

Abstract
Background/Aims
Polyethylene glycol (PEG)-3350, approved by Food and Drug Administration (FDA) only for constipation, combined with 1.9 L of sports drink (SD) (Gatorade®) and bisacodyl (B) is commonly used in outpatient practice for bowel preparation due to cited patient satisfaction and tolerability of this specific regimen. We aim to compare PEG-3350 (Miralax®) with PEG-AA-based (MoviPrep®) in terms of efficacy, patient satisfaction, and the effects of these two regimen on serum electrolytes.
Materials and Methods
This study is a prospective, single-blinded, block randomized trial comparing single-dose PEG-3350+SD+B to split-dose 2-L PEG-AA in the outpatient endoscopy unit in patients undergoing colonoscopy. Basic metabolic profiles were checked on the day of randomization and on the day of procedure. Patients completed a survey on the day of procedure. Bowel preparation quality was assessed using the Boston Bowel Preparation Scale (BBPS) by two endoscopists and a nurse present during the procedure.
Results
We randomized 150 patients (74 PEG-3350+SD+B and 76 PEG-AA). The PEG-AA group had significantly higher BBPS scores in the right colon by Endoscopist 1, Nurse, and Endoscopist 2 (p 0.005, <0.000, 0.001) and in the left and transverse colon by Nurse and Endoscopist 2 (p 0.004, 0.26, 0.000, 0.006). There was no statistically significant difference in patient satisfaction or change in serum electrolytes between the two groups.
Conclusion
Use of single-dose PEG-3350+SD+B results in inferior bowel preparation for colonoscopy compared with split-dose PEGAA and does not provide any advantage in regards to patient satisfaction. We therefore recommend discontinuing the use of PEG 3350 for bowel preparation.
Keywords: Colonoscopy, bowel preparation, Miralax, Moviprep, patient satisfaction, tolerability
INTRODUCTION
In compliance with the evidence that screening colonoscopy reduces the incidence of colorectal cancer (CRC) and mortality, established guidelines recommend screening colonoscopy every 10 years in individuals aged ≥50 years with an average risk for CRC (1–4). In order to assure a high-quality colonoscopy, optimal bowel preparation is essential as it affects the diagnostic accuracy, safety, efficacy, and length of the procedure. Patients with inadequate bowel preparations are more likely to have missed lesions, longer duration of exams, aborted exams, or repeat exams sooner than standard practice guidelines (5–7). This can increase screening costs by 12%-22% (8).
An ideal bowel preparation should not only be able to thoroughly cleanse the colon but also be well tolerated by patients to ensure completion. Bowel preparation remains a major deterrent to patient compliance with CRC screening guidelines (9). At least 5%-15% of patients do not complete their bowel preparation because of the large volume of bowel preparation solution consumption or poor palatability (10). In an effort to improve patient tolerability and adherence, reduced-volume 2-L polyethylene glycol-ascorbic acid (PEG-AA) and electrolyte lavage solutions (ELSs) are now available, with ascorbic acid acting as an additional cathartic and flavoring agent. This reduced-volume preparation demonstrated comparable efficacy and favorable tolerability to the original 4-L PEG-ELS solutions (11–13).
Background
As an alternative to the FDA-approved PEG-ELS solutions, many endoscopists also use PEG-3350 (Miralax®), approved by FDA for constipation, in combination with a sports drink (SD) such as Gatorade® for repletion of electrolytes and bisacodyl (B) tablets (Dulcolax®) as an adjunct stimulant laxative. One study using PEG-3350 in a community setting resulted in good-quality bowel preparations and patient tolerability (14). Subsequent studies compared PEG-3350+SD with 4-L PEG-ELS, some concluding PEG-3350 as a non-inferior bowel preparation (15–17), while others showed higher quality preparations with 4-L PEG-ELS (10,18). There have been no head-to-head comparative trials of PEG-3350+SD+B vs. PEGAA. The aim of our study was to compare the efficacy of bowel preparation, patient satisfaction, and electrolyte abnormalities between these two regimens.
