

Abstract:
Levosimendan is an inodilator that promotes cardiac contractility primarily through calcium sensitization of cardiac troponin C and vasodilatation via opening of adenosine triphosphate–sensitive potassium (KATP) channels in vascular smooth muscle cells; the drug also exerts organ-protective effects through a similar effect on mitochondrial KATP channels. This pharmacological profile identifies levosimendan as a drug that may have applications in a wide range of critical illness situations encountered in intensive care unit medicine: hemodynamic support in cardiogenic or septic shock; weaning from mechanical ventilation or from extracorporeal membrane oxygenation; and in the context of cardiorenal syndrome. This review, authored by experts from 9 European countries (Austria, Belgium, Czech republic, Finland, France, Germany, Italy, Sweden, and Switzerland), examines the clinical and experimental data for levosimendan in these situations and concludes that, in most instances, the evidence is encouraging, which is not the case with other cardioactive and vasoactive drugs routinely used in the intensive care unit. The size of the available studies is, however, limited and the data are in need of verification in larger controlled trials. Some proposals are offered for the aims and designs of these additional studies.
Key Words: inodilator, hemodynamic support, cardiogenic shock, septic shock, weaning, mechanical ventilation, extracorporeal membrane oxygenation, cardiorenal syndrome
THE CALCIUM SENSITIZER LEVOSIMENDAN
Levosimendan is a positive inotropic compound with vasodilatory properties1 used for the treatment of acute decompensated heart failure (HF) and in cases where the use of an inotropic treatment is considered appropriate.2 The principal mechanism of levosimendan is the sensitization of troponin C to calcium in cardiac muscle,3–5 which leads to its unique feature of exerting a positive inotropic effect without increasing myocardial oxygen consumption.6–10 In addition, levosimendan opens adenosine triphosphate–sensitive potassium (KATP) channels in vascular smooth muscle cells11,12 and induces vasodilation of the pulmonary,13 coronary,14,15 and peripheral arteries16 and of the venous circulation.17 By addressing both cardiac inotropy and vascular dilatation, levosimendan improves cardiovascular coupling and cardiac mechanical efficiency. Levosimendan also opens mitochondrial KATP channels18 and exerts an organ-protective and, especially, cardioprotective effect in various settings.19,20 At higher doses, the drug also acts as a phosphodiesterase type 3 (PDE3) inhibitor.1,12,21,22 The effects of levosimendan are not impaired by the concomitant use of beta-blockers.23
Levosimendan has been studied in several therapeutic applications, particularly in the management of acute HF (AHF) patients with low cardiac output24,25 and in high-risk cardiac surgery.26,27 Levosimendan has also shown preliminary positive effects in a range of other conditions requiring inotropic support, including right ventricular failure, cardiogenic shock (CS), septic shock, and Takotsubo cardiomyopathy.28
Owing to its pharmacology, it has become apparent that levosimendan may also have applications in the setting of intensive care medicine. The conceptual framework for this wider use of levosimendan has been set out by Farmakis et al28 and is supported by an array of experimental and observational research29–37 (Box 1).
BOX 1. Expected Effects of Levosimendan in Intensive Care Unit Settings.
General hemodynamic support;
Increased ejection fraction and cardiac index without increase of oxygen consumption;
Peripheral vasodilation and reduction of tissues and organ hypoperfusion;
Increased GFR and renal function;
Decrease in need for catecholamines;
Sustained effects; and
No increase in long-term mortality.
This commentary identifies a range of clinical situations encountered in the intensive care unit (ICU) where levosimendan may offer clinical advantages, either as an adjunct to standard-of-care therapies or as an alternative to conventional therapies (Box 2).
BOX 2. Intensive Care Unit Settings in Which the Use of Levosimendan Has Been Described.
Cardiogenic shock;
Septic shock;
Weaning from ventilator;
Weaning from extracorporeal membrane oxygenation;
Pulmonary hypertension and right ventricular dysfunction; and
Need for hemodynamic support in patients with diuretic resistance.
HEMODYNAMIC SUPPORT IN CARDIAC CRITICAL CARE
In severe AHF and CS, congestion and hypoperfusion lead to a systemic disorder that potentially affects all vital organs. Restoring adequate cardiac output and organ perfusion, and promoting decongestion, are therefore medical priorities during the early phase of treatment.38–40
In AHF leading to tissue hypoperfusion, initial use of an inotrope is advocated.40,41Hence, inotropic support remains a cornerstone of AHF management in these critically ill patients, together with adequate fluid resuscitation (or depletion) and optimization of arterial pressure to suit the individual features of patients.
Reported rates of inotropic support in AHF management vary from 9% in an early US registry42 to >30% in a later international registry43 and 13% in the 2017 European Society of Cardiology (ESC) Heart Failure Long-Term Registry.44 Robust secular trends in the use of inotropes are hard to identify from these fluctuations but dobutamine remains the most frequently used inotrope.
The indication for inotropic support depends largely on the etiology; heading this hierarchy is CS, for which, by definition, virtually all patients are supported by at least one inotropic drug.45 In septic shock, inotropic support is deployed according to current precepts of early goal-directed therapy (EGDT); in recent EGDT trials, rates of inotrope use ranged from ≈15% for patients included in the intervention groups to usually <5% for those in the standard-of-care groups.46 The prevalence of inotropic support at admission was 15%–20% in a recent pragmatic multicenter trial of levosimendan in septic shock.37 Inotropic support may also be considered in cases of obstructive shock, while waiting for the obstruction to be removed, but continuation after that point would be uncommon.
Dobutamine is the first-line inotropic agent for resuscitating patients suffering from either severe AHF and low-cardiac output syndrome40 in CS41,47 or septic shock48 but its administration entails substantial addition of exogenous catecholamines to the endogenous ones already overproduced by the intense activation of the sympathetic autonomous nervous system.
The resulting exacerbation of the beta-adrenergic pathway induces an increase in myocardial oxygen consumption via chronotropic and inotropic effects.49 This catecholamine-induced myocardial oxygenation imbalance exacerbates myocardial ischemia,50,51 especially at the level of the subendocardium.52 Inter alia, excessive adrenergic stimulation is also established as a key factor in the pathophysiology of Takotsubo cardiomyopathy53 and contributes substantially to some manifestations of the septic cardiomyopathies.54
Various large international registries relating to AHF and CS have documented higher rates of morbidity and mortality in patients treated with adrenergic inotropes than in severity-matched peers who did not receive catecholamines42–45; a recent meta-analysis of randomized clinical trials of dobutamine to treat severe (acute or chronic) HF likewise indicated an increased risk of mortality.55 These observations, with others,56 are the basis of the European Society of Intensive Care Medicine AHF/CS guidance that “The use of these [inotropic/vasopressor] agents should, however, be restricted to the shortest possible duration and lowest possible dose to maintain perfusion pressure”57 and the declaration in the ESC HF guidelines that “There is long-standing concern that [inotropes, especially those with adrenergic mechanisms] may increase mortality.”40
In a randomized clinical trial involving patients with acutely exacerbated chronic HF, the PDE3 inhibitor milrinone was shown to increase mortality in patients suffering from ischemic cardiomyopathy58: a similar finding was also reported in a recent large retrospective cohort study of intraoperative inotropic support in cardiac surgery.59 These data indicate that milrinone (and, by extension, other PDE3 inhibitors) is not a fully satisfactory alternative to dobutamine. Similar reservations apply to dopamine44,60 and epinephrine.45,61
The “decatecholaminization” of the critically ill patient represents a new and still-evolving paradigm in the treatment of patients in the ICU.62,63 One avenue for research in this area has been the evaluation of nonadrenergic vasoactive agents.64–66 These include levosimendan, which offers positive cardiovascular effects (ventriculoarterial recoupling, decongestion, and cardiac protection against ischemia–reperfusion injury) as well as potentially advantageous ancillary effects on kidney function and diaphragm muscular fibers, as discussed later in this review.
LEVOSIMENDAN IN CARDIOGENIC SHOCK
Acute myocardial infarction (AMI) is the most common etiology of CS but CS may arise from any situation of acute, severe dysfunction in either ventricle of the heart. CS is relatively rare but often fatal.67
The standard of care in CS consists of primary percutaneous coronary intervention for AMI, fluid therapy, vasopressors, inotropes and, in the last resort, mechanical assistance.68 Data from initial comparator studies indicate that levosimendan may be a useful addition to this regimen.
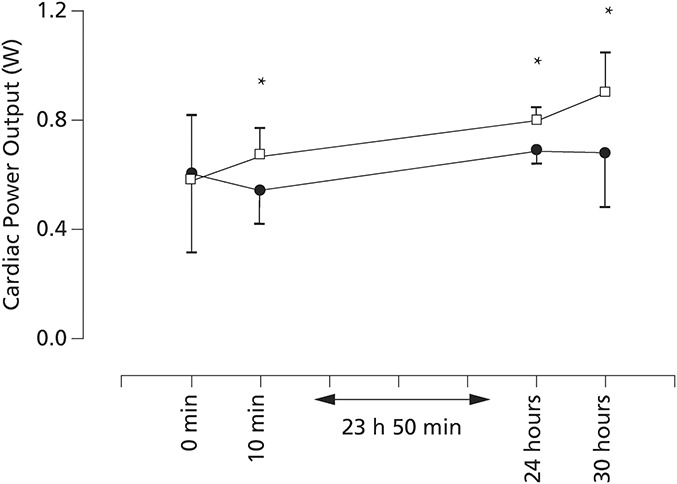
Levosimendan may be a constructive alternative to conventional inotropes for the management of CS. In a trial of 22 consecutive AMI patients who developed CS after percutaneous coronary intervention, levosimendan (24 µg/kg bolus, then 0.1 µg/kg/min for 24 hours) attained the study end point of ≥30% increase in cardiac power output (CPO) consistently better than dobutamine (initial dose 5 µg/kg/min, with subsequent dose increases to reach the desired hemodynamic effect), despite a comparable reduction in pulmonary capillary wedge pressure69 (Fig. 1) (CPO is the product of cardiac output and mean arterial pressure [MAP] and an indicator of cardiac contractility and ventricular–vascular coupling: in effect, it represents the pumping power of the heart and has been identified as the strongest predictor of survival in patients with CS70).
