

Abstract
Background
Metabolic syndrome (MetS) is a cluster of metabolic abnormalities that increases the cardiovascular risk. Regular physical exercise can promote benefits, but the MetS individuals are demotivated to perform it. Thus, new possibilities are important as an alternative intervention. The whole-body vibration can be considered an exercise modality and would be a safe and low-cost strategy to improve functional parameters of individuals in different clinical conditions. The aim of this exploratory study was to assess effects of whole-body vibration on functional parameters of MetS individuals. The hypothesis of this work was that the whole-body vibration could improve the functionality of MetS individuals.
Methods
Twenty-two individuals performed the intervention. The vibration frequency varied from 5 to 14 Hz and the peak-to-peak displacements, from 2.5 to 7.5 mm. Each session consisted of one minute-bout of working time followed by a one minute-bout of passive rest in each peak-to-peak displacement for three-times. The whole-body vibration protocol was applied twice per week for 5 weeks. Data from the trunk flexion, gait speed, sit-to-stand test and handgrip strength were collected. Physiological parameters (blood pressure and heart rate) were also evaluated. The Wilcoxon Rank test and Student t-test were used.
Results
No significant changes (p > 0.05) were observed in physiological parameters (arterial blood pressure and heart rate). Significant improvements were found in trunk flexion (p = 0.01), gait speed (p = 0.02), sit-to-stand test (p = 0.005) and handgrip strength (p = 0.04) after the whole-body vibration.
Conclusions
In conclusion, whole-body vibration may induce biological responses that improve functional parameters in participants with MetS without interfering in physiological parameters, comparing before and after a 5-week whole-body vibration protocol.
Trial registration
Register in the Registro Brasileiro de Ensaios Clínicos (ReBEC) with the number RBR 2bghmh (June 6th, 2016) and UTN: U1111–1181-1177. (virgula).
Keywords: Whole-body vibration, Metabolic syndrome, Functional parameters
Background
According to the International Diabetes Federation (IDF), metabolic syndrome (MetS) is a cluster of metabolic abnormalities that increases the cardiovascular risk. In this context, the insulin resistance and central obesity are considered important factors. Other conditions are relevant in MetS individuals because they can interfere on the management of them, such as i) genetic factors, ii) physical inactivity, iii) aging iv) a proinflammatory state and v) hormonal changes. An increasing risk for type 2 diabetes mellitus (T2DM) and cardiovascular disease is observed in MetS individuals [1–4].
Metabolic impairments caused due to the excessive fat accumulation (central obesity) in obese individuals are associated with increased risk for T2DM, cardiovascular disease, disability and mortality [5, 6]. The central obesity, as observed in MetS participants, negatively affects the function of the insulin receptors within the muscle and is associated with insulin sensitivity through cytokine-mediated pathways [7, 8]. These pathways may help to explain the impairments in the physical function that characterizes the chronic obesity and T2DM and their common complications [9, 10]. This complex process is shown in Fig. 1, where it is verified that poor regular physical activities can lead to MetS. Regular exercise practice, as aerobic exercise, fitness or progressive resistance training exercise, is associated with the improvement of several metabolic parameters, as reduced visceral (abdominal) fat in adults [11] without any change in body mass [12]. It suggests an increase in muscle mass due to exercise training. In a systematic review, Thomas et al., 2006 reported that glycated hemoglobin values decreased after the intervention in physically active groups more than in control groups, in individuals with T2DM [12]. Moreover, Chang et al., 2015 [13] evaluated the body composition, muscular strength, flexibility and cardiorespiratory endurance of community-dwelling elders and it was verified that the presence of MetS was associated with a decrease in flexibility independent on age, gender, and body mass index (BMI).
Fig. 1.

The complex process of the relationship between the poor level daily physical activity and the development of the Metabolic Syndrome
An exercise modality involving mechanical vibration generated in the oscillating/vibratory platform (OVP) is the whole-body vibration (WBV) [14]. Mechanical vibration, defined as an oscillatory motion, can be generated in OVP and transmitted to a subject [15]. The working time, as well as the rest time between bouts, the number of bouts in a session, and the periodicity of the sessions might be also controlled [15, 16]. Other prescriptive factors of WBV include frequency (f), peak-to-peak displacement (D) and the position of the individual [17].
WBV can improve the (i) flexibility in male athletes [18], young men [19], MetS individuals [20, 21], young students [22], divers [23], obese sedentary young people [24]; (ii) muscular strength in trained men [25]; (iii) functionality in individuals with multiple sclerosis [26], in MetS individuals [27] and with severe chronic obstructive pulmonary disease [28]; (iv) quality of life in MetS individuals [29] and children with cerebral palsy [30] and (v) gait speed in children with idiopathic toe walking [31]. Considering the publications in the PubMed database, only a limited number of articles involving studies about the effects of the WBV in MetS individuals is found [20, 21, 27, 29].
Milanese et al., 2018 [32] studied the metabolic effect of WBV (short-term) in physically active young males using indirect calorimetry to access the oxygen consumption and they have shown that WBV increases the metabolic cost of exercise that can be complemented with physical activity programs in several settings. Dutra et al., 2016 [33] concluded that low-intensity vibration improves balance, mobility and muscle strength in the upper and lower limbs in postmenopausal women using a 12-month-WBV protocol. Tseng et al., 2016 [34] reported that WBV training at 20 Hz has significant benefit to the balance and flexibility of elderly who do not engage in habitual exercise. Putting together these considerations and the functional limitations of the MetS individuals to perform physical activities, the relevance of the current study was to assess effects of WBV on functional parameters of these individuals.
Therefore, the aim of this exploratory study was to verify effects of whole-body vibration on functional parameters of MetS individuals. A suitable and feasible WBV protocol was applied twice per week for 5-weeks to evaluate the trunk flexion (TF), gait speed (GS), sit-to-stand test (STS) and handgrip strength (HS). Physiological parameters (systolic-SBP, diastolic blood pressure-DBP and the heart rate-HR) were also determined.
The hypothesis of this study was that the WBV could improve the functionality of MetS individuals.
Methods
Individuals
In this exploratory study, twenty-eight individuals (61.18 ± 8.39 years old) with MetS were selected to evaluate the effect of the WBV in functional parameters. The recruitment of participants was done from April 2014 to January 2016, made through a screening performed by the medical staff of Hospital Universitário Pedro Ernesto (HUPE), Universidade do Estado do Rio de Janeiro (UERJ), Brazil. WBV protocol was performed in the Laboratório de Vibrações Mecânicas e Práticas Integrativas - LAVIMPI, UERJ.
