

Abstract
Aims
To investigate the mediating effects of normative beliefs of drug use on the effects of the #Tamojunto school-based prevention program (Unplugged).
Design
Secondary analysis of a cluster randomized controlled trial.
Setting
Brazil. Participants: A total of 6,391 adolescents (12.68 y.o) from 72 public schools in 6 Brazilian cities. Intervention: Schools were assigned to an experimental condition (#Tamojunto curriculum) or a control condition (no prevention program). Measurements: Baseline data were collected prior to program implementation, and follow-up data were collected 9 and 21 months later. The substances examined were alcohol (including binge drinking), tobacco, marijuana and inhalants. Five in-parallel mediation models evaluated whether the positive and negative beliefs were mediators of the likely effects of the intervention on drug use.
Findings
Lack of evidences regarding differences in normative beliefs or drug use were found between the intervention and control groups. However, there was a clear association between negative drug beliefs and lower consumption (i.e. OR = 0.78; 95% CI 0.70; 0.87, for cannabis use) as well as between positive drug beliefs and higher consumption (i.e. OR = 1.77; 95% CI 1.56; 2.02, for cannabis use) independent of the assigned group.
Conclusions
These results suggest that there is a lack of evidence that the program impact the normative beliefs, as proposed by the theoretical model of the program, suggesting that modifications are needed to produce the intended effect of the program. Negative normative beliefs seem to be a potential protective factor for drug use, but the program’s effect itself on drug use via normative beliefs was not found to be statistically significant. Program activities intended to affect normative beliefs should be improved.
Introduction
Since the 1980s, prevention programs have been created to address the major public health [1,2] issue of the premature use of substances during adolescence [3]. Programs based on a social influence approach, which aims to strengthen personal and interpersonal skills through changes in normative beliefs, are more likely to be effective than programs based on other models [4–7].
In Brazil, although licit and illicit drug use is initiated in early adolescence, between 12 and 14 years of age [8,9], evidence-based drug use prevention programs are not typically implemented in schools [10]. In 2013, to address this gap, the Brazilian government conducted a transcultural adaptation process and implemented the Unplugged program as a public policy. Unplugged is based on drug information, normative beliefs and life skills, showing positive results in reducing episodes of drunkenness as well as reports of frequent cannabis [11], tobacco, and any drug use [12] among European adolescents.
Unplugged was renamed #Tamojunto in Brazil and was submitted to a randomized controlled trial to evaluate its effectiveness among Brazilian students. This study showed that the program seemed to increase first alcohol use (aRR = 1.30, 95% CI 1.13–1.49) and decrease first inhalant use (aRR = 0.78, 95% CI 0.63–0.96) in the intervention group compared to the control group at the 9-month follow up [13]. Considering these contradictory results, an understanding of the mechanisms underlying the success and failure of this program is needed to identify whether the intervention is effective for changing normative beliefs and to determine where program curricula may be improved to achieve the expected outcome. In other words, does the prevention program affect the mediating variables that are targeted by the intervention as proposed in its logic model [14,15], which in turns, change the drug use as main outcome?
Normative beliefs can be defined as the perceptions of others’ approval or disapproval of some behavior [16]. Questions concerning whether substance use can be a source of pleasure or whether people who use a substance should be regretful of that are examples of inquires related to normative beliefs [17]. In a social and cultural environment with positive beliefs about alcohol, children and adolescents are more prone to use it, as they perceive this behavior as social acceptable. It is important to emphasize that there is no consensus on what to ask in order to measure normative beliefs. Qualitative open questions have already been used [18]. In this study, not only beliefs were included, but also questions about interviewees behaviors on specific situations, such as “If you were to move to a new organization that was not using circuit class therapy, or 7-day service would you advocate for these?” and “What would you like to tell researchers, or policy makers or managers of your organization that would improve stroke rehabilitation” [18]. Other study understood normative beliefs as closely related to attitudes, exerting a mediating role between pure beliefs and attitudes [19].
This comprehension of normative beliefs as mediators between cognitive concepts and attitudes seems to be of great importance for elaborating substance use prevention programs. They are targeted in prevention programs with the aim of reducing the effects of social influences in the drug use initiation process, engaging adolescents to think critically about substance use to change their perceptions towards drug use [5]. Normative beliefs are adopted in prevention programs due to the use of two complementary theoretical models, the theory of Reasoned Action–Attitude and the Planned Behavior theory, which are based on the concept that there is always an intention before the behavior itself. Attitudes contribute to modeling the intentions and result from balancing the perceived beneficial and dangerous outcomes of the behavior [15]. In this context, normative beliefs should work as mediators of the intervention effects [20,21], providing an insight into the mechanism [22] via two paths: prevention program activities modifying the mediators [23] and the mediators affecting the outcome measurements [24]. Mediation analysis can be described as the processes that lead to behavioral change, providing an overview of the mechanisms underlying program success or failure [25]. Reliance on the “criteria to establish mediation” logic described in the seminal work of Baron and Kenny [26] are largely no longer recommended by methodologists in the area of mediation analysis. More contemporary approaches has focused on the indirect effect of X on Y [27]. The indirect effect of X (#Tamojunto random assignment) on Y (drug use) through mediator (normative beliefs) quantifies the estimated difference in Y resulting from a one-unit change in X through a sequence of causal steps in which X affects M, which in turn affects Y. Thus, regardless of the intervention impact on drug use or impact the normative beliefs, contemporary mediation model has not postulate that both previously cited path must be statistically significant in order to deflagrate a mediated effect of X on Y via M.
A study that evaluated the short-term mediation factor involved in the effectiveness of the Unplugged program in Europe found that adolescents in the intervention group reduced positive attitudes toward drugs; positive beliefs about cigarettes, alcohol, and cannabis; and the normative perception of peers using tobacco and cannabis [5]. Other social-influence-based school prevention program studies have conducted mediation evaluations and corroborate these findings, showing that normative beliefs are significant mediators between the prevention program activities and adolescents’ drug use [28–30]. However, it should be noted that in the literature of school-based prevention programs, there is a lack of evaluations of mediation mechanisms [31].
Considering the important role that normative beliefs play in drug prevention programs, the purpose of this study is to investigate the mediating effects of the #Tamojunto school-based prevention program (Unplugged) in Brazil on adolescents drug use via two normative beliefs.
Methods
Study design
The present study was based on a secondary analysis of a two-arm school cluster randomized controlled trial (Consort checklist in S1 Table and S2 Table), in which schools were randomly assigned to either the intervention arm (#Tamojunto program) or to a control arm, receiving the usual education curriculum in Brazil (no prevention program), among adolescents in 72 public schools in 6 Brazilian cities (São Paulo, Distrito Federal, São Bernardo do Campo, Florianópolis, Fortaleza and Tubarão), located in 4 Brazilian states. Considering that this is an evaluation of a school intervention, we used the cluster design.
Excel’s macro [command RAND] was used to perform the randomization at the school level, and in the drawn school, all potential classrooms were invited to participate. Data were collected simultaneously in the control and intervention schools at three time points. Pre-test data were collected from February 10 to 21, 2014. The first follow-up assessment was carried out 9 months later (November 10 to 28, 2014), and the second follow-up assessment was conducted 21 months after baseline (November 9 to 28, 2015).
The RCT was registered at the Brazilian Ministry of Health Register of Clinical Trials (REBEC), under protocol number RBR-4mnv5g. The register on REBEC depends on the approval of the University Research Ethics Committee (REC). We have obtained the REC approval on November 2013 and have started the process in REBEC in early 2014. However, it took 7 months to be evaluated in REBEC. It is usually a very slow process (S3 Table). The authors confirm that all ongoing and related trials for this drug/intervention are registered.
All procedures in the present study were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study and the consent procedure were approved by the Ethics in Research Committees at the University of São Paulo (#473.498) on November 23th 2013. Consent to participate in the study was written and obtained from the schools’ directors before randomization and from students, after randomization. All participants took part voluntarily after having given their free and informed consent based on the autonomy of adolescents guaranteed by the Brazilian Statute of the Child and Adolescent (Law No. 8069/1990). Moreover, parents were informed of the study by the directors and could recommend non-participation in data collection if they preferred. However, participation in the intervention was part of the school curriculum and was mandatory for all the students in the participating schools.
