

1. Introduction
Therapeutic communities (TCs) are residential mutual aid based programs that have been applied in the treatment of substance use disorders (De Leon, 2000; Perfas, 2012), criminal behavior (Stevens, 2013) and psychiatric disorders (Veale, Gilbert, Wheatley & Naismith, 2014). TCs for differing problems have somewhat differing structures and roots. In particular, TCs for substance use disorders, which developed in the United States in the 1950s, incorporate professional staff, are structured in a more hierarchical manner and give senior residents more responsibility and power than those for psychiatric disabilities, which developed in Britain at about the same time (Vandevelde, Broekaert, Yates & Kooyman, 2004).
Both varieties of TCs combine social support, a sense that the community as a whole is concerned with the welfare of individual members, with social learning through ongoing dialog and peer feedback on residents’ behaviors in the TC (Broekaert, Vanderplasschen, Temmerman, Ottenberg & Kaplan, 2000; De Leon, 2000; Stevens, 2013; Vandevelde, Broekaert, Yates & Kooyman, 2004). Meta-analyses have found that TC treatment reduces the likelihood of relapse in substance use disorders as well as criminal recidivism (De Leon, 2010; Malivert, Fatseas et al, 2011; Mitchell, Wilson & MacKenzie, 2012; Pearson & Lipton, 1999). However, at least one review has found that there is little evidence of TC effectiveness (Smith, Gates & Foxcroft, 2006), and the meta-analyses that have found TCs to be effective have also frequently found modest effect sizes. TC residents also frequently terminate prematurely, which is of concern given that retention is a known predictor of positive outcomes (Perryman & Dingle, 2015). Researchers have therefore in recent years given increasing attention to process studies aimed at understanding the ways in which TCs bring about change, with the hope of improving outcomes.
One process that has attracted considerable attention is identity change, drawing on the burgeoning literature on social identity and health (Haslam, Jetten, Cruwys, Dingle & Haslam, 2018). Social identity theory argues that individuals define themselves in terms of group membership; this definition, social identity, has fundamental effects on health, for good or ill (Haslam et al, 2018). A TC offers a group that is supportive of recovery, and as residents increasingly identify with the group over time they develop a recovery identity that replaces a user identity (Dingle, Stark, Cruwys and Best, 2014). Since there is increasing evidence that TCs succeed in bringing about such identity change (Best, Lubman, Savic et al, 2014; Dingle, Stark, Cruwys and Best, 2014), research on the processes by which such change might occur is of interest.
In a participant observation study of a TC for residents with substance use disorders, DeBaere, Vanheule & Inslegers (2014) find that TCs influence residents and build affect regulation by disrupting their normal routines—DeBaere et al describe this as a “frustrating environment” (pg. 255)—while offering a safe “holding environment” (pg. 256) in which previously suppressed emotions are encouraged to surface. In a later study of a TC for residents with psychiatric disorders, DeBaere, Vanheule, Van Roy, Meganck, Inslegers and Mol (2014) discuss the importance of encountering “a safe, caring and challenging Other” (pg. 5) in the TC process of change. They posit a multi-step process in which TC residents, following this encounter, engage in their individual ways of interacting with the Other, encounter the Otherness in themselves and begin to live an Other life, characterized by increased resilience, improved social relations and an increased capacity for making choices. While Debaere et al build their theory within a psychoanalytic framework, it appears to describe a change in social identity. Like social identity theory, that change comes about in the course of interactions with others.
What would a TC social network that brought about profound personal change look like? Researchers who have looked at this question have primarily focused on TC resident perceptions of social support from peers, using one of two approaches. The first is to question residents about the level of social support or quality of the environment that they perceive in the communities, without actually asking for information on specific interactions with specific peers (Carr & Ball, 2014; Edelin, Tucker, Stucky, Butler & Muelbach, 2015; Mandell, Edelin, Wenzel, Dahl & Ebener, 2008). It seems likely from these studies that TC resident perception of an orderly therapeutic environment (Carr & Ball, 2014) and trust in peers (Mandell, Edelin, Wenzel, Dahl & Ebener, 2008) predict retention. This approach looks at resident conceptions of the overall community, but does not allow the consideration of social network structure. The second approach focuses on asking individuals in treatment about their relationships with specific peers, or with groups of peers. Richardson (2002) finds that senior TC residents see themselves as having more close friends and report more satisfaction with the support they receive. This approach looks at resident conceptions of particular individuals, but again does not allow the consideration of social network structure beyond individual ties. Best, Lubman, Savic et al (2014) propose the use of a social identity map, which maps the connections between residents and the groups with which they identify, as well as connections between those groups.
There is a substantial body of social network literature that provides theoretical, experimental and field support for the idea that network clustering, the percentage of closed triads that characterize an individual’s network (Wasserman & Faust, 1994), is a powerful determinant of the influence that social networks have on individuals. A triad, not surprisingly, involves three individuals, not merely two. A closed triad exists when all three individuals are directly connected, while an open triad is missing one of those connections. Thus, if A is friends with both B and C, but B and C do not know each other, the triad is open. If A is friends with both B and C, who are friends with each other, the triad is closed. It is quite common for such triads to be closed; as the saying goes, the friend of my friend is also a friend (Malik & Mucha, 2013; Malik, Shi, Lee & Mucha, 2016).