MATERIALS AND METHODS
The study took place at a large urban hospital in the mid-west state of Illinois, USA between February and November 2012. The ethics committee of the institutional review board of the hospital reviewed and approved the study in accordance with federal regulations and any other governing regulations or subparts. All patients provided written informed consent. The trial was registered and listed on http://clinicaltrials.gov (01695863).
This study was a two-arm, single-blinded, prospective, block randomized controlled trial. Study subjects were adults aged 18–80 years undergoing outpatient colonoscopies. Exclusion criteria were consistent with contraindications to currently approved bowel preparations and included patients with ileus or bowel obstruction, bowel perforation, previous alimentary tract surgery, significant gastroparesis or gastric outlet obstruction, toxic colitis or megacolon, or severe ulcerative colitis or if they were pregnant or lactating. We also excluded patients with significant electrolyte abnormalities, renal or hepatic insufficiency, congestive heart failure, or those with impaired consciousness. The power and sample size estimates were based on known efficacy in the PEG-AA group and meaningfully detectable efficacy in the PEG-3350 group. We aimed to include 75 patients in each group. A total of 150 patients were enrolled and assigned to a treatment group using block randomization. This process was blinded to the endoscopists and nurses who participated in grading the efficacy of bowel preparation.
All patients were instructed to be on a clear liquid diet starting on the day prior to the colonoscopy. Patients assigned to the PEG-3350 group were instructed to take 2 tablets of B with 8 ounces of water at 15:00 the day prior to the procedure. At 20:00, they were instructed to mix 238 g of PEG-3350 in 64 ounces of SD and drink 8 ounces of this solution every 15 min until the entire solution is consumed. Patients assigned to the PEG-AA group were instructed to mix packet A and B in 1 L of water and start drinking 8 ounces every 15 min starting at 18:00 the day prior to the colonoscopy until the solution is completely consumed. The same was repeated the morning of their procedure with another 1 L, at least 4 h prior to the colonoscopy.
Colonoscopies were performed in the outpatient endoscopy unit of the same hospital. Procedures were deemed completed with visualization of the appendiceal orifice and ileocecal valve. The Boston Bowel Preparation Scale (BBPS), a validated bowel preparation scoring system (19), was used to evaluate the quality of bowel preparation. BBPS uses a scoring system ranging from 0 to 3 (grading as below), and the right, transverse, and left colon were separately graded (Table 1). Grading using BBPS was performed by the endoscopist performing the procedure (Endoscopist 1), a nurse present during procedure (Nurse), and an endoscopist reviewing pictures of the procedure (Endoscopist 2), which were taken at every 10 cm while withdrawing the colonoscope from the cecum or most proximal area of the colon that could be visualized. The endoscopists and nurses were instructed on the use of BBPS prior to participating in the grading, and they were blinded to the bowel preparation that the patient consumed. The quality of bowel cleansing was evaluated by averaging the BBPS scores from Endoscopist 1, Nurse, and Endoscopist 2. A score of 2–3 represented good-to-excellent bowel preparation, which we will term as adequate. Scores of 0–1 will be considered as inadequate bowel preparation.
Table 1.
Boston bowel preparation scale
| Score | |
|---|---|
| 0 | Unprepared colon segment with mucosa not seen because of solid stool that cannot be cleared |
| 1 | Portion of mucosa of the colon segment seen, but other areas of the colon segment are not well seen because of staining, residual stool, and/or opaque liquid |
| 2 | Minor amount of residual staining, small fragments of stool, and/or opaque liquid, but mucosa of colon segment is seen well. |
| 3 | Entire mucosa of colon segment seen well, with no residual staining, small fragments of stool, or opaque liquid. |
Patients completed a questionnaire that rated their symptoms and impressions with the bowel preparation. Symptoms of nausea, vomiting, bloating, abdominal pain, or cramping were graded on a 5-point scale ranging from 0 (no complaints) to 4 (very severe). Difficulty in completing the bowel preparation was assessed on a 4-point scale ranging from 0 (no difficulty) to 3 (significant difficulty). Overall satisfaction with the bowel preparation was rated on a 5-point scale ranging from 1 (extremely dissatisfied) to 5 (extremely satisfied). In the questionnaire, patients were also asked what percentage of the bowel preparation they completed and if their bowel preparation experience would prevent them from having another colonoscopy in the future.