Population and sample size
Based on the sample size calculation [32] defined to investigate recent binge drinking, the primary outcome of #Tamojunto trial, for a given power of 80%, a significance level of 5% and a difference between groups of 1.5 percentage points (i.e., from 5% to 3.5%), the necessary sample size for each study arm was calculated to be 2,835. To account for losses and for a high intraclass correlation, the sample was increased by 50% and had to draw 4,253 participants in each arm. The parameters used were based on a previously conducted pilot study and data regarding school absences of enrolled students [33].
The target population was students attending 7th and 8th grade (12 to 13 years of age) in the geographical areas of the cities participating in the study. In each of the participating municipalities, 4 to 30 schools were simply randomly selected (in proportion to the size of the city’s population) from all of the public middle schools in these locations (using the national registration list of schools from the Instituto Nacional de Estudos e Pesquisas Educacionais Anísio Teixeira (INEP). Using the schools selected to participate in the study, a second simple, random selection process was performed to match the control and intervention schools at a ratio of 1:1 by municipality.
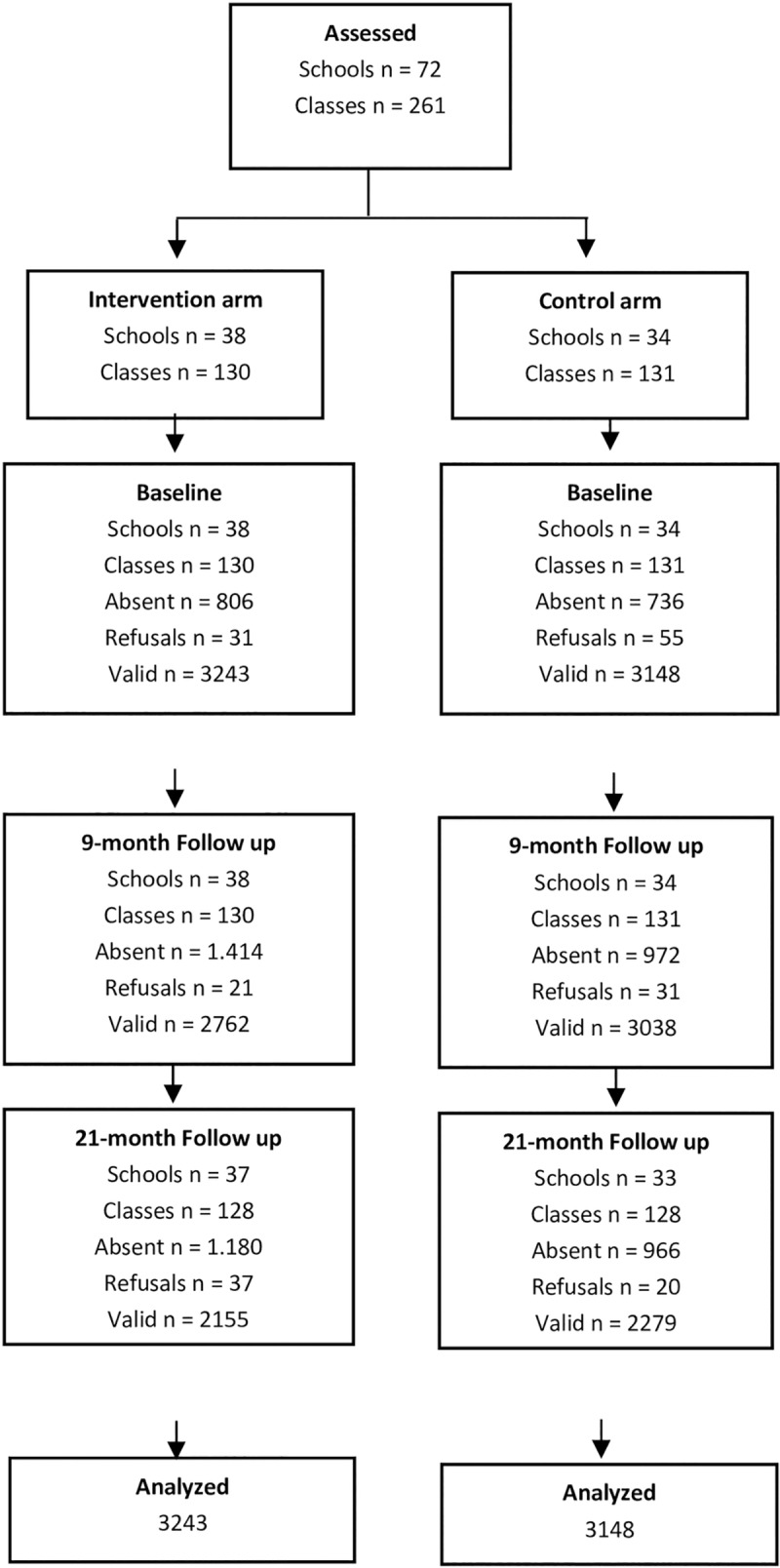
As each school had approximately four 8th grade classes of 30 students each, at least 35 schools in the intervention arm and the same number in the control arm (total of 70 schools) were needed to access the number of students required to maintain the power of the test. Considering a 10% rate of refusal of schools, 38 schools were enrolled in each arm. A total of 72 schools accepted our invitation to participate in the study, as described in Fig 1. In each of the participating municipalities, 4 to 30 schools were randomly selected (in proportion to the size of the city’s population).
Fig 1. CONSORT flow diagram for the randomized controlled trial.
In each of the schools, all 8th grade classes were invited to participate in the study, prior to randomization of groups. In Fortaleza, Santa Catarina and Tubarão, the 7th grade classes of the selected schools were also included because these cities were in the process of changing the age of students assigned to each grade, and the State Education Secretariat requested the inclusion of the 7th grade classes in the study. Details on the study design and sampling methods have been previously presented [13].
Intervention
The Unplugged program was first designed by the EU-DAP group [34] and consists of 12 classes based on a social influence curriculum (4 one-hour classes on attitudes and knowledge of drugs, 4 classes on social and interpersonal skills, and 4 classes on personal skills), with an average class time of 50 minutes. The classes are delivered by class teachers trained and guided by the students’ and the teacher’s manuals. Both manuals are open-access and made available in several languages on the website www.eudap.net.
The implementation and cultural adaptation of the program were the responsibility of the Brazilian Ministry of Health (BMH) team under the supervision of the European developers (in 2013), and the evaluation was conducted by an independent team of federal university professors.
The teachers that delivered the program attended a 16-hour training program facilitated by coaches trained by the European developers, i.e., the master-trainers of the EU-DAP Intervention Planning Group [12]. To guarantee fidelity and dose, teachers were supervised monthly by the coaches from the BMH who had facilitated the initial training. At the end of each class, teachers had to complete a fidelity questionnaire to assess the dose of the program delivered. A total of 87% of the schools completed the 12 program lessons. The other 13% terminated the program between lessons 4 and 11 for two main reasons: the teachers went on medical leave, or they were not comfortable implementing the program.
The English version of the Unplugged material was translated into Portuguese, retaining the original format and subject (educational strategies provided in 12 classes and 3 parent workshops) but with adapted activities. Given the epidemiological profile of illegal drug use among students in Brazil, all information on heroin was excluded and replaced with information on crack-cocaine [8]. Nevertheless, the main changes were made to align the activities of the program with the Alcohol and Other Drugs Policy paradigm advocated by the Brazilian government [35], which is against the “War on Drugs” model. More details about the cultural adaptation process are described in [36].
Instrument and variables
The instrument used for data collection was developed and tested by the EU-DAP and used in previous studies of Unplugged effectiveness [37]. In Brazil, we used a translated and adapted version of the EU-DAP questionnaire in Portuguese [38] that had some questions replaced with items from two questionnaires widely used in several studies among Brazilian students: a questionnaire by the World Health Organization for drug surveys at schools that was adapted by the Brazilian Center for Psychotropic Drug Information [8] and a questionnaire by PENSE (the Brazilian National Survey of School Health) that was used by the BMH [39].