The argument that closed triads strengthen social network support and influence originates with Simmel (1908; see also Malik et al, 2016), and has support from both experimental designs and field studies. In a web based experiment in which participants were assigned to interact in networks of varying levels of clustering, Centola (2010) found that more clustered networks were more effective in bringing about change in health behavior. Centola notes that individuals typically require contact with multiple individuals before they will adopt a behavior, describing this as a complex contagion. Field work done in Malawi confirms that the same model explains adaptation of agricultural techniques (Beaman, Ben Yishtay et al, 2018). In a classic field study, Wellman & Frank (2001) note that, “Network capital works differently than dyadic capital because in a network there may be group pressures to provide support.” (pg 135). They find that individuals who are connected to common alters—that is, whose networks show more clustering—provide more interpersonal support. Lee, Chung and Park (2016) find that individuals with denser social networks receive more social support and report higher levels of subjective well-being.
What is particularly intriguing from the point of view of TC clinical impact and previous research is that an individual whose network is highly clustered is likely to experience it as both more supportive and more influential (Kadushin, 2012). In a highly clustered network, a resident’s peers are in greater contact with one another, and are therefore in a better position to coordinate their perception of the resident’s behavior and how it might best change. This suggests that Debaere et al’s (2014) combination of support and frustration in TCs could be quantified in social network terms as network clustering, which should predict personal and identity change (Dingle, Stark, Cruwys and Best, 2014), and therefore long-term outcomes following treatment. In the current study we analyze network clustering as a predictor of reincarceration following discharge from a correctional TC.
2. Methods
2.1. Data
The use of peer affirmations for prosocial behavior is a fundamental aspect of TC treatment (De Leon, 2000). Previous research indicates that it is likely that TC residents use affirmations as a signaling mechanism to find and maintain connection with peers who are serious about working the program, a conclusion that is consistent with evolutionary cooperation theory (Skyrms, 2004; Campbell, Cranmer, Harvey & Warren, 2018). It is therefore likely that a network of affirmations also represents a network of individuals in the TC who are supporting each other in seeking positive outcomes.
The data capture the network of written affirmations exchanged between 1,312 men residing at a minimum-security community based correctional facility run as a 90 bed TC in a large Midwestern state over a period of eight years. Individual affirmations between the men were summed to create a weighted social network that included a total of 34,667 weighted edges. So, if i affirmed j twice, there would be an edge with a value of two from i to j. This constitutes an archival dataset kept by the facility for clinical purposes, and includes all men who affirmed any peer or received an affirmation from any peer.
Affirmations were recorded in several stages. If a resident wanted to affirm a peer he would write the peer’s name, the date of the affirmation and the content of the affirmation on a form provided for that purpose. A committee of senior residents and staff would then vet the affirmation for legitimacy; for instance, if the affirmation was given for supporting an emotionally distressed peer in group, they would make sure that everyone agreed that the support was given in accord with TC principles. Once the affirmation had been vetted, it was read to all community residents either at morning meeting or at a meal. It would then be entered into a database for the purposes of monitoring the ongoing clinical functioning of the community and the clinical progress of individual residents. The same process was used for all affirmations, regardless of the seniority of residents.
The TC had a maximum stay of six months, although it was possible for a resident to graduate early. It drew from a rural and suburban catchment area that consisted of eight counties. All residents were felony criminal offenders who abused substances and had chosen a sentence in treatment as an alternative to a longer sentence in prison. Treatment did not vary by substance. While the men slept in four different dormitories surrounding a common area, they mingled in groups, meals and work assignments during the day.
2.2. Variables
The outcome of interest was time to reincarceration after participants terminated the program; this data was collected from state records.
The network of affirmations allows for the development of a set of predictors. Of primary interest in this analysis is network clustering, measured as the percentage of closed triads including the participant (often referred to as the clustering coefficient in the network science literature). A closed triad is one that includes connections between each of three individuals. If i and j exchange an affirmation and j and k exchange an affirmation, a triad is closed if either i or k sends an affirmation to the other, and it is open if neither does (Wasserman & Faust, 1994). This measure is a considerable simplification, since it does not account for either the direction of the affirmations or their number. It also combines affirmations given over the length of residents’ stay. However, it is an accepted measure of network clustering (Wasserman & Faust, 1994), and is statistically tractable. It is consistent with the view that affirmations operate as a signaling mechanism, allowing TC residents to connect with and maintain connection with cooperative peers, and with the literature on network clustering as a factor in social influence (Campbell, Cranmer, Harvey & Warren, 2018; Centola, 2010; Skyrms, 2004). It was expected that residents whose networks showed more clustering—that is, a higher percentage of closed triads–would be less likely to be reincarcerated following discharge from the TC.
