

Abstract
Diabetes mellitus is currently a major public health problem. A common complication of diabetes is cardiac dysfunction, which is recognized as a microvascular disease that leads to morbidity and mortality in diabetic patients. While ischemic events are commonly observed in diabetic patients, the risk for developing heart failure is also increased, independent of the severity of coronary artery disease and hypertension. This diabetes-associated clinical entity is considered a distinct disease process referred to as “diabetic cardiomyopathy”. However, it is not clear how diabetes promotes cardiac dysfunction. Vascular endothelial dysfunction is thought to be one of the key risk factors. The impact of diabetes on the endothelium involves several alterations, including hyperglycemia, fatty acid oxidation, reduced nitric oxide (NO), oxidative stress, inflammatory activation, and altered barrier function. The current review provides an update on mechanisms that specifically target endothelial dysfunction, which may lead to diabetic cardiomyopathy.
Keywords: cardiomyopathy, diabetes, diabetic cardiovascular complications, endothelium, vascular, heart failure, metabolism
Introduction
Cardiovascular disease is a major cause of morbidity and mortality in diabetic patients. It has long been established that diabetes significantly increases the risk of cardiovascular disease, with diabetic men being two times more likely to suffer from congestive heart failure (CHF) than non-diabetic individuals and diabetic women being five times more likely to develop CHF [1, 2]. In fact, 68% of deaths in type 2 diabetic patients are caused by cardiac complications [3–6]. Interestingly, a subset of diabetic patients develops left ventricular dysfunction in the absence of coronary artery disease, hypertension, or vascular disease. This observation, first made by Rubler et al. in 1972, is now known as diabetic cardiomyopathy [7]. Currently, diabetic cardiomyopathy is defined as ventricular dysfunction that occurs independently of hypertension or myocardial ischemia in diabetic patients. It is important to note, however, that diabetic cardiomyopathy rarely exists without these features and that the presence of these comorbidities does play a role in enhancing the complications associated with the disease.
While diabetic cardiomyopathy is now recognized as a clinically distinct entity, the mechanisms underlying its pathogenesis are still poorly understood. In this review, we will look at evidence regarding how diabetes-induced endothelial dysfunction mediates cardiac dysfunction. Specifically, we will focus on the hyperglycemia-induced changes that occur in the vascular endothelium during diabetes and how these changes may contribute to the development of diabetic cardiomyopathy. Several potential mechanisms that have been implicated in endothelial dysfunction in diabetic cardiomyopathy will be discussed.
Clinical manifestations of diabetic cardiomyopathy
Diabetic cardiomyopathy affects both type 1 and type 2 diabetic patients and is characterized by a variety of functional and structural changes in the heart. In early stages of the disease, left ventricular diastolic dysfunction (LVDD) is the most prevalent cardiac complication [8, 9]. Although previous reports using Doppler echocardiography have estimated that LVDD affects ~40%–64% of asymptomatic diabetic patients [10], the emergence of more direct and accurate measurements of diastolic function, such as color M-mode and Doppler tissue imaging, have caused these estimates to rise to as high as 75% [11]. Systolic dysfunction is another characteristic of diabetic cardiomyopathy, although it usually develops during the later stages of the disease after diastolic dysfunction has been established [1, 12]. The development of both diastolic and systolic dysfunction in diabetics can be explained by hyperglycemia and hyperinsulinemia rather than by obesity, high blood pressure, or coronary artery disease [13].
Diabetic cardiomyopathy is also associated with left ventricular hypertrophy [14], independent of coronary artery disease [15]. Hypertrophy only seems to be observed in patients with diabetes, not in patients with impaired fasting glucose or impaired glucose tolerance, suggesting that it is a consequence of long-term diabetic effects [16]. In addition, diabetic cardiomyopathy is characterized by an increase in both perivascular and interstitial fibrosis [17–19].
Potential mechanisms underlying diabetic cardiomyopathy
The development of diabetic cardiomyopathy is likely to be multifactorial. Several pathways have been implicated, including vascular endothelial dysfunction, glucose toxicity, mitochondrial dysfunction, and lipotoxicity [20]. It is difficult to determine how each of these factors individually contributes to cardiac dysfunction in diabetic patients. However, involvement of the vascular endothelium is becoming a front-runner in the pathogenesis of this disease. Hyperglycemia, a hallmark of diabetes, has been identified as one of the key causes of endothelial dysfunction in both type 1 and type 2 diabetes [21, 22]. High glucose levels lead to multiple biochemical modifications in endothelial cells and myocytes. These modifications include enhanced non-enzymatic glycation, sorbitol-myo-inositol-mediated changes, redox potential alterations, and the activation of protein kinase C (PKC) [23]. Hyperglycemia also causes an increase in reactive oxygen species (ROS) in endothelial cells, overwhelming the cell’s ability to overcome oxidative stress [24, 25]. In the following section, we will discuss the effects of diabetes on the vascular endothelium and how they may potentially play a role in the development of diabetic cardiomyopathy.
Mechanisms of endothelial dysfunction in diabetic cardiomyopathy
Normal endothelial cell metabolism
Under healthy conditions, endothelial cells are quiescent and play a role in maintaining vascular homeostasis. Endothelial cell metabolism is shown in Fig. 1. Glucose enters the cell through the GLUT-1 transporter, whose activity is predominantly regulated by extracellular glucose concentrations [26]. Glucose uptake through this receptor occurs in an insulin independent manner [27]. Consequently, endothelial cells are more susceptible to hyperglycemia-induced damage than other cell types.
Fig. 1.

Normal endothelial cell metabolism. In healthy endothelial cells, glucose enters the cell through the GLUT-1 receptor, in an insulin independent manner. Energy production occurs mostly by glycolysis, rather than through oxidative phosphorylation. During normal endothelial function, some of the glucose-6-phosphate that is produced during glycolysis gets shunted into the pentose phosphate pathway. The purpose of this pathway is to produce NADPH, an important antioxidant in endothelial cells, as well as pentoses, which can be used to produce nucleic acids, nucleotides, and amino acids. It also allows the conversion of glutathione disulfide (GSSG) back to glutathione (GSH), which helps to prevent oxidative stress by converting H2O2 to H2O
The generation of ATP in endothelial cells occurs primarily via the glycolytic pathway rather than through oxidative phosphorylation [28, 29]. During glycolysis, some glucose-6-phosphate (G-6-P) gets shunted into the pentose phosphate pathway, producing NADPH, an antioxidant found in endothelial cells, as well as pentoses, which can be used to make nucleic acids, nucleotides, and amino acids. This process also allows for the conversion of glutathione disulfide to glutathione, which helps prevent oxidative stress by converting H2O2 to H2O.
Fatty acid oxidation occurs in endothelial cells; however, it is unclear what role this oxidation plays since it seems to contribute very little to energy production in the endothelium [30, 31]. During periods of glucose deprivation, there is an increase in fatty acid oxidation, suggesting a degree of metabolic compensation [32]. Several theories have been proposed for the reason behind fatty acid oxidation in endothelial cells. Fatty acid oxidation is a source of NADPH that helps maintain the redox balance in endothelial cells. The oxidation of lipids may also play a role in regulating endothelial cell permeability [31]. Finally, fatty acid oxidation in endothelial cells may be important in the de novo synthesis of nucleotides by providing the carbon atoms necessary to build aspartate and glutamate [33].