The outcomes analyzed were adolescents’ past 9- and 12-month use (use in the year = yes vs. no) of the following drugs: alcohol (including binge drinking, or the consumption of five or more alcoholic drinks on a single occasion), tobacco, marijuana, and inhalants. The adjustment variables were sex, age and socio-economic class (SES) assessed using the ABEP scale [40]. To evaluate normative beliefs about drugs, we used the scale developed by EU-DAP [5] about negative and positive beliefs about drugs. This is the module from the EU-DAP questionnaire that effectively evaluate the concept of normative beliefs, rather than only attitudes. The 11-item scale assessing attitudes and beliefs about drugs contains 6 items to which a response of “Agree” would constitute a “drug-negative” response, and 5 items to which a response of “Agree” would indicate a “drug-positive” response. The positive beliefs (agree or disagree) related to drug use were as follows: “Using drugs can be a pleasant activity”, “Many things are much riskier than trying drugs”, “Using drugs is fun”, “Drugs help people to experience life fully”, and “The police should not be annoying young people who are trying drugs”. The negative beliefs (agree or disagree) related to drug use were as follows: “A young person should never use drugs”, “Everyone who tries drugs eventually regrets it”, “To experiment with drugs is to give away control of your life”, “Schools should teach the real hazards of taking drugs”, “Drug use is one of the biggest evils in the country”, “The laws about drugs should be made stronger”, and “A young person should never try drugs”.
Contrary to some studies [5] in which the indirect trajectories were estimated using single items as mediators generating multiple mediation models (also called parallel mediation models), we opted to create two parceling scores: one related to the 5 positive items and the other to the 6 negative beliefs. The parceling procedure was adopted to reduce the number of comparisons across the mediators (consequently generating a more parsimonious model). Parceling is supported by the psychometric principles based on the Principle of Aggregation [41,42] and the Law of Large Numbers [43,44]; for additional details, see [45].
To pair (link) the questionnaires of each subject at the three data collection time points (baseline and the two follow-up time points), students filled in a secret code created from their personal information. These codes protected the participants, offering anonymity and confidentiality, and at the same time allowed researchers to link the individual questionnaires collected at the different time points of the study [46]. The secret codes were matched using the Levenshtein algorithm, which identifies similarities among a set of characters. School and class codes were included in the matching process [47]. Final data is presented in S2 Appendix.
Statistical analysis
Five in-parallel mediation models were evaluated to determine if the positive and negative beliefs were mediators of the likely effects of the group intervention assignment (random) on five different outcomes related to drug use: alcohol use, alcohol binge drinking, cannabis use, cigarette use, and inhalant use. In other words, we tested if the random assignment to the intervention (an antecedent variable) influenced the consequent variables (the five outcomes regarding drug use) indirectly through two types of beliefs, taking the school (second level) as the cluster indicator. The covariates were age, sex, SES, and the outcomes at the baseline assessment. Normative beliefs included in the analysis referred to the first follow-up data collection point (9 months after baseline). All analysis included the 72 clusters, which were analyzed via the Mplus’ COMPLEX command to deal with non-independence of the observation (i.e., children nested in schools).
Fig 2 shows the in-parallel mediation model. It should be noted that the covariates (in gray) were also regressed at the same time on the two mediators and on the outcomes [48].
Fig 2. Conceptual model of the mediation model tested.

Due to the study design, an in-cluster randomized clinical trial, missing data across the follow-up time points were imputed to fulfill the intention-to-treat (ITT) paradigm following the CONSORT statements [49]. Multiple imputations were carried out using Bayes estimation of an unrestricted variance-covariance model, which is then used to impute the missing values. Regarding the unrestricted model to use for imputation, the sequential setting available in Mplus [50] version 7.4 was selected because there is a combination of continuous and categorical variables in our mediation models. The sequential setting uses a sequential regression method, also referred to as the chained equations algorithm [51].
Multiple imputations are random draws from the posterior distribution of the missing values [52,53]. Major details regarding the multiple imputation methods can be found in [54]. Five imputation datasets were generated and used in the subsequent analyses using the method from [53] via a robust maximum likelihood (ML) estimator. We opted for such an estimator due to our complex design, where the 3,691 children are nested in 72 schools, producing an ML with odds ratios that are more comprehensible than a probit scale. To evaluate the robustness of the multiple imputation followed by ML analysis (MI-ML), we conducted a sensitivity analysis using two other analytical approaches to deal with the missing values: 1) a listwise approach, where only subjects with complete data on outcomes and covariates are analyzed; and 2) an approach using all data available to estimate the model through full information ML, where each parameter is estimated directly without first filling in missing data values for each individual, assuming values are missing at random.
Indirect effects are in logit scale, and significance was inspected by evaluating the 95% confidence intervals (when zero is contained in the interval, there is a lack of evidence for the indirect effects). The impact of the covariates, group assignment, and mediators on the outcome are expressed in odds ratios with their respective 95% confidence intervals (confidence intervals containing 1 indicate a lack of statistical significance) for the direct effect and logit for the indirect effect.
Lastly, based on the obtained indirect effect estimates described in the results section, we conducted a Monte Carlo simulation analysis to evaluate the power and other parameters related to the sample size of 6391 subjects, presented in the Supplementary File (S3 Table). 1,000 replications were considered and the following criteria, were we took into account to the evaluation of the adequacy of the sample size: 1) the proportion of replications for which the 95% confidence interval contains the true population parameter value, which was depicted in the first column called 95% coverage, where it is expected the values between 0.91 and 0.98. Also, in addition to this criterion, a power for the indirect effects were estimated based on the 6,391 subjects.
Results
The sample comprised 6,391 adolescents in 72 schools (51% females, average age = 12.62 years old, standard deviation [SD] = 0.825, ranging from 11 to 15 years old). The average ABEP score was 28.02 (SD = 8.17), corresponding to a middle-class score. Table 1 shows the frequencies of the past-year drug use at the two time points of assessment (baseline and 21 months after the intervention), together with the missing values.
Table 1. Descriptive statistics of past-year drug use at the two time points (baseline and 21 months after the intervention).
| Baseline | After 21 montds | |||||||
| No (valid) | Yes (valid) | Missing | No (valid) | Yes (valid) | Missing | |||
| Alcohol Use | 4329 (67.7%) | 2015 (31.5%) | 47 (0.7%) | 1894 (29.6%) | 1731 (27.1%) | 2766 (43.3%) | ||
| Alcohol Binge Drinking | 5315 (83.2%) | 1006 (15.7%) | 70 (1.1%) | 2696 (42.2%) | 908 (14.2%) | 2787 (43.6%) | ||
| Cigarette Use | 6058 (95.2%) | 243 (3.8%) | 63 (1.0%) | 3353 (52.5%) | 252 (3.9) | 2786 (43.6%) | ||
| Inhalant Use | 5802 (90.8%) | 525 (8.2%) | 64 (1.0%) | 3232 (50.6%) | 377 (5.9%) | 3609 (56.5%) | ||
| Cannabis Use | 6171 (96.6%) | 156 (2.4%) | 64 (1.0%) | 3324 (52.0%) | 276 (4.3%) | 2791 (43.7%) | ||
| Control | Unplugged | |||||||
| No (valid %) | Yes (valid %) | Missing % | No (valid %) | Yes (valid %) | Missing % | |||
| Baseline | Alcohol Use | 2126 (67.5%) | 1001 (31.8%) | 21 (0.7%) | 2203 (67.9%) | 1014 (31.3%) | 26 (0.8%) | |
| Alcohol Binge Drinking | 2633 (83.6%) | 487 (15.5%) | 28 (0.9%) | 2682 (82.7%) | 519 (16.0%) | 42 (1.3%) | ||
| Cigarette Use | 3005 (95.5%) | 115 (3.7%) | 28 (0.9%) | 3080 (95%) | 128 (3.9) | 35 (1.1.%) | ||
| Inhalant Use | 2867 (91.1%) | 254 (8.1%) | 27 (0.9%) | 2935 (90.5%) | 271 (8.4%) | 37 (1.1%) | ||
| Cannabis Use | 3050 (96.9%) | 73 (2.3%) | 25 (0.8%) | 3121 (96.2%) | 83 (2.6%) | 39 (1.2%) | ||
| 21 months | Alcohol Use | 1005 (31.9%) | 849 (27.05) | 1294 (41.1%) | 889 (27.4%) | 882 (27.2%) | 1472 (45.4%) | |
| Alcohol Binge Drinking | 1384 (44.0%) | 460 (14.6%) | 1304 (41.45) | 1312 (40.5%) | 448 (13.8%) | 1760 (54.3%) | ||
| Cigarette Use | 1724 (54.8%) | 122 (3.9%) | 1302 (41.4%) | 1629 (50.2%) | 130 (4.0%) | 1484 (45.8%) | ||
| Inhalant Use | 1643 (52.2%) | 202 (6.4%) | 1845 (58.6%) | 1589 (49.0%) | 175 (5.4%) | 1764 (54.4%) | ||
| Cannabis Use | 1713 (54.4%) | 133 (4.2%) | 1302 (41.4%) | 1611 (49.7%) | 143 (4.4.%) | 1489 (45.9%) | ||
The mediators, positive (mean = 1.22, SD = 1.11) and negative (mean = 4.92, SD = 1.48) beliefs, had 39.07% and 40.88% missing data points, respectively. Both the intervention and control groups showed an increase in the prevalence of all drugs evaluated during the 21 months period.