FIGURE 1.
Changes in CPO during infusion of levosimendan ( ) and dobutamine (
) and dobutamine ( ) in patients with AMI revascularized by percutaneous coronary intervention and who developed cardiac shock. Data points are mean ± SD. *P < 0.05 (Student's t-test). Data from the study by García-González et al.69
) in patients with AMI revascularized by percutaneous coronary intervention and who developed cardiac shock. Data points are mean ± SD. *P < 0.05 (Student's t-test). Data from the study by García-González et al.69
Levosimendan also compared favorably with the PDE inhibitor enoximone in an exploratory open-label study of CS secondary to AMI, giving a small but significant advantage in death from multiorgan failure (P ≈ 0.02).71 Beneficial hemodynamic effects were recorded in both groups, including enhancement of CPO, but these changes were achieved sooner with levosimendan than with enoximone. There was a significant advantage with levosimendan in terms of fewer deaths from multiorgan failure (P < 0.05). Use of dobutamine and norepinephrine in the levosimendan-treated patients was much lower than that in the enoximone group. It is plausible that part of the survival advantage seen with levosimendan may be attributable to a reduction in exposure to exogenous catecholamines.
Notwithstanding these data, levosimendan is currently regarded as a salvage therapy in CS after dobutamine failure and before extracorporeal life support (ECLS). Any revision of this status will require well-designed randomized controlled studies.72 Until then, the use of levosimendan may be considered in cases of low cardiac output associated with signs of hypoperfusion or deteriorating renal/liver function, especially if beta-blocker use is part of the clinical scenario.
Use of levosimendan is contraindicated in hypovolemia, which must be excluded using echocardiography and/or advanced monitoring and dynamic indices. Cardiac output monitoring (transpulmonary thermodilution or pulmonary artery catheterization in cases of associated right ventricular dysfunction) is highly recommended.
Omitting a loading dose seems a rationale choice, while the maintenance infusion for a total duration of 24 hours (0.05–0.2 μg/kg/min) should be individually adjusted. After levosimendan is started, dobutamine may be weaned according to the hemodynamic and clinical response (generally after 2 hours). As soon as possible, but after weaning of vasopressors, established chronic HF treatments should be (re-)introduced.
In practice, systolic dysfunction and diastolic dysfunction often coexist. The management of circulatory failure related to diastolic dysfunction in critical illness is largely supportive. Adequate fluid resuscitation is often followed by the administration of drugs with a positive lusitropic effect. Levosimendan has been shown to improve diastolic function73 and filling and, importantly, it can be safely combined with beta-blockers, which represent one of the potential treatment modalities for diastolic dysfunction.
LEVOSIMENDAN IN SEPTIC SHOCK
Sepsis is defined nowadays as an infection inducing dysfunction of at least one organ owing to a deregulated host inflammatory response.74 In addition to intrinsic distributive shock due to vascular hyporeactivity and autonomic dysfunction, sepsis can also induce septic cardiomyopathy (SCM) with de novo AHF due to myocardial depression. Such complications contribute to a sepsis mortality rate of ≈30%.74,75 The prevalence of SCM among septic patients varies widely (from 20% to 60%), a state of affairs that reflects both the current lack of a common definition and the heterogeneity of the symptoms.75
Inotropic support is endorsed for restoration of an adequate cardiac output and peripheral oxygen delivery.48 In the absence of a fully evidence-based alternative, dobutamine remains the suggested first-line inotrope for those goals, despite the observations that: (1) high levels of circulating catecholamines and adrenergic overstimulation contribute to the pathophysiology of SCM54,76; (2) the adrenergic response at the cardiomyocyte level is attenuated by downregulation of β-adrenergic receptors77,78; (3) adrenergic drugs have been associated with worse outcomes in a pooled network meta-analysis36; and (4) esmolol, a β1-receptor antagonist, seems to improve the outcome of severe SCM,78 especially in cases of persistent tachycardia.79
Proceeding from the above points, assessment of levosimendan as an alternative inotropic drug in septic shock should address the following clinical goals and criteria.
Dobutamine sparing: reducing the high (toxic) levels of endogenous and pharmacological adrenergic stimulation and hence restoring a better myocardial oxygenation balance, particularly in the case of coronary artery disease with potential catecholamine-induced ischemia.51
Attenuation of multiple-organ failure (MOF): reducing the occurrence and/or severity of sepsis-induced MOF due to better regional blood flow distribution in addition to a global increase in cardiac output, plus pleiotropic effects at the cellular and mitochondrial levels.28,80
Inotropic rescue therapy: restoring inotropic responsiveness in cases of severely attenuated adrenergic response.
Drug safety: replacing adrenergic inotropic drugs without tachyarrhythmia or any additional requirement for vasopressors.
Experimental studies (mainly in animal models of peritonitis-induced septic shock) have demonstrated an improvement in survival, and a reduction in the severity of MOF and anti-inflammatory protective effects with levosimendan.80,81 It must be acknowledged, however, that many of those studies were restricted to comparison versus placebo, not other inotropes.
As regards clinical trials of levosimendan in septic shock, in a monocentric randomized controlled trial, a 24-hour infusion of levosimendan (0.2 µg/kg/min) was compared with dobutamine (5 µg/kg/min) as inotropic support for patients with de novo severe SCM (n = 28) and a left ventricular ejection fraction (LVEF) <45% despite 48 hours of conventional standard-of-care treatment, including dobutamine.82 Levosimendan use was associated with increases in cardiac output and pulmonary decongestion, without an increase in vasopressor requirements (owing to volume expansion) and with more favorable evolution of various MOF surrogates (lactate clearance, venoarterial carbon dioxide gap, gut mucosal perfusion, and renal function). Dobutamine did not materially alter any of these systemic or regional hemodynamic variables.
The findings of this study satisfy the clinical goals identified above and are, to that extent, promising regarding the potential of levosimendan in sepsis and SCM. However, this was a single study with several limitations and must be considered indicative, not definitive.83
The biological mechanisms underpinning this attenuation of MOF have been explored in subsequent clinical trials: levosimendan infusion has been shown to improve microcirculation perfusion,84 relieve mitochondrial oxidative stress,85 and restore the muscular lactate/pyruvate ratio.86 Some of this research, plus additional small clinical trials of heterogeneous quality, has been incorporated into a meta-analysis87 of the effects of levosimendan in septic shock versus standard inotropes (invariably dobutamine where specified). Findings from this exercise (7 studies, 249 patients) included a significant reduction in mortality in the levosimendan group without intergroup differences in MAP or norepinephrine usage.
These clinical observations, together with a strong experimental background, led to the development of a large pragmatic multicenter randomized placebo-controlled trial of levosimendan in sepsis. This study—Levosimendan for the Prevention of Acute oRgan Dysfunction in Sepsis (LeoPARDS; ISRCTN12776039)—examined whether early administration of levosimendan (0.05–0.2 µg/kg/min for 24 hours) could avert the onset of MOF in a broad population of septic shock patients (n = 516) fulfilling the criteria for systemic inflammatory response syndrome due to infection and requiring vasopressor therapy for at least 4 hours.37
LeoPARDS did not fulfill the primary end point of a significant intergroup difference in mean daily Sequential Organ Failure Assessment score favoring levosimendan, and nor was mortality reduced. Although prima facie disappointing, these findings should be considered in perspective. This was a relatively low-risk cohort; most patients were not suffering from either severe circulatory shock or severe SCM needing inotropic support. Moreover, the degree of renal replacement therapy already being undertaken before randomization was substantial and may have led to faster elimination of the study drug in 17% of patients in the intervention group. These reasons may have resulted in LeoPARDS lacking the necessary focus to identify an effect of levosimendan on the patients who could have benefitted.
The currently available clinical evidence in septic shock indicates that: (1) Levosimendan can successfully replace dobutamine in supporting severe de novo AHF due to SCM, with additional positive extracardiac effects owing to amelioration of MOF. These results need to be replicated on a larger scale; and (2) Indiscriminate use of levosimendan (ie, without selecting severe cases of cardiovascular failure) to prevent the development of MOF is safe from a hemodynamic perspective but may confer no clinical benefit.
In addition, however, recent data from patients in septic shock show ventriculoarterial uncoupling due to either ventricular elastance reduction (as in SCM) or increased arterial elastance due to vasopressor therapy, or both: this is a situation in which cardiac mitochondrial function can be severely impaired and the oxygen metabolism altered.88 No data are currently published on the effect of levosimendan on ventriculoarterial coupling in septic shock, but this matter merits research because the mechanism of action of levosimendan may contribute to the restoration of more normal coupling.
Future investigations to refine the role of levosimendan in the management of septic shock should address (1) the severity of AHF (a priori, there is a case for reserving levosimendan for patients more likely to benefit from it, such as those with severely reduced LVEF or significant coronary artery disease26,89); and (2) the timing of the administration (under which heading, matters for attention include investigation of levosimendan as a first-use inotrope for severe SCM to optimize its positive cardioprotective effects as intimated from various lines of research, including randomized trials in cardiac surgery that recorded better outcomes with earlier administration89–92).
