

Supplemental Digital Content is available in the text
Keywords: diabetes mellitus, lixisenatide, meta-analysis, review
Abstract
Objective:
We aimed to systematically evaluate the efficacy and safety of lixisenatide in patients with type 2 diabetes mellitus.
Methods:
PubMed, EMBASE, Cochrane Library, ClinicalTrials.gov, Google, Web of Science and the Chinese Science Citation Database were searched up to March 2018. Randomized controlled trials determining the efficacy and safety of lixisenatide in patients with type 2 diabetes mellitus were eligible for inclusion. Two authors independently extracted the data in a prespecified Microsoft Excel spreadsheet. A meta-analysis was performed using Review Manager 5.3 software. Weighted mean difference (WMD) and relative risk (RR) together with their corresponding 95% confidence intervals (CIs) were estimated, and only the random effects model was used in order to achieve a more conservative estimate of the efficacy and safety.
Results:
Fourteen multicenter randomized controlled trials involving 11,947 patients were eligible for inclusion. Compared to placebo, lixisenatide could more significantly reduce the level of HbA1c (WMD=-0.44; 95% confidence interval [CI] [-0.55,-0.33]), and a higher proportion of lixisenatide-treated patients achieved the HbA1c level of < 7.0% (RR = 1.89, 95% CI [1.75–2.03]) and < 6.5% (RR = 3.03, 95% CI [2.54–3.63]) than the placebo-treated patients. Lixisenatide was also associated with a significant reduction in fasting plasma glucose and 2-hour postprandial plasma glucose levels. The risks for any adverse events, gastrointestinal adverse events, and symptomatic hypoglycemia significantly increased in the lixisenatide-treatedment group compared to those in the placebo group. However, lixisenatideit did not increase the risks of serious adverse events, death, or severe hypoglycemia.
Conclusions:
Lixisenatide was more effective than placebo in patients with type 2 diabetes mellitus, and the mild-to-moderate adverse events were found to be tolerated during the follow-up.
1. Introduction
Diabetes mellitus is one of the leading causes of disability and death worldwide .[1] Currently, there are 425 million people living with diabetes, and the number will increase to 629 million in 2045 .[2] According to the International Diabetes Federation, 3 quarters of the people with diabetes live in low- and middle-income countries. It has the highest number of people with diabetes in the world, with a prevalence of 9.1%. Further, diabetes accounts for 2% of the global health expenditure.[2]
Although a variety of lifestyle and pathophysiological approaches are now available for the management of diabetes, because of the progressive nature of the disease, current management approaches often fail to achieve the glycemic targets (i.e, < 6.5% or < 7.0%) in the long term.[3,4,5] To maintain glycemic control in patients with type 2 diabetes mellitus (T2DM), multiple glucose-lowering agents and/or insulin are required. However, combination therapies are associated with significant adverse effects such as hypoglycemia, weight gain, gastrointestinal (GI) intolerance.[3,6] Therefore, there is an urgent need for developing more effective and better-tolerated glucose-lowering therapies.
The incretin system plays a significant role in the maintenance of glucose homeostasis. Some evidence suggests that glucagon-like peptide-1 (GLP-1) secretion is reduced in subjects with impaired glucose tolerance or T2DM, whereas the responsiveness to GLP-1 is preserved .[7] In recent years, GLP-1 receptor agonists (GLP-1 RAs) have shown promising effects and have become an important therapeutic option in the treatment of T2DM,[5,8] which is owing to the combination of both the promotion of insulin secretion and inhibition of glucagon secretion.[9,10] Studies in vitro and animal models suggested that GLP-1 RAs have the potential to preserve pancreatic islet β-cells by enhancing their proliferation and inhibiting apoptosis.[4,5] In addition, they can reduce the energy intake and therefore may result in weight loss.[4] The benefits of cardioprotection and neuroprotection have also been noted in some studies.[11,12,13]
Native GLP-1 is not suitable for the treatment of T2DM. It can be rapidly resolved by dipeptidyl peptidase-4 (DPP-4), and its half-life is less than 2 minutes .[5,13] Exenatide and liraglutide are 2 representatives of DDP-4-resistant GLP-1 RAs .[14] Their advantages included a low propensity to cause hypoglycemia, the ability to promote weight loss, and confer additional cardiovascular benefits.[6,15] Lixisenatide (AVE0010) is the 3rd synthetic GLP-1 RA; it is a 44-amino acid exendin-4-like GLP-1 RA, which is modified at the C-terminal by 6 Lys residues and deletion of one Pro residue.[5,7,16] Recent clinical studies have shown that lixisenatide is possibly highly effective in patients with T2DM. However, various GLP-1 RAs may have substantial differences in their duration of action and clinical profile. Moreover, the uncertainty associated with some adverse events (AEs) was highlighted in those studies. Thus, the objective of this meta-analysis was to systematically evaluate the efficacy and safety of lixisenatide in patients with T2DM.
2. Methods
The ethical approval was not necessary in this meta-analysis, all of the data were directly extracted from the published randomized controlled trials (RCTs) about lixisenatide for patients with T2DM.