Table 2 shows the impact of all covariates on the outcomes, through direct effects. The direct effects, which represent the simple association between the variables, showed that positive beliefs about drugs are associated with the reporting of past-year consumption for all drugs. There is a gradient of association from licit to illicit drugs, where the strongest association came from cannabis use. Students that reported cannabis use at 21 months were 77% (OR = 1.77; 95% CI 1.56; 2.02) more likely to also have reported positive drug beliefs at 9 months, independent of group allocation, sex, age, SES and baseline drug use.
Table 2. The direct effect and covariate effects on the use of the five drugs examined.
| Group | Age | Sex | SES | Baseline | Positive Beliefs | Negative Beliefs | |
|---|---|---|---|---|---|---|---|
| Alcohol Use (last year) | OR (95% CI), p-value | OR (95% CI), p-value | OR (95% CI), p-value | OR (95% CI), p-value | OR (95% CI), p-value | OR (95% CI), p-value | OR (95% CI), p-value |
| Listwise (n = 2471) | 1.225 (1.005–1.492), 0.044 | 1.100 (0.963–1.255), 0.159 | 1.644 (1.344–2.011), <0.001 | 1.019 (1.008–1.031), 0.001 | 5.533 (4.552–6.726), <0.001 | 1.299 (1.187–1.421), <0.001 | 0.907 (0.850–0.967), 0.003 |
| ML-MAR (n = 4870) | 1.193 (1.014–1.403), 0.033 | 1.053 (0.953–1.164), 0.313 | 1.631 (1.413–1.882), <0.001 | 1.017 (1.007–1.027), 0.001 | 4.914 (4.209–5.737), <0.001 | 1.299 (1.191–1.417), <0.001 | 0.900 (0.845–0.959), 0.001 |
| MI-ML (n = 6391) | 1.170 (0.986–1.388), 0.072 | 1.090 (1.004–1.183), 0.040 | 1.633 (1.367–1.951), <0.001 | 1.016 (1.004–1.027), 0.006 | 4.877 (4.132–5.758), <0.001 | 1.281 (1.180–1.391), <0.001 | 0.894 (0.827–0.965), 0.004 |
| Alcohol Binge Drinking (last year) | |||||||
| Listwise (n = 2459) | 1.116 (0.906–1.375), 0.302 | 1.254 (1.099–1.430), 0.001 | 1.396 (1.120–1.739), 0.003 | 1.015 (1.003–1.027), 0.016 | 4.761 (3.531–6.420), <0.001 | 1.334 (1.210–1.471), <0.001 | 0.894 (0.840–0.952), <0.001 |
| ML-MAR (n = 4842) | 0.990 (0.831–1.179), 0.980 | 1.185 (1.077–1.304), 0.001 | 1.356 (1.146–1.605), <0.001 | 1.012 (1.001–1.022), 0.031 | 4.464 (3.565–5.588), <0.001 | 1.347 (1.229–1.477), <0.001 | 0.886 (0.835–0.939), <0.001 |
| MI-ML (n = 6391) | 0.967 (0.819–1.141), 0.690 | 1.166 (1.043–1.304), 0.007 | 1.369 (1.124–1.667), 0.002 | 1.013 (1.002–1.023), 0.016 | 4.281 (3.291–5.568), <0.001 | 1.392 (1.246–1.555), <0.001 | 0.883 (0.825–0.945), <0.001 |
| Cigarette Use (last year) | |||||||
| Listwise (n = 2457) | 1.165 (0.744–1.826), 0.504 | 1.231 (0.945–1.603), 0.123 | 1.462 (1.095–1.952), 0.010 | 1.007 (0.989–1.025), 0.473 | 7.616 (4.110–14.111), <0.001 | 1.453 (1.278–1.651), <0.001 | 0.785 (0.714–0.889), <0.001 |
| ML-MAR (n = 4846) | 1.071 (0.741–1.548), 0.715 | 1.067 (0.890–1.279), 0.483 | 1.487 (1.159–1.908), 0.002 | 1.006 (0.989–1.023), 0.505 | 6.578 (4.032–10.732), <0.001 | 1.452 (1.287–1.639), <0.001 | 0.789 (0.717–0.869), <0.001 |
| MI-ML (n = 6391) | 1.004 (0.686–1.468), 0.985 | 1.039 (0.910–1.186), 0.569 | 1.682 (1.241–2.280), 0.001 | 1.002 (0.990–1.014), 0.714 | 5.700 (3.758–8.646), <0.001 | 1.814 (1.479–2.225), <0.001 | 0.691 (0.642–0.745), <0.001 |
| Inhalant Use (last year) | |||||||
| Listwise (n = 2463) | 0.980 (0.714–1.277), 0.899 | 0.832 (0.692–1.000), 0.050 | 1.483 (1.157–1.901), 0.002 | 1.012 (0.994–1.030), 0.193 | 4.290 (3.005–6.126), <0.001 | 1.404 (1.236–1.594), <0.001 | 0.946 (0.853–1.049), 0.292 |
| ML-MAR (n = 4849) | 0.877 (0.667–1.153), 0.346 | 0.843 (0.722–0.985), 0.031 | 1.469 (1.163–1.855), 0.001 | 1.012 (0.998–1.026), 0.092 | 3.824 (2.932–4.986), <0.001 | 1.413 (1.250–1.597), <0.001 | 0.936 (0.848–1.034), 0.192 |
| MI-ML (n = 6391) | 0.835 (0.682–1.022), 0.081 | 0.832 (0.713–0.970), 0.019 | 1.551 (1.246–1.930), <0.001 | 1.017 (0.993–1.042), 0.155 | 3.846 (2.773–5.334), <0.001 | 1.564 (1.390–1.761), <0.001 | 0.902 (0.801–1.016), 0.090 |
| Cannabis Use (last year) | |||||||
| Listwise (n = 2451) | 1.187 (0.760–1.855), 0.451 | 1.308 (1.012–1.691), 0.040 | 1.075 (0.767–1.507), 0.673 | 1.004 (0.988–1.020), 0.612 | 5.004 (2.141–11.692), <0.001 | 1.772 (1.556–2.017), <0.001 | 0.780 (0.702–0.867), <0.001 |
| ML-MAR (n = 4847) | 1.039 (0.724–1.491), 0.835 | 1.161 (0.986–1.367), 0.074 | 1.048 (0.842–1.303), 0.676 | 1.004 (0.992–1.016), 0.547 | 6.494 (3.502–12.049), <0.001 | 1.775 (1.554–2.026), <0.001 | 0.784 (0.707–0.869), <0.001 |
| MI-ML (n = 6391) | 0.989 (0.763–1.230), 0.934 | 1.086 (0.922–1.279), 0.321 | 1.200 (0.903–1.593), 0.208 | 0.998 (0.982–1.013), 0.766 | 4.927 (2.637–9.207), <0.001 | 2.569 (2.268–2.910), <0.001 | 0.677 (0.606–0.757), <0.001 |
SES: socio-economic class (SES) assessed using the ABEP scale.