In order to assess the safety of the bowel preparations in regards to serum electrolyte abnormalities, patients had basic metabolic profiles drawn at the time of the randomization and on the day of the colonoscopy at the time of the registration (following completion of bowel preparation and before initiation of colonoscopy).
The primary endpoint of the study was to determine the efficacy of bowel cleansing of PEG-3350+SD+B compared with PEG-AA determined by BBPS. Sample size was calculated to achieve an 80% power to detect a 5% difference in efficacy with a 95% confidence interval. Based on these calculations, 75 patients were required in each arm of the study. The analysis included all patients who underwent colonoscopy. Data analysis included independent samples t-test, Pearson’s χ2 test, and repeated measures analysis of variance which were all performed using Statistical Package for Social Sciences for Windows version 21.0 (IBM Corp.; Armonk, NY, USA).
RESULTS
Sample
A total of 150 patients were recruited and randomized to 75 patients in each arm. Among these, 128 patients arrived for the colonoscopy. Among the eligible 128 patients, 66 were in the PEG-AA group and 62 in the PEG-3350+SD+B group. Three patients in the PEG-AA group and one patient in the PEG-3350+SD+B group completed <75% of the bowel preparation (Table 2).
Table 2.
Demographics
| MoviPrep | Miralax+Gatorade+ Bisacodyl | |
|---|---|---|
| n | 66 | 62 |
| Male | 44.6% | 55.4% |
| Female | 42.6% | 57.4% |
| Ante-meridiem procedure | 26.6% | 28.1% |
| Post-meridiem procedure | 25% | 20.3% |
| First colonoscopy | 79.2% | 65.9% |
Grading from Endoscopist 1 was available for 45 patients in the PEG-AA group and 40 in the PEG-3350+SD+B group. Grading from Nurse was available for 45 patients in the PEG-AA group and 39 in the PEG-3350+SD+B group. Grading from Endoscopist 2 was available for 63 patients in the PEG-AA group and 59 in the PEG-3350+SD+B group. Fifty-one patients from the PEG-AA group and 43 from the PEG-3350+SD+B group completed the patient satisfaction questionnaire.
The length of the procedure was recorded for 33 patients in the PEG-3350+SD+B group, with an average of 25.12 min, compared with 41 in the PEG-AA group, with an average of 23.85 min. There was no statistically significant difference between these values.
The number of polyps detected were recorded in 62 patients in the PEG-3350+SD+B group with an average of 0.93 polyps detected per patient compared with 65 patients in the PEG-AA group with an average of 0.69 polyps detected per patient. There was no statistically significant difference between these values.
Approximately 90.2% of patients in the PEG-3350+SD+ B group completed 100% of the bowel preparation compared with 89.4% in the PEG-AA group.
Quality of bowel preparation
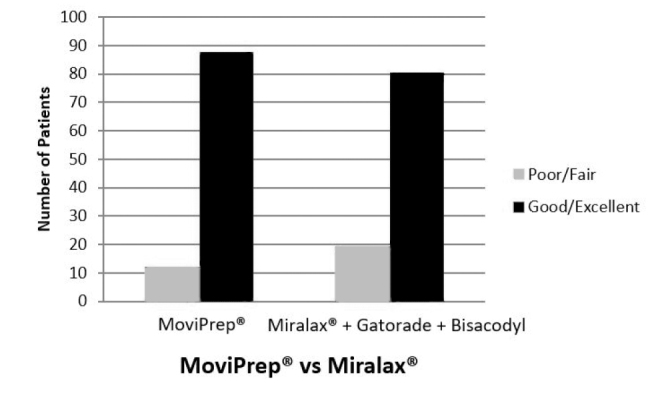
Aggregate BBPS scoring of the right colon was done with 62 patients in the PEG-3350+SD+B group and 65 in the PEG-AA group. In the PEG-3350+SD+B group, 61.3% of patients had adequate bowel cleansing compared with 84.6% of patients in the PEG-AA group, which was statistically significant (p 0.003; Figure 1 and Table 3).