LEVOSIMENDAN AND WEANING FROM THE VENTILATOR
About 10%–20% of intubated patients in ICUs are difficult to wean from mechanical ventilation, resulting in increased morbidity, mortality, and health care costs.93,94 Part of this phenomenon may be attributable to the development of diaphragm weakness in intubated patients. Mechanical ventilation results in rapid loss of diaphragmatic force production.95–97 In one recent study, half of the patients (n = 185) with diaphragmatic dysfunction failed weaning, half of whom died.98 In addition, liberation from mechanical ventilation to spontaneous ventilation may dramatically increase left ventricular filling pressure and pulmonary artery pressure, especially in patients with preexisting cardiac and/or pulmonary comorbidities.
The pathophysiology of muscle weakness in these patients is complex99,100 but includes muscle fiber atrophy and reduced calcium sensitivity of the contractile proteins.101 Because respiratory muscle troponin resembles cardiac troponin, it is plausible that levosimendan may enhance muscular contractility in the same way that it enhances cardiac contractility. This supposition has support from in vitro data,102 experimental research,103 and a healthy volunteer study.104 Positive effects were seen in both slow and rapid diaphragm muscle fibers.102,103
Levosimendan has been compared with dobutamine in difficult-to-wean chronic obstructive pulmonary disease patients.105 Levosimendan resulted in significantly greater inhibition of spontaneous ventilation-induced congestion caused by a rapid increase in pulmonary artery occlusion pressure. Similarly, mean pulmonary artery pressure increased to a lesser extent with levosimendan than with dobutamine. In a prospective observational study in ventilator-dependent difficult-to-wean ICU patients with diminished LVEF (<40%), levosimendan improved cardiac contractility and oxygenation variables and increased the likelihood of separation from mechanical ventilation.93 A study entitled “Effects of Levosimendan on Diaphragm Function in Mechanically Ventilated Patients” (NCT01721434) coordinated by the University Medical Center, Nijmegen, the Netherlands, is currently recruiting.
LEVOSIMENDAN AND WEANING FROM EXTRACORPOREAL MEMBRANE OXYGENATION
Venoarterial extracorporeal membrane oxygenation (VA-ECMO) is increasingly used for short-term management of refractory CS caused by AMI, myocarditis, cardiac surgical procedures in high-risk patients with reduced LVEF, refractory cardiac arrest, and other conditions. In general, it is reserved for situations where pharmacological support of the circulation is not able to restore adequate cardiac output. In cases where there is sufficient recovery of myocardial function during VA-ECMO support, the phase of weaning starts by reducing blood flow through VA-ECMO and thus increasing blood flow to the native heart chambers and pulmonary circulation, ie, increasing the load imposed on both ventricles. In a large observational study, the rate of successful weaning in 4658 patients with CS was reported to be limited to 65.7%.106
A first report on levosimendan in the context of VA-ECMO weaning showed that pretreatment 24 hours before the start of weaning was associated with a 50% reduction in the need for inotropic and/or vasopressor support during or after weaning, compared with a 100% requirement in the retrospective control group (n = 11) (P < 0.003).107 The weaning success rate was significantly higher with levosimendan (83.3% vs. 27.3%; P = 0.0498); the difference in survival rate was substantial but not statistically significant (66.6% vs. 36.4%).
In a recent retrospective analysis of 240 patients on VA-ECMO after cardiovascular surgery, levosimendan was given during the first 24 hours of ECMO support in 74.6% of cases.108 The adjusted hazard ratio for failure of ECMO weaning with levosimendan was significantly improved versus control (hazard ratio 0.41; 95% confidence interval 0.22–0.80; P = 0.008); furthermore, patients in the levosimendan group experienced lower 30-day mortality (P = 0.016) and better long-term survival (Fig. 2). Another study reported improvement in endothelial function after levosimendan infusion in the patients on VA-ECMO, together with an improvement in cardiac function (ie, an increase in cardiac output), facilitating weaning from ECMO.109 Very recent data show that levosimendan enables weaning from ECLS without increasing norepinephrine requirements when compared with a control group receiving milrinone.110
FIGURE 2.
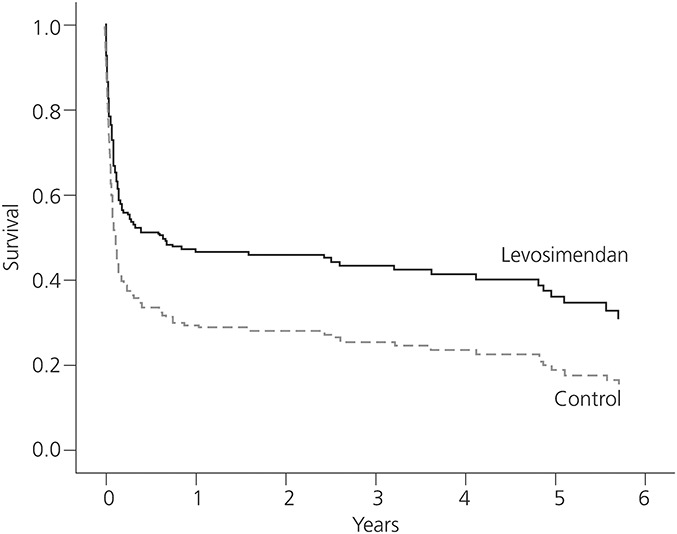
Confounder-adjusted long-term survival (levosimendan vs. control, P = 0.04) in 240 patients weaned from extracorporeal membrane oxygenation. Levosimendan was administered within the first 24 hours after initiation of ECMO therapy, at a standard dose of 12.5 mg in 24 hours. Data from the study by Distelmaier et al.108
Most patients require inotropic drugs to support myocardial contractile function during weaning from VA-ECMO, and the limited clinical evidence currently available suggests that levosimendan offers some important advantages over other inotropes for this vulnerable period: no increase in myocardial oxygen consumption, a prolonged cardiovascular effect (days), and improvement in endothelial function.
LEVOSIMENDAN IN PULMONARY HYPERTENSION AND RIGHT VENTRICULAR DYSFUNCTION
Acute postoperative pulmonary hypertension is a rare but serious event after weaning from cardiopulmonary bypass and must be managed aggressively to avoid right ventricular failure.111,112 The in-hospital mortality rate is high and may reach 70%–75%.113,114 Similar considerations apply in nonsurgical ICUs where right ventricular dysfunction may emerge as a complication of acute respiratory distress syndrome.115
The thin-walled right ventricle has poor tolerance for acute increases in afterload. Ventricular distension leads to severe compromise of contractility concomitant with an increase in oxygen consumption. Ventricular interdependence then implicates the left ventricle, leading to reduced filling, decreased cardiac output and oxygen delivery, and decline in systemic perfusion pressure.116 The pressure gradient for the perfusion of the right coronary artery drops as aortic pressure decreases and right ventricular pressure increases, leading to right ventricular ischemia.117
Augmentation of right ventricular function with inotropic support is central to counteracting this vicious cycle. Levosimendan improves myocardial contractility, with a reduction in pulmonary vascular resistance.118 In an experimental pressure load–induced model of right ventricular failure, levosimendan improved right ventricular to pulmonary artery coupling more than dobutamine.119 The treatment of acute right ventricular failure involves reversing the cause of the increased pulmonary vascular resistance while maintaining adequate MAP. To support adequate systemic arterial tone, a vasopressor is often required, while levosimendan helps to decrease pulmonary vascular resistance and filling pressures.
Investigator-initiated studies have been performed in patients with right ventricular failure. In these, levosimendan reduced increased right ventricular afterload and improved right ventricular contractility and diastolic function.120–123
A recent meta-analysis demonstrated that levosimendan decreased systolic pulmonary pressure and pulmonary vascular resistance concomitant with an increase in right ventricular ejection fraction in patients suffering from acute right HF.124 Much of the extant data come from noncardiac surgery patients suffering from the acute onset of pulmonary hypertension and/or right ventricular dysfunction; data on levosimendan in acute right ventricular failure are sparse though encouraging.125
LEVOSIMENDAN AND RENAL FUNCTION
Evidence for a renal-protective action of levosimendan in preclinical experiments is persuasive but the clinical data set supporting a renal-protective effect rests on a limited number of studies, many of which are small and characterized by heterogeneities.126 The results of those studies acquire significance only when pooled in meta-analyses127–130 but, addressed in that way, the findings are suggestive of a renal-protective effect of levosimendan in a range of cardiac low-output states that may be pertinent to the ICU setting.
Levosimendan has been compared with dobutamine in 88 patients with HF who required inotropic therapy.131 Calculated glomerular filtration rate (GFR) improved in response to levosimendan (0.1–0.2 μg/kg/min, with loading dose at the discretion of individual physicians) but was unchanged in patients who received dobutamine (5 μg/kg/min for at least 6 hours, with subsequent dose alteration or extension beyond 24 hours as judged necessary in individual cases). Complementary findings emerged from a placebo-controlled study in 66 patients hospitalized for decompensated HF and renal dysfunction, with a statistically significant improvement in calculated GFR in patients who received levosimendan (12 μg/kg optional loading dose, then continuous infusion at 0.05–0.2 μg/kg/min for 24 hours). Peak effect was attained 3 days after a 24-hour infusion and the effects persisted for up to 14 days.132 Two open-label studies also reported reduction of serum creatinine levels in levosimendan-treated patients.133,134 In a recent randomized study135 on the effect of levosimendan on renal outcome in 90 cardiac surgery patients with chronic kidney disease and perioperative cardiovascular dysfunction, the authors reported a significant reduction in postoperative acute kidney injury (AKI) and a lower incidence of major complications in the levosimendan arm.
