

Abstract
Objectives:
To assess the influence of brightness and contrast adjustments of digital radiographs on the diagnosis of proximal caries lesions, and to compare with observers' preferences for subjective image quality.
Methods:
80 proximal surfaces of posterior teeth were radiographed using an intraoral digital system (Digora Toto, Soredex, Finland). Initial images and four different combinations of brightness and contrast for each radiography were analysed. Five observers scored the images for the presence and extension of caries lesions. Micro–CT images were used as gold standard. In a second stage, the observers were asked which of the radiographs they preferred for the assessment of caries lesions.
Results:
No differences were found between the original and adjusted radiographic images regarding the area under the receiver operating characteristic curve, sensitivity, and specificity (p > 0.05). There was a significant difference between the micro-CT and the intraoral radiographs (p < 0.0001). Images with high brightness and low contrast presented higher number of true negative cases, but also a decrease in caries detection. On the other hand, there were more cases of overestimation of the presence and extension of caries lesions in images with low brightness and high contrast. The subjective evaluation of image quality showed that radiographs with lower brightness and higher contrast tended to be preferred by observers.
Conclusions:
Brightness and contrast adjustments in digital intraoral radiographs within the range tested in this study do not significantly influence the diagnosis of proximal caries lesions, although observers tend to prefer lower brightness and higher contrast images.
Introduction
Dental caries is a highly prevalent disease in the world population and its correct and early diagnosis is essential to paralyze its progression, with consequent preservation of the dental tissues and maintenance of its vitality.1 Because it is a condition that results in dental demineralization, the imaging examinations are great allies in the diagnosis of caries lesions, especially those located in clinically inaccessible proximal surfaces.2
Even with increased use of advanced imaging modalities, such as CBCT, intraoral radiography is still considered the first-choice examination for the evaluation of proximal caries.2, 3 Intraoral radiographic techniques are efficient, low dose, and cost-effective, and therefore valuable for routine assessment of caries. Furthermore, the improvement of the technology in digital image receivers and softwares has increased the possibility of image enhancements and diagnostic task-specific post-processing adjustments to improve radiographic accuracy.3–8
Brightness and contrast adjustment tools are among the most used image enhancement features during radiographic evaluations performed in scientific research and clinical practice.9, 10 While several studies have allowed the observers to use the brightness and contrast tools freely during the evaluation of digital radiographic images,4,11–14 only one previous study evaluated the interference of these tools in the diagnosis of caries lesions.15 However, in that study published in 1998, the levels of brightness and contrast were not limited nor controlled, and the radiographic system used is currently outdated.15 Therefore, it is not possible to determine at this time if and what level of brightness and contrast adjustments has a negative or positive influence on the detection of caries lesions.
The purpose of this study was to evaluate the influence of brightness and contrast adjustments of digital intraoral radiographs on the diagnosis of proximal caries lesions, as well as to compare these results with observers' preferences for subjective image quality in this diagnostic task.
Methods and materials
Sample selection
The study design was reviewed by the local Institutional Ethics Committee (protocol #2.057.024). The sample was composed of 40 posterior teeth (20 premolars and 20 molars). Teeth with suggestive characteristics of carious lesion (e.g. white spots or dentin colour alteration seen through the enamel) were included and teeth with cavitation reaching dentin, restorations or dental anomalies were excluded.
Teeth were arranged side-by-side in silicone phantoms in groups of five: two molars, two premolars and a non-test canine. The latter was used for all phantoms, in order to simulate clinical scenarios with proximity or contact with the mesial surface of the first premolar.12, 16 A total of 10 phantoms were prepared.