The opposite was observed for negative beliefs about drugs. Negative beliefs at 9 months seemed to predict lower reporting of alcohol use, binge drinking, tobacco use and cannabis use at 21 months, after controlling for the same variables mentioned above. The strongest association occurred for cannabis use (OR = 0.78; 95% CI 0.70; 0.87).
Baseline drug use was also a predictor of drug use at 21 months, as expected. However, the strongest drug use predictor at baseline was tobacco smoking; individuals that reported tobacco smoking at baseline were almost 8 times more likely to also report tobacco smoking after 21 months (OR = 7.6; 95% CI 4.1; 14.1).
Except for cannabis use, being female was associated with past-year drug use at the 21-month follow up. Being female was associated with a 40% increase in past-year binge drinking (OR = 1.40; 95% CI 1.12; 1.74).
Considering that the direct effects were measured after taking into account the group allocation, all of the results presented here are independent of the #Tamojunto program. The odds ratios presented in the text refer to listwise analyses and are corroborated with missing data imputation (ML-MAR and MI-ML).
Table 3 shows the two indirect effects (positive and negative beliefs) and the total indirect effect; indirect effects are reported in logit scale. We found a lack of significance regarding the indirect effects from the random assignment of the positive and negative beliefs, which in turn had lack of effect on the five dichotomous outcomes. Importantly, regardless of the methodological approach used to deal with missing data (listwise, ML-MAR, and MI-ML), the majority of the points estimated, and the confidence intervals were similar, indicating the stability of the estimations and findings. The results suggest that there is lack of effect of the program on the normative beliefs of the students or effect of the normative beliefs on past-year drug use. After Monte Carlo simulation (S3 Table), we observed that our sample size is robust to estimate the indirect effects properly, Details of power analysis are presented on Supplementary file (S3 Table).
Table 3. Mediation path.
| Outcome: Alcohol Use (last year) | via Positive Beliefs | via Negative Beliefs | Total Indirect Effects |
|---|---|---|---|
| Listwise (n = 2471) | 0.017 (-0.007 to 0.041), 0.160 | 0.004 (-0.010 to 0.017), 0.605 | 0.021 (-0.008 to 0.049), 0.154 |
| ML-MAR (n = 4870) | 0.006 (-0.015 to 0.026), 0.591 | 0.003 (-0.009 to 0.016), 0.602 | 0.009 (-0.018 to 0.036), 0.512 |
| MI-ML (n = 6391) | 0.005 (-0.014 to 0.024), 0.629 | 0.002 (-0.012 to 0.016), 0.742 | 0.007 (-0.016 to 0.030), 0.549 |
| Outcome: Alcohol Binge Drinking (last year) | |||
| Listwise (n = 2459) | 0.019 (-0.008 to 0.046), 0.170 | 0.003 (-0.12 to 0.018), 0.706 | 0.022 (-0.010 to 0.054), 0.177 |
| ML-MAR (n = 4842) | 0.006 (-0.018 to 0.031), 0.604 | 0.003 (-0.011 to 0.018), 0.657 | 0.10 (-0.021 to 0.041), 0.420 |
| MI-ML (n = 6391) | 0.006 (-0.015 to 0.028), 0.564 | 0.004 (-0.010 to 0.018), 0.562 | 0.011 (-0.018 to 0.039), 0.690 |
| Outcome: Cigarette Use (last year) | |||
| Listwise (n = 2457) | 0.025 (-0.013 to 0.063), 0.191 | 0.007 (-0.026 to 0.040), 0.672 | 0.032 (-0.019 to 0.083), 0.221 |
| ML-MAR (n = 4846) | 0.011 (-0.022 to 0.038), 0.520 | 0.007 (-0.020 to 0.034), 0.603 | 0.018 (-0.029 to 0.064), 0.455 |
| MI-ML (n = 6391) | 0.023 (-0.025 to 0.07), 0.355 | 0.014 (-0.017 to 0.045), 0.115 | 0.036 (-0.026 to 0.099), 0.254 |
| Outcome: Inhalant Use (last year) | |||
| Listwise (n = 2463) | 0.022 (-0.012 to 0.056), 0.199 | 0.002 (-0.007 to 0.010), 0.675 | 0.024 (-0.012 to 0.060), 0.187 |
| ML-MAR (n = 4849) | 0.006 (-0.022 to 0.034), 0.688 | 0.002 (-0.006 to 0.010), 0.646 | 0.008 (-0.023 to 0.039), 0.626 |
| MI-ML (n = 6391) | 0.006 (-0.024 to 0.037), 0.301 | 0.004 (-0.006 to 0.014), 0.111 | 0.010 (-0.024 to 0.044), 0.258 |
| Outcome: Cannabis Use (last year) | |||
| Listwise (n = 2451) | 0.035 (-0.020 to 0.090), 0.213 | 0.006 (-0.028 to 0.040), 0.730 | 0.041 (-0.026 to 0.107), 0.228 |
| ML-MAR (n = 4847) | 0.011 (-0.036 to 0.058), 0.645 | 0.005 (-0.024 to 0.033), 0.733 | 0.016 (-0.044 to 0.076), 0.605 |
| MI-ML (n = 6391) | 0.020 (-0.042 to 0.082), 0.180 | 0.007 (-0.027 to 0.041), 0.098 | 0.027 (-0.049 to 0.104), 0.172 |
Discussion
The present study used a longitudinal design to test the hypothesis that the #Tamojunto prevention program would change normative beliefs about drug use at 9 months which in turns reduces drug use after 21 months. The null hypothesis, with indirect effects from the random assignment on drug use via positive and negative beliefs, was not rejected. Although the #Tamojunto program did not show statistically significant effects on reducing drug use [13], this paper intended to test whether the program affects normative beliefs and, in the long term, if these beliefs change drug use through a mediation process. However, #Tamojunto showed no success in changing normative beliefs as proposed by the theoretical model program [11,55].
This lack of mediated result is consistent with a systematic review of interventions using normative beliefs to prevent alcohol abuse among university students [56]. However, this finding contradicts the results found in the European Unplugged study, which showed reduced cigarette smoking, drunkenness episodes, and cannabis use through three common mediating factors: attitudes, refusal skills, and perception of the prevalence of the behavior among peers [5]. Other programs have also been successful in targeting normative beliefs in drug prevention programs to reduce drug use [57]: Project MYTRI [28], Project ALERT [30], All Stars [58], and the Aban Aya Youth Project [31].
It is important to state that the role of normative beliefs in prevention programs still remains controversial [59–61]. Two studies from the same group [62,63] found contradictory results among college students and their perceptions and attitudes towards alcohol [59]. Posterior analyses of the same samples found that interventions focusing on normative beliefs had variable efficacy, according to the characteristics of the communities where they were implemented [64]. Therefore, it is fair to infer that cultural and social characteristics play a role in the outcomes of such programs. This could partially explain the different findings from the Brazilian version of the program.
We must consider differences in the implementation process of Unplugged and #Tamojunto. In Brazil, the prevention program was delivered in schools as part of a public policy. Consequently, teacher participation was not voluntary, which may have compromised their engagement in the lessons, thus compromising the fidelity of the intervention, especially concerning normative beliefs [65]. Maintaining implementation standards is a difficult task in Brazil due to teachers’ poor pedagogical backgrounds and their beliefs and ideologies concerning drug use and public policies addressing this issue. This is important, as they are the facilitators of those prevention programs [66]. Data from an evaluation study of the implementation of #Tamojunto showed that only 57% of the classes in the program were completed as described in the manual due to a lack of time and proper knowledge of the content [67]. Additionally, the cultural adaptation of the program should also be considered, as important changes were made in the “Alcohol, Risk and Protection” lesson. Phrases that emphasized the importance of abstaining from alcohol use during adolescence were excluded and reflexive questions about how to avoid alcohol abuse and dependence were added [13], which might have caused changes in the target normative beliefs. Another important aspect that could explain the divergent results is the low quality of Brazilian public schools [68] and the high absenteeism rates of students [69]. These aspects can influence the learning process of students and therefore could be a possible explanation for the difficulty in understanding the activities that involve the changes in the normative beliefs proposed by #Tamojunto.