Diabetes-induced changes in the glycolytic pathway
Metabolic changes associated with the diabetic myocardium have been extensively studied. Under hypoxic or inflammatory conditions, such as those that occur during diabetic cardiomyopathy, endothelial cells work to revascularize tissue to restore the delivery of oxygen and nutrients to damaged areas. Endothelial cells enhance their glycolytic flux even further during vessel sprouting, doubling their glycolytic rate during periods of proliferation or migration [34]. This enhancement allows the cells to migrate into hypoxic areas and proliferate where oxidative metabolism would be impaired. This alteration, in addition to enhanced glucose transportation due to the increase in GLUT-1 activity that occurs during diabetes, causes an increase in intracellular glucose concentrations in diabetic endothelial cells [35]. Endothelial cells address this excess glucose through several mechanisms.
Glucose can be shunted into the side branches of glycolysis, such as the hexosamine biosynthesis pathway, the pentose phosphate pathway, the polyol pathway, and the glycation pathway. The pentose phosphate pathway is a side pathway of glycolysis with two phases: the oxidative phase and the non-oxidative phase. Glucose enters the pentose phosphate pathway as G-6-P. During the oxidative phase, NADPH is produced, whereas during the non-oxidative phase, pentoses are produced. Under hyperglycemic conditions, entry of G-6-P into the pentose phosphate pathway is inhibited, which leads to reduced endothelial cell viability and migration [36]. In addition, inhibition of the pentose phosphate pathway leads to oxidative stress and endothelial dysfunction [37], whereas overexpression of G-6-P dehydrogenase, the first and rate-limiting enzyme of the pentose phosphate pathway, decreases endothelial oxidative stress [38]. The hexosamine biosynthesis pathway converts fructose-6-phosphate (a glycolytic intermediate) to uridine 5′-diphosphate N-acetylglucosamine (UDP-GlcNAc), which under normal conditions, is used for protein glycosylation. However, in diabetic endothelial cells, hyperglycemia-induced glycosylation inhibits endothelial nitric oxide synthase (eNOS) activation [39] and angiogenesis [40]. In the polyol pathway, aldose reductase converts glucose to sorbitol, using up NADPH. Sorbitol then gets converted to fructose and 3-deoxyglucosone, a precursor for the formation of advanced glycation end products (AGEs). Overproduction of AGEs, which occurs during diabetes, causes a variety of detrimental effects in endothelial cells by binding to the receptor for advanced glycation end products (RAGE), such as increasing endothelial cell permeability [41], inhibiting eNOS activity [42], impacting the coagulation system [43, 44], and activating both NADPH oxidase (NOX) and NF-kB [45, 46]. During the glycation pathway, glycolytic intermediates are converted to methylglyoxal, which modifies DNA and proteins. Upregulation of this pathway has been implicated in diabetic cardiomyopathy, leading to an inhibition of eNOS activity in endothelial cells [47, 48].
Hyperglycemia and vascular endothelial permeability
In diabetes, hyperglycemia is caused by reduced insulin levels and/or insulin resistance, leading to excessive levels of glucose circulating in the blood plasma. A blood sugar level with a consistent range between ~5.6 and 7 mmol/L is considered hyperglycemic, whereas a concentration above 11.1 mmol/L is considered diabetic. However, symptoms are usually not noticeable until blood sugars reach even higher levels of ~15–20 mmol/L. Interestingly, short-term hyperglycemia, caused by insulin discontinuation, is associated with an increase in myocardial systolic contractile function in type 2 diabetic patients with or without heart failure [49]. Chronic levels of blood glucose exceeding 7 mmol/L can lead to metabolic derangements in endothelial cells and induce organ damage, as shown in Fig. 2.
Fig. 2.

Hyperglycemia-induced metabolic derangement in endothelial cells. During diabetes, entry of glucose-6-phosphate into the pentose phosphate pathway is inhibited. This causes a reduction in the production of NADPH and a buildup of H2O2, which both contribute to oxidative stress in diabetic endothelial cells
Experimental evidence indicates that hyperglycemic conditions promote increased permeability of the endothelial cell layer in the myocardium while also decreasing capillary density [50]. A potential mechanism for this increased permeability during diabetes is activation of the diacylglycerol (DAG)-PKC signaling pathway [51, 52]. PKC is a family of serine-threonine kinases. The PKC superfamily can be classified into three subfamilies: classical PKC (cPKC; α, β1, β2, and γ), novel PKC (nPKC; δ, ε, η, θ, and μ), and atypical PKC (aPKC: ζ, λ/ι) [53]. The activation of cPKC and nPKC is DAG dependent, whereas the activation of aPKC is not DAG dependent [53]. DAG-dependent subfamilies cPKC and nPKC were previously reported to be associated with vascular permeability in diabetes [54]. Activation of this pathway may contribute to diabetic endothelial dysfunction by increasing endothelial cell permeability and leukocyte adhesion in several tissues, including the heart, retina, and kidney [51]. The mechanism by which PKC activation leads to increased endothelial cell permeability remains unclear. It has recently been shown in human umbilical vein endothelial cells (HUVECs) that hyperglycemia leads to the phosphorylation of myosin light chain (MLC) by PKC, which in turn causes VE-cadherin tyrosine phosphorylation and the disruption of adherens junctions [55]. Proteins associated with endothelial tight junctions include transmembrane, scaffolding, and signaling proteins [56]. In particular, the transmembrane proteins occludin, tricellulin, the claudin family, and junction adhesion molecules, along with the scaffolding zonula occludens proteins (ZO−1, −2, and −3), play major roles in the formation and regulation of tight junctions [57]. Hyperglycemia-mediated activation of PKC is implicated in the development of oxidative stress and is accompanied by an excessive release of free radicals, which promote endothelial barrier dysfunction in many vascular conditions, including diabetes and cerebral ischemia.
Diabetes-induced inhibition of nitric oxide
Another hallmark of endothelial dysfunction is a deficiency in the bioavailability of NO, along with a variety of other vasoactive factors produced by endothelial cells. Under healthy conditions, the endothelium releases vasodilators, such as NO, prostacyclin, and bradykinin, as well as vasoconstrictors, such as vasoconstrictor prostanoids, endothelin, and angiotensin-II. The balance between the release of vasoconstrictors and vasodilators by endothelial cells helps maintain coronary vascular structure. During diabetic cardiomyopathy, an imbalance between the release of constricting and relaxing factors occurs, as shown in Fig. 3. Diabetic conditions cause an upregulation of various vasoconstrictors. For example, an increase in endothelin production has been observed in the diabetic heart [58], which may lead to vessel hypertrophy and increased myocardial fibrosis, both characteristics of diabetic cardiomyopathy [59]. Importantly, vasoconstrictor prostanoids, including vasoconstrictor prostaglandin H2 (PGH2), thromboxane A2 (TXA2), and PGF2α, are also enhanced in diabetes. These products, in turn, upregulate NAPDH oxidase and type 4 and type 5 phosphodiesterases (PDE4 and PDE5), resulting in increased ROS production, degradation of cAMP and cGMP, and vasoconstriction [60, 61]. In addition, in diabetic endothelial cells, there is an impaired response of endothelial-dependent hyperpolarization (EDH) [62]. There are smaller arteries in which endothelium-mediated vasodilation is predominately affected by EDH in vascular smooth muscle cells. EDH causes the relaxation of vascular smooth muscle by hyperpolarizing its cell membrane and closing voltage-operated calcium channels, leading to a reduction in intracellular free calcium levels [63].