Image acquisition
All images were acquired with a direct digital radiographic system Digora Toto (Soredex, Tuusula, Finland), a size 2 CMOS sensor, with a theoretical spatial resolution of 26.3 lp mm−1. The X-ray generator was Focus (Instrumentarium, Tuusula, Finland), operated at 70kVp, 7mA and exposure time of 0.063 s. This exposure time was chosen based on a pilot study, in which the digital receptor was exposed to a range of exposure times (from 0.02 to 0.50 s) and three Oral and Maxillofacial radiologists, working in consensus and blinded to the exposure times, selected which image had density and contrast acceptable for caries detection. When no difference in quality between images with different exposure times could be determined, the lowest exposure time was selected.16
An acrylic device was used to maintain phantoms in position and standardize focus-receptor distance of 40 cm and bitewing projection angulations. Also, a 2.5 cm acrylic block was set between the X-rays beam and the phantoms, to simulate soft tissue attenuation.14 For each phantom two images were acquired: one for the molar region and another for the premolar region, totalling 20 initial images. To standardize initial images, they were all acquired with an aluminum step wedge positioned laterally to the phantom, with eight steps of 2 mm thickness, used to verify the gray values and measure the initial density and contrast (Figure 1). No images presented superimposition of proximal surfaces.
Figure 1.

Acrylic device set, silicone phantom holding teeth in position, aluminum step wedge and sensor used to radiographic acquisitions.
Carious lesions presence and extension were validated by micro-CT, adopted as gold-standard. Teeth were scanned using Skyscan 1174 (Bruker Corp., Kontich, Belgium), at 50 kV, 800 μA.s, 0.5 mm aluminum filter, pixel size of 15 µm, 1 frame, rotation degree of 0.3°, rotation of 180°, 617 basis-images and scanning time of 57 min. The gold standard was assessed independently by two Oral and Maxillofacial radiologists, using the Data Viewer software (Bruker Corp., Kontich, Belgium). Results were compared and, in case of disagreement, the image was re-evaluated by both and a consensus was established.
Image preparation
All radiographic images were exported in TIFF format, with a contrast resolution of 8 bits. In order to standardize initial images, the grey values of the step wedge were measured using software Image J (National Institutes of Health, USA). For image density, the 6 mm thickness aluminum step was set to a grey value of 150 (standard deviation of 20). For image contrast, the differences on grey values between the 6 mm thickness step and the 8 mm and 4 mm steps were up to 40. These values were previously established in a pilot study.
Once density and contrast were standardized and original images were set, each one of the acquisitions had brightness and contrast adjusted with aid of PowerPoint (Microsoft Corporation, Redmond, WA) brightness/contrast tool in four different variations, resulting in five different images for each radiography acquired (original +four adjustments): (V1) −30% brightness and +30% contrast; (V2) −15% brightness and +15% contrast; (V3) original image; (V4) +15% brightness and −15% contrast; and (V5) +30% brightness and −30% contrast, totalling 100 final images.
Image assessment
For caries detection assessment, all images were randomized in a PowerPoint slideshow with black background, being displayed an image per slide with the same size as acquired. Images were assessed in the same room, under dimmed illumination conditions, using a single LCD display of 24.1 inches and resolution of 1920 × 1200 pixels (Barco N.V., Courtrai, Belgium). The use of image manipulation tools was not allowed, except for the zoom tool. Observers were oriented to assess a maximum of 25 images per day and to have an interval of at least 3 days between images assessment, in order to avoid visual fatigue and memorization.
Five Oral and Maxillofacial radiologists with no previous knowledge of the adjustments made independently scored, on a 5-point scale, distal and mesial surfaces of each tooth according to: (1) absence of caries lesion; (2) probably absence of caries lesion; (3) uncertain; (4) probably presence of caries lesion; (5) presence of caries lesion. Additionally, when caries lesions were present (or probably present, i.e. scores 4 or 5), observers had to evaluate their depth in: restricted to the enamel or extending into dentin. 30 days later, 30% of the sample was randomly chosen using a tool of Microsoft Office Excel 2016 (Microsoft Corporation, Redmond, WA) and re-assessed to verify reproducibility.