The inclusion criteria were outpatients of both genders, over 40 years old [35] with a previous clinical diagnosis of MetS based on the criteria described by the IDF [1]. The exclusion criteria were individuals with very high blood pressure (≥ 180/110 mmHg) and not controlled, cardiovascular disease (coronary artery disease or stroke), neurological, musculoskeletal or rheumatologic disease does not permit the performance of WBV. Participants who refused to sign the consent form were also excluded.
As the reduction of the flexibility has been also associated with the MetS [13] and could interfere in the functionality of these individuals, this parameter was considered in the determination of the sample size. For a statistical power of 95% and the significance level of 5%, a sample size of 13 participants was calculated to determine a 17% change in flexibility [20, 36]. The Transparent Reporting of Evaluations with Non-randomized Designs (TREND) statements were used to report all the different steps of the interventions utilized in this study [37]. This study was approved by the Research Ethics Committee of the HUPE, UERJ with the number CAAE 54981315.6.0000.5259, the register in the Registro Brasileiro de Ensaios Clínicos (ReBEC) with the number RBR 2bghmh and UTN: U1111–1181-1177. The principles from the Declaration of Helsinki were followed.
The participants were sedentary, and they were instructed to continue their normal daily activities and medications during the investigation. In general, the medications used by the participants were diuretics, beta blockers, calcium channel blockers, angiotensin-converting-enzyme inhibitors and angiotensin receptor antagonists.
Anthropometric characteristics
The height and body mass were measured on a digital balance (MIC 200 PPA, Micheletti, São Paulo, Brazil). Then, the BMI was calculated by dividing the mass (kg) by the stature squared (m2) [38]. The assessment of the waist circumference (WC) was performed with non-stretchable flexible tapes and the measurement was at the midpoint between the last rib and the iliac crest, according to guidelines by the World Health Organization (WHO) [4].
In an interview, each participant was asked about smoking and physical activity habit and it was considered the answer “yes” or “no”. The participants provided information about hypertension and T2DM diagnosis that the physician had defined (according to IDF).
Primary outcomes
In this investigation, the findings related to the evaluated parameters before and after a five-week protocol involving WBV were considered. Before the first session, the outcomes were performed in the sequence, physiological parameters, gait speed, sit to stand the test, HS and flexibility with a rest of 10 min among them. After the last session, the measurements were performed in the same way to reduce the measurement errors.
Determination of physiological parameters
An automated device (OMRON, model HEM-7113, China) was utilized to record the systolic (SBP) and diastolic blood pressure (DBP) (mmHg), and the heart rate (HR) (beats per min – bpm) from the left arm of seated participants after a 10-min rest before each day of WBV [39] and after the WBV session. There was one minute of rest between each measurement. Mean values of three records were used in the analysis.
Determination of the gait speed
In the evaluation of the GS, the individual was asked to walk on a demarcated distance of 3 m on the floor. Two measures of the walked time (chronometer, cronobio SW2018, Brazil) were obtained, and the best time was considered [40]. The gait speed was calculated dividing the distance by the walked time. This test was performed before and after the WBV protocol.
Determination of the sit-to-stand test
Measures of gait speed and the sit-to-stand (STS) test have been considered as an important component of physical capacity which gives insight on frailty in older adults [41, 42]. To evaluate the lower-limb functional strength, the STS was used in this current study. The subject was asked to sit in an armless chair (with its back supported against a wall) with arms crossed over his/her chest and then instructed to stand and sit five times as quickly as possible. The same chair was used for all participants.
Participants performed two timed trials (chronometer, cronobio SW2018, Brazil), and the second one was considered for analysis. The instructor started the test with “Ready, Set, Go”, started a digital stopwatch on “Go,” and counted aloud each of the five completed sit to stand cycles. The stopwatch was stopped when the subject returned to the seated position for the fifth time [43]. This test was performed before and after the WBV protocol.
Determination of the handgrip strength
The muscular strength of the upper limbs (hand) was accessed through the HS, measured quantitatively using a digital hand dynamometer (EMG830RF, EMG System, São José dos Campos, Brazil). This test aims to verify the strength of the upper limbs - the hands specifically. The individuals were positioned sitting down with a straight back and no armrests and with elbow flexion at 90°. They were asked to grip the dynamometer with their dominant hand using maximum strength for 6 s (chronometer, cronobio SW2018, Brazil). The test was performed three times at 1-min intervals, before and after the WBV protocol, and the maximum score, in kgf, was recorded [43]. Handgrip strength has been recommended as an assessment technique for the measurement of muscle strength, and as the simplest method for assessment of muscle function in clinical practice [43]. Authors have reported that HS may be a good predictor of body cell mass depletion and mortality [43, 44].
Determination of the flexibility
According to the American Council on Exercise, flexibility is related to the ability to move joints through their full range of motion and it is highly desired and relevant to a subject to do their daily activities [45]. The measure of flexibility was performed through the anterior trunk flexion (ATF) test [20, 46], also called fingertip-to-floor distance (FFD) test. This test consisted in measuring the distance between the tip of middle finger and the floor after an anterior trunk flexion, with feet together and without bending the knees [20] (Fig. 2). The distance between the third was determined before and after of WBV session and it was expressed in centimeters.
Fig. 2.

Individual performing the Anterior Trunk Flexion test to measure distance of the third finger and the floor
Intervention
Before the first session of the WBV program, the participants were instructed to continue their normal daily activities and medications during the investigation. All the individuals confirmed over the end of the study that the instructions were followed.
The protocol was performed in 5 weeks (10 sessions), with at least 24 h of rest between each WBV session. This protocol has been used in previous studies involving WBV and MetS individuals [20, 21, 27, 29]. Similarly, Milanese et al., 2013 [32] and Sañudo et al., 2013 [47] have used a protocol twice a week.
In the first session, the individuals sat with bare feet positioned on a side-alternating oscillating/vibratory platform (OVP) (Novaplate, Fitness Evolution ®, São Paulo, Brazil) with knees flexed (130°) controlled by a goniometer [48]. The height of the chair was selected depending on the height of the individual to have similar knee flexion. The hands of the subject were positioned on the knees to facilitate the transmission of the mechanical vibration to the whole body (Fig. 3a). Participants performed three WBV sets of one minute at a frequency of 5 Hz and different peak-to-peak displacements (D) for each set. With this WBV machine, the D depends on the participant’s foot position. The position of the feet (PtF) on the basis of the platform determines three different D (PtF 1–3). The D ranged 2.5–7.5 mm and the PtF used were: a) PtF 1–2.5, b) PtF 2–5.0 and c) PtF 3–7.5 mm (Fig. 4). Milanese et al., 2013 [32] used vibration amplitude that ranged 2.0–5.0 mm. Sá-Caputo et al., 2014 [20], Carvalho-Lima et al., 2017 [29], Paineiras-Domingos et al., 2018 [27] and Sá-Caputo et al., 2018 [21] used the same protocol of this current study. For the identification of the different displacements, longitudinal strips of reflective adhesive tape were applied to the OVP. One-minute inter-set time was permitted.
