

Abstract
The purpose of this research was to assess the association between Gender Inequality Index and prevalence of lifetime intimate partner violence (IPV) among women and men at the state-level. Recently developed 2017 state-level prevalence estimates of IPV among a nationally-representative sample of U.S. non-institutionalized adults between 2010–2012 from the National Intimate Partner and Sexual Violence Survey was combined with calculated indexes for state-level gender inequality. Gender Inequality Index, created by the United Nations, reflects gender-based disadvantage in reproductive health, empowerment, and labor market participation. Correlations and linear regressions were used to examine associations between gender inequality and IPV. Gender Inequality Index values ranged from 0.149 to 0.381. The lifetime prevalence of IPV ranged between 27.8% and 45.3% for women and between 18.5% and 38.6% for men. Across states, the Gender Inequality Index was positively correlated with the prevalence of any form of IPV (r=0.28, p<.05) and psychological IPV among women (r=0.41, p <.01). The adjusted regression model showed a positive association between gender inequality and psychological IPV among women (B = 1.61, SE = .57, p = .007). Structural changes to gender inequality may help to reduce occurrences of IPV and improve the wellbeing and livelihood of women and girls.
1. Introduction
Intimate partner violence (IPV) is a significant public health issue. According to the Centers for Disease Control and Prevention (CDC), IPV describes “any physical, sexual, or psychological harm by a current or former partner or spouse”(Black et al., 2011). In the United States, the estimated lifetime prevalence of IPV experienced by women and men is 35.6% and 28.5%, respectively (Black et al., 2011). Extensive research has demonstrated a myriad of negative health implications of IPV such as mental health symptoms, substance use, physical injuries, and HIV/STI infections (Campbell, 2002; Campbell & Soeken, 1999). In addition to poor health consequences, IPV has additional economic costs. In the United States, the costs of IPV can amount to $5.8 billion annually, of which the majority is related to direct medical and mental health care services (National Center for Injury Prevention and Control, 2003). IPV is a preventable public health issue, and finding ways to reduce the incidence of IPV in the United States requires addressing ecological risk factors of IPV.
The social-ecological model provided a comprehensive framework to better understand and address potential risk factors of IPV (National Center for Injury Prevention and Control, 2015). The social-ecological model considers how risk factors across four ecological levels (i.e., societal, community, relationship, and individual) places people at a greater risk for experiencing and/or perpetrating IPV (National Center for Injury Prevention and Control, 2015). A number of studies have shown how risk factors on the individual, community, and relationship levels are associated with IPV victimization (Walton-Moss, Manganello, Frye, & Campbell, 2005; Willie, Powell, Lewis, Callands, & Kershaw, 2017) and perpetration (Capaldi, Knoble, Shortt, & Kim, 2012; Lipsky, Caetano, Field, & Larkin, 2005). For example, at the individual-level, several studies have shown that experiences of child abuse are positively associated with IPV victimization (Bensley, Van Eenwyk, & Wynkoop Simmons, 2003; Campbell, Greeson, Bybee, & Raja, 2008; Sullivan, Meese, Swan, Mazure, & Snow, 2005). At the community-level, some studies have found that characteristics of one’s social and physical environment, such as community poverty rates, are associated with IPV perpetration (Capaldi et al., 2012). To date, IPV prevention research has provided great insight for the development of individual-level and community-level interventions. However, more research is needed to address how societal-level factors can create an environment that legitimizes and encourages IPV.
Gender inequality is a societal-level risk factor that has received increasing global attention but remains understudied in the United States. According to the United Nations, gender inequality captures “the extent to which men have a better status than women in the context of the social, economic, and political arenas”(United Nations Development Programme, 2013). Recognizing that gender inequality is a multi-dimensional concept, the United Nations created the Gender Inequality Index that evaluates gender differences in three important domains: reproductive health, empowerment, and economic status. In the context of the societal-level of the social-ecological model, gendered stereotypes can lead to unequal access and distribution of resources such as education, employment, and healthcare. Biased access and distribution of resources can lead to gender inequalities between women and men, which favor men. Several studies have shown that countries with high levels of gender inequality are associated with female genital mutilation (Kaplan, Hechavarría, Martín, & Bonhoure, 2011), child mortality rates (Brinda, Rajkumar, & Enemark, 2015), child malnutrition (Marphatia, Cole, Grijalva-Eternod, & Wells, 2016), and obesity (Garawi, Devries, Thorogood, & Uauy, 2014).
Recently, gender inequality has been distinguished as a risk factor for multiple forms of violence. For example, an ecological study in Spain found that the prevalence of IPV was higher in communities with greater gender inequality (Redding, Ruiz-Cantero, Fernández-Sáez, & Guijarro-Garvi, 2017). Also, a cross-national ecological study found a positive association between country-level gender inequality and country-level prevalence of child abuse and neglect (Klevens & Ports, 2017). These studies highlight how gender differences in roles and behaviors can create inequalities, and possibly encourage an environment in which one group becomes empowered and other is disadvantaged (e.g., men being empowered and women being subordinate) (World Health Organization, 2009). In addition to empirical support, there is theoretical support for gender inequality as a risk factor of violence, particularly violence against women. The theory of gender and power proposes that gender inequalities between women and men can place constraints on women’s lifestyles, economic potential, resource allocation, and roles (Connell, 2014). In particular, traditional gender roles and unequal power between women and men may legitimatize the use of violence against women. Similarly, feminist theories postulate that violence is used as a tactic to exert control and dominance over women (Bell & Naugle, 2008). Despite empirical and theoretical underpinnings, only one study in the United States has examined associations between gender inequality and violence. Gressard and colleagues found that state-level prevalence of gender inequality was associated with female adolescent dating violence victimization (Gressard, Swahn, & Tharp, 2015). These findings address an important link between gender inequality and dating violence and while teen dating violence and IPV are associated (Manchikanti Gómez, 2011), the epidemiology of each type of violence might be different. Therefore, additional research is needed to understand whether state-level gender inequality is associated with state-level prevalence of IPV victimization experienced by women and men. We hypothesized that states with higher levels of gender inequality would report high prevalence estimates of IPV victimization by women and not men.