In a second stage, a new PowerPoint presentation was prepared, with the five variations of each radiograph arranged randomly side by side on a single slide with black background (Figure 2). The same observers were asked to indicate their preferred image quality setting (combination of brightness and contrast) for the assessment of caries lesions, by listing the images in order from the best to the worst combination, respectively.
Figure 2.

Radiographic images randomly displayed in a slide for subjective image quality evaluation.
Images were acquired, had brightness and contrast variations applied and randomized in slides by one researcher (HGA), who did not act as observer in the present study.
Statistical analysis
Data were analysed in SPSS v. 22.0 software (IBM Corp, Armonk, NY) with a significance level of 5%. Intra- and interobserver agreements were determined by weighted κ index, as follows: 0.00–0.20, poor; 0.21–0.40, reasonable; 0.41–0.60, moderate; 0.61–0.80, good; 0.81–1.00, excellent. Diagnostic accuracy was determined by the area under the Receiver Operating Characteristic curve (Az), and sensitivity and specificity values were also obtained for each brightness and contrast variation. Diagnostic values were compared by one-way ANOVA, with post-hoc Tukey test. Comparisons between micro-CT (gold standard) and digital intraoral radiography were performed using the McNemar Bowker test.
Results
According to the weighted Kappa test (Table 1), the mean intra- and interobserver agreements ranged from reasonable to good (0.27–0.72) and from poor to moderate (0.05–0.46), respectively. In both cases, the original image (V3) showed the highest reproducibility values, while the V5 variation presented the lowest values.
Table 1.
Weighted kappa test (95% confidence intervals) for intra- and interobserver agreement
| Brightness and contrast variations | Intraobserver agreement | Interobserver agreement | ||
| Mean | (min–max) | Mean | (min–max) | |
| V1 (−30% brightness; +30% contrast) | 0.66 | (0.44–0.87) | 0.45 | (0.26–0.60) |
| V2 (−15% brightness; +15% contrast) | 0.52 | (0.09–0.75) | 0.34 | (0.12–0.54) |
| V3 (original image) | 0.72 | (0.33–0.96) | 0.46 | (0.19–0.73) |
| V4 (+15% brightness; −15% contrast) | 0.53 | (0.30–0.67) | 0.38 | (0.21–0.56) |
| V5 (+30% brightness; −30% contrast) | 0.27 | (0.00–0.44) | 0.05 | (0.02–0.24) |
Average values for the diagnostic tests are shown in Table 2. Diagnostic accuracy, expressed as Az values, sensitivity and specificity showed no differences between the original and adjusted images in the detection of proximal caries lesions. Although not significant, V5 presented lower values in all diagnostic tests. All the original and adjusted images had relatively low values of sensitivity and high specificity.
Table 2.
Mean values (standard deviation) of area under ROC curve (Az), sensitivity and specificity distributed according to the variations of brightness and contrast
| Variables | Brightness and contrast variations | ||||
| V1 | V2 | V3 | V4 | V5 | |
| Accuracy (Az) | 0.68 ± 0.07 | 0.66 ± 0.05 | 0.67 ± 0.05 | 0.67 ± 0.05 | 0.62 ± 0.06 |
| Sensitivity | 0.45 ± 0.17 | 0.45 ± 0.18 | 0.45 ± 0.18 | 0.41 ± 0.16 | 0.40 ± 0.24 |
| Specificity | 0.86 ± 0.13 | 0.84 ± 0.11 | 0.84 ± 0.18 | 0.89 ± 0.11 | 0.78 ± 0.24 |
ROC, receiver operating characteristic.
p > 0.05, according to ANOVA, post-hoc test.