Fig. 3.
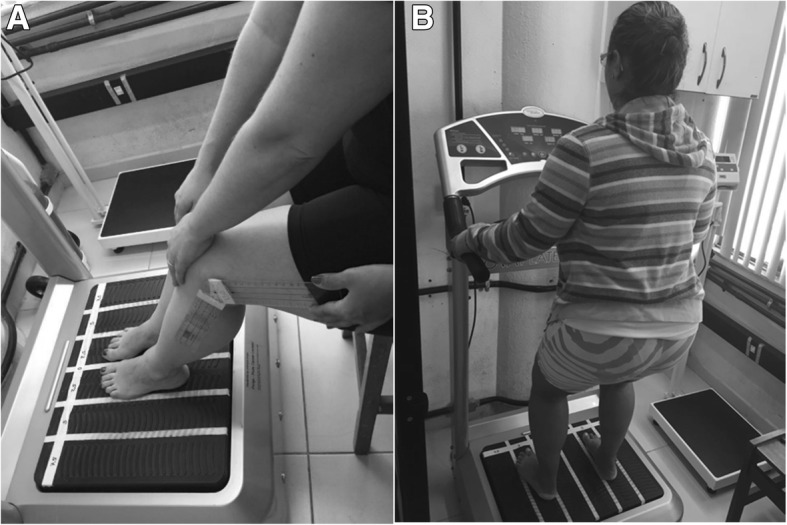
a. Participant seated bare feet on a side-to-side alternating oscillating/vibratory platform with knees flexed. b. Participant with bare feet in the stand position on the side-alternating platform with knees flexed in a stand position
Fig. 4.
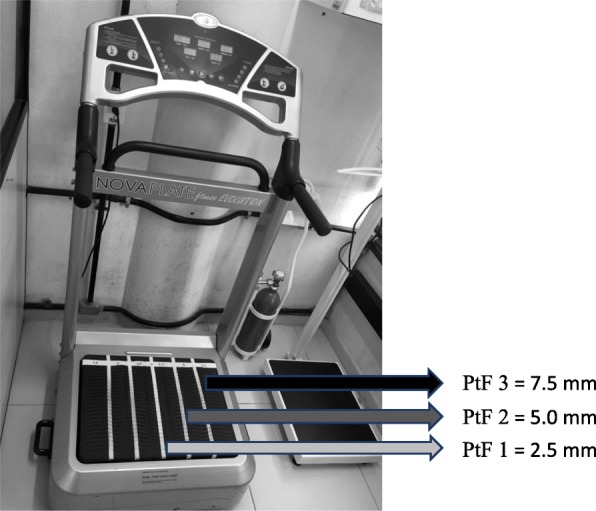
Side-to-side alternating oscillating/vibratory platform used in the study and the positions of the feet (PtF): PtF 1 = 2.5 mm, PtF 2 = 5.0 mm, PtF 3 = 7.5 mm)
From the second up to the tenth session the individuals were barefooted in a standing position on the side-alternating OVP with knees flexed (130°) [48] Fig. 3b. The hands of the subject were positioned on an appropriate place on the platform and all participants positioned the hands in the same place. Participants performed three WBV sets of one minute with the same D described above. One-minute inter-set time was permitted. The total time of the protocol was 17 (9 min of vibration training and 8 min of rest). The frequency in the second session was 6 Hz and 1 Hz was added in the followed sessions until 14 Hz in the tenth session. Similarly, Milanese at al., 2013 [32] have used a protocol with the total time of 19 min (14 min vibration training and 5 min rest) and two vibration amplitude 2.0–5.0 mm. The peak of acceleration was calculated for each set [17].
Statistical analysis
Descriptive statistics included the mean and standard deviation (SD). The Shapiro-Wilk normality test was calculated to determine if the data set can be modeled as a normal distribution. The Wilcoxon rank test and paired t-test were used to compare the change in the different outcome measures from WBV. The level of significance was set at p < 0.05. These analyses were carried out using the Bioestast 5.0 statistic program (Instituto de Desenvolvimento Sustentável Mamirauá, Brazil). Values are expressed as mean and standard derivation (SD) in the text. The reliability of the functional tests was assessed by the coefficient variation and the effect sizes were determined (Cohen’s d). Small effect sizes with d ≤ 0.2, moderate effect sizes are 0.2 < d < 0.8, or large effects sizes are d ≥ 0.8 [49] for parametric data, according the formula, where M = mean and SD = standard derivation. For non-parametric data were calculated correlation coefficients (r) according to the formula r and reported 0.1 as small effect sizes, 0.3 as moderate effect sizes and 0.5 as large effect sizes [50].
Results
The flow diagram with the enrolment of the study is shown in Fig. 5. Twenty-eight individuals were recruited and six were excluded. Consequently, twenty-two participants (20 women and 2 men) participated in this study. They performed the WBV protocol and the results before the first and after the last session are presented.
Fig. 5.
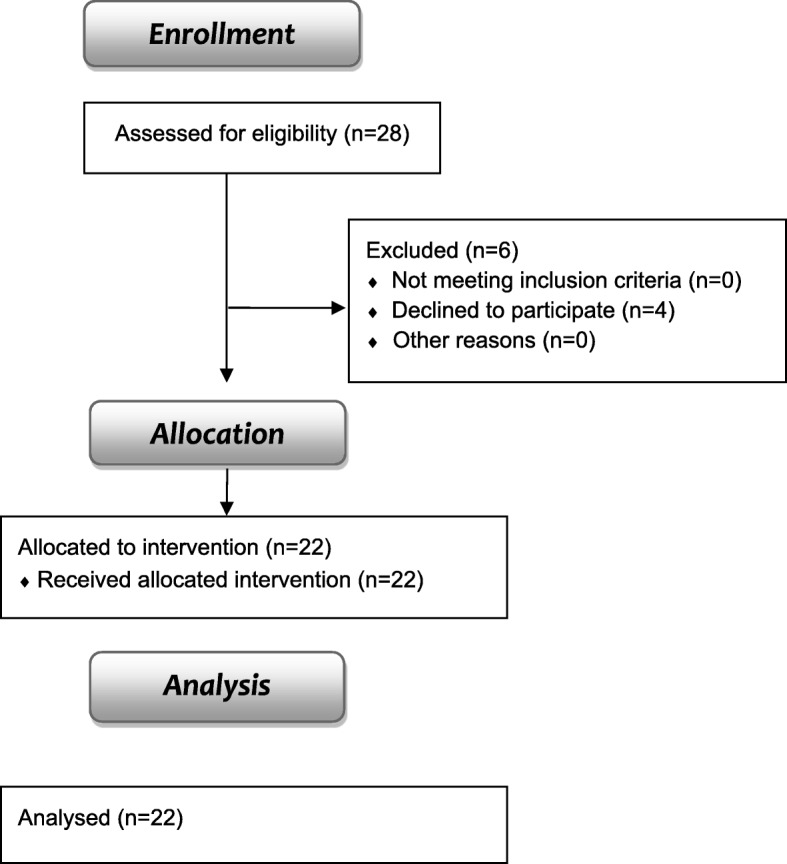
Flow diagram of the clinical intervention
The anthropometric characteristics of the participants are presented in Table 1.