Fig. 3.
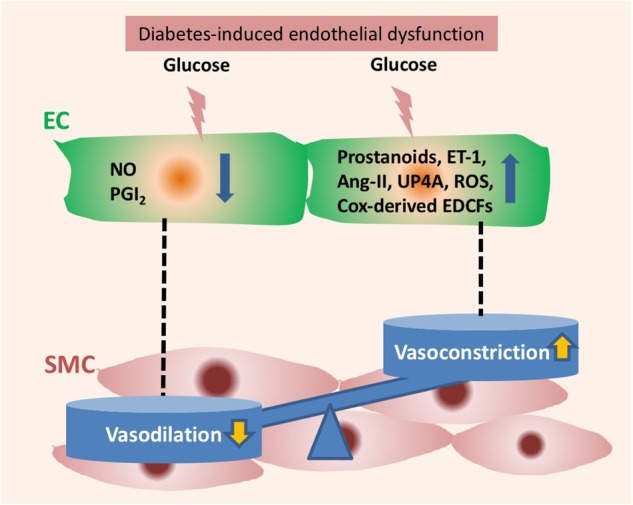
Effect of diabetic endothelial dysfunction on vasodilators and vasoconstrictors. Hyperglycemia in diabetes decreases vasodilation through the decreased bioavailability of nitric oxide (NO) and prostacyclin (PGI2). It also caused an increase in endothelium-derived contracting factors including prostanoids, endothelin-1 (ET-1), angiotensin-II (Ang-II), dinucleotide uridine adenosine tetraphosphate (UP4A), ROS, and cyclooxygenase (COX)-derived prostanoids. EC endothelial cell, SMC smooth muscle cell
A key vasoactive factor involved in endothelium-dependent relaxation is NO. In the presence of oxygen, NO is synthesized from L-arginine and NADPH in a reaction catalyzed by nitric oxide synthase (NOS). In diabetic vessels, however, this NO-dependent vasodilatory response is lost [64–66]. This deficiency may be caused by the inactivation of NO due to an increase in free radicals [67] rather than by the reduced activity or expression of eNOS [68, 69]. Treatment of HUVECs and rat heart endothelial cells with D-glucose leads to an increase in the generation of reactive oxygen intermediates (ROIs) [70]. In addition, there is an increase in mitochondrial ROS concentrations in coronary endothelial cells from diabetic rats [71]. Furthermore, endothelium-dependent vasodilation in diabetic rats can be restored by treatment with antioxidants [72], and treatment of aortas from STZ-induced diabetic rats and hamsters with superoxide dismutase (a specific scavenger of superoxide anions) enhances endothelium-dependent relaxation [73, 74]. This evidence suggests a role for antioxidants in enhancing cardiac function by preventing endothelial dysfunction in the presence of diabetes.
Several mechanisms have been proposed to explain how an increase in oxidative stress can lead to decreased NO availability in diabetic endothelial cells, such as reduced tetrahydrobiopterin (BH4) bioavailability (oxidation of BH4) and eNOS uncoupling [75]. NOX is an enzyme involved in endothelial cell signaling. It catalyzes the reduction of oxygen to superoxide anions (O2−) by using NADPH as an electron donor. During high glucose and insulin-resistant conditions, NOX activity, and thus, superoxide anion production, is increased [76–78]. Superoxide anions react with NO to form peroxynitrite (ONOO−). Peroxynitrite causes eNOS uncoupling, as described in Fig. 4. Peroxynitrite leads to the oxidation of BH4, a cofactor necessary for NOS activity [79, 80]. However, some evidence suggests that the depletion of BH4 is not the main cause of endothelial dysfunction in vivo during periods of oxidative stress [81]. Although it has been shown that BH4 supplementation is an effective treatment for suppressing superoxide anion production and improving vasodilation in the endothelium [82–85], many of these studies were done with concentrations of BH4 that are 100 times larger than physiological concentrations. Thus, other mechanisms have been proposed. For example, peroxynitrite may cause oxidation of the zinc-thiolate center of eNOS, resulting in eNOS uncoupling [86].
Fig. 4.

Mechanism of eNOS uncoupling. During diabetes, hyperglycemia activates NAD(P)H oxidase (NOX), which is responsible for converting oxygen into the superoxide anion (O2-), using up NADPH during the reaction. Superoxide reacts with NO to form peroxynitrite (ONOO-). Peroxynitrite is believed to be the main cause of eNOS uncoupling in endothelial cells. Under normal physiological conditions, NO is synthesized by eNOS from L-arginine and oxygen, using BH4 as a cofactor. During eNOS uncoupling, however, eNOS produces superoxide instead of NO, leading to oxidative stress in endothelial cells. It is thought that peroxynitrite reacts with BH4, and that this loss of BH4 is the main mechanism by which eNOS becomes uncoupled. However, more recent evidence suggests that other mechanisms may be involved
Other mechanisms are involved in NO-induced endothelial dysfunction in diabetes. An endogenous inhibitor of NO synthase, asymmetric dimethylarginine (ADMA), is found at elevated levels in patients with type 2 diabetes [87]. High glucose-induced impairment of dimethylarginine dimethylaminohydrolase (DDAH) activity causes ADMA accumulation and may contribute to a reduction in NO expression and endothelial vasodilator dysfunction in diabetes [88, 89]. The quenching of NO by AGEs in diabetes plays an important role in the development of vasodilatory impairment [90].
Mito-oxidative stress and mitochondrial dysfunction in diabetes
Plenty of evidence indicates that myocardial metabolism is altered in diabetes, which likely contributes to diabetic cardiomyopathy. The mitochondria are the center of metabolism and are thus likely to be impacted by impaired metabolism associated with diabetes. Oxidative stress occurs when there is an imbalance between the production of ROS, which include O2−, NO, the hydroxyl radical, hydrogen peroxide, and peroxynitrite, and the cell’s ability to detoxify reactive intermediates. Hyperglycemia mediates the induction of oxidative stress in the pathogenesis of diabetic complications, including diabetic cardiomyopathy [91]. For example, hyperglycemia leads to an increase in mitochondrial ROS in diabetic endothelial cells, which causes oxidative DNA damage. This damage activates the polyADP-ribose polymerase (PARP-1) pathway, as shown in Fig. 5, a pathway involved in DNA injury. Its activation stimulates the transfer of ADP-ribose units from NAD + to nuclear proteins, resulting in the depletion of NAD + and ATP from the cell. Inhibition of PARP-1 in endothelial cells may prevent endothelial dysfunction caused by diabetes [92]. Activation of PARP-1 also leads to the inhibition of glyceraldehyde-3-phosphate dehydrogenase (GAPDH) [93], causing the buildup of glycolytic intermediates. These intermediates get shunted into several different pathways, including the hexosamine biosynthesis pathway, the polyol pathway, and the glycation pathway, all of which are increased in hyperglycemic endothelial cells [93].
Fig. 5.