2.1. Search strategy
The MEDLINE, EMBASE, Cochrane library, ClinicalTrials.gov, Google, Web of Science, and the Chinese Science Citation Database were searched up to March 2018. The search strategy was not limited by language or region. The search was performed using both free text and medical subject headlines, and search terms including lixisenatide, AVE0010, and diabetes mellitus.
2.2. Inclusion criteria
The eligibility criteria were as follows. First, Study design: single- or double-blind RCTs, without a language limitation. Second, Population: patients ages > 18 years, with inadequately controlled type 2 diabetes and a glycated hemoglobin (HbA1c) level of 7–10%. Third, Intervention: lixisenatide or placebo was administered subcutaneously, with or without oral antidiabetic agents (OADs)/insulin; the dose of lixisenatide was not limited, and the follow-up period was not less than 12 weeks. Fourth, Outcomes: HbA1c level, HbA1c < 7.0% or < 6.5%, fasting plasma glucose (FPG), body weight, rescue therapy, and AEs.
2.3. Study selection and data extraction
Studies were assessed and data were extracted by 2 independent investigators according to the inclusion criteria in a prespecified Microsoft Excel spreadsheet. Disagreements were resolved by discussion with a 3rd author. The following data were collected:
-
1.
Study characteristics (e.g., author, year of publication, sample size, age, sex ratio, duration of diabetes, and baseline HbA1c level);
-
2.
Intervention measures (e.g., does of lixisenatide, once-daily or twice-daily, 1-step or 2-step, morning or evening);
-
3.
Efficacy (e.g., HbA1c level, HbA1c < 7.0% or < 6.5%, FPG, body weight, and rescue therapy);
-
4.
Safety (e.g., serious AEs, death, gastrointestinal disorders, symptomatic hypoglycemia, and severe hypoglycemia); and
-
5.
Risk of bias: (e.g., random sequence generation, allocation concealment, and blinding).
2.4. Risk of bias assessment
Two authors independently evaluated the methodological quality of the included studies according to the Cochrane Risk of Bias tool for RCTs,[17] and differences were resolved by discussion with a 3rd author.
2.5. Statistical analysis
Data were pooled using Review Manager 5.3 software (RevMan 5.3). Weighted mean difference (WMD) and relative risk (RR) together with their corresponding 95% confidence intervals (CIs) were determined. We analyzed all the outcomes with a random effects model in order to provide a more conservative estimate of the efficacy and safety. Statistical heterogeneity was estimated using the I2 statistic with a cutoff of 50%, and the Chi-square test with a P value of < .10. If the I2 > 50% and P < .10, we would remove the studies with obvious heterogeneity (according to the results of forest plot) and re-analyze the data. Finally, a fixed effects model was used to determine the stability of this meta-analysis, and publication bias was assessed using funnel plots.
3. Results
3.1. Study characteristics
Fourteen eligible multicenter RCTs[5,6,14,18–28] were included finally, with a total sample size of 11,947. The flow chart for trial selection is shown in Figure 1. Three RCTs [29–31] were finally excluded because of a short-term follow-up (<12 weeks); one open-label RCT [16] was also removed from this meta-analysis. The characteristics of included studies are listed in Table 1. The baseline HbA1c level was 7 to 10% in all studies, and the follow-up durations were 24 weeks,[6,18–24,26,28] 13 weeks,[5] 12 weeks,[14,27] and 25 months.[25] Lixisenatide 20 μg once daily was subcutaneously administered in most of the included studies. Metformin,[5,18–25,28] sulfonylurea,[6,18–21,25] thiazolidinedione,[24,25] pioglitazone,[22] and insulin[6,23–25,28] were used in different studies for glycemic control.
Figure 1.
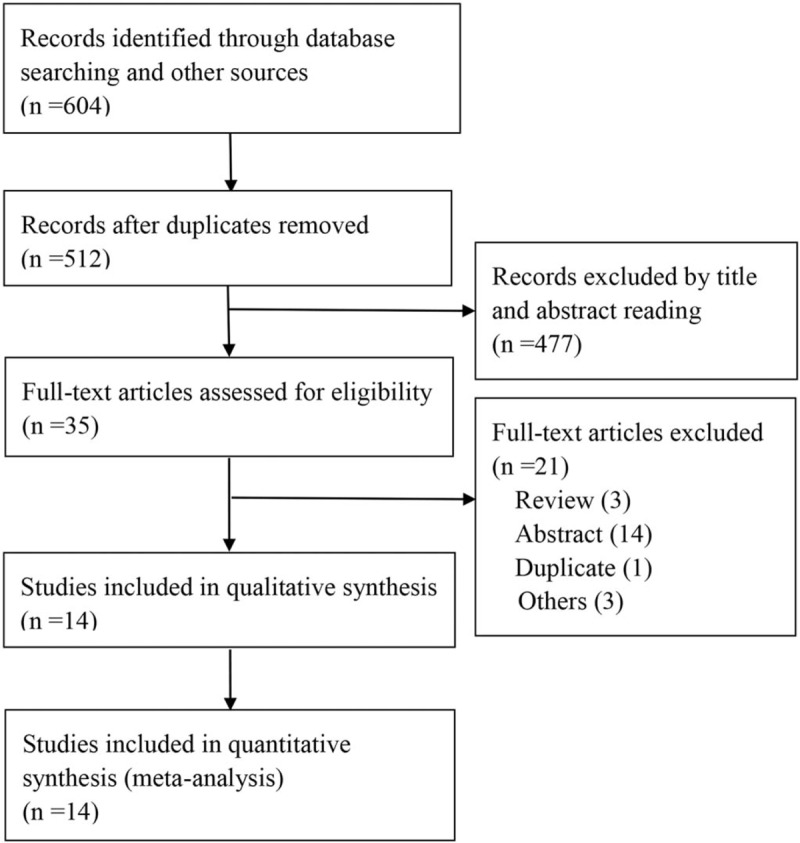
The flow chart of trial selection.