Figure 1.

Graph of revised bowel preparation score for the right colon
Table 3.
Preparation scoring for right colon
| Average of right colon in revised bowel prep scoring | |||
|---|---|---|---|
|
|
|||
| Preparation | Poor/fair (N=34) | Good/excellent (N=93) | p |
| MoviPrep | 10 (15.4%) | 55 (84.6%) | 0.003 |
| Miralax+Gatorade+Bisacodyl | 24 (38.7%) | 38 (61.3%) | |
Aggregate scoring of the transverse colon was done with 61 patients in the PEG-3350+SD+B group and 66 in the PEG-AA group. In the PEG-3350+SD+B group, 72.1% of patients had adequate bowel cleansing compared with 86.4% in the PEG-AA group, which was also statistically significant (p 0.047; Figure 2 and Table 4).
Figure 2.

Graph of revised bowel preparation score for the transverse colon
Table 4.
Preparation scoring for transverse colon
| Average of transverse colon in revised bowel prep scoring | |||
|---|---|---|---|
|
|
|||
| Preparation | Poor/fair (N=26) | Good/excellent (N=101) | p |
| MoviPrep | 9 (13.6%) | 57 (86.4%) | 0.047 |
| Miralax+Gatorade+Bisacodyl | 17 (27.9%) | 44 (72.1%) | |
Aggregate scoring of the left colon was done with 50 patients in the PEG-3350+SD+B group and 58 in the PEG-AA group. In the PEG-3350+SD+B group, 80.6% of patients had adequate bowel cleansing compared with 87.9% in the PEG-AA group (P 0.260; Figure 3 and Table 5). The difference in preparation scores was not statistically significant for the left colon, but the effect (better preparation in the PEG-AA group) was consistent with the right and transverse colon.
Figure 3.
Graph of revised bowel preparation score for the left colon
Table 5.
Preparation scoring for left colon
| Average of left colon in revised bowel prep scoring | |||
|---|---|---|---|
|
|
|||
| Preparation | Poor/fair (N=20) | Good/excellent (N=108) | p |
| MoviPrep | 8 (12.1%) | 58 (87.9%) | 0.260 |
| Miralax+Gatorade+Bisacodyl | 12 (19.4) | 50 (80.6%) | |
A summary of the average scores utilizing BBPS to evaluate the quality of bowel preparation in the right, transverse, and left colon are summarized in Table 6 below.
Table 6.
Summary of bowel preparation scores
| Average boston bowel preparation system | MoviPrep Mean (Standard Deviation) | Miralax+Gatorade+Bisacodyl Mean (Standard Deviation) | p | 95% Confidence interval of the difference |
|---|---|---|---|---|
| Right colon | 2.33 (0.89) | 1.79 (0.72) | 0.000 | 0.269–0.816 |
| Transverse colon | 2.45 (0.72) | 2.06 (0.79) | 0.005 | 0.122–0.655 |
| Left colon | 2.46 (0.70) | 2.24 (0.76) | 0.08 | −0.029–0.484 |
Patient satisfaction and adverse events
When asked if the bowel preparation would prevent them from having another colonoscopy in the future, 4.7% of patients in the PEG-3350+SD+B group said “yes” compared with 5.9% in the PEG-AA group. When asked to score their satisfaction with the bowel preparation, 74.5% of patients in the PEG-3350+SD+B group were quite satisfied to extremely satisfied compared with 66.7% of patients in the PEG-AA group. Approximately 20.9% of patients in the PEG-3350+SD+B group had no objection to the bowel preparation compared with 27.5% in the PEG-AA group. Approximately 4.6% of patients in the PEG-3350+SD+B group were quite dissatisfied to extremely dissatisfied compared with 4.0% in the PEG-AA group. Approximately 86.0% of patients in the PEG-3350+SD+B group had no or minimal difficulty or inconvenience in completing the bowel preparation compared with 86.3% in the PEG-AA group. Patients in the PEG-3350 group were more likely to experience vomiting, but there was no statistically significant difference in reported nausea, bloating, and abdominal pain or cramping (Table 7).