What are the mechanisms behind the clinical observation that levosimendan seems to improve renal function in patients with AHF requiring inotropic support? Inodilators increase cardiac output and also potentially renal blood flow (RBF). It is not immediately evident, however, that an inodilator with renal vasodilating properties also increases GFR: it depends on its effect on the longitudinal distribution of renal vascular resistance. Thus, theoretically, an inodilator that dilates the preglomerular resistance vessels (afferent arterioles) will, at a certain MAP, increase both RBF and GFR. However, an inodilator that preferentially causes vasodilation of the postglomerular resistance vessels (efferent arterioles) will increase RBF but cause a fall in GFR, due to a fall in the upstream glomerular hydraulic pressure. Finally, an inodilator that dilates both preglomerular and postglomerular resistance vessels will induce a pronounced increase in RBF with no change in GFR. Redfors et al136 showed in postcardiac surgery patients that low-dose dopamine (2–4 µg/kg/min) induced a pronounced 40%–50% increase in RBF with no effect on GFR, suggesting vasodilation of both preglomerular and postglomerular resistance vessels. Levosimendan, however, has been shown to increase both RBF and GFR after cardiac surgery, indicating that, in contrast to dopamine, levosimendan improves renal performance by means of preferential preglomerular vasodilation137 (Fig. 3). The major goal in the treatment of AKI is to increase GFR. There is, however, a close association between GFR and renal oxygen consumption138 because any agent that increases GFR will also increase renal oxygen demand. Thus, an ideal inodilator to treat AKI would be one that increases both RBF and GFR. Such an agent will not only increase GFR but will also meet the increased renal metabolic demand by means of increased renal oxygen delivery. Bragadottir et al137 showed that the levosimendan-induced increase in GFR did not impair the renal oxygen supply/demand relationship, suggesting that levosimendan could be an interesting agent for treatment of AHF accompanied by impaired renal function in various clinical settings. In a recent double-blind randomized clinical trial, the same group recently showed that in patients with chronic HF and renal impairment, levosimendan increases GFR to a greater extent than dobutamine and thus may be the preferred inotropic agent for treating patients with cardiorenal syndrome.139
FIGURE 3.
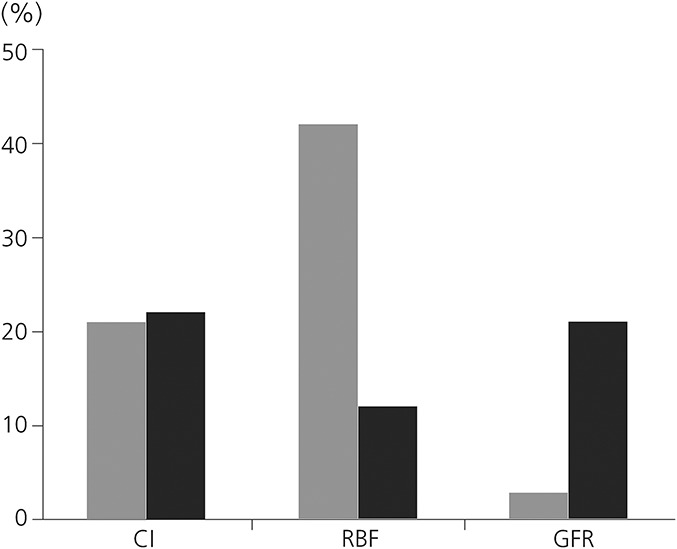
Differential effects of levosimendan (0.1 µg/kg/min) and dopamine (2 µg/kg/min) on RBF and GFR in 30 postcardiac surgery patients. The experimental procedure started 4–6 hours after surgery in the ICU during propofol sedation and mechanical ventilation. Cardiac index (CI) was increased by ≈20% by both drugs. Data from the study by Bragadottir et al.137
Complementary findings were reported from a placebo-controlled study by Fedele et al140 in patients with acute decompensated HF and moderate renal impairment (NCT00527059). Yilmaz et al126 have speculated on the likely contribution of KATP channel-opening effects of levosimendan in vascular smooth muscle to a direct renal-protective effect of levosimendan separate from, and additional to, its effects through improved cardiac function and systemic hemodynamics. Observations on the significance of levosimendan-mediated vasodilatation and decongestion have been made by Damman and Voors.141
Diuretic resistance in HF patients is a common problem. One treatment option could be the administration of levosimendan. This might be a good option before the more aggressive implementation of ultrafiltration.142
OTHER SETTINGS
Is to be noticed that the HFA-ESC Task Force on Takotsubo syndrome143 advocates levosimendan as the single form of inotropic support in cases of unavailable ECLS. Case reports are encouraging,144 and the pathophysiology is conceptually a good fit to the properties of levosimendan.
CONCLUSIONS
Levosimendan has been demonstrated to have potential utility in a range of critical illness scenarios. It must be acknowledged, however, that in each sphere of application, the evidence is incomplete or indicative rather than conclusive, and further clinical evaluation will be needed to substantiate the case for levosimendan and to refine the patient categories and dosage schedules likely to be associated with the greatest clinical benefit.
Having levosimendan a vasodilatory effect, its dosage should be guided in part by following the blood pressure of the patient (as recommended by the indication for use), with bolus omitted or used only if SBP is ≥100 mm Hg145 (Box 3). Meta-analysis of 45 randomized controlled trials in cardiac surgery or cardiology identifies an infusion rate range of 0.05–0.2 μg·kg−1·min−1, with some indications that both lower rates (≤0.1 μg·kg−1·min−1) and omission of bolus dose may confer greater long-term survival advantages over higher doses and use of bolus.146 The presence of a long-lived metabolite is associated with the persistence of the hemodynamic effects of levosimendan147 for 7–10 days after a single 24-hour infusion of levosimendan. The inodilator levosimendan is mainly used for its hemodynamic effects, and the longer action of its active metabolite is fully consistent with the pharmacologic effects observed in the beginning of the treatment: no increase in the rate of adverse events was observed after the 24-hour infusion of levosimendan.148
BOX 3. Recommended Dosage of Levosimendan When Used in Intensive Care Unit Settings.
Levosimendan dosage should be guided by following the blood pressure;
Bolus should be omitted or used only if SBP is ≥100 mm Hg;
An infusion rate range of 0.05–0.2 μg·kg−1·min−1 starting at 0.1 μg·kg−1·min−1 and uptitrated or downtitrated to the doses, which gives hemodynamic stability while avoiding adverse effects such hypotension and/or arrhythmias;
Hypovolemia and hypokalemia should be avoided before and during treatment;
The presence of a long-lived metabolite is associated with the persistence of the hemodynamic effects of levosimendan 7–10 days after a single 24-hour infusion of levosimendan;
Levosimendan is mainly used for its hemodynamic effects, and the longer action of its active metabolite is fully consistent with the pharmacologic effects observed in the beginning of the treatment: no increase in the rate of adverse events (hypotension and/or arrhythmia) is observed after the 24-hour infusion of levosimendan.
The regulatory Phase IIb–III clinical trials program on the efficacy and safety of levosimendan in AHF completed in 2005 (see complete trial list in the study by Pollesello et al149) did not give an unequivocal answer to the question whether the short-term use of levosimendan lowers long-term mortality in patients hospitalized for decompensated AHF irrespectively to its etiology and to the use of comedications during the preacute, periacute, and postacute phase. Some trials showed a significant improvement in survival, whereas some (the larger ones) did not, but the bulk of evidence did overall support the efficacy and safety of the drug, and a market authorization was granted in over 60 countries, with the notable exception of the United States and the United Kingdom. The regulatory studies included a broad variety of patients, both as it regards the etiologies of AHF (eg, de novo vs. chronic decompensated), the monitoring (eg, invasively vs. non-invasively), the time of treatment (eg, early during hospitalization vs. late), and the co-medications (eg, beta-blockade vs. non–beta-blockade). When more homogeneous groups of patients are considered (see the analysis by Kivikko et al91), the short-term effects of levosimendan on symptoms, hemodynamics, and neurohormones are accompanied to a significant long-term effect on survival. As it regards the clinical studies in the ICU field, the same pattern can be seen when comparing the large LeoPARDS study37 with the many previous smaller studies on the use of levosimendan in septic shock150: when the patients are poorly defined, the results are so spread that not any statistical significance can be reached. Therefrom originates the conundrum: in the field of ICU, the large studies needed for “evidence-based medicine” necessarily include a broad spectrum of patients and the effects of drugs can be easily masked in the statistical analyses, whereas smaller (often monocentric) studies can spot significant positive drug effects due to the more homogeneous selection of patients, but their results will remain necessarily limited. We hereby propose possible solutions for a way out.
Central to future investigations must be the identification of robust and relevant end points. An improvement in survival/mortality may be plausible in cases where levosimendan substitutes for an adrenergic inotrope with a documented propensity to increase mortality. In other settings, however, it is not obvious that a mortality gain can be assumed nor is it certain that any such gain, welcome as it would be, would be the most pertinent measurement of any treatment effect. It is, moreover, unclear how far into the future any survival benefit from a short-term intervention in what is likely to be a complex and multifaceted medical crisis should reasonably be expected to extend. None of the conventional adrenergic inotropic drugs have in fact been associated with improvements in hard end points such as mortality, and there are many indications to the contrary. The reported experience of Distelmaier et al108 (Fig. 2) is encouraging regarding the prospect of a long-term advantage in the sphere of weaning from ECMO but may not be similarly applicable in other situations and is in any case in need of corroboration.