Table 1.
The characteristics of included studies in this meta-analysis.

3.2. Risk of bias
Overall, the risk of bias was low (Fig. 2). Patients were randomly divided into 2 groups, and allocation concealment was performed using a centralized interactive voice response system or centralized assignment system in eight studies.[5,6,14,22–25] All of the eligible studies were double-blind trials.[5,6,14,18–28]
Figure 2.
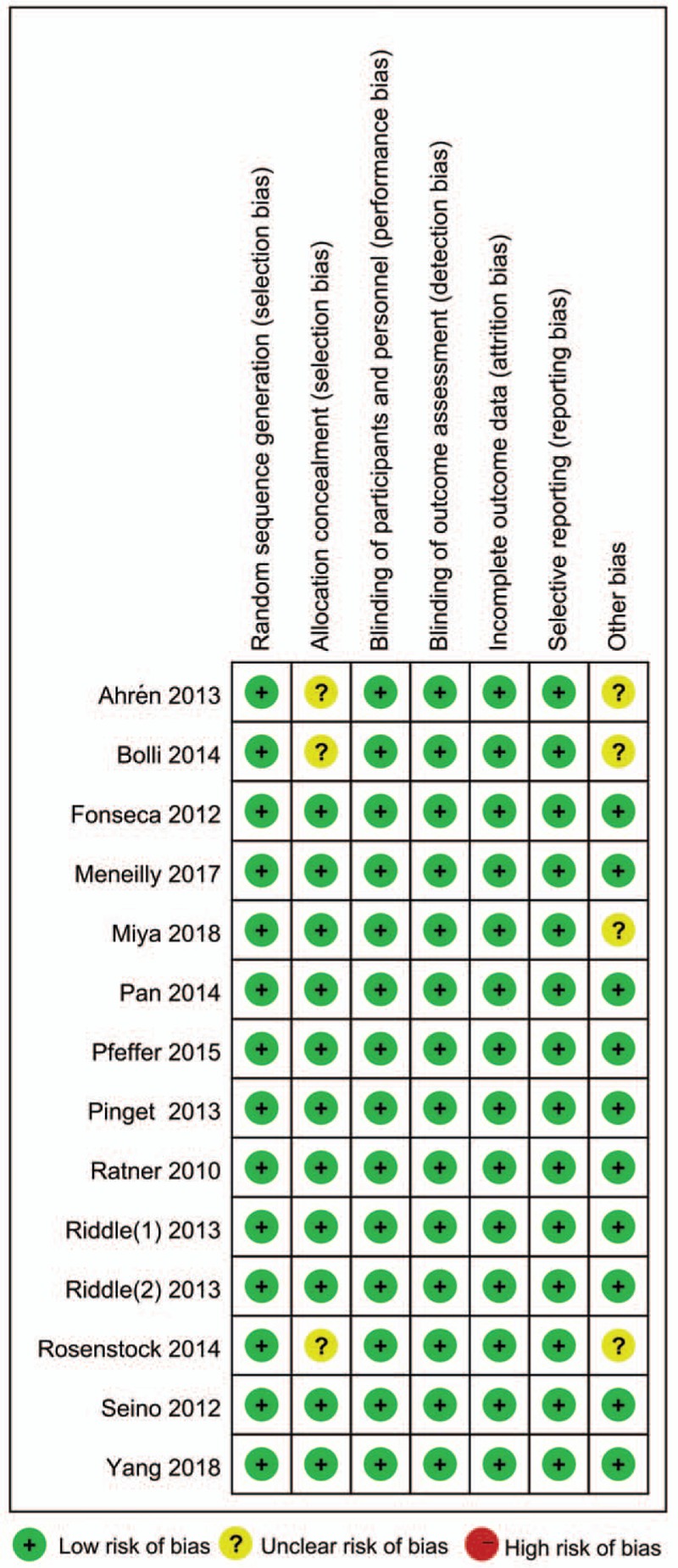
The risk of bias in this meta-analysis.
3.3. Efficacy of lixisenatide for T2DM
3.3.1. HbA1c level
Seven RCTs [5,6,19–21,26,28] reported the HbA1c level at the end of the follow-up. High heterogeneity existed among these studies (I2 = 66%, P = .005). The meta-analysis showed that there was a statistically significant difference between the lixisenatide and placebo groups (WMD = -0.48; 95% CI [-0.60, -0.36]) (Table 2). The forest plot showed obvious heterogeneity between the study by Rosenstock et al. [18] and the other studies. After removing it, a consistent result was obtained compared to that obtained previously (WMD = -0.44; 95% CI, [-0.55, -0.33]) (Fig. 3).