Table 7.
Adverse events
| Patient scoring symptoms/impressions | MoviPrep Mean (Standard deviation) | Miralax+Gatorade+Bisacodyl Mean (Standard deviation) | p |
|---|---|---|---|
| Nausea | 0.3152 (0.61) | 0.3590 (0.77) | 0.772 |
| Vomiting | 0.0000 (0.00) | 0.2821 (0.85) | 0.028 |
| Bloating | 0.4565 (0.72) | 0.6667 (0.89) | 0.235 |
| Abdominal pain or cramping | 0.3043 (0.66) | 0.3590 (0.66) | 0.707 |
| Ability to complete entire prep | 1.8511 (0.46) | 1.8780 (0.39) | 0.773 |
| Would prep prevent from future colonoscopy | 0.0638 (0.24) | 0.0488 (0.21) | 0.764 |
| Overall satisfaction | 3.9468 (1.01) | 4.1463 (1.01) | 0.359 |
| Difficulty/Inconvenience in completing prep | 0.6596 (0.75) | 0.6098 (0.80) | 0.766 |
Effect on serum electrolytes
There was no significant difference in serum electrolytes before and after the bowel preparation in either the PEG-3350 or PEG-AA groups except for sodium in the PEGAA group, which was not clinically significant (Table 8).
Table 8.
Effect on eerum electrolytes
| Electrolyte | Bowel prep | Pre-procedure | Post-procedure | p |
|---|---|---|---|---|
| Calcium | MoviPrep | 9.43 | 9.41 | 0.093 |
| Miralax+Gatorade+Bisacodyl | 9.63 | 9.45 | ||
| Glucose | MoviPrep | 103.67 | 100.23 | 0.801 |
| Miralax+Gatorade+Bisacodyl | 101.47 | 100.06 | ||
| Blood Urea Nitrogen | MoviPrep | 15.4 | 12.4 | 0.599 |
| Miralax+Gatorade+Bisacodyl | 16.83 | 13.39 | ||
| Creatinine | MoviPrep | 0.97 | 0.99 | 0.696 |
| Miralax+Gatorade+Bisacodyl | 0.94 | 0.95 | ||
| Sodium | MoviPrep | 140.06 | 140.98 | 0.042 |
| Miralax+ Gatorade+Bisacodyl | 140.27 | 140 | ||
| Potassium | MoviPrep | 4.24 | 4.35 | 0.596 |
| Miralax+Gatorade+Bisacodyl | 4.37 | 4.55 | ||
| Chloride | MoviPrep | 105.73 | 106.17 | 0.107 |
| Miralax+Gatorade+Bisacodyl | 104.72 | 104.18 | ||
| Bicarbonate | MoviPrep | 23.65 | 21.51 | 0.351 |
| Miralax+Gatorade+Bisacodyl | 24.27 | 22.84 |
DISCUSSION
Our study simulated a community setting in which PEG-3350 is being given as a single post-meridiem (PM) do for bowel preparation, given previous studies that cited its convenience and increased patient satisfaction14. Previous studies compared a PEG-3350+SD regimen vs. 4-L PEG-ELS (GoLytely), demonstrating increased patient satisfaction and tolerability in the PEG-3350 group while producing similar rates of high-quality bowel preparation (15–17). We chose to compare PEG-3350+SD+B to the FDA-approved PM/AM split-dose PEG-AA. Our study found that split-dose PEG-AA produced a statistically significantly higher quality bowel preparation of the right and transverse colon when compared with PEG-3350+SD+ B. Our data showed that PEG-AA also produced a better preparation in the left colon, but this did not achieve statistical significance. With regard to patient tolerability of the bowel preparation, there were more reports of vomiting in the PEG-3350 group. However, there was no significant difference in overall patient satisfaction and tolerability between the two groups. With regard to serum electrolytes, there was a statistically significant increase in serum sodium levels with PEG-AA compared with PEG-3350; however, with a mean difference of only 1.19 mEq/L, this has no clinical significance. There was no statistically significant change in the other serum electrolytes in either group.