Despite these findings for mediation, this paper shows that there is a clear association between negative drug beliefs and lower consumption as well as between positive drug beliefs and higher consumption independent of the group allocation. These results show that investing in normative beliefs as mediators is valuable for reducing drug use, as there is a clear association, corroborating the international guidelines [7]. Programs that do not invest in changing normative beliefs do not show efficacy, even if they invested in enhancing self-esteem, psychological well-being and/or social competence, sports participation, or resistance skills [21,57,70]. Mediation analyses should be a research priority to help program developers understand how prevention programs are working and to provide information to modify the program, especially when it has negative impacts on substance use [29,71]. On the other hand, programs focusing on social influences do not seem to be beneficial to high-risk late adolescents. This may be because these subjects usually have already tried substances and using them is already part of their lifestyle choices and not a consequence of peer influence. In this case, normative beliefs play a less important role in the decision to use drugs [72].
A limitation of this study was the high number of students who were absent at baseline and/or at the follow up, resulting in an attrition rate of 37%. It is worth noting that according to a meta-analysis of school-based preventive interventions, attrition rates vary from 5 to 52% [73]. We also should report as a limitation of the study, that the normative beliefs were evaluated by a scale of perception of social acceptability about the use of drugs in general, without distinction of the type of drug used. Moreover, due to low understanding of the concept by adolescents [38], it was decided not to include in this study the question on beliefs about the number of friends who use drugs, as previously evaluated by Giannotta et al [5]. Another limitation is that normative beliefs are a complex construct that can be accessed via different scales in different studies, making comparison difficult, since there is no normative belief golden standard scale [5]. Moreover, we note that our study may suffer from confounding bias, since we cannot control for all the confounding factors that may affect the relationship between the predictor, the mediator, and the outcome.
The results of this study suggest that this program was not successful for changing normative beliefs, as proposed by the theoretical model of the program. The apparent inability of the program to impact mediators may be partially responsible for the negative outcomes previously identified. Negative normative beliefs seem to be a potential protective factor for drug use, while positive beliefs were identified as a potential risk factor for drug use; however, these beliefs were not influenced by the program itself. The activities of the program aimed at affecting normative beliefs should be improved. Consequently, the Brazilian version of the Unplugged program, #Tamojunto, needs significant revision to produce the intended effects, especially if it is to be delivered as a universal substance abuse prevention program.
Supporting information
(DOCX)
(DOCX)
(DOCX)
(PDF)
(XLS)
Acknowledgments
This study was funded by the Brazilian Ministry of Health (TED 89–2014). We are thankful for the technical team from the Ministry of Health, the State and Municipal Secretariats of Health and Education and all the teachers and adolescents who participated in the study. HCM is thankful to the senior researcher CAPES-Alexander von Humboldt Post-Doc Fellowship (Process number 88881.145593/2017-01).
Data Availability
All relevant data are within the paper and its Supporting Information files.
Funding Statement
This study was funded by the Brazilian Ministry of Health through the TED 89-2014 (PI: Dr. Sanchez). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1.Hall WD, Patton G, Stockings E, Weier M, Lynskey M, Morley KI, et al. Why young people’s substance use matters for global health. The Lancet Psychiatry. Elsevier Ltd; 2016;3: 265–279. 10.1016/S2215-0366(16)00013-4 [DOI] [PubMed] [Google Scholar]
- 2.Degenhardt L, Stockings E, Patton G, Hall WD, Lynskey M. The increasing global health priority of substance use in young people. The Lancet Psychiatry. 2016;3: 251–264. 10.1016/S2215-0366(15)00508-8 [DOI] [PubMed] [Google Scholar]
- 3.Foxcroft DR, Tsertsvadze A. Universal family-based prevention programs for alcohol misuse in young people. Cochrane Database Syst Rev. 2011;9: CD009308 10.1002/14651858.CD009308 [DOI] [PubMed] [Google Scholar]
- 4.Faggiano F, Galanti MR, Bohrn K, Burkhart G, Vigna-Taglianti F, Cuomo L, et al. The effectiveness of a school-based substance abuse prevention program: EU-Dap cluster randomised controlled trial. Prev Med (Baltim). 2008;47: 537–543. 10.1016/j.ypmed.2008.06.018 [DOI] [PubMed] [Google Scholar]
- 5.Giannotta F, Vigna-Taglianti F, Rosaria Galanti M, Scatigna M, Faggiano F. Short-Term Mediating Factors of a School-Based Intervention to Prevent Youth Substance Use in Europe. J Adolesc Heal. Elsevier Ltd; 2014;54: 565–573. 10.1016/j.jadohealth.2013.10.009 [DOI] [PubMed] [Google Scholar]
- 6.Guo J-L, Lee T-C, Liao J-Y, Huang C-M. Prevention of Illicit Drug Use Through a School-Based Program: Results of a Longitudinal, Cluster-Randomized Controlled Trial. J Adolesc Heal. Elsevier Inc.; 2015;56: 314–322. 10.1016/j.jadohealth.2014.12.003 [DOI] [PubMed] [Google Scholar]
- 7.UNODC. International Standards on Drug Use Prevention [Internet]. Viena: United Nations Office on Drugs and Crime; 2015. pp. 1–30. Available: https://www.unodc.org/documents/prevention/UNODC_2013_2015_international_standards_on_drug_use_prevention_E.pdf [Google Scholar]
- 8.Carlini EL de A, Noto AR, Sanchez Z van der M, Carlini CM de A, Locatelli DP, Abeid LR, et al. VI Levantamento nacional sobre o consumo de drogas psicotrópicas entre estudantes do ensino fundamental e médio das redes pública e privada de ensino nas 27 capitais brasileiras. Brasília: SENAD—Secretaria Nacional de Políticas sobre Drogas; 2010. 10.1017/CBO9781107415324.004 [DOI] [Google Scholar]