Table 2.
Outcomes of the meta-analysis and sensitivity analysis.

Figure 3.
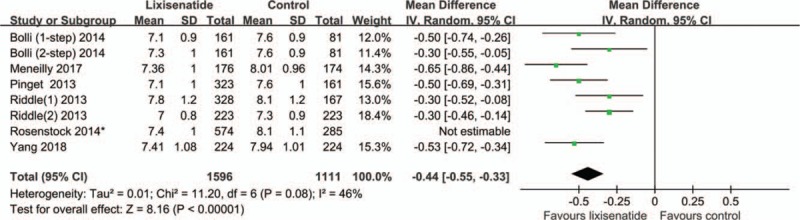
The meta-analysis of HbA1c levels at the end of the follow-up ∗The study by Rosenstock et al showed obvious heterogeneity with others, according to the forest plot. After the study was removed, we obtained results consistent with those obtained before.
3.3.2. HbA1c<7.0%
Eleven RCTs [5,6,14,18–24,28] reported the number of patients with HbA1c < 7.0%. Moderate heterogeneity existed among these studies (I2 = 58%, P = .0005). A comparison of the lixisenatide- and placebo-treated patients with T2DM showed statistically significant difference (RR = 1.94, 95% CI [1.73–2.16]) (Table 2). After the obviously heterogeneous study by Seino et al. [6] was removed, the result was similar to that achieved previously (RR = 1.89, 95% CI [1.75–2.03]) (Fig. 4).
Figure 4.
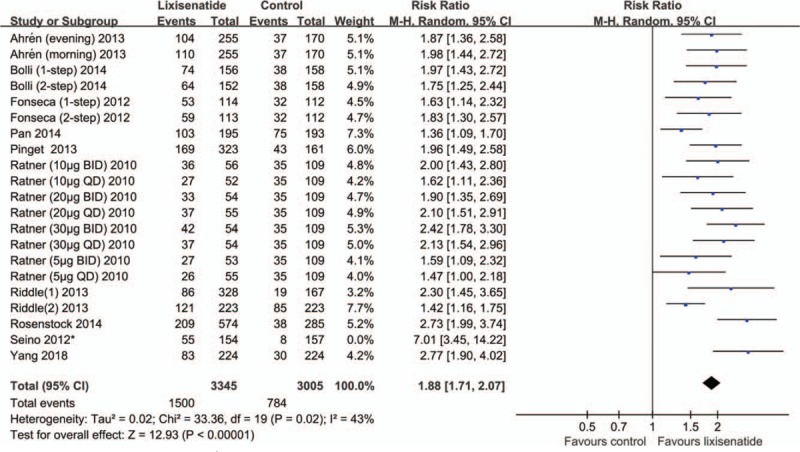
The meta-analysis of HbA1c < 7% ∗ The study by Seino et al showed obvious heterogeneity with others, according to the forest plot. After the study was removed, we obtained results consistent with those obtained before.
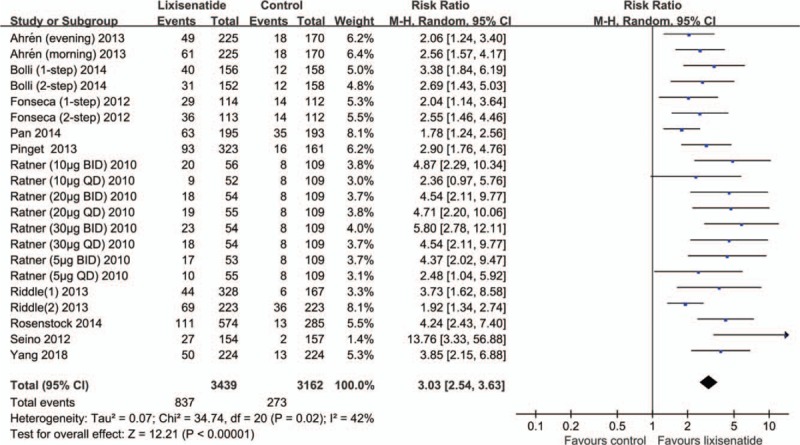
3.3.3. HbA1c<6.5%
Eleven RCTs [5,6,14,18–24,28] reported the number of patients with HbA1c < 6.5%. No significant heterogeneity existed among these studies (I2 = 43%, P = .02). The meta-analysis showed statistically significant differences between lixisenatide- and placebo-treated patients (RR = 3.03, 95% CI [2.54–3.63]) (Fig. 5).
Figure 5.
The meta-analysis of HbA1c < 6.5%.
3.4. FPG
Seven RCTs [5,6,19–21,26,28] reported the FPG levels of their subjects. No significant heterogeneity existed among these studies (I2 = 28%, P = .21). There was a statistically significant difference between the lixisenatide and placebo groups (WMD = -0.43, 95% CI [-0.62, -0.25]) (Table 2).
3.4.1. Body weight
Body weight was reported in 6 [5,6,20,21,26,28] RCTs. No heterogeneity existed among these studies (I2 = 0%, P = .78). There was a statistically significant difference in body weight between the lixisenatide and placebo groups (WMD = -1.34, 95% CI [-2.67,-0.02]) (Table 2).