Effects of mitochondrial oxidative stress on endothelial function. During diabetes, there is an increase in mitochondrial oxidative stress, which causes mitochondrial DNA damage. This activates the PARP-1 pathway in the nucleus of endothelial cells, which has been implicated in response to DNA injury. Activation of PARP-1 has been shown to inhibit Glyceraldehyde-3-Phosphate Dehydrogenase (GAPDH), a key enzyme involved in glycolysis. This inhibition causes the buildup of glycolytic intermediates, which get shunted into the polyol pathway, the hexosamine biosynthesis pathway, or the glycation pathway. These pathways all contribute to endothelial dysfunction. Blue color represents nucleus and green represents the mitochondria
Sphingosine-1-phosphate (S1P), which binds to S1P receptors (S1PRs), also regulates an array of biological activities in endothelial cells. It has recently been demonstrated that high levels of glucose enhance ROS generation and markedly reduce NO in endothelial cells and that this effect is completely reversed by either induction of S1PR1 or reduction in S1PR2 [94]. This finding suggests that S1PR1 and S1PR2 play crucial roles in endothelial dysfunction caused by hyperglycemia-induced ROS production.
In addition, hyperglycemia-induced overproduction of mitochondrial ROS (mtROS) in cultured endothelial cells can be inhibited by AMPK activation [95], which seems to work through the upregulation of MnSOD (a mitochondrial specific antioxidant) [96] and UCP2 [97]. In patients with both coronary artery disease and type 2 diabetes, elevated mtROS levels in the endothelium led to an increase in AMPK activation, which supports a role for AMPK in protection against oxidative stress [98]. The upregulation of AMPK in the endothelium of diabetic mice may also prevent endothelial dysfunction [99]. Thus, AMPK may be a novel therapeutic target in the treatment of diabetes by improving blood glucose homeostasis, lipid profiles, and blood pressure [100]. Taken together, these findings suggest that ROS inhibition may provide beneficial effects in the prevention of diabetic cardiomyopathy.
There is also an imbalance between mitochondrial fission and fusion in diabetic endothelial cells, which may be related to increased oxidative stress. Mitochondrial fission is defined as the division of a mitochondrion into two separate mitochondria, leading to the elimination of damaged and dysfunctional mitochondria. Mitochondrial fusion is the merging of two or more mitochondria into one mitochondrion, which allows for the formation of a dynamic network that can respond to metabolic changes. This balance maintains normal mitochondrial function [101]. An imbalance between mitochondrial fission and fusion may contribute to the development of endothelial dysfunction in diabetes [102]. Exposure of endothelial cells to hyperglycemia leads to an increase in mitochondrial fission, which can be ameliorated by decreasing superoxide anion concentrations [103]. This fission may be caused by an increase in dynamin-related protein 1 (DRP1) expression, an activator of mitochondrial fission, or a decrease in optic atrophy 1 (OPA1), an activator of mitochondrial fusion [103]. Thus, mitochondrial dysfunction in endothelial cells represents a crucial step in the development of endothelial dysfunction.
Conclusion
Although diabetic cardiomyopathy is a complex disease with many possible causes, its underlying mechanisms are still not clear. Metabolic derangements in myocytes have been intensively studied. However, increasing evidence suggests that endothelial dysfunction may be one of the primary mechanisms involved in its pathogenesis. Hyperglycemic conditions in the diabetic heart lead to metabolic derangements and oxidative stress in cardiovascular endothelial cells, which cause multiple effects, such as increased permeability, impaired endothelial relaxation, and a decrease in NO availability. Therefore, endothelial cells represent a potential therapeutic target in the treatment of the disease. More work needs to be done to elucidate the most important pathways involved in the development of diabetic cardiomyopathy. However, studies looking at the prevention of hyperglycemia-induced endothelial dysfunction through BH4 or antioxidant supplementation show promising results. These findings suggest a significant role for endothelial cells in future diagnosis and treatment of the disease.
Acknowledgements
The expert scientific advice of Dr. James K. Liao from the University of Chicago is gratefully acknowledged. This work was supported by a Scientist Development Grant (3SDG17270046) from AHA (to Rongxue Wu) and a Pilot and Feasibility grant at the Chicago DRTC (P30 DK020595) (to Rongxue Wu).
Competing interests
The authors declare no competing interests.
References
- 1.Raev DC. Which left ventricular function is impaired earlier in the evolution of diabetic cardiomyopathy? An echocardiographic study of young type I diabetic patients. Diabetes Care. 1994;17:633–9. doi: 10.2337/diacare.17.7.633. [DOI] [PubMed] [Google Scholar]
- 2.Kannel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol. 1974;34:29–34. doi: 10.1016/0002-9149(74)90089-7. [DOI] [PubMed] [Google Scholar]
- 3.Echouffo-Tcheugui JB, Xu H, DeVore AD, Schulte PJ, Butler J, Yancy CW, et al. Temporal trends and factors associated with diabetes mellitus among patients hospitalized with heart failure: findings from get with The Guidelines-Heart Failure registry. Am Heart J. 2016;182:9–20. doi: 10.1016/j.ahj.2016.07.025. [DOI] [PubMed] [Google Scholar]
- 4.Shah AD, Langenberg C, Rapsomaniki E, Denaxas S, Pujades-Rodriguez M, Gale CP, et al. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1.9 million people. Lancet Diabetes Endocrinol. 2015;3:105–13. doi: 10.1016/S2213-8587(14)70219-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kho C, Lee A, Jeong D, Oh JG, Gorski PA, Fish K, et al. Small-molecule activation of SERCA2a SUMOylation for the treatment of heart failure. Nat Commun. 2015;6:7229. doi: 10.1038/ncomms8229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Severson DL. Diabetic cardiomyopathy: recent evidence from mouse models of type 1 and type 2 diabetes. Can J Physiol Pharmacol. 2004;82:813–23. doi: 10.1139/y04-065. [DOI] [PubMed] [Google Scholar]
- 7.Rubler S, Dlugash J, Yuceoglu YZ, Kumral T, Branwood AW, Grishman A. New type of cardiomyopathy associated with diabetic glomerulosclerosis. Am J Cardiol. 1972;30:595–602. doi: 10.1016/0002-9149(72)90595-4. [DOI] [PubMed] [Google Scholar]
