.
Supervision: Zhan-Qi Tong.
Validation: Zhan-Qi Tong.
Visualization: Zhan-Qi Tong.
Writing – original draft: Mingjun Chen.
Writing – review & editing: Chen Zhang, Zhan-Qi Tong.
Footnotes
Abbreviations: CHM = Chinese herbal medicine, FLE = Flos Lonicerae extract, TCM = traditional Chinese medicine, UTIs = urinary tract infections.
CZ and MJC contributed equally to this work.
The patient has provided written informed consent for the publication of the case and any accompanying images. The ethics committee of Chinese People Liberation Army General Hospital has approved the study.
The authors have no funding and conflicts of interest to disclose.
References
- [1].Salvatore S, Salvatore S, Cattoni E, et al. Urinary tract infections in women. Eur J Obstetr Gynecol Reprod Biol 2011;156:131–6. [DOI] [PubMed] [Google Scholar]
- [2].Setty P, Rekedal L, Warren M. Vaginal estrogen use and effects on quality of life and urogenital morbidity in postmenopausal women after publication of the Women's Health Initiative in New York City. Menopause-the Journal of the North American Menopause Society 2016;23:474. [DOI] [PubMed] [Google Scholar]
- [3].Stamm WE, Hooton TM. Management of urinary tract infections in adults. N Engl J Med 2004;14:1328–34. [DOI] [PubMed] [Google Scholar]
- [4].Raz R, Gennesin Y, Wasser J, et al. Recurrent urinary tract infections in postmenopausal women. Clin Infect Dis 2000;30:152–6. [DOI] [PubMed] [Google Scholar]
- [5].Robinson D, Cardozo L. Estrogens and the lower urinary tract. Neurourol Urodyn 2011;30:754–7. [DOI] [PubMed] [Google Scholar]
- [6].Raz R. Hormone replacement therapy or prophylaxis in postmenopausal women with recurrent urinary tract infection. J Infect Dis 2001;183:74. [DOI] [PubMed] [Google Scholar]
- [7].Robinson D, Toozshobson P, Cardozo L. The effect of hormones on the lower urinary tract. Menopause Int 2013;19:155–62. [DOI] [PubMed] [Google Scholar]
- [8].Torella M, Del DF, Grimaldi A, et al. Efficacy of an orally administered combination of hyaluronic acid, chondroitin sulfate, curcumin and quercetin for the prevention of recurrent urinary tract infections in postmenopausal women. Eur J Obstet Gynecol Reprod Biol 2016;207:125–8. [DOI] [PubMed] [Google Scholar]
- [9].Arnold JJ, Hehn LE, Klein DA. Common questions about recurrent urinary tract infections in women. Am Fam Phys 2016;93:560–9. [PubMed] [Google Scholar]
- [10].Stamm WE, Hooton TM. Management of urinary tract infections in adults. N Engl J Med 1993;329:1328–34. [DOI] [PubMed] [Google Scholar]
- [11].Robinson D, Giarenis I, Cardozo L. The management of urinary tract infections in octogenarian women. J Sci Maturitas 2015;81:343–7. [DOI] [PubMed] [Google Scholar]
- [12].Zhang N, Huang L, Liu S, et al. Traditional Chinese medicine: an alternative treatment option for refractory recurrent urinary tract infections. Clin Infect Dis 2013;56:1355. [DOI] [PubMed] [Google Scholar]
- [13].Jiang J. Reflections on clinical practice of traditional Chinese medicine through treatment of individual cases of urinary tract infection [in Chinese]. J Chin Integrat Med 2008;6:1217–20. [DOI] [PubMed] [Google Scholar]
- [14].Nesterova LV. Evaluation of anti-inflammatory activity of extracts from Siberian plants. Vestn Ross Akad Med Nauk 2009;11:30–4. [PubMed] [Google Scholar]
- [15].Li X, Gu L, Yang L, et al. Aconitine: a potential novel treatment for systemic lupus erythematosus. J Pharmacol Sci 2017;133:115–21. [DOI] [PubMed] [Google Scholar]
- [16].Xu XX, Zhang XH, Diao Y, et al. Achyranthes bidentate saponins protect rat articular chondrocytes against interleukin-1(-induced inflammation and apoptosis in vitro. Kaohsiung J Med Sci 2017;33:62–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Zeng M, Zhang L, Li M, et al. Estrogenic effects of the extracts from the Chinese Yam (Dioscorea opposite Thunb.) and its effective compounds in vitro and in vivo. Molecules 2018;23:E11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Jin XH, Ohgami K, Shiratori K, et al. Effects of blue honeysuckle (Lonicera caerulea L.) extract on lipopolysaccharide-induced inflammation in vitro and in vivo. Exp Eye Res 2006;82:860–7. [DOI] [PubMed] [Google Scholar]
- [19].Wang Y, Zhao H, Lin C, et al. Forsythiaside a exhibits anti-inflammatory effects in LPS-stimulated BV2 microglia cells through activation of Nrf2/HO-1 signaling pathway. Neurochem Res 2016;41:659–65. [DOI] [PubMed] [Google Scholar]
- [20].Zheng Y, Jin Y, Zhu HB, et al. The anti-inflammatory and anti-nociceptive activities of Patrinia villosa and its mechanism on the proinflammatory cytokines of rats with pelvic inflammation. Afr J Tradit Complement Altern Med 2012;9:295–302. [DOI] [PMC free article] [PubMed] [Google Scholar]