The number of peers who eventually graduated from the TC who directly affirmed each resident was included as a control variable, as was the number of peers who eventually graduated who indirectly affirmed each resident at two-degrees of separation, because these variables had been found to predict the proximal outcome of graduation in a previous study (Campbell, Cranmer, Harvey & Warren, 2018). That is, if i affirms j and j affirms k, j has received one direct affirmation and k has received one direct affirmation and one indirect affirmation. We also controlled for eigenvector centrality, the extent to which peers who affirmed a resident had also been affirmed by well-connected peers (Wasserman & Faust, 1994). We added this as a control for connectedness to highly popular nodes that may be informational hubs. Finally, we controlled for the total number of affirmations that residents received from peers who eventually graduated; this is different from the total number of peers who affirmed a given resident, since one peer could affirm the resident several times. This controls for the role of affirmations as positive reinforcement for prosocial behavior. Each affirmation offers positive reinforcement, whereas the number of individuals from whom one receives affirmations is a measure of the presence of a network of individuals with whom one is cooperating (Campbell, Cranmer, Harvey & Warren, 2018).
Apart from network variables, age, race and the number of days spent in treatment were included as outcome predictors (Bonta & Andrews, 2016; Condelli & Hubbard, 1994). Number of days in treatment was used rather than successful graduation because it is a more precise indicator of the amount of time which residents had to form relationships, affirm peers, and receive affirmations from peers. Further, Condelli & Hubbard (1994) and Linley & Warren (under review) showed that time in treatment predicts both outcomes and interpersonal helping behavior following termination from TCs. To ensure the models specified met the proportional hazards assumption for survival analysis, we took natural logarithms of age and days in the program. The TC in question also kept scores on the Level of Service Inventory-Revised (LSI-R) (Andrews & Bonta, 1994), a needs-based instrument that can also serve as a predictor of recidivism. However, including the Level of Service Industry-Revised (LSI-R) score for each resident created violations of the proportional hazards assumption and did not alter the significance of the clustering predictor; we thus excluded LSI-R from the feature model specification.
2.3. Modeling strategy
Regression-based statistical analysis assumes that observations are conditionally independently and identically distributed (i.i.d.); conditioned upon the proper specification of covariates, it is assumed that individuals represented in the data set do not interact with each other and therefore do not influence each other in any way. Any data set drawn from a TC will violate this assumption. As mentioned above, TC treatment, based on mutual aid, is based on exactly the idea that peers interacting will affect each other’s behavior (Hawkins & Wacker, 1986; De Leon, 2000; Perfas, 2012; Stevens, 2013). The principal of TC treatment is diametrically opposed to the principal of i.i.d. As a consequence, if we were to apply traditional regression analysis to the TC data, the likelihood that is maximized will be arbitrarily biased (Cranmer and Desmarais, 2016; Cranmer et al, 2017).
From the substantive point of view of TC clinical theory, treating data from a sample of TC residents as i.i.d. ignores the peer-to-peer interactions that give rise to clinical change. In order to assess the role of the social network of peer affirmations in predicting TC resident outcomes we therefore use a network based statistical model, the Temporal Network Autocorrelation Model (TNAM) (Liefeld & Cranmer, 2016). The TNAM generalizes previous statistical work on spatial autocorrelation to networks, allowing the inclusion of network position as a predictor of outcomes, while also allowing the incorporation of exogenous variables, such as age or race, as predictors of outcomes within a variety of models, including generalized linear models (Liefeld & Cranmer, 2016). The analysis presented here makes a novel methodological contribution by deriving a TNAM-based semiparametric Cox survival model. This new model allows us to test the relationship of network position and reincarceration following termination from the TC. To account for any individual level variation that may make some residents more prone to reincarceration than others, a participant-level frailty term is used. These terms, introduced by Clayton (1978) and Vaupel et al. (1979) and discussed by Box-Steffensmeier and De Boef (2006), account for unit-to-unit based variation and confounding and are commonplace in survival analysis (Box-Steffensmeier and Jones, 2004). Thus, while we do not include individual LSI-R scores (Andrews & Bonta, 1994) in the model, the frailty term should account for possible omitted variable bias.
3. Results
3.1. Descriptive statistics
During the period of observation, 80.7% of residents graduated from the TC. Roughly 49% of all participants were reincarcerated over the course of the eight year censored observation period. 85% of all residents were of European-American descent. Descriptive statistics for continuous variables can be found in Table 1. For those participants who were reincarcerated, time until reincarceration or censoring varies greatly, from 7 days through 2978 days, with a mean of 801.482 days. Roughly 16.8% of all triads are closed, but the range per participant extended from 0 (no triads were closed) to 100% (all triads were closed). The mean number of successful peers who directly affirmed each participant is 14.66, while the range was from 0–65. The mean number of successful peers who indirectly affirmed each participant is 34.08, with a range of 0 to 95. The mean duration of stay in logged days was 4.961, with a range of 2.708 to 5.193 and a standard deviation of 0.340. Graphs of the distributions of all variables can be found in Figure 1.
Table 1.
Descriptive Statistics for All Variables Included in Any Model Fit.
| Variable | Minimum | Maximum | Mean | Standard Deviation |
|---|---|---|---|---|
| Graduation | 0 | 1 | 0.807 | 0.395 |
| Recidivism | 0 | 1 | 0.491 | 0.500 |
| Gap Time (Days) | 7 | 2978 | 801.482 | 770.699 |
| Log Age | 2.890 | 3.091 | 3.329 | 0.289 |
| Log Days | 2.708 | 5.193 | 4.961 | 0.340 |
| Race | 0 | 1 | 0.151 | 0.358 |
| Peers Directly Affirming |
0 | 65 | 14.662 | 11.899 |
| Peers Indirectly Affirming |
0 | 95 | 34.079 | 11.590 |
| Weighted Affirmations |
0 | 186 | 22.408 | 23.172 |
| Eigenvector Centrality |
0.00 | 0.218 | 0.009 | 0.025 |
| Clustering Coefficient |
0 | 1 | 0.168 | 0.098 |
Figure 1. Distributions for All Variables Included in Any Model Fit.