We consider, for these reasons, that an overemphasis on crude mortality may not be the most informative approach to future clinical trials of levosimendan. We are inclined toward the position of Schumann et al,72 who have advocated the evaluation of EGDT in CS and low-cardiac output syndrome, arguing that refining the best therapeutic strategy is more constructive than trying to identify the “best” drug for hemodynamic support. Similarly, identifying the most effective regimen for, say, weaning from ECMO or the management of pulmonary hypertension needs to take a wider view of the issue than simply focusing too closely on the impact of a single intervention, perhaps delivered for a short period. The adoption of hierarchical end points in clinical trials of levosimendan in HF (eg, LEODOR; NCT03437226)151 is an innovation that may also find applications in future clinical trials in the ICU setting and may enable a more nuanced appraisal of the impact of levosimendan in those situations.
DECLARATIONS
This project did not receive any financial support. The manuscript is derived by the authors from the proceedings of a series of tutorial lectures on “Levosimendan in ICU” at the ESICM-LIVES annual congress in Vienna, Austria, on 25–26 September 2017. PP is a full-time employee of Orion Pharma. None of the other authors have conflict of interest. Editorial assistance in the preparation of this article was provided by Peter Hughes (Hughes Associates, Oxford, United Kingdom).
Footnotes
The authors report no conflicts of interest.
REFERENCES
- 1.Papp Z, Édes I, Fruhwald S, et al. Levosimendan: molecular mechanisms and clinical implications: consensus of experts on the mechanisms of action of levosimendan. Int J Cardiol. 2012;159:82–87. [DOI] [PubMed] [Google Scholar]
- 2.Nieminen MS, Fruhwald S, Heunks LM, et al. Levosimendan: current data, clinical use and future development. Heart Lung Vessel. 2013;5:227–245. [PMC free article] [PubMed] [Google Scholar]
- 3.Pollesello P, Ovaska M, Kaivola J, et al. Binding of a new Ca2+ sensitizer, levosimendan, to recombinant human cardiac troponin C. A molecular modelling, fluorescence probe, and proton nuclear magnetic resonance study. J Biol Chem. 1994;269:28584–28590. [PubMed] [Google Scholar]
- 4.Pääkkönen K, Annila A, Sorsa T, et al. Solution structure and main chain dynamics of the regulatory domain (Residues 1-91) of human cardiac troponin C. J Biol Chem. 1998;273:15633–15638. [DOI] [PubMed] [Google Scholar]
- 5.Sorsa T, Heikkinen S, Abbott MB, et al. Binding of levosimendan, a calcium sensitizer, to cardiac troponin C. J Biol Chem. 2001;276:9337–9343. [DOI] [PubMed] [Google Scholar]
- 6.Kaheinen P, Pollesello P, Levijoki J, et al. Effects of levosimendan and milrinone on oxygen consumption in isolated guinea-pig heart. J Cardiovasc Pharmacol. 2004;43:555–561. [DOI] [PubMed] [Google Scholar]
- 7.Eriksson O, Pollesello P, Haikala H. Effect of levosimendan on balance between ATP production and consumption in isolated perfused guinea-pig heart before ischemia or after reperfusion. J Cardiovasc Pharmacol. 2004;44:316–321. [DOI] [PubMed] [Google Scholar]
- 8.Ukkonen H, Saraste M, Akkila J, et al. Myocardial efficiency during calcium sensitization with levosimendan: a noninvasive study with positron emission tomography and echocardiography in healthy volunteers. Clin Pharmacol Ther. 1997;61:596–607. [DOI] [PubMed] [Google Scholar]
- 9.Ukkonen H, Saraste M, Akkila J, et al. Myocardial efficiency during levosimendan infusion in congestive heart failure. Clin Pharmacol Ther. 2000;68:522–531. [DOI] [PubMed] [Google Scholar]
- 10.Lilleberg J, Nieminen MS, Akkila J, et al. Effects of a new calcium sensitizer, levosimendan, on haemodynamics, coronary blood flow and myocardial substrate utilization early after coronary artery bypass grafting. Eur Heart J. 1998;19:660–668. [DOI] [PubMed] [Google Scholar]
- 11.Yokoshiki H, Katsube Y, Sunagawa M, et al. The novel calcium sensitizer levosimendan activates the ATP-sensitive K+ channel in rat ventricular cells. J Pharmacol Exp Ther. 1997;283:375–383. [PubMed] [Google Scholar]
- 12.Pataricza J, Krassói I, Höhn J, et al. Functional role of potassium channels in the vasodilating mechanism of levosimendan in porcine isolated coronary artery. Cardiovasc Drugs Ther. 2003;17:115–121. [DOI] [PubMed] [Google Scholar]
- 13.De Witt BJ, Ibrahim IN, Bayer E, et al. An analysis of responses to levosimendan in the pulmonary vascular bed of the cat. Anesth Analg. 2002;94:1427–1433. [DOI] [PubMed] [Google Scholar]
- 14.Gruhn N, Nielsen-Kudsk JE, Theilgaard S, et al. Coronary vasorelaxant effect of levosimendan, a new inodilator with calcium-sensitizing properties. J Cardiovasc Pharmacol. 1998;31:741–749. [DOI] [PubMed] [Google Scholar]
- 15.Kaheinen P, Pollesello P, Levijoki J, et al. Levosimendan increases diastolic coronary flow in isolated guinea-pig heart by opening ATP-sensitive potassium channels. J Cardiovasc Pharmacol. 2001;37:367–374. [DOI] [PubMed] [Google Scholar]
- 16.Erdei N, Papp Z, Pollesello P, et al. The levosimendan metabolite OR-1896 elicits vasodilation by activating the K(ATP) and BK(Ca) channels in rat isolated arterioles. Br J Pharmacol. 2006;148:696–702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Höhn J, Pataricza J, Petri A, et al. Levosimendan interacts with potassium channel blockers in human saphenous veins. Basic Clin Pharmacol Toxicol. 2004;94:271–273. [DOI] [PubMed] [Google Scholar]
- 18.Kopustinskiene DM, Pollesello P, Saris NE. Potassium-specific effects of levosimendan on heart mitochondria. Biochem Pharmacol. 2004;68:807–812. [DOI] [PubMed] [Google Scholar]
- 19.Pollesello P, Papp Z. The cardioprotective effects of levosimendan: preclinical and clinical evidence. J Cardiovasc Pharmacol. 2007;50:257–263. [DOI] [PubMed] [Google Scholar]
- 20.Tritapepe L, De Santis V, Vitale D, et al. Levosimendan pre-treatment improves outcomes in patients undergoing coronary artery bypass graft surgery. Br J Anaesth. 2009;102:198–204. [DOI] [PubMed] [Google Scholar]
- 21.Raasmaja A, Talo A, Haikala H, et al. Biochemical properties of OR-1259: a positive inotropic and vasodilatory compound with an antiarrhythmic effect. Adv Exp Med Biol. 1992;311:423. [DOI] [PubMed] [Google Scholar]
- 22.Lilleberg JM, Sundberg S, Leikola-Pelho T, et al. Hemodynamic effects of the novel cardiotonic drug simendan: echocardiographic assessment in healthy volunteers. Cardiovasc Drugs Ther. 1994;8:263–269. [DOI] [PubMed] [Google Scholar]
- 23.Mebazaa A, Nieminen MS, Filippatos GS, et al. Levosimendan vs. dobutamine: outcomes for acute heart failure patients on beta-blockers in SURVIVE. Eur J Heart Fail. 2009;11:304–311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Follath F, Cleland JG, Just H, et al. Steering Committee and Investigators of the Levosimendan Infusion versus Dobutamine (LIDO) Study. Efficacy and safety of intravenous levosimendan compared with dobutamine in severe low-output heart failure (the LIDO study): a randomised double-blind trial. Lancet. 2002;360:196–202. [DOI] [PubMed] [Google Scholar]
- 25.Moiseyev VS, Põder P, Andrejevs N, et al. ; RUSSLAN Study Investigators. Safety and efficacy of a novel calcium sensitizer, levosimendan, in patients with left ventricular failure due to an acute myocardial infarction. A randomized, placebo-controlled, double-blind study (RUSSLAN). Eur Heart J. 2002;23:1422–1432. [DOI] [PubMed] [Google Scholar]
- 26.Sanfilippo F, Knight JB, Scolletta S, et al. Levosimendan for patients with severely reduced left ventricular systolic function and/or low cardiac output syndrome undergoing cardiac surgery: a systematic review and meta-analysis. Crit Care. 2017;21:252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Guarracino F, Heringlake M, Cholley B, et al. Use of levosimendan in cardiac surgery: an update after the LEVO-CTS, CHEETAH, and LICORN trials in the light of clinical practice. J Cardiovasc Pharmacol. 2018;71:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Farmakis D, Alvarez J, Gal TB, et al. Levosimendan beyond inotropy and acute heart failure: evidence of pleiotropic effects on the heart and other organs: an expert panel position paper. Int J Cardiol. 2016;222:303–312. [DOI] [PubMed] [Google Scholar]
- 29.Balzer F, Treskatsch S, Spies C, et al. Early administration of levosimendan is associated with improved kidney function after cardiac surgery—a retrospective analysis. J Cardiothorac Surg. 2014;9:167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Alvarez J, Baluja A, Selas S, et al. A comparison of dobutamine and levosimendan on hepatic blood flow in patients with a low cardiac output state after cardiac surgery: a randomised controlled study. Anaesth Intensive Care. 2013;41:719–727. [DOI] [PubMed] [Google Scholar]
- 31.Brunner SN, Bogert NV, Schnitzbauer AA, et al. Levosimendan protects human hepatocytes from ischemia-reperfusion injury. PLoS One. 2017;12:e0187839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Gallagher KM, O’Neill S, Harrison EM, et al. Recent early clinical drug development for acute kidney injury. Expert Opin Investig Drugs. 2017;26:141–154. [DOI] [PubMed] [Google Scholar]