Table 3 summarizes the findings related to each radiographic variation regarding the presence and extension of caries lesions. There was a significant difference between the gold-standard and the radiographic images (p < 0.0001), regardless of whether these images were original or adjusted (Figure 3). The rate of correct answers ranged from 46% (V5) to 50.5% (V2). Increased brightness associated with decreased contrast (i.e. V4 and V5) yielded higher rate of true negative diagnoses (healthy surfaces), although the lowest true positive rates were also observed among these cases. On the other hand, there were more cases of overestimation of the presence and extension of caries lesions among images with decreased brightness and the increased contrast (V1 and V2).
Table 3.
Total number of proximal surfaces diagnosed as “healthy”, caries restricted to “enamel” and caries extending into “dentin” by the five evaluators (400 proximal faces), distributed according to the different variations of brightness and contrast
| Brightness and contrast variations | Gold-standard (micro-CT) |
Total (n = 400) |
||
|
Healthy (n = 160) |
Enamel (n = 140) |
Dentine (n = 100) |
||
| V1 | ||||
| Healthy | 140 (87.5) | 92 (65.7) | 47 (47) | 279 |
| Enamel | 16 (10) | 40 (28.6) | 35 (35) | 91 |
| Dentine | 4 (2.5) | 8 (5.7) | 18 (18) | 30 |
| V2 | ||||
| Healthy | 139 (86.9) | 90 (64.3) | 45 (45) | 274 |
| Enamel | 20 (12.5) | 48 (34.3) | 40 (40) | 108 |
| Dentine | 1 (0.6) | 2 (1.4) | 15 (15) | 18 |
| V3 | ||||
| Healthy | 138 (86.3) | 94 (67.1) | 46 (46) | 278 |
| Enamel | 19 (11.9) | 41 (29.3) | 40 (40) | 100 |
| Dentine | 3 (1.9) | 5 (3.6) | 14 (14) | 22 |
| V4 | ||||
| Healthy | 147 (91.9) | 101 (72.1) | 52 (52) | 300 |
| Enamel | 12 (7.5) | 35 (25) | 36 (36) | 83 |
| Dentine | 1 (0.6) | 4 (2.9) | 12 (12) | 17 |
| V5 | ||||
| Healthy | 157 (98.1) | 119 (85) | 69 (69) | 345 |
| Enamel | 3 (1.9) | 21 (15) | 25 (25) | 49 |
| Dentine | 0 (0) | 0 (0) | 6 (6) | 6 |
p > 0.001 according to McNemar Bowker test, for all brightness and contrast variations evaluated.
Figure 3.
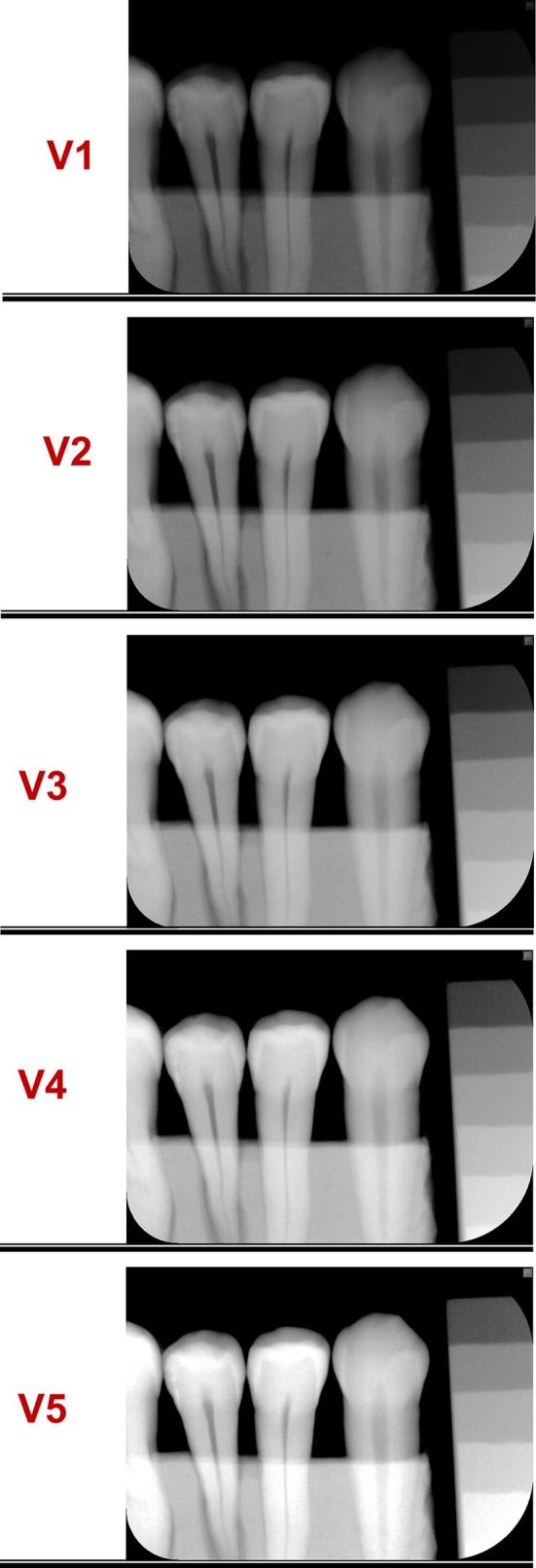
Radiographic images of the region of premolar teeth adjusted in the five brightness and contrast variations (V1–V5) showing caries lesions reaching only the enamel (mesial and distal surfaces of the first premolar) and a caries lesion reaching enamel and dentin (distal surface of the second premolar).
The subjective evaluation of image quality showed that radiographs with lower brightness and higher contrast (V1 and V2) tended to be preferred by observers for the diagnosis of proximal caries lesions (Figure 4). The V1 and V2 variations were classified as “best” and “good” in 70 and 66% of the cases, respectively. The original image was classified as “regular” in most cases. In contrast, V4 and V5 were considered “bad” and “worst” in 74 and 100% of the cases, respectively.