3.4.2. Rescue therapy
Nine RCTs [5,6,18,19,20,22,23,26,28] reported the proportion of patients who received rescue therapy during follow-up. No heterogeneity existed among these studies (I2 = 0%, P = .66). The meta-analysis showed that there was a statistically significant difference in the patients who received rescue therapy during follow-up between the lixisenatide and placebo groups (RR = 0.39, 95% CI [0.30–0.51]) (Table 2).
3.5. Others
Five RCTs [5,18,20,21,28] reported glucose excursion, and 5 RCTs [5,20,21,26,28] reported the 2-hour postprandial plasma glucose (PPG) levels after a standardized breakfast. The meta-analysis showed statistically significant differences for these factors between lixisenatide and placebo groups (WMD = -3.91, 95% CI [-4.72, -3.10]; WMD = -4.31, 95% CI [-5.50, -3.12], respectively) (Table 2).
3.6. Safety of lixisenatide for T2DMs
3.6.1. Any AEs and discontinuation
Twelve RCTs [5,6,14,18–24,26,28] and 14 RCTs (5, 6, 14, 18–28) respectively reported the outcomes of any AEs and discontinuation due to AEs. No significant heterogeneity existed among these studies (I2 = 46%, P = .009; I2 = 0%, P = .52, respectively). It was found that lixisenatide may increase the risk of any AEs and the rate of discontinuation due to AEs, and there were statistically significant differences with regard to these factors between the lixisenatide and placebo groups (RR = 1.14, 95% CI [1.08–1.19]; RR = 1.79, 95% CI [1.57–2.05], respectively) (Table 2).
3.6.2. Serious AEs and death
Thirteen RCTs [5,6,14,18–26,28] reported serious AEs, and drug-related deaths occurred in 6 included studies [5,6,20–22,26]. There was no heterogeneity among these studies (I2 = 0%, P = .51; I2 = 0%, P = .82). Lixisenatide was not associated with serious AEs or death in patients with T2DM; no statistically significant difference with regard to these factors between the lixisenatide and placebo groups (RR = 0.94, 95% CI [0.86–1.04]; RR = 0.73, 95% CI [0.18–2.98], respectively) (Table 2).
3.7. Gastrointestinal AEs
Gastrointestinal AEs included gastrointestinal disorders, nausea, vomiting, and diarrhea. They were respectively reported in 13,[5,6,14,18–23,25–28] 12,[5,6,14,18–24,26,28] 12,[5,6,14,18–24,26,28] and 10[5,6,18–24,26] RCTs. The meta-analysis showed that compared to the placebo in patients with T2DM, lixisenatide could increase the risks of gastrointestinal disorders (I2 = 74%, P < .00001; RR = 2.23, 95% CI [1.86–2.68]), nausea (I2 = 30%, P = .09; RR = 4.09, 95% CI [3.38–4.95]), vomiting (I2 = 18%, P = .23; RR = 5.57, 95% CI [3.88–7.98]), and diarrhea (I2 = 7%, P = .38; RR = 1.28, 95% CI [1.05–1.55]); there were statistically significant differences in these events between the 2 groups (Table 2).
3.8. Hypoglycemia
All RCTs [5,6,14,18–28] reported patients with symptomatic hypoglycemia and severe hypoglycemia; severe hypoglycemia was reported in 5 studies [5,20,21,25,26]. No significant heterogeneity existed among these studies (I2 = 0%, P = .61; I2 = 0%, P = .45). The meta-analysis showed that compared to the placebo, lixisenatide was associated with the risk of symptomatic hypoglycemia (RR = 1.36, 95% CI [1.24–1.50]). However, there was no statistically significant difference in severe hypoglycemia between the 2 groups (RR = 0.74, 95% CI [0.40–1.36]) (Table 2).
3.9. Skin reaction
Injection-site reactions and allergic reactions were respectively reported in 9[5,6,18–23] and 6[19–23,28] RCTs. Our meta-analysis showed that lixisenatide could increase the risk of injection-site reactions (I2 = 0%, P = .61; RR = 2.05, 95% CI [1.43–2.95]). However, there were statistically significant differences in allergic reactions between the lixisenatide and placebo groups (I2 = 0%, P = .97; RR = 2.11, 95% CI [0.68–6.54]) (Table 2).
3.10. Publication bias
A publication bias was shown by funnel plots for HbA1c < 7.0% and HbA1c < 6.5%. The funnel plots were relatively symmetrical, suggesting that there was no publication bias in this meta-analysis (Figure S1–2).
3.11. Sensitivity analysis
A sensitivity analysis was performed using a fixed-effects model to determine the stability of this meta-analysis. All of the results were consistent with that obtained using random-effects model (Table 2).
