

Abstract
Rationale:
Pathological fracture of the mandible caused by radicular cyst is rare. This report describes a unique case of a mandibular pathological fracture caused by radicular cyst, arising from an endodontically treated molar.
Patient concern:
A 49-year-old female was referred to our department with persistent pain in left mandibular angle, accompanying with restricted mouth opening and malocclusion.
Diagnose:
An orthopantomograph (OPG) showed a unilocular lesion with a relatively well-defined border, and the lesion was associated with a fracture in the inferior border of the mandible.
Intervention:
This patient was treated through curettage of the cyst combined with open reduction and internal fixation of the fracture.
Outcomes:
At the 1-year follow-up visit, the patient did not have any complaints, and the radiographs indicated the consolidation of the fracture without recurrence of cyst.
Lessons:
This case report highlights the routine follow-up of endodontically treated teeth in order to check for apical healing and detect the cystic change at early stages.
Keywords: curettage, mandible, open reduction and internal fixation, pathological fracture, radicular cyst
1. Introduction
Pathological fractures of the mandible are defined as fractures caused by the underlying pathologic lesion in the mandible, accounting for fewer than 2% of all fractures of the mandible.[1–4] Pathological fractures usually result from regions of osteomyelitis, osteoradionecrosis, bisphosphonate-related osteonecrosis of the jaw, and idiopathic reasons, or are facilitated by cystic lesions, benign, malignant, and metastatic tumors.[1–8] Pathological fractures of the mandible associated with benign cystic lesions are relatively rare, particularly the pathological fractures arisen from radicular cysts.
This report describes a rare case of mandibular pathological fracture caused by radicular cyst in a 49-year-old female. The cyst arose from an endodontically treated mandibular second molar and resulted in a pathological fracture. The literature search indicated that this is 1 among only 5 other reported cases since 1964 in which a pathological fracture of the mandible caused by radicular cyst.[3,9,10]
2. Case report
A 49-year-old female was referred to our department with persistent pain in left mandibular angle. The patient had been experiencing this symptom for 3 months after biting on a peanut. The medical history of the patient revealed no systemic, endocrine, or metabolic disorders. On extraoral examination, no obvious abnormality was detected except restricted mouth opening. Intraoral examination revealed the malocclusion and the mandibular left first molar was restored with a crown. The patient declared that the mandibular left first and second molars were endodontically treated 5 years ago. An orthopantomograph (OPG) showed a unilocular lesion with a relatively well-defined border extending from the mandibular left second molar to the lower third molar. The dimension of the cystic lesion was 2.3 cm×1.7 cm×2.1 cm. The mandibular left third molar was horizontal impacted and its crown was located in the cystic lesion area. The lesion was associated with an obvious fracture in the inferior border of the mandible (Fig. 1). It was even more obvious by 3-dimensional computed tomography (CT). The patient was tentatively diagnosed as having a pathologic fracture in the left mandible. The medical records of the patient revealed that the patient underwent endodontic treatment because periapical inflammation in the mandibular left first and second molars 5 years ago. In addition, there was no cystic lesion in the mandibular left molars 5 years ago. The patient admitted that she had never returned to the dentist for follow-up in the past 5 years. The Ethics Committee of School and Hospital of Stomatology, Wuhan University gave approval for this case report. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Figure 1.
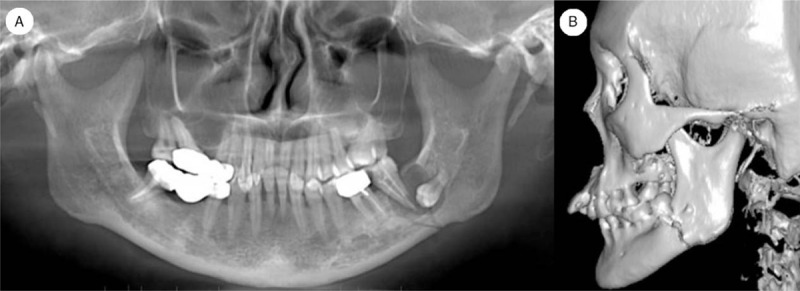
A and B, the OPG and CT show an unilocular cystic lesion in the left mandibular angle associated with pathological fracture, and the second and the first molars were endodontically treated. CT = computed tomography, OPG= orthopantomograph.