Density plots are used for continuous variables; bar plots are used for dichotomous variables.
3.2. Modeling results
The Cox model was fit using forward entry. Results are displayed in Table 2, which includes model coefficients and standard error for each variable in successive models along with the Akaike Information Criteria (AIC) and Therneau-Grambusch proportional hazard (PH) test for each successive model (Grambsch and Therneau, 1994). Lower values of the AIC indicate better model fit, while a PH value below .10 suggests that the model violates the proportional hazards assumption (Box-Steffensmeier and Jones, 2004). The individual level covariates, log-age, race and log-days in treatment, are entered first. As the log-age of a TC resident increases, the hazard for reincarceration decreases; that is, older residents are less likely to be reincarcerated following termination (b = −0.89, se = .24 in Model 7, with good comparative model fit as measured by the AIC (8448.71) and no indication of proportional hazards violations (PH = 0.12), (b = −0.89, se = .24). As log-days spent in treatment increases, the hazard function for reincarceration decreases (b = −2.59, se = .20, again in Model 7). As residents spend longer in treatment they are less likely to be reincarcerated after release. This finding is also significant at any conventional threshold in all models. Race is not statistically significantly related to the hazard function for reincarceration.
Table 2.
Cox TNAM Model Results.
| Model 1 |
Model 2 |
Model 3 |
Model 4 |
Model 5 |
Model 6 |
Model 7 |
Model 8 |
|
|---|---|---|---|---|---|---|---|---|
| Age | −0.48*** | −0.48*** | −1.03*** | −0.91*** | −0.87*** | −0.88*** | −0.89*** | −0.89*** |
| (0.17) | (0.17) | (0.24) | (0.24) | (0.24) | (0.24) | (0.24) | (0.24) | |
| Black | −0.08 | −0.17 | −0.17 | −0.21 | −0.21 | −0.20 | −0.20 | |
| (0.13) | (0.18) | (0.18) | (0.18) | (0.18) | (0.18) | (0.18) | ||
| Days | −2.66*** | −2.77*** | −2.68*** | −2.60*** | −2.59*** | −2.59*** | ||
| (0.18) | (0.19) | (0.19) | (0.20) | (0.20) | (0.20) | |||
| Clustering Coefficient | −1.39* | −2.38** | −2.37** | −2.38** | −2.37** | |||
| (0.69) | (0.74) | (0.74) | (0.75) | (0.75) | ||||
| Peers Directly Affirming | −0.02*** | −0.01 | −0.01 | |||||
| (0.01) | (0.01) | (0.01) | ||||||
| Peers Indirectly Affirming | −0.01 | −0.01 | −0.01* | |||||
| (0.01) | (0.01) | (0.01) | ||||||
| Eigenvector Centrality | 1.86 | 1.84 | ||||||
| (3.11) | (3.13) | |||||||
| Weighted Affirmations | −0.01 | |||||||
| (0.00) | ||||||||
| AIC | 8663.20 | 8663.64 | 8478.69 | 8474.47 | 8455.02 | 8447.70 | 8448.71 | 8449.42 |
| R2 | 0.33 | 0.33 | 0.71 | 0.71 | 0.71 | 0.71 | 0.71 | 0.71 |
| Max. R2 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| Num. events | 644 | 644 | 644 | 644 | 644 | 644 | 644 | 644 |
| Num. obs. | 1312 | 1312 | 1312 | 1312 | 1312 | 1312 | 1312 | 1312 |
| Missings | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| PH test | 0.34 | 0.14 | 0.03 | 0.06 | 0.08 | 0.07 | 0.12 | 0.08 |
p < 0.001
p < 0.01
p < 0.05
When first entered in Model 4, an increase in triadic closure reduces the hazard of reincarceration, a finding that is statistically significant at the p = .05 level (b = −1.39, se = 0.69). Following the introduction of the number of successful peers who directly affirm ego in model 5, the relationship grows stronger (b = −2.38, se = 0.74) and remains effectively unchanged as further variables are entered into the model. This supports the hypothesis that residents whose networks are more highly clustered are at lower hazard of reincarceration. In practical terms, a one standard deviation increase in the clustering coefficient above the mean while holding all other variables at their mean or median increases the probability of remaining free from incarceration after one year from .55 (95% CI = .51–.59) to .62 (95% CI = .56–.69), while a two standard deviation increase increases the probability to 69 (95% CI = .59–.79). Figure 2 shows the predicted probability of remaining free of incarceration at the end of one year as a function of the clustering coefficient. As the clustering coefficient increases the likelihood of remaining free of incarceration at the end of one year also increases, from 42% if no triads are closed to roughly 93% if all triads are closed.
Figure 2. Predicted Probability Curve, Clustering Coefficient, Model 7.