Table 1.
Anthropometric characteristics of the participants
| Variables | Mean ± SD or (percentage) |
|---|---|
| Height (m) | 1.63 ± 0.07 |
| Body mass (kg) | 83.65 ± 16.27 |
| WC (cm) | 103.17 ± 11.09 |
| BMI (kg/m2) | 31.16 ± 5.35 |
| Smoker (%) | 1 (5.26) |
| T2DM (%) | 7 (36.84) |
| Hypertension (%) | 17 (89.47) |
| Physical activity (%) | 4 (21.05) |
WC waist circumference, BMI body mass index, T2DM type 2 diabetes mellitus
The findings of the physiological parameters as SBP, DBP and HR are presented in Table 2. No significant changes were observed after the WBV with a small effect size (d = 0.12), (d = 0.15) and (d = 0.09) respectively.
Table 2.
Values of the physiological parameters before and after the WBV protocol
| Before WBV Mean ± SD |
After WBV Mean ± SD |
p-value | Effect-size | |
|---|---|---|---|---|
| SBP (mmHg) | 128.93 ± 15.72 | 126.02 ± 15.10 | 0.59 | d = 0.12 |
| DBP (mmHg) | 68.08 ± 9.40 | 66.77 ± 7.93 | 0.66 | d = 0.15 |
| HR (bpm) | 67.17 ± 13.28 | 68.37 ± 12.59 | 0.50 | d = 0.09 |
SBP systolic blood pressure, DBP diastolic blood pressure, HR heart rate, p- significance at p ≤ 0.05, d- Cohen’s d
Concerning the findings of functional parameters (HS, ATF, GS and STS test) before and after the intervention with the WBV protocol, the data are presented in Table 3. It was verified an improvement on the functionality of the individuals with MetS, as it presented.
Table 3.
Values of functional parameters before and after the WBV protocol
| Before WBV Mean ± SD |
After WBV Mean ± SD |
p-value | Effect-size | |
|---|---|---|---|---|
| HS (kgf) | 20.02 ± 7.72 | 22.41 ± 6.53 | 0.04 | d = 0.33 |
| ATF (cm) | 16.31 ± 10.31 | 13.34 ± 11.02 | 0.01 | r = 0.60 |
| GS (m/s) | 0.73 ± 0.20 | 0.83 ± 0.27 | 0.02 | d = 0.42 |
| STS (s) | 20.25 ± 7.74 | 16.24 ± 3.99 | 0.005 | r = 0.65 |
HS handgrip strength, ATF anterior trunk flexion – anterior trunk flexion test, GS gait speed, STS sit-to-stand test; p- significance at p ≤ 0.05, d- Cohen’s d, r- correlation coefficients
A significant difference (p = 0.005) in the STS test, with a decrease in the time to perform the test, was found, with a large effect size (r = 0.65).
Considering the ATF, a significant decrease in this distance (p = 0.01), was found with a large effect size (r = 0.60). The data about ATF are presented in centimeters.
About the GS, significant (p = 0.02) changes, with an increase, were observed after the WBV protocol, with a moderate effect size (d = 0.42).
A significant difference (p = 0.04), with an increase in the HS, was found after the WBV protocol, with moderate effect size (d = 0.33).
Discussion
There is a limited number of publications about the effects of WBV in individuals with MetS [20, 21, 27, 29] involving flexibility, muscular strength, functionality, quality of life and gait speed. The current study demonstrates the possible benefits of WBV to increase the functionality of individuals with MetS. A 5-week (10 sessions) protocol involving WBV improved the functional parameters compared to baseline values. Moreover, physiological parameters were not altered. In addition, the improvement involving the use of WBV might be explained due to WBV can promote coordinated muscle actions [51]. The appropriate muscle responses can occur with correct working of spinal reflex, brain stem balance and cognitive programming [52]. Thus, the muscle stimulus can improve the functionality [53] and adjustment afferent and efferent signals which, in turn, will lead to “training” effects for the sensorimotor system [54]. Studies have described that WBV could reduce the stiffness and hysteresis of the tendon, alter properties of the intramuscular connective tissue and possibly modify those of other passive skeletal structures related to the range of motion for a determined joint [15, 55].
The protocol used in the current study did not alter the physiological parameters (SBP, DBP and HR) of the individuals. These data are important and demonstrate the safety of this protocol with WBV to MetS individuals. Yule et al., 2016 [56] reported that a short-term WBV training with side-alternating OVP did not affect physiological parameters of the patients with chronic stroke. This agrees with the findings reported by Robbins et al., 2014 [57] in which WBV with 40 Hz in a synchronous platform in healthy participants.
Physical limitations, complications and the decrease of the muscle strength of the individuals with MetS can be explained through the relationship between the composition of skeletal muscle tissue and all the affected metabolic pathways [9, 10] (Fig. 1).
Handgrip strength testing is increasingly being used in clinical settings, for example in the assessment of sarcopenia, frailty and undernutrition in hospitalized older people [43]. Sarcopenia, frailty and muscle weakness have been described in individuals with obesity and metabolic disturbs [58] and WBV can be positive effects in these clinical conditions.