- 33.Varvarousi G, Xanthos T, Sarafidou P, et al. Role of levosimendan in the management of subarachnoid hemorrhage. Am J Emerg Med. 2016;34:298–306. [DOI] [PubMed] [Google Scholar]
- 34.Wang X, Li S. Effect of small-dose levosimendan on mortality rates and organ functions in Chinese elderly patients with sepsis. Clin Intervent Aging. 2017;12:917–921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Wang X, Ma S, Liu Y, et al. Effects and mechanism analysis of combined infusion by levosimendan and vasopressin on acute lung injury in rats septic shock. Cell Biochem Biophys. 2014;70:1639–1645. [DOI] [PubMed] [Google Scholar]
- 36.Belletti A, Benedetto U, Biondi-Zoccai G, et al. The effect of vasoactive drugs on mortality in patients with severe sepsis and septic shock. A network meta-analysis of randomized trials. J Crit Care. 2017;37:91–98. [DOI] [PubMed] [Google Scholar]
- 37.Gordon AC, Perkins GD, Singer M, et al. Levosimendan for the prevention of acute organ dysfunction in sepsis. N Engl J Med. 2016;375:1638–1648. [DOI] [PubMed] [Google Scholar]
- 38.Cecconi M, De Backer D, Antonelli M, et al. Consensus on circulatory shock and hemodynamic monitoring. Task Force of the European Society of Intensive Care Medicine. Intensive Care Med. 2014;40:1795–1815. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Vincent J-L, De Backer D. Circulatory shock. N Engl J Med. 2013;369:1726–1734. [DOI] [PubMed] [Google Scholar]
- 40.Ponikowski P, Voors AA, Anker SD, et al. ; ESC Scientific Document Group. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–2200. [DOI] [PubMed] [Google Scholar]
- 41.Mebazaa A, Tolppanen H, Mueller C, et al. Acute heart failure and cardiogenic shock: a multidisciplinary practical guidance. Intensive Care Med. 2016;42:147–163. [DOI] [PubMed] [Google Scholar]
- 42.Abraham WT, Adams KF, Fonarow GC, et al. ; ADHERE Scientific Advisory Committee and Investigators, ADHERE Study Group. In-hospital mortality in patients with acute decompensated heart failure requiring intravenous vasoactive medications. J Am Coll Cardiol. 2005;46:57–64. [DOI] [PubMed] [Google Scholar]
- 43.Mebazaa A, Parissis J, Porcher R, et al. Short-term survival by treatment among patients hospitalized with acute heart failure: the global ALARM-HF registry using propensity scoring methods. Intensive Care Med. 2010;37:290–301. [DOI] [PubMed] [Google Scholar]
- 44.Mebazaa A, Motiejunaite J, Gayat E, et al. ; ESC Heart Failure Long-Term Registry Investigators. Long-term safety of intravenous cardiovascular agents in acute heart failure: results from the European Society of Cardiology Heart Failure Long-Term Registry. Eur J Heart Fail. 2018;20:332–341. [DOI] [PubMed] [Google Scholar]
- 45.Tarvasmäki T, Lassus J, Varpula M, et al. ; CardShock study investigators. Current real-life use of vasopressors and inotropes in cardiogenic shock—adrenaline use is associated with excess organ injury and mortality. Crit Care. 2016;20:208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Angus DC, Barnato AE, Bell D, et al. A systematic review and meta-analysis of early goal-directed therapy for septic shock: the ARISE, ProCESS and ProMISe Investigators. Intensive Care Med. 2015;41:1549–1560. [DOI] [PubMed] [Google Scholar]
- 47.van Diepen S, Katz JN, Albert NM, et al. ; American Heart Association Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing, Council on Quality of Care and Outcomes Research; and Mission: Lifeline. Contemporary management of cardiogenic shock: a scientific statement from the American Heart Association. Circulation. 2017;136:e232–68. [DOI] [PubMed] [Google Scholar]
- 48.Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Crit Care Med. 2017;45:486–552. [DOI] [PubMed] [Google Scholar]
- 49.Heusch G. Heart rate in the pathophysiology of coronary blood flow and myocardial ischaemia: benefit from selective bradycardic agents. Br J Pharmacol. 2008;153:1589–1601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Schulz R, Rose J, Martin C, et al. Development of short-term myocardial hibernation. Its limitation by the severity of ischemia and inotropic stimulation. Circulation. 1993;88:684–695. [DOI] [PubMed] [Google Scholar]
- 51.Beohar N, Erdogan AK, Lee DC, et al. Acute heart failure syndromes and coronary perfusion. J Am Coll Cardiol. 2008;52:13–16. [DOI] [PubMed] [Google Scholar]
- 52.Duncker DJ, Koller A, Merkus D, et al. Regulation of coronary blood flow in health and ischemic heart disease. Prog Cardiovasc Dis. 2015;57:409–422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Pelliccia F, Kaski JC, Crea F, et al. Pathophysiology of takotsubo syndrome. Circulation. 2017;135:2426–2441. [DOI] [PubMed] [Google Scholar]
- 54.Rudiger A, Singer M. Mechanisms of sepsis-induced cardiac dysfunction. Crit Care Med. 2007;35:1599–1608. [DOI] [PubMed] [Google Scholar]
- 55.Tacon CL, McCaffrey J, Delaney A. Dobutamine for patients with severe heart failure: a systematic review and meta-analysis of randomised controlled trials. Intensive Care Med. 2012;38:359–367. [DOI] [PubMed] [Google Scholar]
- 56.Schmittinger CA, Torgersen C, Luckner G, et al. Adverse cardiac events during catecholamine vasopressor therapy: a prospective observational study. Intensive Care Med. 2012;38:950–958. [DOI] [PubMed] [Google Scholar]
- 57.Gheorghiade M, Follath F, Ponikowski P, et al. ; European Society of Cardiology, European Society of Intensive Care Medicine. Assessing and grading congestion in acute heart failure: a scientific statement from the acute heart failure committee of the heart failure association of the European Society of Cardiology and endorsed by the European Society of Intensive Care Medicine. Eur J Heart Fail. 2010;12:423–433. [DOI] [PubMed] [Google Scholar]
- 58.Felker GM, Benza RL, Chandler AB, et al. ; OPTIME-CHF Investigators. Heart failure etiology and response to milrinone in decompensated heart failure: results from the OPTIME-CHF study. J Am Coll Cardiol. 2003;41:997–1003. [DOI] [PubMed] [Google Scholar]
- 59.Nielsen DV, Torp-Pedersen C, Skals RK, et al. Intraoperative milrinone versus dobutamine in cardiac surgery patients: a retrospective cohort study on mortality. Crit Care. 2018;22:51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.De Backer D, Biston P, Devriendt J, et al. ; SOAP II Investigators. Comparison of dopamine and norepinephrine in the treatment of shock. N Engl J Med. 2010;362:779–789. [DOI] [PubMed] [Google Scholar]
- 61.Levy B, Perez P, Perny J, et al. Comparison of norepinephrine-dobutamine to epinephrine for hemodynamics, lactate metabolism, and organ function variables in cardiogenic shock. A prospective, randomized pilot study. Crit Care Med. 2011;39:450–455. [DOI] [PubMed] [Google Scholar]
- 62.Singer M. Catecholamine treatment for shock—equally good or bad? Lancet. 2007;370:636–637. [DOI] [PubMed] [Google Scholar]
- 63.Andreis DT, Singer M. Catecholamines for inflammatory shock: a Jekyll-and-Hyde conundrum. Intensive Care Med. 2016;42:1387–1397. [DOI] [PubMed] [Google Scholar]
- 64.Coquerel D, Sainsily X, Dumont L, et al. The apelinergic system as an alternative to catecholamines in low-output septic shock. Crit Care. 2018;22:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.He X, Su F, Taccone FS, et al. A selective V(1A) receptor agonist, selepressin, is superior to arginine vasopressin and to norepinephrine in ovine septic shock. Crit Care Med. 2016;44:23–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Khanna A, English SW, Wang XS, et al. ; ATHOS-3 Investigators. Angiotensin II for the treatment of vasodilatory shock. N Engl J Med. 2017;377:419–430. [DOI] [PubMed] [Google Scholar]
- 67.Reynold HR, Hochmann JS. Cardiogenic shock: current concepts and improving outcomes. Circulation. 2008;117:686–697. [DOI] [PubMed] [Google Scholar]
- 68.Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC), Steg PG, James SK, Atar D, et al. ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2012;33:2569–2619. [DOI] [PubMed] [Google Scholar]
- 69.García-González MJ, Domínguez-Rodríguez A, Ferrer-Hita JJ, et al. Cardiogenic shock after primary percutaneous coronary intervention: effects of levosimendan compared with dobutamine on haemodynamics. Eur J Heart Fail. 2006;8:723–728. [DOI] [PubMed] [Google Scholar]
- 70.Williams SG, Wright DJ, Tan LB. Management of cardiogenic shock complicating acute myocardial infarction: towards evidence based medical practice. Heart. 2000;83:621–626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Fuhrmann JT, Schmeisser A, Schulze MR, et al. Levosimendan is superior to enoximone in refractory cardiogenic shock complicating acute myocardial infarction. Crit Care Med. 2008;36:2257–2266. [DOI] [PubMed] [Google Scholar]