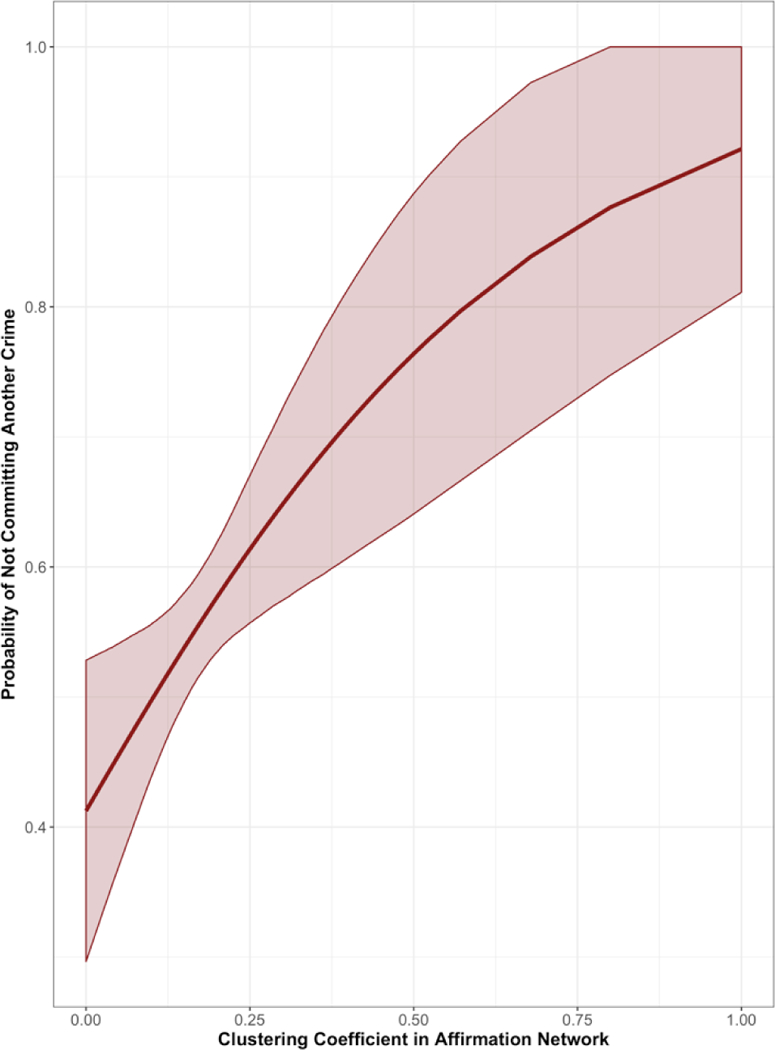
Predicted probability of not committing another crime after a year of leaving the TC over the full range of values for a member’s local Affirmations Network Clustering Coefficient. All other binary or continuous variables are held at their modal or average values respectively. Probabilities based on results from Model 7.
The relationship between the variable number of successful peers who directly affirm ego and the hazard of reincarceration is negative and statistically significant when added to the model (b = −0.02, se = 0.01). Once the variable number of successful peers who indirectly affirm ego is added to the model, neither direct nor indirect successful peers who affirms are statistically significant (b = −0.01, se = 0.01). Eigenvector centrality is not statistically significant (b = 1.86, se = 3.11), nor is the total number of affirmations received from peers (b = −.01, se = 0.00). When the variable number of successful peers who directly affirm ego is removed from the model, the number of successful peers who indirectly affirm ego statistically significantly predicts the hazard of reincarceration (b = −0.01, se − 0.01).
4. Discussion
In this study, those participants with more clustered networks had a substantially lower hazard of reincarceration. While both age and days in treatment are themselves predictive of reincarceration, they do not account for this difference. Both the number of successful peers who directly and indirectly affirm participants act as confounders. This appears to be a result of network structure. If more peers affirm a resident there are more possible triads to close, while at least some indirect affirmations from peers close triads. Both direct and indirect affirmations reduce the hazard of reincarceration when entered individually but do not do so when entered together. Given that there must be a direct affirmation before indirect affirmations are possible, this complex relationship may stem from multicollinearity (Mills, 2011; Wasserman & Faust, 1994).
This study has at least two limitations. The first is that only one type of edge, the exchange of written affirmations, is used. The second is that it only uses data from one TC. Replication at other sites with other measures would be useful in furthering our understanding of the relationship between resident social networks and TC outcomes. Replication at TCs which serve women would be particularly useful, since it is known that the networks of women typically include a higher percentage of closed triads than those of men (Kadushin, 2012).
Despite these limitations, the results have implications for TC clinical theory as well as TC research. Most obviously, they offer quantitative confirmation for the earlier qualitative findings on the importance of close peer relations in TCs (DeBaere, Vanheule, Van Roy, Meganck, Inslegers & Mol, 2014; DeBaere, Vanheule & Inslegers, 2014; Stevens, 2013) as well as the more general TC clinical principle that the community of peers is itself an effective method of treatment (De Leon, 2000). Given the difference in status between professional staff and residents, along with the considerably larger numbers of residents at any TC, only peers can form the dense network clusters that predict success in this study.