- 9.Malta DC, Mascarenhas M, Porto D, Duarte E, Sardinha L, Barreto S, et al. Prevalence of alcohol and drug consumption among adolescents: data analysis of the National Survey of School Health Prevalência do consumo de álcool e dos dados da Pesquisa Nacional de Saúde Escolar. Rev Bras Epidemiol. 2011;14: 136–146. 10.1590/S1415-790X2011000500014. [DOI] [PubMed] [Google Scholar]
- 10.Pereira APD, Paes ÂT, Sanchez ZM. Factors associated with the implementation of programs for drug abuse prevention in schools. Rev Saude Publica. 2016;50: 1–10. 10.1590/S01518-8787.2016050006855ED [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Faggiano F, Vigna-Taglianti F, Burkhart G, Bohrn K, Cuomo L, Gregori D, et al. The effectiveness of a school-based substance abuse prevention program: 18-Month follow-up of the EU-Dap cluster randomized controlled trial. Drug Alcohol Depend. 2010;108: 56–64. 10.1016/j.drugalcdep.2009.11.018 [DOI] [PubMed] [Google Scholar]
- 12.Gabrhelik R, Duncan A, Miovsky M, Furr-Holden CDM, Stastna L, Jurystova L. “Unplugged”: A school-based randomized control trial to prevent and reduce adolescent substance use in the Czech Republic. Drug Alcohol Depend. 2012;124: 79–87. 10.1016/j.drugalcdep.2011.12.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sanchez ZM, Valente JY, Sanudo A, Pereira APD, Cruz JI, Schneider D, et al. The #Tamojunto Drug Prevention Program in Brazilian Schools: a Randomized Controlled Trial. Prev Sci. 2017;18: 772–782. 10.1007/s11121-017-0770-8 [DOI] [PubMed] [Google Scholar]
- 14.Kreeft P Van Der, Wiborg G, Galanti MR, Siliquini R, Bohrn K, Scatigna M, et al. “Unplugged”: A new European school programme against substance abuse. Drugs-Education Prev Policy. 2009;16: 167–181. 10.1080/09687630701731189 [DOI] [Google Scholar]
- 15.Vadrucci S, Vigna-Taglianti FD, van der Kreeft P, Vassara M, Scatigna M, Faggiano F, et al. The theoretical model of the school-based prevention programme Unplugged. Glob Health Promot. 2016;23: 49–58. 10.1177/1757975915579800 [DOI] [PubMed] [Google Scholar]
- 16.Marcoux BC, Shope JT. Application of the Theory of Planned Behavior to adolescent use and misuse of alcohol. Health Educ Res. 1997;12: 323–331. 10.1093/her/12.3.323 [DOI] [Google Scholar]
- 17.Sidani JE, Shensa A, Barnett TE, Cook RL, Primack BA. Knowledge, Attitudes, and Normative Beliefs as Predictors of Hookah Smoking Initiation: A Longitudinal Study of University Students. Nicotine Tob Res. 2014;16: 647–654. 10.1093/ntr/ntt201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Van Kessel G, Hillier S, English C. Physiotherapists’ attitudes toward circuit class therapy and 7 day per week therapy is influenced by normative beliefs, past experience, and perceived control: A qualitative study. Physiother Theory Pract. Taylor & Francis; 2017;33: 850–858. 10.1080/09593985.2017.1357152 [DOI] [PubMed] [Google Scholar]
- 19.Massarwi AA, Khoury-Kassabri M. Serious physical violence among Arab-Palestinian adolescents: The role of exposure to neighborhood violence, perceived ethnic discrimination, normative beliefs, and, parental communication. Child Abus Negl. Elsevier Ltd; 2017;63: 233–244. 10.1016/j.chiabu.2016.11.002 [DOI] [PubMed] [Google Scholar]
- 20.Griffin KW, Botvin GJ. Evidence-Based Interventions for Preventing Substance Use Disorders in Adolescents. Child Adolesc Psychiatr Clin N Am. 2010;19: 505–526. 10.1016/j.chc.2010.03.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Cuijpers P. Effective ingredients of school-based drug prevention programs. Addict Behav. 2002;27: 1009–1023. 10.1016/S0306-4603(02)00295-2 [DOI] [PubMed] [Google Scholar]
- 22.Mackinnon DP, Dwyer JH. Estimating Mediated Effects in Prevention Studies. Eval Rev. 1993;17: 144–158. 10.1177/0193841X9301700202 [DOI] [Google Scholar]
- 23.Chen H. Theory-driven evaluations London: Sage; 1990. [Google Scholar]
- 24.MacKinnon DP, Lockwood CM, Hoffman JM, West SG, Sheets V. A comparison of methods to test mediation and other intervening variable effects. Psychol Methods. 2002;7: 83–104. 10.1037//1082-989X.7.1.83 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.MacKinnon DP, Fairchild AJ, Fritz MS. Mediation Analysis. Annu Rev Psychol. 2007;58: 593–614. 10.1146/annurev.psych.58.110405.085542 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Baron RM, Kenny D a. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51: 1173–1182. 10.1037/0022-3514.51.6.1173 [DOI] [PubMed] [Google Scholar]
- 27.Hayes AF, Rockwood NJ. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav Res Ther. Elsevier Ltd; 2017;98: 39–57. 10.1016/j.brat.2016.11.001 [DOI] [PubMed] [Google Scholar]
- 28.Bate SL, Stigler MH, Thompson MS, Arora M, Perry CL, Reddy KS, et al. Psychosocial Mediators of a School-Based Tobacco Prevention Program in India: Results from the First Year of Project MYTRI. Prev Sci. 2009;10: 116–128. 10.1007/s11121-008-0113-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Teasdale B, Stephens PC, Sloboda Z, Grey SF, Stephens RC. The influence of program mediators on eleventh grade outcomes for seventh grade substance users and nonusers. Drug Alcohol Depend. 2009;102: 11–18. 10.1016/j.drugalcdep.2008.11.010 [DOI] [PubMed] [Google Scholar]
- 30.Orlando M, Ellickson PL, McCaffrey DF, Longshore DL. Mediation Analysis of a School-Based Drug Prevention Program: Effects of Project ALERT. Prev Sci. 2005;6: 35–46. 10.1007/s11121-005-1251-z [DOI] [PubMed] [Google Scholar]
- 31.Liu LC, Flay BR. Evaluating Mediation in Longitudinal Multivariate Data: Mediation Effects for the Aban Aya Youth Project Drug Prevention Program. Prev Sci. 2009;10: 197–207. 10.1007/s11121-009-0125-1 [DOI] [PubMed] [Google Scholar]
- 32.Lwanga SK, Lemeshow S. Sample size determination in health studies: A practicle manual World Health Organization. Geneva: World Health Organization; 1991. [Google Scholar]
- 33.Sanchez ZM, Sanudo A, Andreoni S, Schneider D, Pereira APD, Faggiano F. Efficacy evaluation of the school program Unplugged for drug use prevention among Brazilian adolescents. BMC Public Health. BMC Public Health; 2016;16: 1206 10.1186/s12889-016-3877-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kreeft P Van Der, Wiborg G, Galanti MR, Siliquini R, Bohrn K, Scatigna M, et al. ‘Unplugged’: A new European school programme against substance abuse. Drugs Educ Prev Policy. 2009;16: 167–181. 10.1080/09687630701731189 [DOI] [Google Scholar]
- 35.Brasil. Guia Estratégico para o Cuidado de Pessoas com Necessidades Relacionadas ao COnsumo de Álcool e Outras Drogas: Guia AD. Departamento de Ações Programáticas Estratégicas., editor. Brasilia—DF; 2015.