2. Methods
2.1. Sample
This study obtained state-level data from multiple sources (described below). This study focused on the 50 U.S. states and the District of Columbia because data for IPV victimization was not available for the U.S. territories (i.e., Puerto Rico; the U.S. Virgin Islands; Guam and the Northern Mariana Islands; and American Samoa).
2.2. Measures
We obtained state-level prevalence estimates for IPV from the State Report of the 2010–12 National Intimate Partner and Sexual Violence Survey (Smith et al., 2017). The National Intimate Partner and Sexual Violence Survey measured five forms of IPV: contact sexual violence, stalking, physical violence, psychological aggression, and control of reproductive or sexual health. The National Intimate Partner and Sexual Violence Survey defines contact sexual violence as “a combined measure including rape, being made to penetrate someone else, sexual coercion, and/or unwanted sexual contact”; stalking is “a pattern of harassing or threatening tactics used by a perpetrator that is both unwanted and causes fear or safety concerns in the victim”; and physical violence as “a range of behaviors from slapping, pushing or shoving to severe acts” (Smith et al., 2017). Also, psychological aggression “includes expressive aggression and coercive control” and control of reproductive or sexual health includes the refusal by an intimate partner to use a condom (Smith et al., 2017). For this study, we only included IPV estimates that were available for both women and men. Thus, we used three types of state-level prevalence estimates for IPV (see Figure 1 in Supplemental Material). The first type of IPV represents the proportion of people in each state population with a history of either contact sexual violence, physical violence, and/or stalking (hereafter known as Any form of IPV victimization). The second type of IPV represents the proportion of people in each state population with a history of only physical IPV victimization. The third type of IPV represents the proportion of people in each state with a history of experiencing psychological aggression (hereafter known as psychological IPV).
Figure 1.
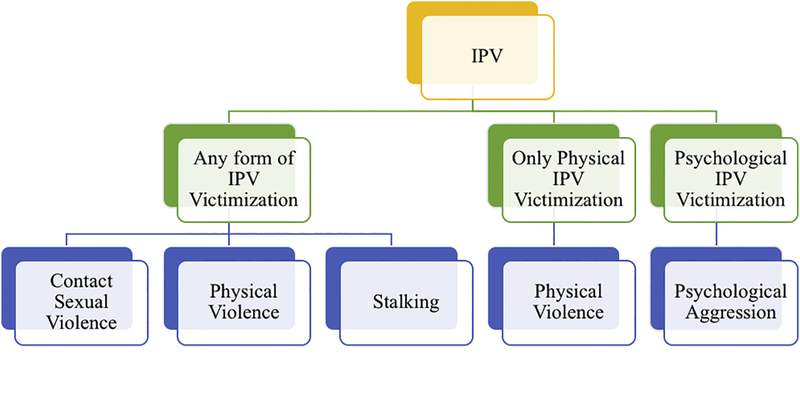
Graphical depiction of the operationalization of intimate partner violence (IPV). Green boxes illustrate the three types of IPV analyzed in the current study. Blue boxes illustrate the types of IPV collected in the National Intimate Partner and Sexual Violence Survey (NISVS). Control of reproductive health is not shown in this figure but was captured in the NISVS
State-level Gender Inequality Indexes were calculated using methods outlined in the United Nations Development Programme report (United Nations Development Programme, 2016). State-level gender inequality was calculated based on five indicators: 1) maternal mortality ratio, 2) teen birth rate, 3) government representation, 4) educational attainment, and 5) labor force participation. The United Nations defines maternal mortality ratio as the ratio of the number of maternal deaths during a given time period per 100,000 live births during the same-time period (https://mdgs.un.org/unsd/mdg/Metadata.aspx?IndicatorId=0&SeriesId=553). In 2009, the National Vital Statistics Reports did not report maternal mortality data due to a revision on the U.S. Standard Certificate of Death which led to differential reporting and identification of maternal deaths across states (Murphy, Xu, & Kochanek, 2013). As a result, estimates for state-level maternal mortality were calculated using the data from the CDC Wonder database (Centers for Disease Control Prevention, 1999). Using the CDC Wonder database, maternal deaths were captured as the number of deaths that were proximal to pregnancy, childbirth, and the puerperium (ICD 10 O00-O99). To construct state-level maternal mortality, we divided the number of live births by the number of maternal deaths, and then multiplied by 100,000. Several states had unreliable estimates for maternal deaths in 2009. As a result, we constructed a state-level maternal mortality rate from 2005–2009. Maternal mortality estimates were unreliable for four states (i.e., Alaska, Maine, Rhode Island, and Vermont) across this five year range, and as a result, the threshold value of 10 deaths per 100,000 was used for those states. This threshold value was chosen due to the sensitivity analyses conducted by the Human Development Report Office (Gaye, Klugman, Kovacevic, Twigg, & Zambrano, 2010). In particular, this threshold helps to “avoid the statistical uncertainty in relatively very small numbers” and countries with less than 10 deaths per 100,000 are performing at a similar level (Gaye et al., 2010). State-level estimates for teen birth rates were obtained from the National Vital Statistics Reports for 2009. The teen birth rates were defined as the number of live births per 1,000 women ages 15–19 years old (Murphy et al., 2013). For government representation, the percentage of women and men in the state legislature in 2009 was used (Women’s Legislative Network of NCSL, 2010). For educational attainment, the percentage of women and men ≥25 years who reported having at least a high school diploma from the American Community Survey was used (U.S. Census Bureau, 2010). For the labor force participation, the percentage of women and men between the ages of 20–64 years in a non-institutionalized population who participated in the labor force (i.e., either employed or unemployed) was used from the American Community Survey (U.S. Census Bureau, 2010). According to the American Community Survey, unemployed individuals were classified in the civilian labor force if they met the criteria were at least 16 years old and “if they 1) were neither “at work” nor “with a job but not at work” during the reference week, and 2) were actively looking for work during the last four weeks, and 3) were available to start a job” (U.S. Census Bureau, 2010).