Somewhat less obviously, these findings should encourage us to rethink the role of peer feedback in TCs. Because TC theory emphasizes social learning, it is natural to think of peer affirmations as positive reinforcement for prosocial behavior. But this role, which they doubtless do perform, does not explain why the percentage of closed triads in a network of affirmations should predict reincarceration. Further, the number of affirmations that residents receive from peers does not predict reincarceration, whereas the number of peers who send affirmations, their eventual graduation status and the extent to which those peers are connected does. It seems likely, therefore, that the affirmation network reflects a latent cooperative network; residents use affirmations to signal cooperative peers and thereby arrange and maintain clusters of peers who work together in achieving TC goals of sobriety, right living and identity change. This constitutes network cooperation (Gallo & Yan, 2015; Rand & Nowak, 2013; Skyrms, 2004).
The possibility that tightly bound cliques may reinforce negative behavior and thereby undermine treatment effectiveness is a traditional concern of TC clinicians (Deleon, 2000). But qualitative studies have found that TC residents see close and reciprocal relationships with others as fundamental to their process of personal change (Miller, Sees and Brown, 2006; Stevens, 2013). Recent social network studies also lend credence to the idea that groups of TC residents may work together because they trust each other and support each other towards program success (Doogan & Warren, 2017; Campbell, Cranmer, Harvey & Warren, 2018). The current study adds to the growing body of findings indicating that tightly bound groups in TCs can improve resident outcomes. While a longstanding clinical concern should not be lightly dismissed, it might be more productive for both researchers and clinicians to begin to define the situations in which cliques are either productive or counterproductive. For instance, social identity theory suggests that lasting recovery from substance use disorder arises from identity change that is contingent on interaction with peers who are also committed to recovery (Haslam et al, 2018). It is also possible that whether or not a resident is a member of a clique in the sense of TC clinical theory (De Leon, 2000) depends on the number of closed triads in his social network. Perhaps one closed triad indicates a clique, while three or four indicate that the resident is part of multiple connected groups of individuals who hold each other accountable to TC standards of behavior.
The results in this study go beyond current social identity findings, and most other findings that apply social network ideas to recovery from substance use, in an important way by demonstrating the vital significance of indirect ties. This constitutes a conundrum for both TC residents and clinicians. Of those variables that negatively correlate with the hazard of reincarceration in all models, residents can control the length of time they spend in the TC. They obviously cannot control their age. But they also cannot completely control the level of triad closure in their networks, since one link in the triad is between two peers. Residents also cannot control who affirms them; they can simply engage in prosocial actions. Success in TCs is therefore to some extent a function of the actions of others. (See also Campbell, Cranmer, Harvey & Warren, 2018.) This suggests that it is important for clinicians to cultivate interpersonal helping relationships across the community as a whole so as to create a positive unit environment. This is known to influence retention (Carr & Ball, 2014; Edelin, Tucker, Stucky, Butler & Muelbach, 2015; Mandell, Edelin, Wenzel, Dahl & Ebener, 2008). This study goes one step further in that triad closure predicts a distal outcome, reincarceration, and not simply the proximal outcome of retention. In light of this current study, it might be reasonable to help new TC residents form relationships with groups of peers who are actively exchanging mutual aid in accord with TC principles. The ability to form such relationships may be an important individual level predictor of clinical outcomes.
On the level of the TC as a whole, TC clinical researchers have recently begun to discuss the possibility that adding psychoeducational groups to TC programming can have the problematic side effect of eroding the time in which TC residents work together in formal or informal ways, thereby forging relationships and learning from their interactions (Yates, Burns & McCabe, 2017). This study adds weight to that concern. To the extent that network clustering predicts outcomes, residents will need time to build the clusters.
TC clinicians and researchers could also give attention to interventions that attempt to establish clustered networks that encourage prosocial behavior among residents, and it is worth considering interventions meant to improve TC functioning in social network terms. For instance, the British Phoenix Futures TC engages its residents in a program of outdoor projects known as Recovery Through Nature (Aslan, 2016). Qualitative analysis suggests that residents value both the exposure to nature and the relationships which form over the course of the projects (Aslan, 2016). There has at this point been no study of the structure of the social networks that residents form in the course of this program.
The finding that network structure predicts reincarceration has other implications for TC researchers. While some meta-analyses and systematic reviews have found that TC treatment is effective for both substance use disorders and criminal behavior (Mitchell, Wilson & McKenzie, 2012; Lees, Manning & Rawlings, 2004) others have not (Smith, Gates & Foxcroft, 2006) or have found benefits in the short term that are uncertain in the long term (Malivert, Fatseas, Denis, Langlois & Auriacombe, 2011). At the same time, predictors of distal outcomes following TC treatment have remained few and far between; graduation (De Leon, Wexler & Jainchill, 1982) and length of stay (Condelli & Hubbard, 1994; Hubbard, Craddock, & Anderson 2003; Toumbourou, Hamilton & Fallon, 1998) are the two for which we have the best evidence, while researchers have recently turned their attention to identity change (Dingle, Stark, Cruwys & Best, 2015). One reason that few distal outcome predictors have been found may be that some reside in the broader social network that TC residents form, rather than in individual characteristics or even dyadic interactions. Moreover, to the extent that network structure predicts outcomes, failure to include social network predictors is likely to introduce omitted variable bias that can obscure the predictive value of other variables and of TC treatment itself.