- 8.Schannwell CM, Schneppenheim M, Perings S, Plehn G, Strauer BE. Left ventricular diastolic dysfunction as an early manifestation of diabetic cardiomyopathy. Cardiology. 2002;98:33–39. doi: 10.1159/000064682. [DOI] [PubMed] [Google Scholar]
- 9.Leung M, Phan V, Whatmough M, Heritier S, Wong VW, Leung DY. Left ventricular diastolic reserve in patients with type 2 diabetes mellitus. Open Heart. 2015;2:e000214. doi: 10.1136/openhrt-2014-000214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Patil VC, Patil HV, Shah KB, Vasani JD, Shetty P. Diastolic dysfunction in asymptomatic type 2 diabetes mellitus with normal systolic function. J Cardiovasc Dis Res. 2011;2:213–22. doi: 10.4103/0975-3583.89805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Boyer JK, Thanigaraj S, Schechtman KB, Perez JE. Prevalence of ventricular diastolic dysfunction in asymptomatic, normotensive patients with diabetes mellitus. Am J Cardiol. 2004;93:870–5. doi: 10.1016/j.amjcard.2003.12.026. [DOI] [PubMed] [Google Scholar]
- 12.Walker AM, Patel PA, Rajwani A, Groves D, Denby C, Kearney L, et al. Diabetes mellitus is associated with adverse structural and functional cardiac remodelling in chronic heart failure with reduced ejection fraction. Diab Vasc Dis Res. 2016;13:331–40. doi: 10.1177/1479164116653342. [DOI] [PubMed] [Google Scholar]
- 13.Henry RM, Paulus WJ, Kamp O, Kostense PJ, Spijkerman AM, Dekker JM, et al. Deteriorating glucose tolerance status is associated with left ventricular dysfunction—the Hoorn Study. Neth J Med. 2008;66:110–7. [PubMed] [Google Scholar]
- 14.Eguchi K, Boden-Albala B, Jin Z, Rundek T, Sacco RL, Homma S, et al. Association between diabetes mellitus and left ventricular hypertrophy in a multiethnic population. Am J Cardiol. 2008;101:1787–91. doi: 10.1016/j.amjcard.2008.02.082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ilercil A, Devereux RB, Roman MJ, Paranicas M, O’Grady MJ, Welty TK, et al. Relationship of impaired glucose tolerance to left ventricular structure and function: The Strong Heart Study. Am Heart J. 2001;141:992–8. doi: 10.1067/mhj.2001.115302. [DOI] [PubMed] [Google Scholar]
- 16.Rerkpattanapipat P, D’Agostino RB, Jr., Link KM, Shahar E, Lima JA, Bluemke DA, et al. Location of arterial stiffening differs in those with impaired fasting glucose versus diabetes: implications for left ventricular hypertrophy from the Multi-Ethnic Study of Atherosclerosis. Diabetes. 2009;58:946–53. doi: 10.2337/db08-1192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Shimizu M, Umeda K, Sugihara N, Yoshio H, Ino H, Takeda R, et al. Collagen remodelling in myocardia of patients with diabetes. J Clin Pathol. 1993;46:32–6. doi: 10.1136/jcp.46.1.32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Regan TJ, Lyons MM, Ahmed SS, Levinson GE, Oldewurtel HA, Ahmad MR, et al. Evidence for cardiomyopathy in familial diabetes mellitus. J Clin Invest. 1977;60:884–99. doi: 10.1172/JCI108843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Yue Y, Meng K, Pu Y, Zhang X. Transforming growth factor beta (TGF-beta) mediates cardiac fibrosis and induces diabetic cardiomyopathy. Diabetes Res Clin Pract. 2017;133:124–30. doi: 10.1016/j.diabres.2017.08.018. [DOI] [PubMed] [Google Scholar]
- 20.Bugger H, Abel ED. Molecular mechanisms of diabetic cardiomyopathy. Diabetologia. 2014;57:660–71. doi: 10.1007/s00125-014-3171-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Ma¨kimattila S, Virkama¨ki A, Groop PH, Cockcroft J, Utriainen T, Fagerudd J, et al. Chronic hyperglycemia impairs endothelial function and insulin sensitivity via different mechanisms in insulin-dependent diabetes mellitus. Circulation. 1996;94:1276–82. doi: 10.1161/01.CIR.94.6.1276. [DOI] [PubMed] [Google Scholar]
- 22.Ding Y, Vaziri ND, Coulson R, Kamanna VS, Roh DD. Effects of simulated hyperglycemia, insulin, and glucagon on endothelial nitric oxide synthase expression. Am J Physiol Endocrinol Metab. 2000;279:E11–7. doi: 10.1152/ajpendo.2000.279.1.E11. [DOI] [PubMed] [Google Scholar]
- 23.Fang ZY, Prins JB, Marwick TH. Diabetic cardiomyopathy: evidence, mechanisms, and therapeutic implications. Endocr Rev. 2004;25:543–67. doi: 10.1210/er.2003-0012. [DOI] [PubMed] [Google Scholar]
- 24.Zurova-Nedelcevova J, Navarova J, Drabikova K, Jancinova V, Petrikova M, Bernatova I, et al. Participation of reactive oxygen species in diabetes-induced endothelial dysfunction. Neuro Endocrinol Lett. 2006;27(Suppl 2):168–71. [PubMed] [Google Scholar]
- 25.Sada K, Nishikawa T, Kukidome D, Yoshinaga T, Kajihara N, Sonoda K, et al. Hyperglycemia induces cellular hypoxia through production of mitochondrial ROS followed by suppression of aquaporin-1. PLoS ONE. 2016;11:e0158619. doi: 10.1371/journal.pone.0158619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mandarino LJ, Finlayson J, Hassell JR. High glucose downregulates glucose transport activity in retinal capillary pericytes but not endothelial cells. Invest Ophthalmol Vis Sci. 1994;35:964–72. [PubMed] [Google Scholar]
- 27.Kaiser N, Sasson S, Feener EP, Boukobza-Vardi N, Higashi S, Moller DE, et al. Differential regulation of glucose transport and transporters by glucose in vascular endothelial and smooth muscle cells. Diabetes. 1993;42:80–9. doi: 10.2337/diab.42.1.80. [DOI] [PubMed] [Google Scholar]
- 28.Dobrina A, Rossi F. Metabolic properties of freshly isolated bovine endothelial cells. Biochim Biophys Acta. 1983;762:295–301. doi: 10.1016/0167-4889(83)90084-8. [DOI] [PubMed] [Google Scholar]
- 29.Hansen SS, Aasum E, Hafstad AD. The role of NADPH oxidases in diabetic cardiomyopathy. Biochim Biophys Acta. 2017;1864(5 Pt B):1908–1913. doi: 10.1016/j.bbadis.2017.07.025. [DOI] [PubMed] [Google Scholar]
- 30.Helies-Toussaint C, Gambert S, Roller P, Tricot S, Lacour B, Grynberg A. Lipid metabolism in human endothelial cells. Biochim Et Biophys Acta-Mol Cell Biol Lipids. 2006;1761:765–74. doi: 10.1016/j.bbalip.2006.05.013. [DOI] [PubMed] [Google Scholar]
- 31.Patella F, Schug ZT, Persi E, Neilson LJ, Erami Z, Avanzato D, et al. Proteomics-based metabolic modeling reveals that fatty acid oxidation (FAO) controls endothelial cell (EC) permeability. Mol Cell Proteom. 2015;14:621–34. doi: 10.1074/mcp.M114.045575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Koziel A, Woyda-Ploszczyca A, Kicinska A, Jarmuszkiewicz W. The influence of high glucose on the aerobic metabolism of endothelial EA.hy926 cells. Pflug Arch. 2012;464:657–69. doi: 10.1007/s00424-012-1156-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Schoors S, Bruning U, Missiaen R, Queiroz KC, Borgers G, Elia I, et al. Fatty acid carbon is essential for dNTP synthesis in endothelial cells. Nature. 2015;520:192–97. doi: 10.1038/nature14362. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.De Bock K, Georgiadou M, Schoors S, Kuchnio A, Wong BW, Cantelmo AR, et al. Role of PFKFB3-driven glycolysis in vessel sprouting. Cell. 2013;154:651–63. doi: 10.1016/j.cell.2013.06.037. [DOI] [PubMed] [Google Scholar]