WHO reports that physical inactivity favors the reduction of the flexibility [59]. Furthermore, Chang et al., 2015 [13] suggest that exercise interventions to increase flexibility should be implemented to test its possible therapeutic effect on MetS individuals and that the flexibility should be included in the complete evaluation for MetS. As the WBV involves mechanical stretching, this fact could justify the increase of the flexibility by this modality of exercise generated by vibration produced in OVP and the improvements observed in participants exposed to WBV. Sá-Caputo et al., 2014 [20] and 2018 [21]; Gomes and Guimarães, 2004 [60] have reported improvement of the flexibility of participants that have performed WBV. Dallas et al., 2015 [23] examined acute effects of different vibration loads of WBV on flexibility and explosive strength of lower limbs in springboard divers. They reported that WBV is also recommended to increase flexibility and vertical jump height in sports.
In the current study, the mean baseline of the STS test was 20.25 s (Table 3), indicating a somewhat reduced lower-limb muscle strength. Studies have reported an improvement of the lower-limb muscle strength due to WBV in untrained [24] and trained adults [25]. Delecluse et al., 2003 [61] have described that squatting posture during WBV stimulation strengthens the quadriceps muscles, which are knee extensors. The improvement in the STS test time (from 20.25 to 16.24 s), observed in the current investigation may also be related to this WBV stimulation. Williams et al., 2016 [31] described that WBV increases the gait velocity in children with idiopathic toe walking. It could be potentially due to a rapid increase in ankle range of motion or a neuromodulation response.
WBV with the present protocol may improve significantly the functional parameters analyzed, HS, ATF, GS and STS test after the 5-week intervention. The mechanism that explains the effect of WBV on physical function may be a chain of rapid muscle contractions that occur during the exercise. It might directly activate the neuromuscular system in the lower extremities.
Due to the WBV, acute changes occur in endurance-associated parameters such as energy metabolism and turnover [22, 24, 62] and in the neuromuscular activation in the lower extremities [23, 24]. A significant increase in popliteal blood flow (100%) and in the local muscle perfusion in the gastrocnemius and vastus lateralis muscles were found during and after the WBV [19]. Furthermore, Rittweger, 2000 [15] observed an increase in VO2, dependent on frequency and amplitude and an augmented energy turnover during WBV. Thus, the metabolic and energetic changes occur due to the response to an enhancement in activation intensity in the muscles of the lower extremities during the stimulus promoted by WBV. It could be speculated that the more exposed the muscles are to WBV, the greater the neuromuscular and metabolic demand. Therefore, these findings could aid to understand the improvement of the functional parameters.
The long exposure to WBV and high-frequency vibration seem to have dangerous side effects on the human body [63]. To prevent these potentially dangerous side-effects, it is important to consider safe exercise protocols with a controlled exposure of mechanical vibrations, as the protocol of this investigation. Moreover, side-effects related to WBV were not found in the current study. This could be associated with the controlled parameters used in this protocol with WBV.
A rationale to justify the use of the WBV instead of other activities such as a gym session is due to the simple, feasible, inexpensive, controlled, safe and suitable procedure when performed with the supervision of a qualified professional. Besides various benefits in individuals of different populations, the improvement of the quality of life has been also reported in MetS individuals [29].
There are some limitations in the current study. Firstly, the results (daily activity, daily working, smoking, physical activity and daily energy intake) were not controlled for. Secondly, no long-term follow-up data were available after the intervention, so the long-lasting effects were not investigated. Thirdly, this investigation is an exploratory study and it did not have a control group. Finally, the external validity of this intervention considering its generalizability to other settings (like the everyday-living condition) was not explored. In consequence, further investigations are required.
Conclusion
In conclusion, WBV may promote an additional effect on local stochastic muscle endurance. It could be speculated that the improvements in local muscle endurance may be caused by adaptations in energy metabolism and turnover, which is associated with vibration-induced changes in neuromuscular activation, that could aid to explain our findings. Moreover, the biological responses to the 5-week WBV protocol would be related to the improvement of the functional parameters on the MetS individuals (HS, ATF test, GS and STS test) without interfering in physiological parameters (SBP, DBP and HR). Further studies are warranted to gain new knowledge about the effects of WBV on MetS individuals.
Acknowledgments
The authors are thankful to UERJ and Dr. Mario Pereira for all the support in this study.
Funding
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior – Brazil (CAPES) - Finance Code 001. The Brazilian Agencies (CNPq, UERJ and FAPERJ) also offered a financial support.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- ATF
Anterior trunk flexion test
- BMI
Body mass index
- d
Cohen’s d
- D
Peak-to-peak displacement
- DBP
Diastolic blood pressure
- f
Frequency
- FFD
Fingertip-to-floor distance
- GS
Gait speed
- HR
Heart rate
- HS
Handgrip strength
- HUPE
Hospital Universitário Pedro Ernesto
- IDF
International Diabetes Federation
- MetS
Metabolic syndrome
- OVP
Oscillating/vibratory platform
- Paccel
Peak acceleration
- PtF
Position of the feet
- r
correlation coefficients
- ReBEC
Registro Brasileiro de Ensaios Clínicos
- SBP
Systolic blood pressure
- SD
Standard deviation
- SE
Standard error
- STS
Sit-to-stand test
- T2DM
Type 2 diabetes mellitus
- TREND
Transparent Reporting of Evaluations with Non-randomized Designs statements
- UERJ
Universidade do Estado do Rio de Janeiro
- WBV
Whole-body vibration
- WC
Waist circumference
- WHO
World Health Organization
Authors’ contributions
DDCDS-C, LLP-D, AF-S, EMDA and ASR participated in the elaboration and execution of the study. DDCDS-C and LLP-D did the statistical analysis. MB-F, RT and AS coordinated the study and helped on the draft of manuscript. MFTN, WO, RO, AB, CBM and XC reviewed. DDCDS-C, LLP-D and MB-F approved the final version of this investigation. LLP-D submitted the manuscript. All authors read and approved the final manuscript.
Ethics approval and consent to participate
The authors declare that they have no competing interest. This study was approved by the Research Ethics Committee of the HUPE, UERJ with the number CAAE 54981315.6.0000.5259 and the register in the Registro Brasileiro de Ensaios Clínicos (ReBEC) with the number RBR 2bghmh.
All the participants of this study signed sign the consent form.
Consent for publication
All individuals in Figs. 2 and 3 gave written informed consent for their images to be used in this publication.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Danúbia Sá-Caputo, Email: dradanubia@gmail.com.
Laisa Liane Paineiras-Domingos, Email: laisanit@gmail.com.
Arlete Francisca-Santos, Email: fisioarlete@hotmail.com.
Elzi Martins dos Anjos, Email: elzimartins45@gmail.com.
Aline Silva Reis, Email: fisio.alinereis@hotmail.com.
Mario Fritsch Toros Neves, Email: mariofneves@gmail.com.
Wille Oigman, Email: oigmanrlk@terra.com.br.