In addition to producing higher quality bowel preparation, there was also a reduction in the disparities found across the three areas of the colon in the PEG-AA group. For the PEG-3350 group, the disparity between the left and right colon was a BBPS rating of 0.45 (left, 2.24; right, 1.79) compared with a disparity of 0.13 for the PEG-AA group (left, 2.46; right, 2.33). This means that there will be less fluctuation in the quality of information obtained for a single patient, improving the overall reliability of the procedure. Less internal variation means one has greater confidence in the obtained diagnostic results. Bowel preparations have been and continue to be extensively studied as newer agents and formulations are introduced. PEG-3350 along with an electrolyte-replenishing SD continues to be used as an acceptable regimen. Many studies have shown this regimen to be non-inferior to the traditional 4-L PEG-ELS. It is easy to conceptualize that the PEG-3350 is better tolerated by patients as it consists of a total of only 2 L.
Now that 2-L PEG-AA is widely available and commonly prescribed by practitioners, it does not seem as though a PEG-3350+SD regimen is needed as an alternative bowel preparation regimen on the basis of patient tolerability. Our study confirms this, showing that PEG-AA, in comparison to PEG-3350+SD+B, produces a higher quality bowel preparation with no significant difference in patient tolerability or satisfaction. This could avoid the need for a repeat colonoscopy, reduce healthcare spending, and prevent an additional day off from work for a patient. In conclusion, we recommend the use of PEG-AA over a PEG-3350-based bowel preparation regimen.
A previous study demonstrated higher BPPS score using a split-dose PEG-3350+SD vs. single-dose PEG-3350+SD (16). The comparison of single-dose PEG-3550+SD+B to a split-dose PEG-AA bowel preparation regimen was intentionally done to imitate a real-life community gastroenterology practice because despite the fact that split-dose bowel prep has been unequivocally shown to be a better and significantly more effective way of providing quality colonoscopy, physicians in practice nonetheless continue to offer single-day PEG-3350 bowel preparation on the notion that this is as effective as other forms of bowel preparation. For future study, it would be interesting to compare split-dose PEG-3350 with split-dose PEG-AA. If such a study were to show no significant difference in bowel preparation quality between the two groups, there could be utility in the use of a PEG-3350+SD regimen for those who do not have access to PEG-AA.
Footnotes
Presented in: This study was presented at the United European Gastroenterological Conference, October 2013, Berlin, Germany.
“See Editorial 4–6”
Ethics Committee Approval: Ethics committee approval was received for this study from the ethic commitee of Rush University Medical Center. (January 5, 2011/Approval number: 11042705-IRB01)
Informed Consent: Written informed consent was obtained from patients who participated in this study.
Peer-review: Externally peer-reviewed.
Author contributions: Concept - M.A.K.; Design - M.A.K., M.B.; Supervision - M.A.K.; Resource - K.B.P., G.S., L.F., A.K., M.B.; Materials - K.B.P., G.S., L.F.; Data Collection and/or Processing - G.S., L.F., A.K., M.B.; Analysis and/or Interpretation - M.A.K., A.K.; Literature Search - K.B.P., M.N.; Writing - K.B.P., M.N.; Critical Reviews - M.A.K., M.N.