- 72.Schumann J, Henrich EC, Strobl H, et al. Inotropic agents and vasodilator strategies for the treatment of cardiogenic shock or low cardiac output syndrome. Cochrane Database Syst Rev. 2018;1:CD009669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Jörgensen K, Bech-Hanssen O, Houltz E, et al. Effects of levosimendan on left ventricular relaxation and early filling at maintained preload and afterload conditions after aortic valve replacement for aortic stenosis. Circulation. 2008;117:1075–1081. [DOI] [PubMed] [Google Scholar]
- 74.Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA. 2016;315:801–810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Beesley SJ, Weber G, Sarge T, et al. Septic cardiomyopathy. Crit Care Med. 2018;46:625–634. [DOI] [PubMed] [Google Scholar]
- 76.Suzuki T, Suzuki Y, Okuda J, et al. Sepsis-induced cardiac dysfunction and β-adrenergic blockade therapy for sepsis. J Intensive Care. 2017;5:22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Wu LL, Yang SL, Yang RC, et al. G protein and adenylate cyclase complex-mediated signal transduction in the rat heart during sepsis. Shock. 2003;19:533–537. [DOI] [PubMed] [Google Scholar]
- 78.Rudiger A. Beta-block the septic heart. Crit Care Med. 2010;38:S608–S612. [DOI] [PubMed] [Google Scholar]
- 79.Morelli A, Ertmer C, Westphal M, et al. Effect of heart rate control with esmolol on hemodynamic and clinical outcomes in patients with septic shock. JAMA. 2013;310:1683–1691. [DOI] [PubMed] [Google Scholar]
- 80.Wang Q, Yokoo H, Takashina M, et al. Anti-inflammatory profile of levosimendan in cecal ligation-induced septic mice and in lipopolysaccharide-stimulated macrophages. Crit Care Med. 2015;43:e508–20. [DOI] [PubMed] [Google Scholar]
- 81.Tsao CM, Li KY, Chen SJ, et al. Levosimendan attenuates multiple organ injury and improves survival in peritonitis-induced septic shock: studies in a rat model. Crit Care. 2014;18:652. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Morelli A, De Castro S, Teboul JL, et al. Effects of levosimendan on systemic and regional hemodynamics in septic myocardial depression. Intensive Care Med. 2005;31:638–644. [DOI] [PubMed] [Google Scholar]
- 83.Creteur J, Bouckaert Y, Mélot C, et al. Effects of levosimendan on systemic and regional hemodynamics in septic myocardial depression. Intensive Care Med. 2006;32:790; author reply 791–2. [DOI] [PubMed] [Google Scholar]
- 84.Morelli A, Donati A, Ertmer C, et al. Levosimendan for resuscitating the microcirculation in patients with septic shock: a randomized controlled study. Crit Care. 2010;14:R232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Torraco A, Carrozzo R, Piemonte F, et al. Effects of levosimendan on mitochondrial function in patients with septic shock: a randomized trial. Biochimie. 2014;102:166–173. [DOI] [PubMed] [Google Scholar]
- 86.Hajjej Z, Meddeb B, Sellami W, et al. Effects of levosimendan on cellular metabolic alterations in patients with septic shock: a randomized controlled pilot study. Shock. 2017;48:307–312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Zangrillo A, Putzu A, Monaco F, et al. Levosimendan reduces mortality in patients with severe sepsis and septic shock: a meta-analysis of randomized trials. J Crit Care. 2015;30:908–913. [DOI] [PubMed] [Google Scholar]
- 88.Guarracino F, Ferro B, Morelli A, et al. Ventriculoarterial decoupling in human septic shock. Crit Care. 2014;18:R80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Mehta RH, Leimberger JD, van Diepen S, et al. ; LEVO-CTS Investigators. Levosimendan in patients with left ventricular dysfunction undergoing cardiac surgery. N Engl J Med. 2017;376:2032–2042. [DOI] [PubMed] [Google Scholar]
- 90.du Toit EF, Genis A, Opie LH, et al. A role for the RISK pathway and K ATP channels in pre- and post-conditioning induced by levosimendan in the isolated guinea pig heart. Br J Pharmacol. 2008;154:41–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Kivikko M, Pollesello P, Tarvasmäki T, et al. Effect of baseline characteristics on mortality in the SURVIVE trial on the effect of levosimendan vs dobutamine in acute heart failure: Sub-analysis of the Finnish patients. Int J Cardiol. 2016;215:26–31. [DOI] [PubMed] [Google Scholar]
- 92.Levin R, Degrange M, Del Mazo C, et al. Preoperative levosimendan decreases mortality and the development of low cardiac output in high-risk patients with severe left ventricular dysfunction undergoing coronary artery bypass grafting with cardiopulmonary bypass. Exp Clin Cardiol. 2012;17:125–130. [PMC free article] [PubMed] [Google Scholar]
- 93.Sterba M, Banerjee A, Mudaliar Y. Prospective observational study of levosimendan and weaning of difficult-to-wean ventilator dependent intensive care patients. Crit Care Resusc. 2008;10:182–186. [PubMed] [Google Scholar]
- 94.Goligher EC, Dres M, Fan E, et al. Mechanical ventilation-induced diaphragm atrophy strongly impacts clinical outcomes. Am J Respir Crit Care Med. 2018;197:204–213. [DOI] [PubMed] [Google Scholar]
- 95.Demoule A, Molinari N, Jung B, et al. Patterns of diaphragm function in critically ill patients receiving prolonged mechanical ventilation: a prospective longitudinal study. Ann Intensive Care. 2016;6:75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Dot I, Pérez-Teran P, Samper MA, et al. Diaphragm dysfunction in mechanically ventilated patients. Arch Bronconeumol. 2017;53:150–156. [DOI] [PubMed] [Google Scholar]
- 97.Hermans G, Agten A, Testelmans D, et al. Increased duration of mechanical ventilation is associated with decreased diaphragmatic force: a prospective observational study. Crit Care. 2010;14:R127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Jung B, Moury PH, Mahul M, et al. Diaphragmatic dysfunction in patients with ICU-acquired weakness and its impact on extubation failure. Intensive Care Med. 2016;42:853–861. [DOI] [PubMed] [Google Scholar]
- 99.Tang H, Smith IJ, Hussain SN, et al. The JAK-STAT pathway is critical in ventilator-induced diaphragm dysfunction. Mol Med. 2015;20:579–589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 100.Larsson L, Friedrich O. Critical illness myopathy (CIM) and ventilator-induced diaphragm muscle dysfunction (VIDD): acquired myopathies affecting contractile proteins. Compr Physiol. 2016;7:105–111. [DOI] [PubMed] [Google Scholar]
- 101.Ottenheijm CA, Heunks LM, Sieck GC, et al. Diaphragm dysfunction in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;172:200–205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.van Hees HW, Dekhuijzen PN, Heunks LM. Levosimendan enhances force generation of diaphragm muscle from patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2009;179:41–47. [DOI] [PubMed] [Google Scholar]
- 103.van Hees HW, Andrade Acuna G, Linkels M, et al. Levosimendan improves calcium sensitivity of diaphragm muscle fibres from a rat model of heart failure. Br J Pharmacol. 2011;162:566–573. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Doorduin J, Sinderby CA, Beck J, et al. The calcium sensitizer levosimendan improves human diaphragm function. Am J Respir Crit Care Med. 2012;185:90–95. [DOI] [PubMed] [Google Scholar]
- 105.Ouanes-Besbes L, Ouanes I, Dachraoui F, et al. Weaning difficult-to-wean chronic obstructive pulmonary disease patients: a pilot study comparing initial hemodynamic effects of levosimendan and dobutamine. J Crit Care. 2011;26:15–21. [DOI] [PubMed] [Google Scholar]
- 106.Aso S, Matsui H, Fushimi K, et al. In-hospital mortality and successful weaning from venoarterial extracorporeal membrane oxygenation: analysis of 5,263 patients using a national inpatient database in Japan. Crit Care. 2016;20:80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Affronti A, di Bella I, Carino D, et al. Levosimendan may improve weaning outcomes in venoarterial ECMO patients. ASAIO J. 2013;59:554–557. [DOI] [PubMed] [Google Scholar]
- 108.Distelmaier K, Roth C, Schrutka L, et al. Beneficial effects of levosimendan on survival in patients undergoing extracorporeal membrane oxygenation after cardiovascular surgery. Br J Anaesth. 2016;117:52–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Sangalli F, Avalli L, Laratta M, et al. Effects of levosimendan on endothelial function and hemodynamics during weaning from veno-arterial extracorporeal life support. J Cardiothorac Vasc Anesth. 2016;30:1449–1453. [DOI] [PubMed] [Google Scholar]
- 110.Jacky A, Rudiger A, Krüger B, et al. Comparison of levosimendan and milrinone for ECLS weaning in patients after cardiac surgery—a retrospective before and after study. J Cardiothorac Vasc Anesth. 2018;32:2112–2119. [DOI] [PubMed] [Google Scholar]
- 111.Gordon C, Collard CD, Pan W. Intraoperative management of pulmonary hypertension and associated right heart failure. Curr Opin Anaesthesiol. 2010;23:49–56. [DOI] [PubMed] [Google Scholar]
- 112.Lahm T, McCaslin CA, Wozniak TC, et al. Medical and surgical treatment of acute right ventricular failure. J Am Coll Cardiol. 2010;56:1435–1446. [DOI] [PubMed] [Google Scholar]
- 113.Kaul TK, Fields BL. Postoperative acute refractory right ventricular failure: incidence, pathogenesis, management and prognosis. Cardiovasc Surg. 2000;8:1–9. [DOI] [PubMed] [Google Scholar]