Figure 4.

Distribution of brightness and contrast variations according to the observers’ preference for diagnosis of proximal caries lesions.
Discussion
The early diagnosis of dental caries is a challenge for dentists and oral radiologists and represents an important step in guiding dental therapeutic procedures. In this sense, intraoral digital radiographs play an essential role in dental evaluation and currently, several methods of image enhancement have been investigated in order to improve the performance of this imaging modality.5, 17 However, previous studies had evaluated enhancement tools provided by the proprietary software of digital systems. As the brightness and contrast adjustments seem to be the most used tools in digital imaging analysis and they are freely applied in many researches, it is important to study their influence on specific diagnostic tasks. To the best of our knowledge, this study was the first to assess the influence of the controlled adjustment of brightness and contrast in the evaluation of the presence and extension of caries lesions, besides investigating the observers' preference for the subjective image quality in such diagnostic task.
Considering that radiographic diagnosis of caries lesions is related to the detection of differences in density between the dental hard tissues and the demineralized tissues, it would be expected that images with higher contrast and lower brightness would improve the detection of caries lesions, as pointed out by Pontual et al16. Nevertheless, it is known that the perception of the differences in density of a radiographic image can vary between individuals, as well as the occurrence of visual edge effect such as the “Mach Band”, which can lead to the misinterpretation of the presence or depth of caries lesions.18, 19 It is also important to highlight that the variations of brightness and contrast levels used here still provided images acceptable for diagnosis.
Micro-CT analyses of proximal surfaces showed a balanced distribution of lesions (40% healthy, 35% enamel and 25% dentine lesions), and only non-cavitated surfaces were part of our study. Cavitated lesions were excluded from our sample because their radiographic and clinical detection is considerably more favourable than the others,11, 20,21 and the detection of non-cavitated lesions is especially important because it facilitates the use of non-invasive treatment.13
Regarding the viewing conditions for radiographic interpretation, Pakkala et al22 and Hellén-Halme and Lith23 reported that ambient light levels do not affect the ability to detect carious lesions in digital radiographs. However, other studies24, 25 reported higher accuracy for this diagnostic task in dimmed-light condition. For this reason, we preferred to carry out the evaluations in a dimly lit room.