State-level sociodemographic factors were obtained from the U.S. Census Bureau through the American Community Survey (U.S. Census Bureau, 2010). The sociodemographic factors that were tested for statistical significance with state-level IPV prevalence in this study were: median age (in years), median household income ($1,000 increments), and percentage of the population that identified as Hispanic, non-Hispanic African descent, non-Hispanic Asian, non-Hispanic American Indian, and non-Hispanic Native Hawaiian and Other Pacific Islander.
2.3. Analysis
Pearson correlation coefficients were used to examine the association between the Gender Inequality Index, indicators of gender inequality, IPV prevalence estimates for women and men, and socio-demographics. Linear regression was used to model the relationship between gender inequality and prevalence estimates of IPV, controlling for state-level sociodemographic factors. State-level sociodemographic factors that were significantly correlated with IPV prevalence estimates for women and/or men were controlled for in the regression analyses. A standardized version of gender inequality was used a predictor in the regression analyses. The standardized version of gender inequality is the z-score. The z-score was used in order to provide an appropriate and meaningful characterization of the effect size for gender inequality. Residual plots and collinearity diagnostics were examined for heteroscedasticity and multicollinearity issues. Data on IPV and Gender Inequality Index were imported and analyzed using SPSS version 24 (IBM SPSS Statistics, 2012). Analyses were conducted in 2017 and this study was exempted by Yale University’s Institutional Review Board.
3. Results
3.1. Characterizing State-Level IPV Estimates and Gender Inequality Index Values
As reported in the National Intimate Partner and Sexual Violence Survey State Report, there were differences in state-level lifetime prevalence estimates for any form of IPV against women and men (Table 1).(Smith et al., 2017) Kentucky (45.3%), Nevada (43.8%), and Alaska (43.3%) had the highest estimated prevalence for any form of women’s IPV victimization. Virginia (38.6%), Idaho (38.2%), and Oklahoma (37.8%) had the highest estimated prevalence for any form of men’s IPV victimization.
Table 1.
State-Level Gender Inequality Index Values and Prevalence Estimates of Intimate Partner Violence Victimization for Women and Men in the 50 U.S. States and D.C., 2010
| Womena | Mena | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| State | Gender Inequality Index |
Rank for Gender Inequality Index |
Any IPV |
Rank for Any IPV |
Physical IPV |
Psychologica 1 IPV |
Any IPV | Rank for Any IPV |
Physica 1IPV |
Psychologica 1 IPV |
| Alabama | 0.259 | 29 | 37.5 | 27 | 32.4 | 46.4 | 29.5 | 18 | 28.6 | 44.8 |
| Alaska | 0.381 | 51 | 43.3 | 49 | 33.2 | 54.2 | 30.2 | 19 | 26.9 | 50.4 |
| Arizona | 0.368 | 49 | 42.6 | 48 | 38.6 | 55.4 | 33.4 | 36 | 29.8 | 55.4 |
| Arkansas | 0.313 | 40 | 40.8 | 42 | 34 | 45.2 | 34.8 | 40 | 33.5 | 53.9 |
| California | 0.231 | 18 | 34.9 | 16 | 30 | 44.6 | 31.1 | 26 | 27.9 | 50.2 |
| Colorado | 0.341 | 45 | 36.8 | 23 | 32.4 | 47.4 | 30.5 | 23 | 29.4 | 50.9 |
| Connecticut | 0.149 | 1 | 37.7 | 30 | 31.7 | 44.8 | 33.9 | 38 | 32.1 | 47.6 |
| Delaware | 0.213 | 9 | 37.6 | 28 | 34.9 | 39.7 | 32.7 | 32 | 32 | 47.1 |
| District of Columbia | 0.345 | 46 | 39.0 | 33 | 35.1 | 50.1 | 25.5 | 7 | 23.9 | 52.8 |
| Florida | 0.247 | 24 | 37.9 | 31 | 34.1 | 46 | 29.3 | 16 | 26.9 | 46.2 |
| Georgia | 0.268 | 31 | 37.4 | 26 | 33.7 | 45.5 | 30.4 | 21 | 27.9 | 49.7 |