- 36.Abreu S, Lopes J, Pereira D, Yamaoka P, Carvalho S, Simonsen A. De Unplugged a #Tamojunto: a experiência brasileira de adaptação de um programa europeu In: Sanchez Z., Schneider D., Pedroso R, editor. Prevenção ao uso de drogas no Brasil. Brasilia: Ministério da Saúde; 2017. [Google Scholar]
- 37.Faggiano F, Vigna-Taglianti FD, Versino E, Zambon A, Borraccino A, Lemma P. School-based prevention for illicit drugs use: A systematic review. Prev Med (Baltim). 2008;46: 385–396. 10.1016/j.ypmed.2007.11.012 [DOI] [PubMed] [Google Scholar]
- 38.Cainelli de Oliveira Prado M, Schneider DR, Sañudo A, Pereira APD, Horr JF, Sanchez ZM. Transcultural Adaptation of Questionnaire to Evaluate Drug Use Among Students: The Use of the EU-Dap European Questionnaire in Brazil. Subst Use Misuse. 2016;51: 449–458. 10.3109/10826084.2015.1117108 [DOI] [PubMed] [Google Scholar]
- 39.IBGE. Pesquisa Nacional da Saúde do Escolar 2012 (PeNSE) Ciência & Saúde Coletiva. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística—IBGE; 2013. [Google Scholar]
- 40.ABEP AB de E de P. Critério de Classificação Econômica do Brasil [Criteria for Economic Classification in Brazil]. In: Ibope [Internet]. São Paulo; 2012 [cited 15 Feb 2017] pp. 1–5. Available: http://www.abep.org/criterio-brasil
- 41.Matsunaga M. Item Parceling in Structural Equation Modeling: A Primer [Internet]. Communication Methods and Measures. 2008. 10.1080/19312450802458935 [DOI] [Google Scholar]
- 42.Rushton JP, Brainerd CJ, Pressley M. Behavioral development and construct validity: The principle of aggregation. Psychol Bull. 1983;94: 18–38. 10.1037/0033-2909.94.1.18 [DOI] [Google Scholar]
- 43.Hau K-T, Marsh HW. The use of item parcels in structural equation modelling: Non-normal data and small sample sizes. Br J Math Stat Psychol. 2004;57: 327–351. 10.1111/j.2044-8317.2004.tb00142.x [DOI] [PubMed] [Google Scholar]
- 44.MacCallum RC, Widaman KF, Zhang SB, Hong SH. Sample Size in Factor Analysis. Psychol Methods. 1999;4: 84–99. 10.1037/1082-989x.4.1.84 [DOI] [Google Scholar]
- 45.Little TD, Rhemtulla M, Gibson K, Schoemann AM. Why the items versus parcels controversy needn’t be one. Psychol Methods. 2013;18: 285–300. 10.1037/a0033266 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Galanti MR, Siliquini R, Cuomo L, Melero JC, Panella M, Faggiano F. Testing anonymous link procedures for follow-up of adolescents in a school-based trial: The EU-DAP pilot study. Prev Med (Baltim). 2007;44: 174–177. 10.1016/j.ypmed.2006.07.019 [DOI] [PubMed] [Google Scholar]
- 47.Levenshtein V. Binary codes capable of correcting deletions, insertions and reversals. SSSR DANeditor. Dokl Akad Nauk SSSR. Doklady Akademii Nauk SSSR; 1965;163: 845–848. [Google Scholar]
- 48.Hayes A. Introduction to mediation, moderation, and conditional process analysis: A regression-based approach Guilford Press; 2013. [Google Scholar]
- 49.Schulz KF, Altman DG, Moher D. CONSORT 2010 Statement: updated guidelines for reporting parallel group randomised trials. Trials. 2010;11: 32 10.1186/1745-6215-11-32 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Muthén L, Muthén BO. Mplus Statistical Analysis With Latent Variables User ‘ s Guide (Sixth Edition). Los Angeles, CA: Muthén & Muthén; 2010. [Google Scholar]
- 51.Raghunathan T, Lepkowski J, Van Hoewyk J, Solenberger P. A multivariate technique for multiply imputing missing values using a sequence of regression models. Surv Methodol. 2001;27: 85–95. [Google Scholar]
- 52.Schafer J. Analysis of incomplete multivariate data London: Chapman & Hall; 1997. [Google Scholar]
- 53.Rubin D. Multiple Imputation for Nonresponse in Surveys [Internet]. New York: John Wiley & Sons, Ltd; 1987. 10.1002/9780470316696 [DOI] [Google Scholar]
- 54.Enders C. Applied Missing data analysis New York: Guilford Press; 2010. [Google Scholar]
- 55.Pedroso RT, Abreu S, Kinoshita RT. Aprendizagens da intersetorialidade entre saúde e educação na prevenção do uso de álcool e outras drogas. Textura. 2015;33: 9–24. Available: http://www.periodicos.ulbra.br/index.php/txra/article/view/1339 [Google Scholar]
- 56.Foxcroft DR, Moreira MT, Almeida Santimano NM, Smith LA. Social norms information for alcohol misuse in university and college students In: Foxcroft DR, editor. Cochrane Database of Systematic Reviews. Chichester, UK: John Wiley & Sons, Ltd; 2015. 10.1002/14651858.CD006748.pub4 [DOI] [Google Scholar]
- 57.Lee NK, Cameron J, Battams S, Roche A. What works in school-based alcohol education: A systematic review. Health Educ J. 2016;75: 780–798. 10.1177/0017896915612227 [DOI] [Google Scholar]
- 58.McNeal RB, Hansen WB, Harrington NG, Giles SM. How all Stars Works: An Examination of Program Effects on Mediating Variables. Heal Educ Behav. 2004;31: 165–178. 10.1177/1090198103259852 [DOI] [PubMed] [Google Scholar]
- 59.Padon AA, Rimal RN, Jernigan D, Siegel M, DeJong W. Tapping Into Motivations for Drinking Among Youth: Normative Beliefs About Alcohol Use Among Underage Drinkers in the United States. J Health Commun. 2016;21: 1079–1087. 10.1080/10810730.2016.1222030 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Rimal RN. Modeling the relationship between descriptive norms and behaviors: A test and extension of the theory of normative social behavior (TNSB). Health Commun. 2008;23: 103–116. 10.1080/10410230801967791 [DOI] [PubMed] [Google Scholar]
- 61.Thomas R, MacLellan J, Perera R. School-based programmes for preventing smoking In: Thomas RE, editor. Cochrane Database of Systematic Reviews. Chichester, UK: John Wiley & Sons, Ltd; 2013. p. CD001293 10.1002/14651858.CD001293.pub3 [DOI] [Google Scholar]
- 62.DeJong W, Schneider SK, Towvim LG, Murphy MJ, Doerr EE, Simonsen NR, et al. A Multisite Randomized Trial of Social Norms Marketing Campaigns to Reduce College Student Drinking: A Replication Failure. Subst Abus. 2009;30: 127–140. 10.1080/08897070902802059 [DOI] [PubMed] [Google Scholar]
- 63.DeJong W, Schneider SK, Towvim LG, Murphy MJ, Doerr EE, Simonsen NR, et al. A Multisite Randomized Trial of Social Norms Marketing Campaigns to Reduce College Student Drinking. J Stud Alcohol. 2006;67: 868–879. 10.1080/08897070902802059 [DOI] [PubMed] [Google Scholar]
- 64.Scribner RA, Theall KP, Mason K, Simonsen N, Schneider SK, Towvim LG, et al. Alcohol prevention on college campuses: the moderating effect of the alcohol environment on the effectiveness of social norms marketing campaigns. J Stud Alcohol Drugs. 2011;72: 232–239. Available: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3052893/pdf/jsad232.pdf [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Ringwalt CL, Vincus A, Ennett S, Johnson R, Rohrbach LA. Reasons for Teachers’ Adaptation of Substance Use Prevention Curricula in Schools with Non-White Student Populations. Prev Sci. 2004;5: 61–67. 10.1023/B:PREV.0000013983.87069.a0 [DOI] [PubMed] [Google Scholar]
- 66.Cahill H. Challenges in adopting evidence-based school drug education programmes. Drug Alcohol Rev. 2007;26: 673–679. 10.1080/09595230701613593 [DOI] [PubMed] [Google Scholar]
- 67.Medeiros PFP, Cruz JI, Schneider DR, Sanudo A, Sanchez ZM. Process evaluation of the implementation of the Unplugged Program for drug use prevention in Brazilian schools. Subst Abuse Treat Prev Policy. 2016; 1–11. 10.1186/s13011-015-0046-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.INEP. Estudo exploratório sobre o professor brasileiro com base nos resultados do Censo escolar da Educação Básica 2007 [Internet]. Brasília: INEP; 2009. Available: portal.mec.gov.br/dmdocuments/estudoprofessor.pdf [Google Scholar]
- 69.PISA. Brasil no PISA 2015: análises e reflexões sobre o desempenho dos estudantes brasileiros São Paulo: Fundação Santillana; 2016. [Google Scholar]
- 70.Tobler NS, Roona MR, Ochshorn P, Marshall DG, Streke A V., Stackpole KM. School-Based Adolescent Drug Prevention Programs: 1998 M eta-Analysis. J Prim Prev. 2000;20: 275–336. 10.1023/A:1021314704811 [DOI] [Google Scholar]
- 71.Komro KA, Perry C, Williams C, Stigler MH, Farbakhsh K, Veblen-Mortenson S. How did Project Northland reduce alcohol use among young adolescents? Analysis of mediating variables. Health Educ Res. 2001;16: 59–70. 10.1093/her/16.1.59 [DOI] [PubMed] [Google Scholar]
- 72.Onrust SA, Otten R, Lammers J, Smit F. School-based programmes to reduce and prevent substance use in different age groups: What works for whom? Systematic review and meta-regression analysis. Clin Psychol Rev. 2016;44: 45–59. 10.1016/j.cpr.2015.11.002 [DOI] [PubMed] [Google Scholar]
- 73.Strøm HKH, Adolfsen F, Fossum S, Kaiser S, Martinussen M, Belcher H, et al. Effectiveness of school-based preventive interventions on adolescent alcohol use: a meta-analysis of randomized controlled trials. Subst Abuse Treat Prev Policy. 2014;9: 48 10.1186/1747-597X-9-48 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOCX)
(DOCX)
(DOCX)
(PDF)
(XLS)
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.