Results demonstrated an overall low accuracy of intraoral radiography for diagnosis of caries lesions, with low sensitivity and high specificity values, as reported previously.11, 12,16,26,27 According to Pontual et al16, caries diagnostic methods with high specificity at the expense of some loss of sensitivity seem preferable, as the clinical consequences of false positive results can cause unnecessary restorative treatment. Additionally, the use of fluoride dentifrices over time may lead incipient caries to develop slowly, arrest or remineralize. So, the combined clinical and radiographic follow-up is valuable for proper caries diagnosis and treatment management.16
Several studies comparing the performance of conventional radiographs and digital systems in the detection of proximal caries lesions found no differences between image receptors.3,11–13,16,21,26,28 However, some of them did not control the use of image manipulation tools, allowing the evaluators to use them freely during radiographic interpretation,11–13 while other studies did not allow image enhancement,26, 28 or did not mention it clearly.3, 16,21 Standardization of image settings is important because excessive levels of brightness and/or contrast and also the lack of some degree of adjustments may impair diagnosis.
Surprisingly, the range of brightness and contrast variations tested in our study did not have a positive or negative influence on the detection of proximal caries lesions. When evaluating the effects of these tools on caries diagnosis, Tyndall et al15 concluded that contrast and brightness enhancements controlled by the operator seemed to decrease the diagnostic accuracy of caries lesions. Different diagnostic criteria and study design may explain the different results found in that study, since the level of adjustments performed by the observers, and their preferences, were not recorded. Moreover, the caries lesions were considered present only if its histologic depth was halfway through the enamel or beyond, and the digital system used by them in late 1990s is currently outdated.15
Although these adjustments are the most commonly performed by dental practitioners, most studies in the literature investigated other image enhancement tools in the evaluation of caries, such as negative filter,17, 29 sharpen,17 specific contrast enhancement,4 image enhancement filter designed for caries detection,30 and the simultaneous use of more than one image tool.5, 6,17 The influence of these image adjustments varied between favourable,5, 6,30 indifferent4, 17 and harmful29; however, the methodological variability of these studies should also be considered, such as the difference between digital systems evaluated (indirect,30 semi-direct4–6,17 and direct acquisitions4, 29 and the presence of natural caries lesions4–6,29,30 or induced by demineralization,5, 17 cavitated4, 29 or not,5, 17 which makes it difficult to compare results.
The diagnostic accuracy of the intraoral radiography on caries diagnosis has been related to the depth of the lesion.11, 27 In the present study, the overall detection of caries was better when it reached dentin, although in most cases the depths recorded by the observers did not correspond to those identified in the gold standard, as previously reported.16, 30 Even though the performance of the radiography had not differed significantly between the variations of brightness and contrast tested, images with higher contrast and lower brightness favoured the correct detection of a greater number of caries lesions. Such image settings (V1, V2) were also classified by the evaluators as the ones with best quality for the diagnosis of caries and presented higher values of agreement than those with higher brightness and lower contrast (V4 and V5).
Considering our results and the fact that brightness and contrast adjustments may require longer clinical time depending on the software used, they should be performed only if the dental clinician really feels more confident to make the diagnosis. As an ex vivo study, the present research is marked by the absence of clinical information, which are important in the diagnostic decision-making and could improve the performance during the radiographic interpretation. Further investigations should be carried out involving other diagnostic tasks in order to know whether brightness and contrast adjustments interfere on the accuracy of digital radiographs evaluations. In addition, it is known that the “Mach band” visual effect can also occur at the interface of dental restorations. Although studies evaluating the performance of digital radiographs in detecting recurrent caries have found that even the type of restorative material (amalgam or resin) may influence these results,14 information on methods of image enhancement for this diagnosis is still scarce in the literature.