| Hawaii | 0.240 | 21 | 34.7 | 14 | 31 | 43.5 | 24.1 | 4 | 23.2 | 41.6 |
| Idaho | 0.271 | 32 | 33 | 5 | 28.4 | 43.5 | 38.2 | 50 | 34.1 | 48.6 |
| Illinois | 0.217 | 10 | 41.5 | 44 | 33.9 | 48.4 | 25.9 | 9 | 24.2 | 41 |
| Indiana | 0.380 | 50 | 42.5 | 47 | 36.6 | 51.8 | 27.9 | 11 | 27.1 | 52.5 |
| Iowa | 0.183 | 4 | 35.3 | 18 | 28.6 | 45.4 | 29.3 | 16 | 27.1 | 42 |
| Kansas | 0.249 | 25 | 33.9 | 9 | 28.4 | 45.8 | 31.1 | 26 | 29.9 | 42.9 |
| Kentucky | 0.280 | 33 | 45.3 | 51 | 42.1 | 57.2 | 35.5 | 45 | 32.1 | 47.7 |
| Louisiana | 0.263 | 30 | 35.9 | 20 | 31.7 | 46.9 | 35.2 | 42 | 30.8 | |
| Maine | 0.291 | 36 | 39.3 | 35 | 34.2 | 53.5 | 33.6 | 37 | 32.3 | 52.7 |
| Maryland | 0.224 | 14 | 34.4 | 13 | 28.8 | 48.6 | 28.8 | 13 | 26.8 | 41.6 |
| Massachusetts | 0.309 | 38 | 33.9 | 9 | 26.8 | 44.1 | 31.7 | 28 | 30.3 | 47.5 |
| Michigan | 0.257 | 27 | 36.1 | 21 | 31.3 | 51.9 | 25.8 | 8 | 23.3 | 42.5 |
| Minnesota | 0.311 | 39 | 33.9 | 9 | 26.2 | 42.3 | 25.1 | 5 | 23.5 | 38.7 |
| Mississippi | 0.340 | 44 | 39.7 | 38 | 34.8 | 46.1 | 31.7 | 28 | 30.4 | 46.9 |
| Missouri | 0.245 | 23 | 41.8 | 45 | 37.8 | 54.8 | 35.2 | 42 | 32.8 | 54 |
| Montana | 0.287 | 35 | 37.2 | 25 | 30.3 | 47 | 34.6 | 39 | 32.5 | 51.3 |
| Nebraska | 0.228 | 16 | 33.7 | 8 | 30 | 46.9 | 28 | 12 | 24.8 | 45.3 |
| Nevada | 0.191 | 6 | 43.8 | 50 | 38.7 | 50.8 | 32.8 | 33 | 31.1 | 56.2 |
| New Hampshire | 0.178 | 2 | 34.7 | 14 | 28.2 | 45.1 | 35.4 | 44 | 31.9 | 42.8 |
| New Jersey | 0.218 | 11 | 35.8 | 19 | 26.3 | 43.1 | 27.4 | 10 | 27 | 44.4 |
| New Mexico | 0.286 | 34 | 37.6 | 28 | 31.1 | 48 | 33.3 | 35 | 31.5 | 49.1 |
| New York | 0.230 | 17 | 31.7 | 3 | 28.5 | 40.7 | 29 | 14 | 25.2 | 46 |
| North Carolina | 0.209 | 8 | 35.2 | 17 | 32.3 | 44.4 | 30.3 | 20 | 26.5 | 43.1 |
| North Dakota | 0.257 | 27 | 29.7 | 2 | 27.4 | 42.8 | 18.5 | 1 | 17.8 | 41.5 |
| Ohio | 0.243 | 22 | 38 | 32 | 34.5 | 46.8 | 33 | 34 | 31.3 | 48.8 |
| Oklahoma | 0.360 | 48 | 40.1 | 40 | 37.3 | 52.3 | 37.8 | 49 | 36.1 | 52 |
| Oregon | 0.190 | 5 | 39.8 | 39 | 35 | 52.4 | 36.2 | 46 | 34.4 | 44.5 |
| Pennsylvania | 0.253 | 26 | 37.1 | 24 | 32.1 | 46.3 | 30.4 | 21 | 27.8 | 40.4 |
| Rhode Island | 0.320 | 41 | 32.6 | 4 | 28.9 | 44.5 | 25.4 | 6 | 24.1 | 41.5 |
| South Carolina | 0.345 | 46 | 42.3 | 46 | 36.4 | 53.1 | 29.2 | 15 | 25.4 | 44 |
| South Dakota | 0.238 | 20 | 27.8 | 1 | 25.4 | 36.6 | 23.6 | 3 | 22.8 | 29.3 |
| Tennessee | 0.226 | 15 | 39.6 | 37 | 34.2 | 48.1 | 36.8 | 48 | 33.8 | 52.8 |
| Texas | 0.293 | 37 | 40.1 | 40 | 35.1 | 52 | 34.9 | 41 | 31.1 | 52.2 |
| Utah | 0.223 | 13 | 33.6 | 6 | 26.8 | 41.6 | 21.4 | 2 | 19.3 | 41.5 |
| Vermont | 0.323 | 42 | 39.2 | 34 | 32.8 | 51.2 | 30.9 | 25 | 28.9 | 45.6 |
| Virginia | 0.191 | 6 | 33.6 | 6 | 30 | 44.6 | 38.6 | 51 | 27 | 43.5 |
| Washington | 0.180 | 3 | 41.4 | 43 | 37.5 | 48.7 | 31.7 | 28 | 28 | 46.9 |
| West Virginia | 0.237 | 19 | 39.4 | 36 | 36.3 | 48.5 | 36.3 | 47 | 34 | 50.9 |
| Wisconsin | 0.219 | 12 | 36.3 | 22 | 31.2 | 48 | 32.1 | 31 | 28.7 | 45.7 |
| Wyoming | 0.337 | 43 | 33.9 | 9 | 29.7 | 51.9 | 30.5 | 23 | 28.2 | 40.9 |
As reported in the National Intimate Partner and Sexual Violence Survey State Report1
Rankings are in ascending order (arranged from smallest to largest)
State-level Gender Inequality Indexes are displayed in Table 1. Gender Inequality Indexes ranged from 0.149 to 0.381, with a mean of 0.26 and standard deviation of 0.05 (Table 2). Connecticut (0.149), New Hampshire (0.178), and Washington (0.180) had the three smallest values for gender inequality. Alaska (0.381), Indiana (0.380) and Arizona (0.368) had the three highest values for gender inequality.