5. Conclusion
TC clinicians have long claimed that the community itself is the method of treatment. This study adds quantitative support and nuance to that idea. The finding that resident clustering predicts outcomes following termination from the TC means that a simple model in which TC residents deliver clinical treatment to peers in the form of peer feedback is inadequate to capture the clinical process of these programs. It also implies that those social support constructs which presume direct contact between the giver of support and the recipient are not sufficient to understand TC clinical processes. Indirect contacts also matter, and the structure of those contacts matters. Further analyses of the way in which TCs influence residents should work toward a more detailed understanding of the processes that go into successful interpersonal helping and the interventions by which clinicians can foster successful groupings among TC residents.
Highlights:
Social network analysis of predictors of reincarceration following discharge from therapeutic communities (TCs).
Analysis conducting using the temporal network autocorrelation model (TNAM) applied to a network of 34,667 edges consisting of affirmations exchanged between 1,312 male TC residents.
Clustering in resident networks measured by percentage of closed triads.
TC residents whose social networks show more clustering have a lower hazard of reincarceration.
This is true when controlling for age, length of stay, graduation of peers with whom they are linked in the network and race.
Acknowledgments
This research was supported by grants 1R21DA023474 - 01A2 and 1R34DA043079-01A1 from the National Institute on Drug Abuse. The authors would also like to express their gratitude for helpful discussions with Carole Harvey, David Best and Rowdy Yates.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Arai S & Nicolaides C (2017). Exercise contagion in a global social network. Nature Communications, 8, Article Number 14753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Andrews DA, & Bonta J (1995). The level of service inventory-revised [User manual] Toronto, Canada: Multi-Health Systems, Inc. [Google Scholar]
- Best D, Lubman DI, Savic M, Wilson A, Dingle G, Haslam SA, Haslam C & Jetten J (2014). Social and transitional identity: exploring social networks and their significance in a therapeutic community setting. Therapeutic Communities, 35(1), 10–20. [Google Scholar]
- Bonta J & Andrews DA (2016). The psychology of criminal conduct (6th ed.). Routledge: Abingdon-on-Thames, United Kingdom. [Google Scholar]
- Box-Steffensmeier JM & De Boef S (2006). Repeated events survival models: the conditional frailty model. Statistics in Medicine, 25(20), 3518–3533. [DOI] [PubMed] [Google Scholar]
- Box-Steffensmeier JM & Jones BS (2004). Event history modeling: A guide for social scientists Cambridge: Cambridge University Press. [Google Scholar]
- Broekaert E, Vanderplasschen W, Temmerman I, Ottenberg DJ & Kaplan C (2000). Retrospective study of similarities and relations between American drug-free therapeutic communities and European therapeutic communities for children and adults. Journal of Psychoactive Drugs, 32(4), 407–417. [DOI] [PubMed] [Google Scholar]
- Campbell BW, Cranmer S, Harvey C & Warren K (2018). Therapeutic community graduates cluster together in social networks: Evidence for spatial selection as a cooperative mechanism in therapeutic communities. Addictive Behaviors, 79, 74–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carr WA, & Ball SA (2014). Predictors and treatment outcomes of perceived ward atmosphere among therapeutic community residents. Journal of Substance Abuse Treatment, 46(5), 567–573. [DOI] [PubMed] [Google Scholar]
- Clayton DG (1978). A model for association in bivariate life tables and its application in epidemiological studies of familial tendency in chronic disease incidence. Biometrika, 65(1), 141–151. [Google Scholar]
- Condelli WS, & Hubbard RL (1994). Relationship between time spent in treatment and client outcomes from therapeutic communities. Journal of Substance Abuse Treatment, 11(1), 25–33. [DOI] [PubMed] [Google Scholar]
- Cranmer SJ & Desmarais BA (2016). A Critique of Dyadic Design. International Studies Quarterly, 60(2), 355–362. [Google Scholar]
- Cranmer SJ, Leifeld P, McClurg S, & Rolfe M. (2017). Navigating the Range of Statistical Tools for Inferential Network Analysis. American Journal of Political Science, 61(1), 247–251. [Google Scholar]
- Debaere V, Vanheule S & Inslegers R (2014). Beyond the “black box” of the Therapeutic Community for substance abusers: A participant observation study on the treatment process. Addiction Research and Theory, 22(3), 251–262. [Google Scholar]
- Debaere V, Vanheule S, Van Roy K, Meganck R, Inslegers R & Mol M (2014). Changing encounters with the other: A focus group study on the process of change in a therapeutic community. Psychoanalytic Psychology, 33(3), 406–419. [Google Scholar]
- De Leon G (2000). The Therapeutic Community: Theory, Model, and Method New York, NY: Springer Publishing Co. [Google Scholar]
- De Leon G, Wexler H & Jainchill N (1982). The therapeutic community: Success and improvement rates 5 years after treatment. The International Journal of the Addictions, 17(4), 703–747. [DOI] [PubMed] [Google Scholar]