4. Discussion
Incretin based therapies, such as the GLP-1RAs, represent a major advancement in T2DM treatment.[28,32] Several GLP-1 RAs are available and are increasingly been used as monotherapies or “add-on” therapies to OADs/insulin.[16,33] As a novel agent in this class, lixisenatide is receiving attention as a T2DM treatment. Our meta-analysis showed that, compared with placebo, lixisenatide could significantly reduce the level of HbA1c, and a significantly higher proportion of lixisenatide-treated patients achieved the HbA1c targets of < 7.0% and < 6.5%. Further, compared to placebo, lixisenatide was associated with a significant reduction in FPG and 2-hour PPG levels after a standardized breakfast. These findings are consistent with those of recent studies.[6,14,18–25] Horowitz et al [34] hold the view that GLP-1 participates in the regulation of appetite and energy intake. However, in this meta-analysis, there was no statistically significant difference in body weight at the end of follow-up between the 2 groups. This finding is inconsistent with the dominant idea in some studies.[18,19,23,24,32,35]
The mechanisms of lixisenatide's glucose-lowering effect have been investigated in several studies .[32] It was shown that lixisenatide could restore the 1st and 2nd-phase insulin responses and accelerate glucose disposition .[32,34] At the same time, lixisenatide could reduce the postprandial glycemic excursions by sustained slowing of gastric emptying, which is of fundamental significance for patients with T2DM.[36] In addition, it is thought that GLP-1 could reduce appetite and energy intake,[37] although no statistically significant difference was found in body weight between the 2 groups in this meta-analysis. It is most noteworthy that various GLP-1 RAs may exhibit different effects on pre- and postprandial glucose levels. Buse et al [38] performed a direct comparison between liraglutide and exenatide, 2 different kinds of GLP-1 RAs, in patients with inadequately controlled T2DM. Results showed that liraglutide more significantly reduced the FPG level while exenatide had a greater effect on PPG excursions. Similar results were found for lixisenatide and liraglutide in type 2 diabetic patients .[30] Some small open-label trials shown that short-acting GLP-1 RAs seem to have a preserved and sustained effect on glucagon secretion and gastric emptying in patients with type 1 diabetes, which could translate into effective lowering of postprandial glucose excursions .[39] However, there is no direct evidence of how lixisenatide works in patients with type 1 diabetes.
The safety profile of lixisenatide was another focus in this meta-analysis. Lixisenatide is associated with the potential risk of any AEs, and a larger proportion of patients with lixisenatide discontinued treatment due to the AE as well. Even so, there were no statistical differences in serious AEs and death between the lixisenatide and placebo groups. The incidence of gastrointestinal AEs was higher in the lixisenatide group than in the placebo group. The most common gastrointestinal AEs included gastrointestinal disorders, nausea, vomiting, and diarrhea. Most of them were mild to moderate in intensity, reduced with ongoing treatment, and resolved within 6 to 8 weeks.[21,32] In our meta-analysis, the percentage of patients with symptomatic hypoglycemia was 13.5% in the lixisenatide group and 9.4% in the placebo group (P < .01). However, the incidence of severe hypoglycemia was comparable between the lixisenatide and placebo (P = .25). In addition, lixisenatide could significantly reduce the frequency of rescue therapy (P < .01). Moreover, it resulted in a lower incidence of hypoglycemia and better gastrointestinal tolerability than those associated with other GLP-1 RAs such as exenatide and liraglutide.[16,30]
There are several strengths of our meta-analysis. First, all of the eligible studies were RCTs, sample size (11,947) was large. Furthermore, the studies were double-blind. Second, an interactive voice response or web-based system was used in most of these studies to ensure sufficient concealment of random allocation. Third, all of the patients were ages > 18 years and had an HbA1c level of 7 to 10%. However, 1 limitation that could not be ignored was the short-term follow-up (≥ 12 weeks, ≤ 24 weeks). Because lixisenatide is a new drug, longer-term studies are required to determine the efficacy and safety of lixisenatide in patients with T2DM.
Compared to placebo, lixisenatide could significantly reduce the levels of HbA1c, FPG, and PPG, and higher proportion of lixisenatide-treated patients achieved the HbA1c targets of < 7.0% and < 6.5% in lixisenatide-treatment group. It increased the incidence of mild-to-moderate gastrointestinal AEs and symptomatic hypoglycemia, but it was not associated with serious AEs, death, or severe hypoglycemia. In conclusion, lixisenatide was effective and relatively well tolerated in patients with inadequately controlled T2DM.
Acknowledgments
Thanks for the support of Gansu province Science and Technology Support Program. The sponsors had no involvement in the study design, data collection and analysis, the writing or the decision to submit the manuscript for publication.
Author contributions
Data curation: Hui-han Zhang, Zhe-yuan Wang.
Formal analysis: Zhe-yuan Wang, Gen-nian Wang.
Investigation: Xiao-dong Xu.
Methodology: Gen-nian Wang, Feng-xian Wei, Xiao-dong Xu.
Resources: Ya-wu Zhang.
Software: Man-cai Wang, Feng-xian Wei.
Visualization: Zhen-gang Wei.
Writing – original draft: Zhen-gang Wei, Man-cai Wang, Ya-wu Zhang.
Writing – review & editing: You-cheng Zhang.
Supplementary Material
Footnotes
Abbreviations: AEs = adverse events, CIs = confidence intervals, DPP-4 = dipeptidyl peptidase-4, FPG = fasting plasma glucose, GLP-1 = glucagon-like peptide-1, IDF = International Diabetes Federation, OAD = oral antidiabetic agents, PPG = postprandial plasma glucose, RAs = receptor agonists, RCT = randomized controlled trial, RevMan = Review Manager, RR = relative risk, T2DM = type 2 diabetes mellitus, WMD = weighted mean difference.