Table 2.
Means, Standard Deviations, and Correlations with Gender Inequality, Prevalence Estimates of Intimate Partner Violence among Women and Men, and Socio-demographics in the 50 U.S. States and D.C., 2010
| M (SD) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Gender Inequality Index | .26 (.05) | - | |||||||||||||
| 2. Any IPV—Women | 37.7 (3.7) | .28* | - | ||||||||||||
| 3. Physical IPV—Women | 32.3 (3.8) | .22 | .89** | - | |||||||||||
| 4. Psychological IPV-Women | 47.4 (4.3) | .41** | .77** | .73** | - | ||||||||||
| 5. Any IPV—Men | 30.9 (4.4) | −.06 | .42** | .44** | .36** | - | |||||||||
| 6. Physical IPV—Men | 28.5 (3.9) | .01 | .47** | .47** | .36** | .92** | - | ||||||||
| 7. Psychological IPV Men | 46.6 (5.1) | .29* | .67** | .64** | .53** | .56** | .60** | - | |||||||
| 8. Age | 27.5 (2.3) | −.21 | −.01 | .02 | .02 | .20 | .27 | −.10 | - | ||||||
| 9. Income | 49.9 (8.1) | −.22 | −.27 | −.42** | −.24 | −.29* | −.34* | −.23 | −.06 | - | |||||
| 10. Hispanic or Latino | 10.6 (9.9) | −.01 | .08 | .05 | .03 | .06 | .05 | .28* | −.35* | .15 | - | ||||
| 11.Non-Hispanic African Descent | 12.1 (11.8) | .08 | .17 | .22 | .001 | −.01 | −.07 | .14 | −.20 | −.01 | −.04 | - | |||
| 12. Non-Hispanic Asian | 4.3 (6.3) | −.18 | −.09 | −.09 | −.18 | −.21 | −.22 | −.05 | −.04 | .48** | .29* | −.07 | - | ||
| 13. Non-Hispanic American Indian | 1.7 (3.5) | .32* | .02 | −.06 | −.01 | .01 | .01 | −.03 | −.23 | .06 | .27 | −.30* | −.10 | - | |
| 14. Non-Hispanic Native Hawaiian | .003 (.01) | −.06 | −.05 | −.03 | −.11 | −.23 | −.21 | −.11 | −.02 | .26 | .02 | −.17 | .87** | −.01 | - |
IPV= Intimate Partner Violence.
p < .05
p < .01,
p < .001.
Any IPV, refers to contact sexual, physical, and stalking victimization by an intimate partner.
3.2. Bivariate Correlations between State-Level Gender Inequality Values and IPV Estimates
Table 2 shows the correlations between gender inequality, IPV prevalence estimates for women and men, and state-level demographics. Gender inequality was positively correlated with any form of IPV for women (r = .28, p = .01) and psychological IPV for women (r = .41, p < .01). For men, gender inequality was positively correlated with psychological IPV (r = .29, p < .05).
3.3. Bivariate Correlations between Indicators of State-Level Gender Inequality and IPV Estimates
3.3.A. Women’s IPV Victimization
There were significant correlations between the indicators for gender inequality and IPV victimization among women. Teen birth rate was positively correlated with any form of IPV victimization (r = .43, p <.01), physical IPV victimization (r = .54, p < .001), and psychological IPV victimization among women (r = .34, p = .01). Educational attainment for women was inversely associated with any form of IPV victimization (r = −.33, p = .01) and physical IPV victimization among women (r = −.43, p = .002). Educational attainment for men was inversely associated with any form of IPV victimization (r = −.49, p < .001) and physical IPV victimization (r = −.53, p < .001). Labor force participation for women was inversely associated with any form of IPV victimization (r = −.50, p < .001), physical IPV victimization (r = −.53, p < .001), and psychological IPV victimization among women (r = −.30, p = .03). Labor force participation for men was inversely associated with any form of IPV victimization (r = −.48, p < .001), physical IPV victimization (r = −.59, p < .001), and psychological IPV victimization among women (r = .32, p = .02).
3.3.B. Men’s IPV Victimization
There were also significant correlations between the indicators for gender inequality and IPV victimization among men. Teen birth rate was positively correlated with physical IPV victimization (r = .29, p = .03) and psychological IPV victimization among men (r = .40, p = .003). Educational attainment for women was inversely associated with psychological IPV victimization among men (r = −.39, p = .005). Educational attainment for men was inversely associated with any form of IPV victimization (r = −.32, p = .02), physical IPV victimization (r = −.28, p = .04), and psychological IPV victimization among men (r = −.35, p = .01). Labor force participation for women was inversely associated with any form of IPV victimization (r = −.44, p = .001), physical IPV victimization (r = −.42, p = .002), and psychological IPV victimization among men (r = −.47, p = .001). Labor force participation for men was inversely associated with any form of IPV victimization (r = −.43, p = .002), physical IPV victimization (r = −.45, p = .001), and psychological IPV victimization among men (r = −.42, p = .002).