- 35.Sone H, Deo BK, Kumagai AK. Enhancement of glucose transport by vascular endothelial growth factor in retinal endothelial cells. Invest Ophthalmol Vis Sci. 2000;41:1876–84. [PubMed] [Google Scholar]
- 36.Zhang Z, Apse K, Pang J, Stanton RC. High glucose inhibits glucose-6-phosphate dehydrogenase via cAMP in aortic endothelial cells. J Biol Chem. 2000;275:40042–7. doi: 10.1074/jbc.M007505200. [DOI] [PubMed] [Google Scholar]
- 37.Leopold JA, Cap A, Scribner AW, Stanton RC, Loscalzo J. Glucose-6-phosphate dehydrogenase deficiency promotes endothelial oxidant stress and decreases endothelial nitric oxide bioavailability. FASEB J. 2001;15:1771–3. doi: 10.1096/fj.00-0893fje. [DOI] [PubMed] [Google Scholar]
- 38.Leopold JA, Zhang YY, Scribner AW, Stanton RC, Loscalzo J. Glucose-6-phosphate dehydrogenase overexpression decreases endothelial cell oxidant stress and increases bioavailable nitric oxide. Arterioscler Thromb Vasc Biol. 2003;23:411–7. doi: 10.1161/01.ATV.0000056744.26901.BA. [DOI] [PubMed] [Google Scholar]
- 39.Du XL, Edelstein D, Dimmeler S, Ju Q, Sui C, Brownlee M. Hyperglycemia inhibits endothelial nitric oxide synthase activity by posttranslational modification at the Akt site. J Clin Invest. 2001;108:1341–8. doi: 10.1172/JCI11235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Luo B, Soesanto Y, McClain DA. Protein modification by O-linked GlcNAc reduces angiogenesis by inhibiting Akt activity in endothelial cells. Arterioscler Thromb Vasc Biol. 2008;28:651–7. doi: 10.1161/ATVBAHA.107.159533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Wautier JL, Zoukourian C, Chappey O, Wautier MP, Guillausseau PJ, Cao R, et al. Receptor-mediated endothelial cell dysfunction in diabetic vasculopathy. Soluble receptor for advanced glycation end products blocks hyperpermeability in diabetic rats. J Clin Invest. 1996;97:238–43. doi: 10.1172/JCI118397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Soro-Paavonen A, Zhang WZ, Venardos K, Coughlan MT, Harris E, Tong DC, et al. Advanced glycation end-products induce vascular dysfunction via resistance to nitric oxide and suppression of endothelial nitric oxide synthase. J Hypertens. 2010;28:780–8. doi: 10.1097/HJH.0b013e328335043e. [DOI] [PubMed] [Google Scholar]
- 43.Esposito C, Fasoli G, Plati AR, Bellotti N, Conte MM, Cornacchia F, et al. Long-term exposure to high glucose up-regulates VCAM-induced endothelial cell adhesiveness to PBMC. Kidney Int. 2001;59:1842–9. doi: 10.1046/j.1523-1755.2001.0590051842.x. [DOI] [PubMed] [Google Scholar]
- 44.Katakami N. Mechanism of development of atherosclerosis and cardiovascular disease in diabetes mellitus. J Atheroscler Thromb. 2017;25:27–39. doi: 10.5551/jat.RV17014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Bierhaus A, Chevion S, Chevion M, Hofmann M, Quehenberger P, Illmer T, et al. Advanced glycation end product-induced activation of NF-kappaB is suppressed by alpha-lipoic acid in cultured endothelial cells. Diabetes. 1997;46:1481–90. doi: 10.2337/diab.46.9.1481. [DOI] [PubMed] [Google Scholar]
- 46.Li J, Schmidt AM. Characterization and functional analysis of the promoter of RAGE, the receptor for advanced glycation end products. J Biol Chem. 1997;272:16498–506. doi: 10.1074/jbc.272.26.16498. [DOI] [PubMed] [Google Scholar]
- 47.Dhar A, Dhar I, Desai KM, Wu L. Methylglyoxal scavengers attenuate endothelial dysfunction induced by methylglyoxal and high concentrations of glucose. Br J Pharmacol. 2010;161:1843–56. doi: 10.1111/j.1476-5381.2010.01017.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Su Y, Qadri SM, Wu L, Liu L. Methylglyoxal modulates endothelial nitric oxide synthase-associated functions in EA.hy926 endothelial cells. Cardiovasc Diabetol. 2013;12:134. doi: 10.1186/1475-2840-12-134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Nielsen R, Norrelund H, Kampmann U, Botker HE, Moller N, Wiggers H. Effect of acute hyperglycemia on left ventricular contractile function in diabetic patients with and without heart failure: two randomized cross-over studies. PLoS ONE. 2013;8:e53247. doi: 10.1371/journal.pone.0053247. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Viberti GC. Increased capillary permeability in diabetes mellitus and its relationship to microvascular angiopathy. Am J Med. 1983;75:81–4. doi: 10.1016/0002-9343(83)90257-7. [DOI] [PubMed] [Google Scholar]
- 51.Hempel A, Maasch C, Heintze U, Lindschau C, Dietz R, Luft FC, et al. High glucose concentrations increase endothelial cell permeability via activation of protein kinase C alpha. Circ Res. 1997;81:363–71. doi: 10.1161/01.RES.81.3.363. [DOI] [PubMed] [Google Scholar]
- 52.Yuan SY, Ustinova EE, Wu MH, Tinsley JH, Xu W, Korompai FL, et al. Protein kinase C activation contributes to microvascular barrier dysfunction in the heart at early stages of diabetes. Circ Res. 2000;87:412–7. doi: 10.1161/01.RES.87.5.412. [DOI] [PubMed] [Google Scholar]
- 53.Mellor H, Parker PJ. The extended protein kinase C superfamily. Biochem J. 1998;332(Pt 2):281–92. doi: 10.1042/bj3320281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Ishii H, Jirousek MR, Koya D, Takagi C, Xia P, Clermont A, et al. Amelioration of vascular dysfunctions in diabetic rats by an oral PKC beta inhibitor. Science. 1996;272:728–31. doi: 10.1126/science.272.5262.728. [DOI] [PubMed] [Google Scholar]
- 55.Haidari M, Zhang W, Willerson JT, Dixon RA. Disruption of endothelial adherens junctions by high glucose is mediated by protein kinase C-beta-dependent vascular endothelial cadherin tyrosine phosphorylation. Cardiovasc Diabetol. 2014;13:112. doi: 10.1186/1475-2840-13-112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Bauer HC, Traweger A, Zweimueller-Mayer J, Lehner C, Tempfer H, Krizbai I, et al. New aspects of the molecular constituents of tissue barriers. J Neural Transm (Vienna) 2011;118:7–21. doi: 10.1007/s00702-010-0484-6. [DOI] [PubMed] [Google Scholar]