The patient underwent surgery for treatment of the cystic lesion and the fracture. Curettage of the cyst and the extraction of the third molar were performed via an intraoral approach and afterwards, open reduction and internal fixation of the fracture was carried out via an extraoral approach. The histopathology examination confirmed the cystic lesion as a radicular cyst (Fig. 2). The postoperative OPG and CT show the cavity of enucleated cyst and the internal fixation of the fractures (Fig. 3).
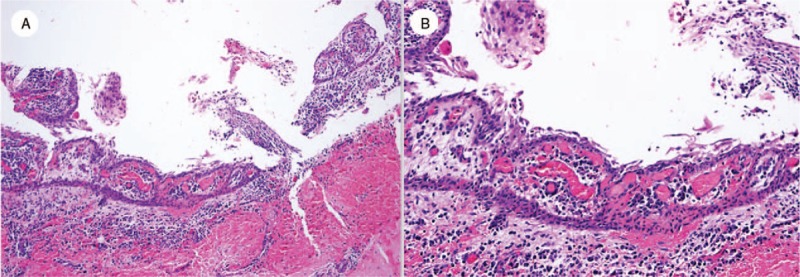
Figure 2.

A and B, the histopathologic diagnosis is radicular cyst, and the cystic lesion is lined with stratified squamous epithelium (Hematoxylin-eosin stain, original magnification ×100 in A and ×200 in B).
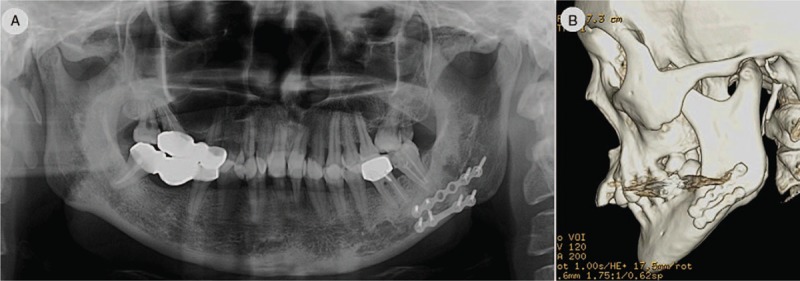
Figure 3.
A and B, the postoperative OPG and CT show the cavity of enucleated cyst and the fixation of the fractures by miniplates and screws. CT = computed tomography, OPG= orthopantomograph.
At the 4-month follow-up visit, the patient's symptoms resolved completely, and the OPG revealed that the fracture healed already, combing with bony healing in the cavity of enucleated cyst (Fig. 4). At the 1-year follow-up visit, the patient did not have any complaints, and the radiographs indicated the consolidation of the fracture without recurrence of cyst (Fig. 5).
Figure 4.

The OPG at the 4-month follow-up shows that bony union of the fracture and the bony healing in the cavity of enucleated cyst. OPG= orthopantomograph.
Figure 5.
A and B, the OPG and CT at the 1-year follow-up show the consolidation of the fracture and full bone regeneration in the cavity of enucleated cyst. CT = computed tomography, OPG= orthopantomograph.
3. Discussion
In this case, reported by us, there was no cystic lesion in the mandibular left molars 5 years ago. The patient admitted that she had never returned to the dentist for follow-up in the past 5 years. Therefore, it can be deduced that the radicular cyst was formed after the endodontic treatment. Complexity of the root canal makes it possible that the bacteria were not eradicated completely after endodontic treatment, which will lead to apical infection and even radicular cyst. A radicular cyst is an inflammatory cyst preceded by a chronic radicular granuloma and stimulation of cell rests of Malassez, partially or completely coated unkeratinized squamous epithelium in capsule.[11–13] This case highlights the routine follow-up of endodontically treated teeth in order to check for apical healing and detect cystic change at early stages.