Zhen-gang Wei and Man-cai Wang, these authors contributed equally to this work.
Supplemental Digital Content is available for this article.
Conflicts of Interest and Source of Funding: The work was supported by Gansu province Science and Technology Support Program (1204FKCA138). No potential conflict of interest relevant to this article was reported.
References
- [1].Vos T, Allen C, Arora M, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388:1545–602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [2].International Diabetes Federation (IDF) [homepage on the Internet]. IDF diabetes atlas. 8th edition. [updated 2017]. Available from: http://www.idf.org/diabetesatlas. [Google Scholar]
- [3].Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in type 2 diabetes: a patient-centered approach: position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 2012;35:1364–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [4].Bolli GB, Owens DR. Lixisenatide, a novel GLP-1 receptor agonist: efficacy, safety and clinical implications for type 2 diabetes mellitus. Diabetes Obes Metab 2014;16:588–601. [DOI] [PubMed] [Google Scholar]
- [5].Ratner RE, Rosenstock J, Boka G, et al. Dose-depenadent effects of the once-daily GLP-1 receptor agonist lixisenatide in patients with Type 2 diabetes inadequately controlled with metformin: a randomized, double-blind, placebo-controlled trial. Diabetes Med 2010;27:1024–32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Seino Y, Min KW, Niemoeller E, et al. Randomized, double-blind, placebo-controlled trial of the once-daily GLP-1 receptor agonist lixisenatide in Asian patients with type 2 diabetes insufficiently controlled on basal insulin with or without a sulfonylurea (GetGoal-L-Asia). Diabetes Obes Metab 2014;16:588–601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Werner U, Haschke G, Herling AW, et al. Pharmacological profile of lixisenatide: a new GLP-1 receptor agonist for the treatment of type 2 diabetes. Regul Pept 2010;164:58–64. [DOI] [PubMed] [Google Scholar]
- [8].Meier JJ. GLP-1 receptor agonists for individualized treatment of type 2 diabetes mellitus. Nat Rev Endocrinol 2012;8:728–42. [DOI] [PubMed] [Google Scholar]
- [9].Fineman MS, Cirincione BB, Maggs D, et al. GLP-1 based therapies: differential effects on fasting and postprandial glucose. Diabetes Obes Metab 2012;14:675–88. [DOI] [PubMed] [Google Scholar]
- [10].Aroda VR, Ratner R. The safety and tolerability of GLP-1 receptor agonists in the treatment of type 2 diabetes: a review. Diabetes Metab Res Rev 2011;27:528–42. [DOI] [PubMed] [Google Scholar]
- [11].Fisher M. Glucagon-like peptide 1 receptor agonists and cardiovascular risk in type 2 diabetes: a clinical perspective. Diabetes Obes Metab 2015;17:335–42. [DOI] [PubMed] [Google Scholar]
- [12].Mundil D, Cameron-Vendrig A, Husain M. GLP-1 receptor agonists: a clinical perspective on cardiovascular effects. Diab Vasc Dis Res 2012;9:95–108. [DOI] [PubMed] [Google Scholar]
- [13].Forst T, Pfützner A. Pharmacological profile, efficacy and safety of lixisenatide in type 2 diabetes mellitus. Expert Opin Pharmacother 2013;14:2281–96. [DOI] [PubMed] [Google Scholar]
- [14].Fonseca VA, Alvarado-Ruiz R, Raccah D, et al. Efficacy and safety of the once-daily GLP-1 receptor agonist lixisenatide in monotherapy: a randomized, double-blind, placebo-controlled trial in patients with type 2 diabetes (GetGoal-Mono). Diabetes Care 2012;35:1225–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [15].Wang B, Zhong J, Lin H, et al. Blood pressure-lowering effects of GLP-1 receptor agonists exenatide and liraglutide: a meta-analysis of clinical trials. Diabetes Obes Metab 2013;15:737–49. [DOI] [PubMed] [Google Scholar]
- [16].Rosenstock J, Raccah D, Korányi L, et al. Efficacy and safety of lixisenatide once daily versus exenatide twice daily in type 2 diabetes inadequately controlled on metformin: a 24-week, randomized, open-label, active-controlled study (GetGoal-X). Diabetes Care 2013;36:2945–51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ 2011;343:d5928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Rosenstock J, Hanefeld M, Shamanna P, et al. Beneficial effects of once-daily lixisenatide on overall and postprandial glycemic levels without significant excess of hypoglycemia in type 2 diabetes inadequately controlled on a sulfonylurea with or without metformin (GetGoal-S). J Diabetes Complications 2014;28:386–92. [DOI] [PubMed] [Google Scholar]
- [19].2014;Bolli GB, Munteanu M, Dotsenko S, et al. Efficacy and safety of lixisenatide once daily vs. placebo in people with Type 2 diabetes insufficiently controlled on metformin (GetGoal-F1). Diabet Med. 31:176–84. [DOI] [PubMed] [Google Scholar]