- Dingle GA, Stark C, Cruwys T, & Best D (2015). Breaking good: Breaking ties with social groups may be good for recovery from substance misuse. British Journal of Social Psychology, 54(2), 236–254. [DOI] [PubMed] [Google Scholar]
- Edelin MO, Tucker JS, Stucky BD, Butler J & Muehlbach B (2015). Developing an assessment of the adolescent therapeutic community treatment process via client report. Journal of Child & Adolescent Substance Abuse, 24(5), 274–281. [Google Scholar]
- Grambsch PM & Therneau TM (1994). Proportional hazards tests and diagnostics based on weighted residuals. Biometrika, 81(3), 515–526. [Google Scholar]
- Haslam C, Jetten J, Cruwys T, Dingle GA & Haslam SA (2018). The New Psychology of Health: Unlocking the Social Cure New York: Routledge. [Google Scholar]
- Hawkins JD & Wacker N (1986). Side bets and secondary adjustments in therapeutic communities. In De Leon G & Ziegenfuss JT (Eds.), Therapeutic communities for addictions: Readings in theory, research and practice (pp. 141–155). Springfield, Illinois: Charles C. Thomas. [Google Scholar]
- Hubbard RL, Craddock SG, & Anderson J (2003). Overview of 5-year followup outcomes in the Drug Abuse Treatment Outcome Studies (DATOS). Journal of Substance Abuse Treatment, 25(3), 125–134. [DOI] [PubMed] [Google Scholar]
- Kadushin C (2012). Understanding Social Networks: Theories, Concepts and Findings New York, NY: Oxford University Press. [Google Scholar]
- Lee S, Chung JE & Park N (2016). Linking cultural capital with subjective well-being and social support: The role of communication networks. Social Science Computer Review, 34(2), pgs 172–196. [Google Scholar]
- Lees J, Manning N, & Rawlings B (2004). A culture of enquiry: Research evidence and the therapeutic community. Psychiatric Quarterly, 75(3), 279–293. [DOI] [PubMed] [Google Scholar]
- Leifeld P & Cranmer S (2016). A theoretical and empirical comparison of the temporal exponential random graph model and the stochastic actor-oriented model. arXiv Available at https://arxiv.org/pdf/1506.06696.pdf.
- Malik N & Mucha PJ (2013). Role of social environment and social clustering in spread of opinions in coevolving networks. Chaos, 23(4), 043123–1–043123–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malik N, Shi F, Lee H & Mucha PJ (2016). Transitivity reinforcement in the coevolving voter model. Chaos, 26(12), 123112–1–123112–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malivert M, Fatséas M, Denis C, Langlois E, & Auriacombe M (2011). Effectiveness of therapeutic communities: A systematic review. European Addiction Research, 18(1), 1–11. [DOI] [PubMed] [Google Scholar]
- Mandell W, Edelen MO, Wenzel SL, Dahl J, & Ebener P (2008). Do dimensions of therapeutic community treatment predict retention and outcomes? Journal of Substance Abuse Treatment, 35(3), 223–231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitchell O, Wilson D and Layton MacKenzie D (2012). The Effectiveness of Incarceration-Based Drug Treatment on Criminal Behavior [Online] Available from: http://www.thehealthwell.info/node/308898 [Accessed: 4th June 2018]
- Perfas F (2012). Deconstructing the therapeutic community: A practice guide for addiction professionals Red Hook, NY: Hexagram Publishing. [Google Scholar]
- Richardson L (2002). Substance abusers’ friendships and social support networks in the therapeutic community. Therapeutic Communities, 23(2), 85–103. [Google Scholar]
- Skyrms B (2004). The Stag Hunt and the Evolution of Social Structure Cambridge, England: Cambridge University Press. [Google Scholar]
- Smith LA, Gates S, & Foxcroft D (2006). Therapeutic communities for substance related disorder. Cochrane Database of Systematic Reviews 2006, Issue 1. [DOI] [PubMed] [Google Scholar]
- Stevens A (2013). Offender rehabilitation and therapeutic communities: Enabling change the TC way New York, NY: Routledge. [Google Scholar]
- Toumbourou J, Hamilton M, & Fallon B (1998). Treatment level progress and time spent in treatment in the prediction of outcomes following drug-free therapeutic community treatment. Addiction, 93(7), 1051–1064 [DOI] [PubMed] [Google Scholar]
- Vandevelde S, Broekaert E, Yates R, & Kooyman M (2004). The development of the therapeutic community in correctional establishments: A comparative retrospective account of the ‘democratic’ Maxwell Jones TC and the hierarchical concept-based TC in prison. International Journal of Social Psychiatry, 50(1), 66–79. [DOI] [PubMed] [Google Scholar]
- Veale D, Gilbert P, Wheatley J & Naismith I (2014). A new therapeutic community: Development of a compassion-focussed and contextual behavioural environment. Clinical Psychology and Psychotherapy, 22(4), 285–303. [DOI] [PubMed] [Google Scholar]
- Vaupel JW, Manton KG, & Stallard E (1979). The impact of heterogeneity in individual frailty on the dynamics of mortality. Demography, 16(3), 439–454. [PubMed] [Google Scholar]
- Wasserman S, & Faust K (1994). Social network analysis: Methods and applications New York, NY: Cambridge University Press. [Google Scholar]
- Wellman B & Frank K (2001). Network capital in a multi-level world: Getting support from personal communities. In Lin N, Burt R & Cook K (eds.), Social Capital: Theory and Research Chicago: Aldine de Gruyter, pgs. 233–274. [Google Scholar]
- Yates R, Burns J & McCabe L (2017). Integration: Too much of a bad thing? Journal of Groups in Addiction & Recovery, 12(2–3), 196–206. [Google Scholar]