3.4. Regression Associations between State-Level Gender Inequality and IPV Estimates
Bivariate models showed a positive association between gender inequality and two forms of IPV victimization experienced by women: lifetime prevalence of any form of IPV and psychological IPV only (Table 3). However, after controlling for median income, only the association between gender inequality and psychological IPV victimization among women remained significant. The multivariable model showed that a one standard deviation increase in the Gender Inequality Index was associated with a 1.61 percentage point increase in the prevalence of women’s psychological IPV (SE = .57, p = .007). The standard deviation is 1 because the z-score value of the Gender Inequality Index was used. In the multivariable models, gender inequality was not significantly associated with men’s IPV victimization (Table 3). No issues of heteroscedasticity and multicollinearity were found.
Table 3.
Bivariate and Multivariable Associations between State-Level Gender Inequality and State-Level Prevalence Estimates of Intimate Partner Violence among Women and Men in the 50 U.S. States and D.C., 2010.
| Women | Men | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Any IPVe | Physical IPV | Psychological IPV |
Any IPVe | Physical IPV | Psychological IPV |
|||||||
| B (SE) | R2 | B (SE) | R2 | B (SE) | R2 | B (SE) | R2 | B (SE) | R2 | B (SE) | R2 | |
| Gender Inequality Indexa,d | 1.03 (.50) | .05 | 0.83 (.52) | .03 | 1.76 (.56) | .15 | −.28 (.62) | .01 | .04 (.56) | .02 | 1.52 (.70) | .07 |
| p-value | .05 | .12 | .003 | .65 | .28 | .03 | ||||||
| Gender Inequality Indexb,c,d | .84 (.51) | .10 | 0.49 (.50) | .15 | 1.61 (.57) | .16 | −.59 (.61) | .06 | −.28 (.55) | .08 | 1.33 (.72) | .11 |
| p-value | .15 | .32 | .007 | .33 | .61 | .07 | ||||||
Bivariate association.
Multivariable association.
Adjusting for median income (in $1000 increments).
Regression coefficients can be interpreted as one standard deviation increase in the Gender Inequality Index value is associated with an increase or decrease in the prevalence of IPV victimization.
Any Form of IPV, refers to contact sexual, physical, and stalking victimization by an intimate partner.
4. Discussion
This is one of the first studies to examine the associations between state-level gender inequality and prevalence of IPV among women and men in the United States. The Gender Inequality Index captures the loss in human development and achievements due to gender disparities with values ranging from 0 (perfect equality) to 1 (total inequality) (Gaye et al., 2010). Although the United States has consistently ranked among the top 50 countries for low gender inequality (Gaye et al., 2010), our study demonstrates great variation in gender inequality among the individual states. For example, in Connecticut, there is only a 15 percent loss in human development due to gender inequality; unlike Alaska where gender inequality accounts for 38 percent loss in human development. These findings suggest that women’s wellbeing and experiences of gender disadvantage are different according to the state one resides. Consistent with our hypothesis, our findings suggest that higher values of gender inequality was associated with higher values for the prevalence of IPV experienced by women. These findings may have important implications for structural-level interventions to reduce IPV against women in the United States.
Our findings suggest that state-level gender inequality is associated with the state-level estimates for IPV victimization among women, but not among men. In general, these findings are align with research among U.S. adolescents (Gressard et al., 2015) and adult women in other countries (Redding et al., 2017). For example, Gressard et al. (2015) found that gender inequality in the United States was associated with physical dating victimization among female adolescents, but inequality did not relate to dating victimization among male adolescents (Gressard et al., 2015). Similarly, Redding and colleagues found greater gender inequality was associated with higher rates of IPV-related mortality among women (Redding et al., 2017). According to feminist theory, the social constructions of gender produce social norms that influence relationships and interactions between women and men (Heise & Kotsadam, 2015; Renzetti, Edleson, & Bergen, 2011; United Nations Development Programme, 2013). In patriarchal societies, violence can be used to subordinate women in order to gain and maintain power and control (Yodanis, 2004). Thus, it is possible that gender-based inequities between women and men creates an environment that legitimizes IPV against women, minimizes these experiences, and/or sanctions weak criminalization policies for IPV. More research on the impact of societal-level determinants of IPV in the United States are needed. For example, it may be useful for future research to examine the relationship between gender inequality and restrictive (e.g., policies permitting insurance discrimination against individuals with a history of IPV) vs. protective IPV-related policies (e.g., policies prohibiting discrimination against employees with a history of IPV) in the United States.
All of the individual indicators of the Gender Inequality Index except government representation were significantly correlated with IPV victimization for both women and men. It is possible that reproductive health, educational attainment, and labor force participation are stronger indicators and dimensions of state-level gender inequality than government representation. This finding is contrary to other studies that have used political participation among women and men as an important proxy for gender inequality (Kenworthy & Malami, 1999). It would be useful for future research to investigate broader forms of political participation that might be more indicative of gender inequality in the United States such as women’s political empowerment “a process of increasing capacity for women, leading to greater choice, agency, and participation in societal decision-making” (Sundström, Paxton, Wang, & Lindberg, 2017).