Ricardo Oliveira, Email: rico_de_oliveira@yahoo.com.br.
Andrea Brandão, Email: andreaabrandao@terra.com.br.
Christiano Bittencourt Machado, Email: cbmfisio@gmail.com.
Xavier Chiementin, Email: xavier.chiementin@univ-reims.fr.
Redha Taiar, Email: redha.taiar@univ-reims.fr.
Alessandro Sartório, Email: sartorio@auxologico.it.
Mario Bernardo-Filho, Email: bernardofilhom@gmail.com.
References
- 1.Sossa C, Delisle H, Agueh V, Sodjinou R, Ntandou G, Makoutodé M. Lifestyle and dietary factors associated with the evolution of cardiometabolic risk over four years in west-African adults: the Benin study. J Obes. 2013;2013:298024. doi: 10.1155/2013/298024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Alberti KG, Zimmet P, Shaw J. Metabolic syndrome-a new worldwide definition. A consensus statement from the international diabetes federation. Diabet Med. 2006;23:469–480. doi: 10.1111/j.1464-5491.2006.01858.x. [DOI] [PubMed] [Google Scholar]
- 3.Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, Fruchart JC, James WP, Loria CM, Smith SC, Jr, International Diabetes Federation Task Force on Epidemiology and Prevention, National Heart, Lung, and Blood Institute, American Heart Association, World Heart Federation, International Atherosclerosis Society, International Association for the Study of Obesity Harmonizing the metabolic syndrome: A joint interim statement of the international diabetes federation task force on epidemiology and prevention; national heart, lung, and blood institute; American Heart Association; world heart federation; international atherosclerosis society; and international association for the study of obesity. Circulation. 2009;120:1640–1645. doi: 10.1161/CIRCULATIONAHA.109.192644. [DOI] [PubMed] [Google Scholar]
- 4.Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, Gordon DJ, Krauss RM, Savage PJ, Smith SC, Jr, Spertus JA, Costa F. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, lung, and blood institute scientific statement. Circulation. 2005;112:2735–2752. doi: 10.1161/CIRCULATIONAHA.105.169404. [DOI] [PubMed] [Google Scholar]
- 5.Cade WT. Diabetes-related microvascular and macrovascular diseases in the physical therapy setting. Phys Ther. 2008;88:1322–1335. doi: 10.2522/ptj.20080008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Alley DE, Chang VW. The changing relationship of obesity and disability. 1988–2004. JAMA. 2007;298:2020–2027. doi: 10.1001/jama.298.17.2020. [DOI] [PubMed] [Google Scholar]
- 7.Stehno-Bittel L. Intricacies of fat. Phys Ther. 2008;88:1265–1278. doi: 10.2522/ptj.20080034. [DOI] [PubMed] [Google Scholar]
- 8.Wei Y, Chen K, Whaley-Connell AT, Stump CS, Ibdah JA, Sowers JR. Skeletal muscle insulin resistance: the role of inflammatory cytokines and reactive oxygen species. Am J Physiol Regul Integr Comp Physiol. 2008;294:673–680. doi: 10.1152/ajpregu.00561.2007. [DOI] [PubMed] [Google Scholar]
- 9.Park SW, Goodpaster BH, Strotmeyer ES, de Rekeneire N, Harris TB, Schwartz AV, Tylavsky FA, Newman AB. Decreased muscle strength and quality in older adults with type 2 diabetes: the health, aging, and body composition study. Diabetes. 2006;55:1813–1818. doi: 10.2337/db05-1183. [DOI] [PubMed] [Google Scholar]
- 10.Park SW, Goodpaster BH, Strotmeyer ES, Kuller LH, Broudeau R, Kammerer C, de Rekeneire N, Harris TB, Schwartz AV, Tylavsky FA, Cho YW, Newman AB. Health, aging, and body composition study. Accelerated loss of skeletal muscle strength in older adults with type 2 diabetes: the health, aging, and body composition study. Diabetes Care. 2007;30:1507–1512. doi: 10.2337/dc06-2537. [DOI] [PubMed] [Google Scholar]
- 11.Ohkawara K, Tanaka S, Miyachi M, Ishikawa-Takata K, Tabata I. A dose-response relation between aerobic exercise and visceral fat reduction: systematic review of clinical trials. Int J Obes. 2007;31:1786–1797. doi: 10.1038/sj.ijo.0803683. [DOI] [PubMed] [Google Scholar]
- 12.Thomas DE, Elliott EJ, Naughton GA. Exercise for type 2 diabetes mellitus. Cochrane Database Syst Rev. 2006;3:CD002968. doi: 10.1002/14651858.CD002968.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chang KV, Hung CY, Li CM, Lin YH, Wang TG, Tsai KS, Han DS. Reduced flexibility associated with metabolic syndrome in community-dwelling elders. PLoS One. 2015;10:0117167. doi: 10.1371/journal.pone.0117167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Olivares PR, Gusi N, Parraca JA, Adsuar JC, Del Pozo-Cruz B. Tilting whole body vibration improves quality of life in women with fibromyalgia: a randomized controlled trial. J Altern Complement Med. 2011;17:723–728. doi: 10.1089/acm.2010.0296. [DOI] [PubMed] [Google Scholar]
- 15.Rittweger J, Beller G, Felsenberg D. Acute physiological effects of exhaustive whole-body vibration exercise in man. Clin Physiol. 2000;20:134–142. doi: 10.1046/j.1365-2281.2000.00238.x. [DOI] [PubMed] [Google Scholar]
- 16.Sá-Caputo DC, Costa-Cavalcanti R, Carvalho-Lima RP, Arnóbio A, Bernardo RM, Ronikeile-Costa P, Kutter C, Giehl PM, Asad NR, Paiva DN, Pereira HV, Unger M, Marin PJ, Bernardo-Filho M. Systematic review of whole body vibration exercises in the treatment of cerebral palsy: brief report. Dev Neurorehabil. 2015;24:1–7. doi: 10.3109/17518423.2014.994713. [DOI] [PubMed] [Google Scholar]
- 17.Rauch F, Sievanen H, Boonen S, Cardinale M, Degens H, Felsenberg D, Roth J, Schoenau E, Verschueren S, Rittweger J. International Society of Musculoskeletal and Neuronal Interactions. Reporting whole-body vibration intervention studies: recommendations of the International Society of Musculoskeletal and Neuronal Interactions. J Musculoskelet Neuronal Interact. 2010;10:193–198. [PubMed] [Google Scholar]
- 18.Issurin VB, Liebermann DG, Tenenbaum G. Effect of vibratory stimulation training on maximal force and flexibility. J Sports Sci. 1994;12:561–566. doi: 10.1080/02640419408732206. [DOI] [PubMed] [Google Scholar]