- 57.Murakami T, Frey T, Lin C, Antonetti DA. Protein kinase c-beta phosphorylates occludin regulating tight junction trafficking in vascular endothelial growth factor-induced permeability in vivo. Diabetes. 2012;61:1573–83. doi: 10.2337/db11-1367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Chen S, Evans T, Mukherjee K, Karmazyn M, Chakrabarti S. Diabetes-induced myocardial structural changes: role of endothelin-1 and its receptors. J Mol Cell Cardiol. 2000;32:1621–9. doi: 10.1006/jmcc.2000.1197. [DOI] [PubMed] [Google Scholar]
- 59.Liefeldt L, Rylski B, Walcher F, Manhart J, Kron S, Rosenke YW, et al. Effects of transgenic endothelin-2 overexpression on diabetic cardiomyopathy in rats. Eur J Clin Invest. 2010;40:203–10. doi: 10.1111/j.1365-2362.2009.02251.x. [DOI] [PubMed] [Google Scholar]
- 60.Muzaffar S, Shukla N, Bond M, Sala-Newby GB, Newby AC, Angelini GD, et al. Superoxide from NADPH oxidase upregulates type 5 phosphodiesterase in human vascular smooth muscle cells: inhibition with iloprost and NONOate. Br J Pharmacol. 2008;155:847–56. doi: 10.1038/bjp.2008.300. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Muzaffar S, Jeremy JY, Angelini GD, Shukla N. NADPH oxidase 4 mediates upregulation of type 4 phosphodiesterases in human endothelial cells. J Cell Physiol. 2012;227:1941–50. doi: 10.1002/jcp.22922. [DOI] [PubMed] [Google Scholar]
- 62.Csanyi G, Lepran I, Flesch T, Telegdy G, Szabo G, Mezei Z. Lack of endothelium-derived hyperpolarizing factor (EDHF) up-regulation in endothelial dysfunction in aorta in diabetic rats. Pharmacol Rep. 2007;59:447–55. [PubMed] [Google Scholar]
- 63.Sena CM, Pereira AM, Seica R. Endothelial dysfunction—a major mediator of diabetic vascular disease. Biochim Biophys Acta. 2013;1832:2216–31. doi: 10.1016/j.bbadis.2013.08.006. [DOI] [PubMed] [Google Scholar]
- 64.Williams SB, Cusco JA, Roddy MA, Johnstone MT, Creager MA. Impaired nitric oxide-mediated vasodilation in patients with non-insulin-dependent diabetes mellitus. J Am Coll Cardiol. 1996;27:567–74. doi: 10.1016/0735-1097(95)00522-6. [DOI] [PubMed] [Google Scholar]
- 65.Johnstone MT, Creager SJ, Scales KM, Cusco JA, Lee BK, Creager MA. Impaired endothelium-dependent vasodilation in patients with insulin-dependent diabetes mellitus. Circulation. 1993;88:2510–6. doi: 10.1161/01.CIR.88.6.2510. [DOI] [PubMed] [Google Scholar]
- 66.Heygate KM, Lawrence IG, Bennett MA, Thurston H. Impaired endothelium-dependent relaxation in isolated resistance arteries of spontaneously diabetic rats. Br J Pharmacol. 1995;116:3251–9. doi: 10.1111/j.1476-5381.1995.tb15132.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Hamed S, Brenner B, Aharon A, Daoud D, Roguin A. Nitric oxide and superoxide dismutase modulate endothelial progenitor cell function in type 2 diabetes mellitus. Cardiovasc Diabetol. 2009;8:56. doi: 10.1186/1475-2840-8-56. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.El-Omar MM, Lord R, Draper NJ, Shah AM. Role of nitric oxide in posthypoxic contractile dysfunction of diabetic cardiomyopathy. Eur J Heart Fail. 2003;5:229–39. doi: 10.1016/S1388-9842(03)00010-2. [DOI] [PubMed] [Google Scholar]
- 69.Stockklauser-Farber K, Ballhausen T, Laufer A, Rosen P. Influence of diabetes on cardiac nitric oxide synthase expression and activity. Biochim Biophys Acta. 2000;1535:10–20. doi: 10.1016/S0925-4439(00)00078-8. [DOI] [PubMed] [Google Scholar]
- 70.Rosen P, Du X, Sui GZ. Molecular mechanisms of endothelial dysfunction in the diabetic heart. Adv Exp Med Biol. 2001;498:75–86. doi: 10.1007/978-1-4615-1321-6_11. [DOI] [PubMed] [Google Scholar]
- 71.Cho YE, Basu A, Dai A, Heldak M, Makino A. Coronary endothelial dysfunction and mitochondrial reactive oxygen species in type 2 diabetic mice. Am J Physiol Cell Physiol. 2013;305:1033. doi: 10.1152/ajpcell.00234.2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Xia Z, Nagareddy PR, Guo Z, Zhang W, McNeill JH. Antioxidant N-acetylcysteine restores systemic nitric oxide availability and corrects depressions in arterial blood pressure and heart rate in diabetic rats. Free Radic Res. 2006;40:175–84. doi: 10.1080/10715760500484336. [DOI] [PubMed] [Google Scholar]
- 73.Hattori Y, Kawasaki H, Abe K, Kanno M. Superoxide dismutase recovers altered endothelium-dependent relaxation in diabetic rat aorta. Am J Physiol. 1991;261:H1086–94. doi: 10.1152/ajpheart.1991.261.4.H1086. [DOI] [PubMed] [Google Scholar]
- 74.Voinea M, Georgescu A, Manea A, Dragomir E, Manduteanu I, Popov D, et al. Superoxide dismutase entrapped-liposomes restore the impaired endothelium-dependent relaxation of resistance arteries in experimental diabetes. Eur J Pharmacol. 2004;484:111–8. doi: 10.1016/j.ejphar.2003.11.004. [DOI] [PubMed] [Google Scholar]
- 75.Vanhoutte PM, Shimokawa H, Feletou M, Tang EH. Endothelial dysfunction and vascular disease—a 30th anniversary update. Acta Physiol (Oxf) 2017;219:22–96. doi: 10.1111/apha.12646. [DOI] [PubMed] [Google Scholar]
- 76.Sukumar P, Viswambharan H, Imrie H, Cubbon RM, Yuldasheva N, Gage M, et al. Nox2 NADPH oxidase has a critical role in insulin resistance-related endothelial cell dysfunction. Diabetes. 2013;62:2130–4. doi: 10.2337/db12-1294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Christ M, Bauersachs J, Liebetrau C, Heck M, Gunther A, Wehling M. Glucose increases endothelial-dependent superoxide formation in coronary arteries by NAD(P)H oxidase activation: attenuation by the 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor atorvastatin. Diabetes. 2002;51:2648–52. doi: 10.2337/diabetes.51.8.2648. [DOI] [PubMed] [Google Scholar]
- 78.Hink U, Li H, Mollnau H, Oelze M, Matheis E, Hartmann M, et al. Mechanisms underlying endothelial dysfunction in diabetes mellitus. Circ Res. 2001;88:E14–22. doi: 10.1161/01.RES.88.2.e14. [DOI] [PubMed] [Google Scholar]
- 79.Landmesser U, Dikalov S, Price SR, McCann L, Fukai T, Holland SM, et al. Oxidation of tetrahydrobiopterin leads to uncoupling of endothelial cell nitric oxide synthase in hypertension. J Clin Invest. 2003;111:1201–9. doi: 10.1172/JCI200314172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Alp NJ, Mussa S, Khoo J, Cai S, Guzik T, Jefferson A, et al. Tetrahydrobiopterin-dependent preservation of nitric oxide-mediated endothelial function in diabetes by targeted transgenic GTP-cyclohydrolase I overexpression. J Clin Invest. 2003;112:725–35. doi: 10.1172/JCI17786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Schmidt K, Rehn M, Stessel H, Wolkart G, Mayer B. Evidence against tetrahydrobiopterin depletion of vascular tissue exposed to nitric oxide/superoxide or nitroglycerin. Free Radic Biol Med. 2010;48:145–52. doi: 10.1016/j.freeradbiomed.2009.10.038. [DOI] [PubMed] [Google Scholar]