4.1. Study Limitations and Strengths
There are several study limitations that should be taken into consideration. The National Intimate Partner and Sexual Violence Survey is a unique and rich dataset describing the epidemiology of intimate partner and sexual violence in the United States (Centers for Disease Control Prevention, 2010). However, for this study we only included state-level prevalence estimates that were available for both women and men and across the majority of states. It would be useful for future research to replicate our study with a new wave of National Intimate Partner and Sexual Violence Survey data, if that becomes available. Due to state-level measurement issues with maternal mortality, the current measure for maternal mortality ratio might be under-reported for some states. Consistent state-level surveillance measures for maternal mortality are needed in order to improve the precision of the Gender Inequality Index and inform programming for maternal health. Due to the low sample size, this study was only able to control for a small number of potential covariates. Thus, the multivariable linear regression results are subject to confounding by other potential variables. Finally, ecological studies are useful for examining associations at the population-level. Since the data in the study is aggregated at the state-level, our findings cannot guarantee that an association is present at the individual-level (i.e., ecological fallacy). Future research should explore the implications of gender inequality and prevalence of IPV at the individual-level.
In conclusion, there is evidence to suggest that gender inequality relates to IPV prevalence estimates in the United States, specifically among women. In this study, we examined the association between gender inequality and IPV prevalence among women and men across 50 United States and the District of Columbia. Thus, our findings may have important implications for structural-level changes that can occur among states with high Gender Inequality Index values. In particular, states with high Gender Inequality Index values may need to devise ways to reduce gender-based inequities. Creating an egalitarian environment that supports the wellbeing of women may weaken gender power dynamics and reduce the incidence of IPV. Some ways that states with high Gender Inequality Index values can improve women’s status and potentially reduce IPV incidence is by establishing state campaigns that promote women and girls’ involvement in the labor force and higher education areas and implement campaigns that change discriminatory gender-based norms and attitudes. Comprehensive approaches to dismantle gender inequality may help reduce occurrences of IPV and improve the wellbeing and livelihood of women.
Highlights.
There is state-level variation in gender inequality index scores
Gender inequality was associated with higher psychological IPV among women
Gender inequality was not associated with IPV among men
Acknowledgements
This research was supported, in part, by the National Institute of Mental Health (F31MH113508; T32MH020031; R25MH083620).
This research was supported, in part, by the National Institute of Mental Health under F31MH113508 (PI: Tiara C. Willie, MA).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Disclosures
The authors report no conflict of interests.
The authors report no real or perceived vested interests that relate to this article that could be construed as a conflict of interest.
Contributor Information
Tiara C. Willie, Chronic Disease Epidemiology, Yale School of Public Health, New Haven, Connecticut, USA..
Trace S. Kershaw, Social and Behavioral Sciences, Yale School of Public Health, and Director of T32 Training, Center for Interdisciplinary Research on AIDS, New Haven, Connecticut, USA..
References
- Bell KM, & Naugle AE (2008). Intimate partner violence theoretical considerations: Moving towards a contextual framework. Clinical Psychology Review, 28(7), 1096–1107. [DOI] [PubMed] [Google Scholar]
- Bensley L, Van Eenwyk J, & Wynkoop Simmons K. (2003). Childhood family violence history and women’s risk for intimate partner violence and poor health. American Journal of Preventive Medicine, 25(1), 38–44. [DOI] [PubMed] [Google Scholar]
- Black MC, Basile KC, Breiding MJ, Smith SG, Walters ML, Merrick MT, & Stevens M (2011). National intimate partner and sexual violence survey Atlanta, GA: Centers for Disease Control and Prevention. [Google Scholar]
- Brinda EM, Rajkumar AP, & Enemark U (2015). Association between gender inequality index and child mortality rates: a cross-national study of 138 countries. BMC Public Health, 15(1), 97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Campbell JC (2002). Health consequences of intimate partner violence. The Lancet, 359(9314), 1331–1336. [DOI] [PubMed] [Google Scholar]
- Campbell JC, & Soeken KL (1999). Forced Sex and Intimate Partner Violence: Effects on Women’s Risk and Women’s Health. Violence Against Women, 5(9), 1017–1035. doi: 10.1177/1077801299005009003 [DOI] [Google Scholar]
- Campbell R, Greeson MR, Bybee D, & Raja S (2008). The co-occurrence of childhood sexual abuse, adult sexual assault, intimate partner violence, and sexual harassment: a mediational model of posttraumatic stress disorder and physical health outcomes. Journal of Consulting and Clinical Psychology, 76(2), 194–207. doi: 10.1037/0022-006X.76.2.194 [DOI] [PubMed] [Google Scholar]
- Capaldi DM, Knoble NB, Shortt JW, & Kim HK (2012). A systematic review of risk factors for intimate partner violence. Partner Abuse, 3(2), 231–280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control Prevention. (1999). Underlying cause of death 1999–2013 on CDC WONDER online database, released 2015