- 114.Ochiai Y, McCarthy PM, Smedira NG, et al. Predictors of severe right ventricular failure after implantable left ventricular assist device insertion: analysis of 245 patients. Circulation. 2002;106(12 Suppl 1):I198–I202. [PubMed] [Google Scholar]
- 115.Zochios V, Parhar K, Tunnicliffe W, et al. The right ventricle in ARDS. Chest. 2017;152:181–193. [DOI] [PubMed] [Google Scholar]
- 116.Price LC, Wort SJ, Finney SJ, et al. Pulmonary vascular and right ventricular dysfunction in adult critical care: current and emerging options for management: a systematic literature review. Crit Care. 2010;14:R169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Vlahakes GJ, Turley K, Hoffman JI. The pathophysiology of failure in acute right ventricular hypertension: hemodynamic and biochemical correlations. Circulation. 1981;63:87–95. [DOI] [PubMed] [Google Scholar]
- 118.Slawsky MT, Colucci WS, Gottlieb SS, et al. Acute hemodynamic and clinical effects of levosimendan in patients with severe heart failure. Study Investigators Circ. 2000;102:2222–2227. [DOI] [PubMed] [Google Scholar]
- 119.Kerbaul F, Rondelet B, Demester JP, et al. Effects of levosimendan versus dobutamine on pressure load-induced right ventricular failure. Crit Care Med. 2006;34:2814–2819. [DOI] [PubMed] [Google Scholar]
- 120.Parissis JT, Paraskevaidis I, Bistola V, et al. Effects of levosimendan on right ventricular function in patients with advanced heart failure. Am J Cardiol. 2006;98:1489–1492. [DOI] [PubMed] [Google Scholar]
- 121.Poelzl G, Zwick RH, Grander W, et al. Safety and effectiveness of levosimendan in patients with predominant right heart failure. Herz. 2008;33:368–373. [DOI] [PubMed] [Google Scholar]
- 122.Russ MA, Prondzinsky R, Carter JM, et al. Right ventricular function in myocardial infarction complicated by cardiogenic shock: improvement with levosimendan. Crit Care Med. 2009;37:3017–3023. [DOI] [PubMed] [Google Scholar]
- 123.Morelli A, Teboul JL, Maggiore SM, et al. Effects of levosimendan on right ventricular afterload in patients with acute respiratory distress syndrome: a pilot study. Crit Care Med. 2006;34:2287–2293. [DOI] [PubMed] [Google Scholar]
- 124.Qiu J, Jia L, Hao Y, et al. Efficacy and safety of levosimendan in patients with acute right heart failure: a meta-analysis. Life Sci. 2017;184:30–36. [DOI] [PubMed] [Google Scholar]
- 125.Guerrero-Orriach JL, Ariza-Villanueva D, Florez-Vela A, et al. Cardiac, renal, and neurological benefits of preoperative levosimendan administration in patients with right ventricular dysfunction and pulmonary hypertension undergoing cardiac surgery: evaluation with two biomarkers neutrophil gelatinase-associated lipocalin and neuronal enolase. Ther Clin Risk Manag. 2016;12:623–630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126.Yilmaz MB, Grossini E, Silva Cardoso JC, et al. Renal effects of levosimendan: a consensus report. Cardiovasc Drugs Ther. 2013;27:581–590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127.Pisano A, Monti G, Landoni G. Levosimendan: new indications and evidence for reduction in perioperative mortality? Curr Opin Anaesthesiol. 2016;29:454–461. [DOI] [PubMed] [Google Scholar]
- 128.Bove T, Matteazzi A, Belletti A, et al. Beneficial impact of levosimendan in critically ill patients with or at risk for acute renal failure: a meta-analysis of randomized clinical trials. Heart Lung Vessel. 2015;7:35–46. [PMC free article] [PubMed] [Google Scholar]
- 129.Zhou C, Gong J, Chen D, et al. Levosimendan for prevention of acute kidney injury after cardiac surgery: a meta-analysis of randomized controlled trials. Am J Kidney Dis. 2016;67:408–416. [DOI] [PubMed] [Google Scholar]
- 130.Knezevic I, Poglajen G, Hrovat E, et al. The effects of levosimendan on renal function early after heart transplantation: results from a pilot randomized trial. Clin Transpl. 2014;28:1105–1111. [DOI] [PubMed] [Google Scholar]
- 131.Yilmaz MB, Yalta K, Yontar C, et al. Levosimendan improves renal function in patients with acute decompensated heart failure: comparison with dobutamine. Cardiovasc Drugs Ther. 2007;21:431–435. [DOI] [PubMed] [Google Scholar]
- 132.Hou ZQ, Sun ZX, Su CY, et al. Effect of levosimendan on estimated glomerular filtration rate in hospitalized patients with decompensated heart failure and renal dysfunction. Cardiovasc Ther. 2013;31:108–114. [DOI] [PubMed] [Google Scholar]
- 133.Zemljic G, Bunc M, Yazdanbakhsh AP, et al. Levosimendan improves renal function in patients with advanced chronic heart failure awaiting cardiac transplantation. J Card Fail. 2007;13:417–421. [DOI] [PubMed] [Google Scholar]
- 134.Silva-Cardoso J, Ferreira J, Oliveira-Soares A, et al. ; PORTLAND Investigators. Effectiveness and safety of levosimendan in clinical practice. Rev Port Cardiol. 2009;28:143–153. [PubMed] [Google Scholar]
- 135.Zangrillo A, Alvaro G, Belletti A, et al. ; CHEETAH Study Group. Effect of levosimendan on renal outcome in cardiac surgery patients with chronic kidney disease and perioperative cardiovascular dysfunction: a substudy of a multicenter randomized trial. J Cardiothorac Vasc Anesth. 2018;32:2152–2159. [DOI] [PubMed] [Google Scholar]
- 136.Redfors B, Bragadottir G, Sellgren J, et al. Dopamine increases renal oxygenation: a clinical study in post-cardiac surgery patients. Acta Anaesthesiol Scand. 2010;54:183–190. [DOI] [PubMed] [Google Scholar]
- 137.Bragadottir G, Redfors B, Ricksten SE. Effects of levosimendan on glomerular filtration rate, renal blood flow, and renal oxygenation after cardiac surgery with cardiopulmonary bypass: a randomized placebo-controlled study. Crit Care Med. 2013;41:2328–2335. [DOI] [PubMed] [Google Scholar]
- 138.Singh P, Ricksten SE, Bragadottir G, et al. Renal oxygenation and haemodynamics in acute kidney injury and chronic kidney disease. Clin Exp Pharmacol Physiol. 2013;40:138–147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139.Lannemyr L, Ricksten S-E, Rundqvist B, et al. Differential effects of levosimendan and dobutamine on glomerular filtration rate in patients with heart failure and renal impairment: a randomized double-blind controlled TrialJ. Am Heart Assoc. 2018;7:e008455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 140.Fedele F, Bruno N, Brasolin B, et al. Levosimendan improves renal function in acute decompensated heart failure: possible underlying mechanisms. Eur J Heart Fail. 2014;16:281–288. [DOI] [PubMed] [Google Scholar]
- 141.Damman K, Voors AA. Levosimendan improves renal function in acute decompensated heart failure: cause and clinical application. Editorial to: “Levosimendan improves renal function in patients with acute decompensated heart failure: comparison with dobutamine by Yilmaz et al”. Cardiovasc Drugs Ther. 2007;21:403–404. [DOI] [PubMed] [Google Scholar]
- 142.ter Maaten JM, Valente MA, Damman K, et al. Diuretic response in acute heart failure—pathophysiology, evaluation, and therapy. Nat Rev Cardiol. 2015;12:184–192. [DOI] [PubMed] [Google Scholar]
- 143.Lyon AR, Bossone E, Schneider B, et al. Current state of knowledge on Takotsubo syndrome: a Position Statement from the Taskforce on Takotsubo Syndrome of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail. 2016;18:8–27. [DOI] [PubMed] [Google Scholar]
- 144.Santoro F, Ieva R, Ferraretti A, et al. Safety and feasibility of levosimendan administration in takotsubo cardiomyopathy: a case series. Cardiovasc Ther. 2013;31:e133–7. [DOI] [PubMed] [Google Scholar]
- 145.Altenberger J, Gustafsson F, Harjola VP, et al. Levosimendan in acute and advanced heart failure: an appraisal of the clinical database and evaluation of its therapeutic applications. J Cardiovasc Pharmacol. 2018;71:129–136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 146.Landoni G, Biondi-Zoccai G, Greco M, et al. Effects of levosimendan on mortality and hospitalization. A meta-analysis of randomized controlled studies. Crit Care Med. 2012;40:634–646. [DOI] [PubMed] [Google Scholar]
- 147.Kivikko M, Lehtonen L, Colucci WS. Sustained hemodynamic effects of intravenous levosimendan. Circulation. 2003;107:81–86. [DOI] [PubMed] [Google Scholar]
- 148.Packer M, Colucci W, Fisher L, et al. ; REVIVE Heart Failure Study Group. Effect of levosimendan on the short-term clinical course of patients with acutely decompensated heart failure. JACC Heart Fail. 2013;1:103–111. [DOI] [PubMed] [Google Scholar]
- 149.Pollesello P, Parissis J, Kivikko M, et al. Levosimendan meta-analyses: is there a pattern in the effect on mortality? Int J Cardiol. 2016;209:77–83. [DOI] [PubMed] [Google Scholar]
- 150.Chang W, Xie JF, Xu JY, et al. Effect of levosimendan on mortality in severe sepsis and septic shock: a meta-analysis of randomised trials. BMJ Open. 2018;8:e019338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 151.Pölzl G, Allipour Birgani S, Comín-Colet J, et al. Repetitive levosimendan infusions for patients with advanced chronic heart failure in the vulnerable post-discharge period. ESC Heart Fail. 2018. 10.1002/ehf2.12366. [DOI] [PMC free article] [PubMed] [Google Scholar]