- 19.Di Giminiani R, Manno R, Scrimaglio R, Sementilli G, Tihanyi J. Effects of individualized whole-body vibration on muscle flexibility and mechanical power. J Sports Med Phys Fitness. 2010;50:139–151. [PubMed] [Google Scholar]
- 20.Sá-Caputo Dda C, Ronikeili-Costa P, Carvalho-Lima RP, Bernardo LC, Bravo-Monteiro MO, Costa R, de Moraes-Silva J, Paiva DN, Machado CB, Mantilla-Giehl P, Arnobio A, Marin PJ, Bernardo-Filho M. Whole body vibration exercises and the improvement of the flexibility in patient with metabolic syndrome. Rehabil Res Pract. 2014;2014:628518. doi: 10.1155/2014/628518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sá-Caputo DC, Paineiras-Domingos LL, Oliveira R, et al. Acute effects of whole-body vibration on the pain level, flexibility, and cardiovascular responses in individuals with metabolic syndrome. Dose-Response. 2018;16(4):1559325818802139. doi: 10.1177/1559325818802139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Di Giminiani R, Fabiani L, Baldini G, Cardelli G, Giovannelli A, Tihanyi J. Hormonal and neuromuscular responses to mechanical vibration applied to upper extremity muscles. PLoS One. 2014;9:e111521. doi: 10.1371/journal.pone.0111521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Dallas G, Paradisis G, Kirialanis P, Mellos V, Argitaki P, Smirniotou A. The acute effects of different training loads of whole body vibration on flexibility and explosive strength of lower limbs in divers. Biol Sport. 2015;32:235–241. doi: 10.5604/20831862.1163373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Katzmarzyk PT, Janssen I, Ardern CI. Physical inactivity, excess adiposity and premature mortality. Obes Rev. 2003;4:257–290. doi: 10.1046/j.1467-789X.2003.00120.x. [DOI] [PubMed] [Google Scholar]
- 25.Stewart JA, Cochrane DJ, Morton RH. Differential effects of whole body vibration durations on knee extensor strength. J Sci Med Sport. 2009;12:50–53. doi: 10.1016/j.jsams.2007.09.005. [DOI] [PubMed] [Google Scholar]
- 26.Ebrahimi A, Eftekhari E, Etemadifar M. Effects of whole body vibration on hormonal & functional indices in patients with multiple sclerosis. Indian J Med Res. 2015;142:450–458. doi: 10.4103/0971-5916.169210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Paineiras-Domingos LL, da Cunha S-CD, Reis AS, et al. Assessment through the short physical performance battery of the functionality in individuals with metabolic syndrome exposed to whole-body vibration exercises. Dose-Response. 2018;16(3):1559325818794530. doi: 10.1177/1559325818794530. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Braz Júnior DS, Dornelas de Andrade A, Teixeira AS, Cavalcanti CA, Morais AB, Marinho PE. Whole-body vibration improves functional capacity and quality of life in patients with severe chronic obstructive pulmonary disease (COPD): a pilot study. Int J Chron Obstruct Pulmon Dis. 2015;10:125–132. doi: 10.2147/COPD.S73751. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Carvalho-Lima RP, Sá-Caputo DC, Moreira-Marconi E, Dionello C, Paineiras-Domingos LL, Sousa-Gonçalves CR, Morel DS, Frederico EH, Neves MF, Oliveira R, Oigman W, Marin PJ, Paiva DN, Bernardo-Filho M. Quality of life of patients with metabolic syndrome is improved after whole body vibration exercises. Afr J Tradit Complement Altern Med. 2017;14:59–65. doi: 10.21010/ajtcam.v14i4S.8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Moreau NG, Bodkin AW, Bjornson K, Hobbs A, Soileau M, Lahasky K. Effectiveness of rehabilitation interventions to improve gait speed in children with cerebral palsy: systematic review and meta-analysis. Phys Ther. 2016; PubMed PMID: 27313240. [DOI] [PMC free article] [PubMed]
- 31.Williams CM, Michalitsis J, Murphy AT, Rawicki B, Haines TP. Whole-Body Vibration Results in Short-Term Improvement in the Gait of Children with Idiopathic Toe Walking. J Child Neurol. 2016; PubMed. PMID: 27071469. [DOI] [PubMed]
- 32.Milanese C, Piscitelli F, Zenti MG, Moghetti P, Sandri M, Zancanaro C. Ten-week whole-body vibration training improves body composition and muscle strength in obese women. Int J Med Sci. 2013;10:307–311. doi: 10.7150/ijms.5161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Dutra MC, de Oliveira ML, Marin RV, Kleine HC, Silva OL, Lazaretti-Castro M. Whole-body vibration improves neuromuscular parameters and functional capacity in osteopenic postmenopausal women. Menopause. 2016; PubMed PMID: 27326815. [DOI] [PubMed]
- 34.Tseng SY, Hsu PS, Lai CL, Liao WC, Lee MC, Wang CH. Effect of two frequencies of whole-body vibration training on balance and flexibility of the elderly: a randomized controlled trial. Am J Phys Med Rehabil. 2016; PubMed PMID: 27088462. [DOI] [PubMed]
- 35.Salaroli LB, Saliba RA, Zandonade E, Molina Mdel C, Bissoli NS. Prevalence of metabolic syndrome and related factors in bank employees according to different defining criteria. Brazil Clinics. 2013;68:69–74. doi: 10.6061/clinics/2013(01)OA11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.LEE. http://www.lee.dante.br/pesquisa/amostragem/calculo_amostra.html. Accessed 29 Mar 2016.
- 37.Des Jarlais DC, Lyles C, Crepaz N. TREND Group Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: the TREND statement. Am J Public Health. 2004;94:361–366. doi: 10.2105/AJPH.94.3.361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Sañudo B, Alfonso-Rosa R, Del Pozo-Cruz B, Del Pozo-Cruz J, Galiano D, Figueroa A. Whole body vibration training improves leg blood flow and adiposity in patients with type 2 diabetes mellitus. Eur J Appl Physiol. 2013;113:2245–2252. doi: 10.1007/s00421-013-2654-3. [DOI] [PubMed] [Google Scholar]
- 39.Brazilian Society of Cardiology. III Brazilian guidelines on dyslipidemias and guidelines on the prevention of atherosclerosis of the Department of Atherosclerosis of the Brazilian Society of Cardiology. Arq Bras Cardiol. 2001;77:1–48.