Pathological fractures caused by cystic lesions of the jaws are less than those caused by osteoradionecrosis,[1] accordingly pathological fractures caused by radicular cyst are rare. Radicular cysts are the most common odontogenic cyst[14], accounting for approximately 70% of all cysts in the jaw. However, the incidence of pathological fracture of jaw caused by radicular cyst is very low. As an explanation, the extent of radicular cyst is usually limited. Besides, the fistula will often occur once the cyst develops to a considerable size. Therefore, patients are usually treated before the pathological fracture caused by radicular cyst. In the literature review, we found only 5 cases of radicular cysts presenting as facial fractures (Table 1).
Table 1.
Reported cases of pathological fractures caused by radicular cyst in English-language literature.

Symptoms of pathological fractures caused by radicular cysts include swelling, pain, or paresthesia. Marsden described a patient with pathological fracture presenting as swelling, pain, and ecchymosis.[9] In the case reported by Amos et al,[10] the symptoms were swelling and paresthesia. The major symptom in the case presented in this article was pain. The most prevalent site of jaw cyst is the anterior maxillary region.[15–17] However, the majority of the pathological fractures of the jaw occur in the mandible. Among the 5 cases of pathological fracture caused by radicular cyst, four cases occurred in the mandible but only 1 occurred in the maxilla. The mandible occupies a third of the lower face, and is prone to injury with protruding position, leading to a high incidence of fractures. The most common site of these pathological fractures due to radicular cysts mentioned above is the mandibular angle.
Treatment of pathological fractures can be challenging, and it may be different according to etiology.[4–7] The treatment of pathological fracture caused by radicular cyst should be determined according to the extent of the lesion. If there is sufficient bone left to buttress the fracture, open reduction and internal fixation should be performed, in association with cyst curettage or marsupialization.[1–3,18–20] When remaining healthy bone is not sufficient or it is separated by a great defect, it could be necessary to resect the involved bone region, eventually followed by immediate or secondary reconstruction.[1] Two cases reported by Gerhards et al[3] were treated with cyst curettage and internal fixation. In the case reported by Amos et al,[10] the fracture was treated conservatively with oral antibiotics considering no displacement of the fracture. In the case reported by us, only 2 teeth were involved in the radicular cyst (one of which was an impacted third molar), and the extent of the lesion was relatively small. Therefore, curettage of the cyst, open reduction and internal fixation of the fracture were performed. Radiographs showed no recurrence of cyst and complete union of the fracture 1 year after operation.
This case highlights the regular follow-up of endodontically treated teeth in order to check for apical healing and detect cystic change at early stages. Although pathological fractures caused by radicular cysts are rare, clinicians should fully anticipate their occurrence. Once the cysts are formed, they should be treated in time in order to avoid pathological fracture. With regard to the treatment of pathological fracture caused by radicular cyst, it should be determined according to the extent of lesion, and most of the patients treated with cyst curettage combined with open reduction and internal fixation can achieve a good result.
Author contributions
Conceptualization: Zhi Li and Wei Zhang.
Data curation: Xian Xiao, Jia-Wei Dai, Zhi Li, and Wei Zhang.
Formal analysis: Jia-Wei Dai, Zhi Li, and Wei Zhang.
Investigation: Xian Xiao, Zhi Li, and Wei Zhang.
Methodology: Wei Zhang.
Resources: Wei Zhang.
Writing – original draft: Xian Xiao and Jia-Wei Dai.
Writing – review & editing: Zhi Li and Wei Zhang.
Wei Zhang orcid: 0000-0001-9298-4497.
Footnotes
Abbreviations: CT = computed tomography, OPG= orthopantomograph.
Xian Xiao and Jia-Wei Dai have contributed equally to this work and are co-first authors.
The authors have no conflicts of interest to disclose.