Conflict of Interest: No conflict of interest was declared by the authors.
Financial Disclosure: The authors declared that this study has received no financial support
REFERENCES
- 1.Lewis JD, Gelfand JM, Troxel AB, et al. Immunosuppressant medications and mortality in inflammatory bowel disease. Am J Gastroenterol. 2008;103:1428–35. doi: 10.1111/j.1572-0241.2008.01836.x. https://doi.org/10.1111/j.1572-0241.2008.01836.x [DOI] [PubMed] [Google Scholar]
- 2.Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy. the national polyp study workgroup. N Engl J Med. 1993;329:1977–81. doi: 10.1056/NEJM199312303292701. https://doi.org/10.1056/NEJM199312303292701 [DOI] [PubMed] [Google Scholar]
- 3.Rex DK, Johnson DA, Lieberman DA, Burt RW, Sonnenberg A. Colorectal cancer prevention 2000: screening recommendations of the american college of gastroenterology. American College of Gastroenterology. Am J Gastroenterol. 2000;95:868–77. doi: 10.1111/j.1572-0241.2000.02059.x. https://doi.org/10.1016/S0002-9270(00)00851-0 [DOI] [PubMed] [Google Scholar]
- 4.Florin TH, Paterson EW, Fowler EV, Radford-Smith GL. Clinically active Crohn’s disease in the presence of a low C-reactive protein. Scand J Gastroenterol. 2006;41:306–11. doi: 10.1080/00365520500217118. https://doi.org/10.1080/00365520500217118 [DOI] [PubMed] [Google Scholar]
- 5.Kaminski MF, Regula J, Kraszewska E, et al. Quality indicators for colonoscopy and the risk of interval cancer. N Engl J Med. 2010;362:1795–1803. doi: 10.1056/NEJMoa0907667. https://doi.org/10.1056/NEJMoa0907667 [DOI] [PubMed] [Google Scholar]
- 6.Froehlich F, Wietlisbach V, Gonvers JJ, Burnand B, Vader JP. Impact of colonic cleansing on quality and diagnostic yield of colonoscopy: The European Panel of Appropriateness of Gastrointestinal Endoscopy European multicenter study. Gastrointest Endosc. 2005;61:378–84. doi: 10.1016/s0016-5107(04)02776-2. https://doi.org/10.1016/S0016-5107(04)02776-2 [DOI] [PubMed] [Google Scholar]
- 7.Harewood GC, Sharma VK, de Garmo P. Impact of colonoscopy preparation quality on detection of suspected colonic neoplasia. Gastrointest Endosc. 2003;58:76–9. doi: 10.1067/mge.2003.294. https://doi.org/10.1067/mge.2003.294 [DOI] [PubMed] [Google Scholar]
- 8.Rex DK, Imperiale TF, Latinovich DR, Bratcher LL. Impact of bowel preparation on efficiency and cost of colonoscopy. Am J Gastroenterol. 2002;97:1696–1700. doi: 10.1111/j.1572-0241.2002.05827.x. https://doi.org/10.1111/j.1572-0241.2002.05827.x [DOI] [PubMed] [Google Scholar]
- 9.Harewood GC, Wiersema MJ, Melton LJ., 3rd A prospective, controlled assessment of factors influencing acceptance of screening colonoscopy. Am J Gastroenterol. 2002;97:3186–94. doi: 10.1111/j.1572-0241.2002.07129.x. https://doi.org/10.1111/j.1572-0241.2002.07129.x [DOI] [PubMed] [Google Scholar]
- 10.Enestvedt BK, Fennerty MB, Eisen GM. Randomised clinical trial: MiraLAX vs. Golytely - a controlled study of efficacy and patient tolerability in bowel preparation for colonoscopy. Aliment Pharmacol Ther. 2011;33:33–40. doi: 10.1111/j.1365-2036.2010.04493.x. https://doi.org/10.1111/j.1365-2036.2010.04493.x [DOI] [PubMed] [Google Scholar]