- [20].Yu Pan C, Han P, Liu X, et al. Lixisenatide treatment improves glycaemic control in Asian patients with type 2 diabetes mellitus inadequately controlled on metformin with or without sulfonylurea: a randomized, double-blind, placebo-controlled, 24-week trial (GetGoal-M-Asia). Diabetes Metab Res Rev 2014;30:726–35. [DOI] [PubMed] [Google Scholar]
- [21].Ahrén B, Leguizamo Dimas A, Miossec P, et al. Efficacy and safety of lixisenatide once-daily morning or evening injections in type 2 diabetes inadequately controlled on metformin (GetGoal-M). Diabetes Care 2013;36:2543–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Pinget M, Goldenberg R, Niemoeller E, et al. Efficacy and safety of lixisenatide once daily versus placebo in type 2 diabetes insufficiently controlled on pioglitazone (GetGoal-P). Diabetes Obes Metab 2013;15:1000–7. [DOI] [PubMed] [Google Scholar]
- [23].Riddle MC, Aronson R, Home P, et al. Adding once-daily lixisenatide for type 2 diabetes inadequately controlled by established basal insulin: a 24-week, randomized, placebo-controlled comparison (GetGoal-L). Diabetes Care 2013;36:2489–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Riddle MC, Forst T, Aronson R, et al. Adding once-daily lixisenatide for type 2 diabetes inadequately controlled with newly initiated and continuously titrated basal insulin glargine: a 24-week, randomized, placebo-controlled study (GetGoal-Duo 1). Diabetes Care 2013;36:2497–503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Pfeffer MA, Claggett B, Diaz R, et al. Lixisenatide in patients with type 2 diabetes and acute coronary syndrome. N Engl J Med 2015;373:2247–57. [DOI] [PubMed] [Google Scholar]
- [26].Meneilly GS, Roy-Duval C, Alawi H, et al. Lixisenatide therapy in older patients with type 2 diabetes inadequately controlled on their current antidiabetic treatment: the GetGoal-O Randomized Trial. Diabetes Care 2017;40:485–93. [DOI] [PubMed] [Google Scholar]
- [27].Miya A, Nakamura A, Miyoshi H, et al. Satisfaction of switching to combination therapy with lixisenatide and basal insulin in patients with type 2 diabetes receiving multiple daily insulin injection therapy: a randomized controlled trial. J Diabetes Investig 2018;9:119–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [28].Yang W, Min K, Zhou Z, et al. Efficacy and safety of lixisenatide in a predominantly Asian population with type 2 diabetes insufficiently controlled with basal insulin: the GetGoal-L-C randomized trial. Diabetes Obes Metab 2018;20:335–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [29].Seino Y, Takami A, Boka G, et al. Pharmacodynamics of the glucagon-like peptide-1 receptor agonist lixisenatide in Japanese and Caucasian patients with type 2 diabetes mellitus poorly controlled on sulphonylureas with/without metformin. Diabetes Obes Metab 2014;16:739–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Kapitza C, Forst T, Coester HV, et al. Pharmacodynamic characteristics of lixisenatide once daily versus liraglutide once daily in patients with type 2 diabetes insufficiently controlled on metformin. Diabetes Obes Metab 2013;15:642–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Lorenz M, Pfeiffer C, Steinsträsser A, et al. Effects of lixisenatide once daily on gastric emptying in type 2 diabetes--relationship to postprandial glycemia. Regul Pept 2013;185:1–8. [DOI] [PubMed] [Google Scholar]
- [32].Cryer PE. Minireview: glucagon in the pathogenesis of hypoglycemia and hyperglycemia in diabetes. Endocrinology 2012;153:1039–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Unger RH, Cherrington AD. Glucagonocentric restructuring of diabetes: a pathophysiologic and therapeutic makeover. J Clin Invest 2012;122:4–12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Horowitz M, Rayner CK, Jones KL. Mechanisms and clinical efficacy of lixisenatide for the management of type 2 diabetes. Adv Ther 2013;30:81–101. [DOI] [PubMed] [Google Scholar]
- [35].Bagger JI, Knop FK, Holst JJ, et al. Glucagon antagonism as a potential therapeutic target in type 2 diabetes. Diabetes Obes Metab 2011;13:965–71. [DOI] [PubMed] [Google Scholar]
- [36].Holst JJ, Vilsboll T. Combining GLP-1 receptor agonists with insulin: therapeutic rationales and clinical findings. Diabetes Obes Metab 2013;15:3–14. [DOI] [PubMed] [Google Scholar]
- [37].Raccah D, Gourdy P, Sagnard L, et al. Lixisenatide as add-on to oral antidiabetic therapy: an effective treatment for glycemic control with body weight benefits in type 2 diabetes. Diabetes Metab Res Rev 2014;30:742–8. [DOI] [PubMed] [Google Scholar]
- [38].Buse JB, Rosenstock J, Sesti G, et al. Liraglutide once a day versus exenatide twice a day for type 2 diabetes: a 26-week randomised, parallel-group, multinational, open-label trial (LEAD-6). Lancet 2009;374:39–47. [DOI] [PubMed] [Google Scholar]
- [39].Albèr A, Brønden A, Knop FK. Short-acting glucagon-like peptide-1 receptor agonists as add-on to insulin therapy in type 1 diabetes: a review. Diabetes Obes Metab 2017;19:915–25. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.