References
- [1].Coletti D, Ord RA. Treatment rationale for pathological fractures of the mandible: a series of 44 fractures. Int J Oral Maxillofac Surg 2008;37:215–22. [DOI] [PubMed] [Google Scholar]
- [2].Choi BJ, Choi SC, Kwon YD. Aneurysmal bone cyst causing a pathologic fracture of the mandibular condyle. J Oral Maxillofac Surg 2011;69:2995–3000. [DOI] [PubMed] [Google Scholar]
- [3].Gerhards F, Kuffner HD, Wagner W. Pathological fractures of the mandible. Int J Oral Maxillofac Surg 1998;27:186–90. [DOI] [PubMed] [Google Scholar]
- [4].Boffano P, Roccia F, Gallesio C, et al. Pathological mandibular fractures: a review of the literature of the last two decades. Dent Traumatol 2013;29:185–96. [DOI] [PubMed] [Google Scholar]
- [5].Ogasawara T, Sano K, Hatsusegawa C, et al. Pathological fracture of the mandible resulting from osteomyelitis successfully treated with only intermaxillary elastic guiding. Int J Oral Maxillofac Surg 2008;37:581–3. [DOI] [PubMed] [Google Scholar]
- [6].Horta R, Monteiro D, Neto T, et al. Microsurgical reconstruction for radiation- and bisphosphonate-induced mandible osteonecrosis based on patient-specific physiopathologic mechanisms. J Craniofac Surg 2014;25:1793–6. [DOI] [PubMed] [Google Scholar]
- [7].Boffano P, Roccia F, Gallesio C, et al. Surgical management of pathologic mandibular fractures. J Craniofac Surg 2012;23:e560–2. [DOI] [PubMed] [Google Scholar]
- [8].Iizuka T, Tanner S, Berthold H. Mandibular fractures following third molar extraction. A retrospective clinical and radiological study. Int J Oral Maxillofac Surg 1997;26:338–43. [DOI] [PubMed] [Google Scholar]
- [9].Marsden J. Fracture of the mandible due to radicular and residual odontogenic cysts. Br J Oral Surg 1964;2:71–5. [DOI] [PubMed] [Google Scholar]
- [10].Amos M, Dalghous A, Alkhabuli J, et al. Massive maxillary radicular cyst presenting as facial fracture and abscess, a case report. Libyan J Med 2007;2:211–3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Daley TD, Wysocki GP, Pringle GA. Relative incidence of odontogenic tumors and oral and jaw cysts in a Canadian population. Oral Surg Oral Med Oral Pathol 1994;77:276–80. [DOI] [PubMed] [Google Scholar]
- [12].Jones AV, Craig GT, Franklin CD. Range and demographics of odontogenic cysts diagnosed in a UK population over a 30-year period. J Oral Pathol Med 2006;35:500–7. [DOI] [PubMed] [Google Scholar]
- [13].Ochsenius G, Escobar E, Godoy L, et al. Odontogenic cysts: analysis of 2,944 cases in Chile. Med Oral Patol Oral Cir Bucal 2007;12:E85–91. [PubMed] [Google Scholar]
- [14].Núñez-Urrutia S, Figueiredo R, Gay-Escoda C. Retrospective clinicopathological study of 418 odontogenic cysts. Med Oral Patol Oral Cir Bucal 2010;15:e767–73. [DOI] [PubMed] [Google Scholar]
- [15].Meningaud JP, Oprean N, Pitak-Arnnop P, et al. Odontogenic cysts: a clinical study of 695 cases. J Oral Sci 2006;48:59–62. [DOI] [PubMed] [Google Scholar]
- [16].Açikgöz A, Uzun-Bulut E, Özden B, et al. Prevalence and distribution of odontogenic and nonodontogenic cysts in a Turkish population. Med Oral Patol Oral Cir Bucal 2012;17:e108–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Avelar RL, Antunes AA, Carvalho RW, et al. Odontogenic cysts: a clinicopathological study of 507 cases. J Oral Sci 2009;51:581–6. [DOI] [PubMed] [Google Scholar]
- [18].Ezsias A, Sugar AW. Pathological fractures of the mandible: a diagnostic and treatment dilemma. Br J Oral Maxillofac Surg 1994;32:303–6. [DOI] [PubMed] [Google Scholar]
- [19].Kalantar Motamedi MH. Aneurysmal bone cysts of the jaws: clinicopathological features, radiographic evaluation and treatment analysis of 17 cases. J Craniomaxillofac Surg 1998;26:56–62. [DOI] [PubMed] [Google Scholar]
- [20].Goddard R, Patel N. Aneurysmal bone cyst masquerading as unknown mandibular metastatic deposit causing pathological fracture. Dent Update 2007;34:230–2. 234. [DOI] [PubMed] [Google Scholar]