- 11.DiPalma JA, Wolff BG, Meagher A, Cleveland Mv. Comparison of reduced volume versus four liters sulfate-free electrolyte lavage solutions for colonoscopy colon cleansing. Am J Gastroenterol. 2003;98:2187–91. doi: 10.1111/j.1572-0241.2003.07690.x. https://doi.org/10.1111/j.1572-0241.2003.07690.x [DOI] [PubMed] [Google Scholar]
- 12.Bitoun A, Ponchon T, Barthet M, et al. Results of a prospective randomised multicentre controlled trial comparing a new 2-L ascorbic acid plus polyethylene glycol and electrolyte solution vs. sodium phosphate solution in patients undergoing elective colonoscopy. Aliment Pharmacol Ther. 2006;24:1631–42. doi: 10.1111/j.1365-2036.2006.03167.x. https://doi.org/10.1111/j.1365-2036.2006.03167.x [DOI] [PubMed] [Google Scholar]
- 13.Ell C, Fischbach W, Bronisch HJ, et al. Randomized trial of low-volume PEG solution versus standard PEG + electrolytes for bowel cleansing before colonoscopy. Am J Gastroenterol. 2008;103:883–93. doi: 10.1111/j.1572-0241.2007.01708.x. https://doi.org/10.1111/j.1572-0241.2007.01708.x [DOI] [PubMed] [Google Scholar]
- 14.Stratton S, Shelton P, Carleton V, Griglione GR. Feasibility of polyethylene glycol (PEG) 3350 (Miralax) for colon preparation prior to lower endoscopic examination in healthy adults; experience in a community clinic setting. Am J Gastroenterol. 2008;103:2163–4. doi: 10.1111/j.1572-0241.2008.01982_20.x. https://doi.org/10.1111/j.1572-0241.2008.01982_20.x [DOI] [PubMed] [Google Scholar]
- 15.Shieh FK, Gunaratnam N, Mohamud SO, Schoenfeld P. Mira-LAX-gatorade bowel prep versus GoLytely before screening colonoscopy: an endoscopic database study in a community hospital. J Clin Gastroenterol. 2012;46:96–100. doi: 10.1097/MCG.0b013e3182617bfb. https://doi.org/10.1097/MCG.0b013e3182617bfb [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Samarasena JB, Muthusamy VR, Jamal MM. Split-dosed Mira-LAX/Gatorade is an effective, safe, and tolerable option for bowel preparation in low-risk patients: a randomized controlled study. Am J Gastroenterol. 2012;107:1036–42. doi: 10.1038/ajg.2012.115. https://doi.org/10.1038/ajg.2012.115 [DOI] [PubMed] [Google Scholar]
- 17.McKenna T, Macgill A, Porat G, Friedenberg FK. Colonoscopy preparation: polyethylene glycol with Gatorade is as safe and efficacious as four liters of polyethylene glycol with balanced electrolytes. Dig Dis Sci. 2012;57:3098–105. doi: 10.1007/s10620-012-2266-5. https://doi.org/10.1007/s10620-012-2266-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Enestvedt BK, Brian Fennerty M, Zaman A, Eisen GM. MiraLAX vs. Golytely: is there a significant difference in the adenoma detection rate? Aliment Pharmacol Ther. 2011;34:775–82. doi: 10.1111/j.1365-2036.2011.04795.x. https://doi.org/10.1111/j.1365-2036.2011.04795.x [DOI] [PubMed] [Google Scholar]
- 19.Lai EJ, Calderwood AH, Doros G, Fix OK, Jacobson BC. The boston bowel preparation scale: a valid and reliable instrument for colonoscopy- oriented research. Gastrointest Endosc. 2009;69:620–5. doi: 10.1016/j.gie.2008.05.057. https://doi.org/10.1016/j.gie.2008.05.057 [DOI] [PMC free article] [PubMed] [Google Scholar]