- Centers for Disease Control Prevention. (2010). The national intimate partner and sexual violence survey (NISVS) Atlanta, GA: National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. [Google Scholar]
- Connell RW (2014). Gender and power: Society, the person and sexual politics: John Wiley & Sons. [Google Scholar]
- Garawi F, Devries K, Thorogood N, & Uauy R (2014). Global differences between women and men in the prevalence of obesity: is there an association with gender inequality? European Journal of Clinical Nutrition, 68(10), 1101–1106. [DOI] [PubMed] [Google Scholar]
- Gaye A, Klugman J, Kovacevic M, Twigg S, & Zambrano E (2010). Measuring key disparities in human development: The gender inequality index. Human Development Research Paper, 46, 1–37. [Google Scholar]
- Gressard LA, Swahn MH, & Tharp AT (2015). A first look at gender inequality as a societal risk factor for dating violence. American Journal of Preventive Medicine, 49(3), 448–457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heise LL, & Kotsadam A (2015). Cross-national and multilevel correlates of partner violence: an analysis of data from population-based surveys. The Lancet Global Health, 3(6), e332–e340. [DOI] [PubMed] [Google Scholar]
- IBM SPSS Statistics. (2012). IBM SPSS Statistics 21.0 for Windows Chicago: IBM. [Google Scholar]
- Kaplan A, Hechavarría S, Martín M, & Bonhoure I (2011). Health consequences of female genital mutilation/cutting in the Gambia, evidence into action. Reproductive health, 8(1), 26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kenworthy L, & Malami M (1999). Gender inequality in political representation: A worldwide comparative analysis. Social Forces, 78(1), 235–268. [Google Scholar]
- Klevens J, & Ports KA (2017). Gender Inequity Associated with Increased Child Physical Abuse and Neglect: a Cross-Country Analysis of Population-Based Surveys and Country-Level Statistics. Journal of Family Violence, 1–8. [DOI] [PMC free article] [PubMed]
- Lipsky S, Caetano R, Field CA, & Larkin GL (2005). Psychosocial and substance-use risk factors for intimate partner violence. Drug and Alcohol Dependence, 78(1), 39–47. [DOI] [PubMed] [Google Scholar]
- Manchikanti Gómez A (2011). Testing the cycle of violence hypothesis: Child abuse and adolescent dating violence as predictors of intimate partner violence in young adulthood. Youth & society, 43(1), 171–192. [Google Scholar]
- Marphatia AA, Cole TJ, Grijalva-Eternod C, & Wells JC (2016). Associations of gender inequality with child malnutrition and mortality across 96 countries. Global Health, Epidemiology and Genomics, 1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murphy SL, Xu J, & Kochanek KD (2013). National vital statistics reports. National Vital Statistics Reports, 61(4). [PubMed] [Google Scholar]
- National Center for Injury Prevention and Control. (2003). Costs of Intimate Partner Violence Against Women in the United States Atlanta, GA: Centers fof Disease Control and Prevention,. [Google Scholar]
- National Center for Injury Prevention and Control. (2015). The Social-Ecological Model: A Framework for Prevention Retrieved 10/30/2017, 2017, from https://www.cdc.gov/violenceprevention/overview/social-ecologicalmodel.html
- Redding EM, Ruiz-Cantero MT, Fernández-Sáez J, & Guijarro-Garvi M (2017). Gender inequality and violence against women in Spain, 2006–2014: towards a civilized society. Gaceta Sanitaria, 31(2), 82–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Renzetti CM, Edleson JL, & Bergen RK (2011). Companion Reader on Violence Against Women: SAGE. [Google Scholar]
- Smith SG, Basile KC, Gilbert LK, Merrick MT, Patel N, Walling M, & Jain A (2017). National Intimate Partner and Sexual Violence Survey (NISVS): 2010–2012 state report.
- Sullivan TP, Meese KJ, Swan SC, Mazure CM, & Snow DL (2005). Precursors and correlates of women’s violence: Child abuse traumatization, victimization of women, avoidance coping, and psychological symptoms. Psychology of Women Quarterly, 29(3), 290–301. [Google Scholar]
- Sundström A, Paxton P, Wang Y-T, & Lindberg SI (2017). Women’s Political Empowerment: A New Global Index, 1900–2012. World Development, 94, 321–335. [Google Scholar]
- U.S. Census Bureau. (2010). American Community Survey: American Fact-Finder: 2010–2012, 3 Year Estimates Retrieved 9/30/2017, 2017, from https://www.census.gov/programs-surveys/acs/
- United Nations Development Programme. (2013). Humanity divided: Confronting inequality in developing countries: UNDP; New York^ eNY NY. [Google Scholar]
- United Nations Development Programme. (2016). Technical Notes Human Development Report 2016 New York, NY. [Google Scholar]
- Walton-Moss BJ, Manganello J, Frye V, & Campbell JC (2005). Risk factors for intimate partner violence and associated injury among urban women. Journal of Community Health, 30(5), 377–389. [DOI] [PubMed] [Google Scholar]
- Willie TC, Powell A, Lewis J, Callands T, & Kershaw T (2017). Who is at risk for intimate partner violence victimization: using latent class analysis to explore interpersonal polyvictimization and polyperpetration among pregnant young couples. Violence and Victims, 32(3), 545–564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Women’s Legislative Network of NCSL. (2010). Women in State Legislatures: 2010 Legislative Session Retrieved 9/30/2017, 2017, from http://www.ncsl.org/legislators-staff/legislators/womens-legislative-network/women-in-state-legislatures-2010.aspx
- World Health Organization; (2009). Violence prevention: The evidence. Promoting gender equality to prevent violence against women Geneva: WHO; Retrieved on July, 20, 2013. [Google Scholar]
- Yodanis CL (2004). Gender inequality, violence against women, and fear: A cross-national test of the feminist theory of violence against women. Journal of Interpersonal Violence, 19(6), 655–675. [DOI] [PubMed] [Google Scholar]