- 82.Kikuchi C, Kajikuri J, Hori E, Nagami C, Matsunaga T, Kimura K, et al. Aortic superoxide production at the early hyperglycemic stage in a rat type 2 diabetes model and the effects of pravastatin. Biol Pharm Bull. 2014;37:996–1002. doi: 10.1248/bpb.b13-00975. [DOI] [PubMed] [Google Scholar]
- 83.Pannirselvam M, Simon V, Verma S, Anderson T, Triggle CR. Chronic oral supplementation with sepiapterin prevents endothelial dysfunction and oxidative stress in small mesenteric arteries from diabetic (db/db) mice. Br J Pharmacol. 2003;140:701–6. doi: 10.1038/sj.bjp.0705476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Heitzer T, Krohn K, Albers S, Meinertz T. Tetrahydrobiopterin improves endothelium-dependent vasodilation by increasing nitric oxide activity in patients with Type II diabetes mellitus. Diabetologia. 2000;43:1435–8. doi: 10.1007/s001250051551. [DOI] [PubMed] [Google Scholar]
- 85.Meininger CJ, Marinos RS, Hatakeyama K, Martinez-Zaguilan R, Rojas JD, Kelly KA, et al. Impaired nitric oxide production in coronary endothelial cells of the spontaneously diabetic BB rat is due to tetrahydrobiopterin deficiency. Biochem J. 2000;349:353–6. doi: 10.1042/bj3490353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Zou MH, Shi C, Cohen RA. Oxidation of the zinc-thiolate complex and uncoupling of endothelial nitric oxide synthase by peroxynitrite. J Clin Invest. 2002;109:817–26. doi: 10.1172/JCI0214442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Abbasi F, Asagmi T, Cooke JP, Lamendola C, McLaughlin T, Reaven GM, et al. Plasma concentrations of asymmetric dimethylarginine are increased in patients with type 2 diabetes mellitus. Am J Cardiol. 2001;88:1201–3. doi: 10.1016/S0002-9149(01)02063-X. [DOI] [PubMed] [Google Scholar]
- 88.Xiong Y, Fu YF, Fu SH, Zhou HH. Elevated levels of the serum endogenous inhibitor of nitric oxide synthase and metabolic control in rats with streptozotocin-induced diabetes. J Cardiovasc Pharmacol. 2003;42:191–6. doi: 10.1097/00005344-200308000-00006. [DOI] [PubMed] [Google Scholar]
- 89.Lin KY, Ito A, Asagami T, Tsao PS, Adimoolam S, Kimoto M, et al. Impaired nitric oxide synthase pathway in diabetes mellitus: role of asymmetric dimethylarginine and dimethylarginine dimethylaminohydrolase. Circulation. 2002;106:987–92. doi: 10.1161/01.CIR.0000027109.14149.67. [DOI] [PubMed] [Google Scholar]
- 90.Bucala R, Tracey KJ, Cerami A. Advanced glycosylation products quench nitric oxide and mediate defective endothelium-dependent vasodilatation in experimental diabetes. J Clin Invest. 1991;87:432–8. doi: 10.1172/JCI115014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Patel H, Chen J, Das KC, Kavdia M. Hyperglycemia induces differential change in oxidative stress at gene expression and functional levels in HUVEC and HMVEC. Cardiovasc Diabetol. 2013;12:142. doi: 10.1186/1475-2840-12-142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Garcia Soriano F, Virag L, Jagtap P, Szabo E, Mabley JG, Liaudet L, et al. Diabetic endothelial dysfunction: the role of poly(ADP-ribose) polymerase activation. Nat Med. 2001;7:108–13. doi: 10.1038/83241. [DOI] [PubMed] [Google Scholar]
- 93.Du X, Matsumura T, Edelstein D, Rossetti L, Zsengeller Z, Szabo C, et al. Inhibition of GAPDH activity by poly(ADP-ribose) polymerase activates three major pathways of hyperglycemic damage in endothelial cells. J Clin Invest. 2003;112:1049–57. doi: 10.1172/JCI18127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Chen S, Yang J, Xiang H, Chen W, Zhong H, Yang G, et al. Role of sphingosine-1-phosphate receptor 1 and sphingosine-1-phosphate receptor 2 in hyperglycemia-induced endothelial cell dysfunction. Int J Mol Med. 2015;35:1103–8. doi: 10.3892/ijmm.2015.2100. [DOI] [PubMed] [Google Scholar]
- 95.Kukidome D, Nishikawa T, Sonoda K, Imoto K, Fujisawa K, Yano M, et al. Activation of AMP-activated protein kinase reduces hyperglycemia-induced mitochondrial reactive oxygen species production and promotes mitochondrial biogenesis in human umbilical vein endothelial cells. Diabetes. 2006;55:120–7. doi: 10.2337/diabetes.55.01.06.db05-0943. [DOI] [PubMed] [Google Scholar]
- 96.Wang XR, Zhang MW, Chen DD, Zhang Y, Chen AF. AMP-activated protein kinase rescues the angiogenic functions of endothelial progenitor cells via manganese superoxide dismutase induction in type 1 diabetes. Am J Physiol Endocrinol Metab. 2011;300:E1135–45. doi: 10.1152/ajpendo.00001.2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Xie Z, Zhang J, Wu J, Viollet B, Zou MH. Upregulation of mitochondrial uncoupling protein-2 by the AMP-activated protein kinase in endothelial cells attenuates oxidative stress in diabetes. Diabetes. 2008;57:3222–30. doi: 10.2337/db08-0610. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 98.Mackenzie RM, Salt IP, Miller WH, Logan A, Ibrahim HA, Degasperi A, et al. Mitochondrial reactive oxygen species enhance AMP-activated protein kinase activation in the endothelium of patients with coronary artery disease and diabetes. Clin Sci (Lond) 2013;124:403–11. doi: 10.1042/CS20120239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Li FY, Lam KS, Tse HF, Chen C, Wang Y, Vanhoutte PM, et al. Endothelium-selective activation of AMP-activated protein kinase prevents diabetes mellitus-induced impairment in vascular function and reendothelialization via induction of heme oxygenase-1 in mice. Circulation. 2012;126:1267–77. doi: 10.1161/CIRCULATIONAHA.112.108159. [DOI] [PubMed] [Google Scholar]
- 100.Viollet B, Lantier L, Devin-Leclerc J, Hebrard S, Amouyal C, Mounier R, et al. Targeting the AMPK pathway for the treatment of Type 2 diabetes. Front Biosci (Landmark Ed) 2009;14:3380–400. doi: 10.2741/3460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Bereiter-Hahn J, Voth M. Dynamics of mitochondria in living cells: shape changes, dislocations, fusion, and fission of mitochondria. Microsc Res Tech. 1994;27:198–219. doi: 10.1002/jemt.1070270303. [DOI] [PubMed] [Google Scholar]
- 102.Shenouda SM, Widlansky ME, Chen K, Xu G, Holbrook M, Tabit CE, et al. Altered mitochondrial dynamics contributes to endothelial dysfunction in diabetes mellitus. Circulation. 2011;124:444–53. doi: 10.1161/CIRCULATIONAHA.110.014506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Makino A, Scott BT, Dillmann WH. Mitochondrial fragmentation and superoxide anion production in coronary endothelial cells from a mouse model of type 1 diabetes. Diabetologia. 2010;53:1783–94. doi: 10.1007/s00125-010-1770-4. [DOI] [PMC free article] [PubMed] [Google Scholar]