- 40.States RA, Salem Y, Pappas E. Overground gait training for individuals with chronic stroke: a Cochrane systematic review. J Neurol Phys Ther. 2009;33:179–186. doi: 10.1097/NPT.0b013e3181c29a8c. [DOI] [PubMed] [Google Scholar]
- 41.Roberts HC, Denison HJ, Martin HJ, Patel HP, Syddall H, Cooper C, Sayer AA. A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardized approach. Age Ageing. 2011;40:423–429. doi: 10.1093/ageing/afr051. [DOI] [PubMed] [Google Scholar]
- 42.Bohannon RW. Sit-to-stand test for measuring the performance of lower extremity muscles. Percept Motor Skills. 1995;80:163–174. doi: 10.2466/pms.1995.80.1.163. [DOI] [PubMed] [Google Scholar]
- 43.Lord SR, Murray SM, Chapman K, Munro B, Tiedemann A. Sit-to-stand performance depends on sensation, speed, balance, and psychological status in addition to strength in older people. J Gerontol A Biol Sci Med Sci. 2002;57:M539–M543. doi: 10.1093/gerona/57.8.M539. [DOI] [PubMed] [Google Scholar]
- 44.Alkurdi ZD, Dweiri YM. A biomechanical assessment of isometric handgrip force and fatigue at different anatomical positions. J Appl Biomech. 2010;26:123–133. doi: 10.1123/jab.26.2.123. [DOI] [PubMed] [Google Scholar]
- 45.The Impact of Flexibility Training on Performance. https://www.acefitness.org/education-and-resources/professional/expert-articles/5598/the-impact-of-flexibility-training-on-performance. Accessed 20 July 2018.
- 46.Lamari N, Marino LC, Cordeiro JA, Pellegrini AM. Trunk anterior flexibility in adolescents after height growth speed peak. Acta Ortop Bras. 2007;15:25–29. doi: 10.1590/S1413-78522007000100005. [DOI] [Google Scholar]
- 47.Sañudo B, Carrasco L, de Hoyo M, Oliva-Pascual-Vaca Á, Rodríguez-Blanco C. Changes in body balance and functional performance following whole-body vibration training in patients with fibromyalgia syndrome: a randomized controlled trial. J Rehabil Med. 2013;45:678–684. doi: 10.2340/16501977-1174. [DOI] [PubMed] [Google Scholar]
- 48.Tankisheva E, Bogaerts A, Boonen S, Feys H, Verschueren S. Effects of intensive whole-body vibration training on muscle strength and balance in adults with chronic stroke: a randomized controlled pilot study. Arch Phys Med Rehabil. 2014;95:439–446. doi: 10.1016/j.apmr.2013.09.009. [DOI] [PubMed] [Google Scholar]
- 49.Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:146–156. doi: 10.1093/gerona/56.3.M146. [DOI] [PubMed] [Google Scholar]
- 50.Maciej T, Ewa T. The need to report effect size estimates revisited. An overview of some recommended measures of effect size. Trends Sports Sci. 2014;1:19–25. [Google Scholar]
- 51.Weber-Rajek M, Mieszkowski J, Niespodziński B, Ciechanowska K. Whole-body vibration exercise in postmenopausal osteoporosis. Prz Menopauzalny. 2015;14:41–47. doi: 10.5114/pm.2015.48679. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Radebold A, Cholewicki J, Polzhofer GK, Greene HS. Impaired postural control of the lumbar spine is associated with delayed muscle response times in patients with chronic idiopathic low back pain. Spine. 2001;26:724–730. doi: 10.1097/00007632-200104010-00004. [DOI] [PubMed] [Google Scholar]
- 53.Rogan S, Hilfiker R, Schmid S, Radlinger L. Stochastic resonance whole-body vibration training for chair rising performance on untrained elderly: a pilot study. Arch Gerontol Geriatr. 2012;55:468–473. doi: 10.1016/j.archger.2012.02.011. [DOI] [PubMed] [Google Scholar]
- 54.Haas CT, Turbanski S, Kessler K, Schmidtbleicher D. The effects of random whole-body vibration on motor symptoms in Parkinson’s disease. NeuroRehabilitation. 2006;21:29–36. [PubMed] [Google Scholar]
- 55.Hazell TJ, Thomas GW, Deguire JR, Lemon PW. Vertical whole-body vibration does not increase cardiovascular stress to static semi-squat exercise. Eur J Appl Physiol. 2008;104:903–908. doi: 10.1007/s00421-008-0847-y. [DOI] [PubMed] [Google Scholar]
- 56.Yule CE, Stoner L, Hodges LD, Cochrane DJ. Does short-term whole-body vibration training affect arterial stiffness in chronic stroke? A preliminary study. J Phys Ther Sci. 2016;28:996–1002. doi: 10.1589/jpts.28.996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Robbins D, Yoganathan P, Goss-Sampson M. The influence of whole body vibration on the central and peripheral cardiovascular system. Clin Physiol Funct Imaging. 2014;34:364–369. doi: 10.1111/cpf.12103. [DOI] [PubMed] [Google Scholar]
- 58.Choi KM. Sarcopenia and sarcopenic obesity. Korean J Intern Med. 2016;31:1054–1060. doi: 10.3904/kjim.2016.193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.WHO (World Health Organization), 2005. Preventing Chronic Diseases: a vital investment: WHO Global report. Accessed 29 March 2016.
- 60.Gomes EC, Guimarães GV. Physical exercise and metabolic syndrome. Rev Bras Med Esporte. 2004;10 ISSN 1806-9940.
- 61.Delecluse C, Roelants M, Verschueren S. Strength increase after whole body vibration compared with resistance training. Med Sci Sports Exerc. 2003;35:1033–1041. doi: 10.1249/01.MSS.0000069752.96438.B0. [DOI] [PubMed] [Google Scholar]
- 62.Beavers KM, Hsu FC, Houston DK, Beavers DP, Harris TB, Hue TF, Kim LJ, Koster A, Penninx BW, Simonsick EM, Strotmeyer ES, Kritchevsky SB, Nicklas BJ. Health ABC study. The role of metabolic syndrome, adiposity, and inflammation in physical performance in the health ABC study. J Gerontol A Biol Sci Med Sci. 2013;68:617–623. doi: 10.1093/gerona/gls213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Abercromby AF, Amonette WE, Layne CS, McFarlin BK, Hinman MR, Paloski WH. Vibration exposure and biodynamic responses during whole-body vibration training. Med Sci Sports Exerc. 2007;39:1794–1800. doi: 10.1249/mss.0b013e3181238a0f. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.