In conclusion, the brightness and contrast adjustments, within the range tested, do not influence the diagnosis of approximal caries. Therefore, we suggest that observers adjust these parameters according to their discretion, but that they also should keep in mind that the brightness and contrast adjustments should be limited at levels that are known to not compromise the diagnosis.
Contributor Information
Eduarda HL Nascimento, Email: eduarda.hln@gmail.com.
Hugo Gaêta-Araujo, Email: hugogaeta@hotmail.com.
Karla F Vasconcelos, Email: karlafav13@gmail.com.
Bernardo B Freire, Email: bernardobarbosafreire@hotmail.com.
Christiano Oliveira-Santos, Email: oliveirach@usp.br.
Francisco Haiter-Neto, Email: haiter@fop.unicamp.br.
Deborah Q Freitas, Email: deborahq@unicamp.br.
REFERENCES
- 1.World Health Organization (WHO). Sugars and dental caries. Geneva: WHO. 2017. Available from: http://apps.who.int/iris/bitstream/10665/259413/1/WHO-NMH-NHD-17.12-eng.pdf [accessed 26 January 2018].
- 2.Wenzel A. Radiographic display of carious lesions and cavitation in approximal surfaces: advantages and drawbacks of conventional and advanced modalities. Acta Odontol Scand 2014; 72: 251–64. doi: 10.3109/00016357.2014.888757 [DOI] [PubMed] [Google Scholar]
- 3.Kayipmaz S, Sezgin ÖS, Saricaoğlu ST, Çan G. An in vitro comparison of diagnostic abilities of conventional radiography, storage phosphor, and cone beam computed tomography to determine occlusal and approximal caries. Eur J Radiol 2011; 80: 478–82. doi: 10.1016/j.ejrad.2010.09.011 [DOI] [PubMed] [Google Scholar]
- 4.Haak R, Wicht MJ, Noack MJ. Conventional, digital and contrast-enhanced bitewing radiographs in the decision to restore approximal carious lesions. Caries Res 2001; 35: 193–9. doi: 10.1159/000047455 [DOI] [PubMed] [Google Scholar]
- 5.Kajan ZD, Tayefeh Davalloo R, Tavangar M, Valizade F. The effects of noise reduction, sharpening, enhancement, and image magnification on diagnostic accuracy of a photostimulable phosphor system in the detection of non-cavitated approximal dental caries. Imaging Sci Dent 2015; 45: 81–7. doi: 10.5624/isd.2015.45.2.81 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Møystad A, Svanaes DB, Risnes S, Larheim TA, Gröndahl HG. Detection of approximal caries with a storage phosphor system. A comparison of enhanced digital images with dental X-ray film. Dentomaxillofac Radiol 1996; 25: 202–6. doi: 10.1259/dmfr.25.4.9084274 [DOI] [PubMed] [Google Scholar]
- 7.Wenzel A. A review of dentists' use of digital radiography and caries diagnosis with digital systems. Dentomaxillofac Radiol 2006; 35: 307–14. doi: 10.1259/dmfr/64693712 [DOI] [PubMed] [Google Scholar]
- 8.Parks ET. Digital radiographic imaging: is the dental practice ready? J Am Dent Assoc 2008; 139: 477–81. [DOI] [PubMed] [Google Scholar]
- 9.Wenzel A, Hirsch E, Christensen J, Matzen LH, Scaf G, Frydenberg M. Detection of cavitated approximal surfaces using cone beam CT and intraoral receptors. Dentomaxillofac Radiol 2013; 42: 39458105. doi: 10.1259/dmfr/39458105 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rovaris K, de Faria Vasconcelos K, do Nascimento EH, Oliveira ML, Freitas DQ, Haiter-Neto F. Brazilian young dental practitioners' use and acceptance of digital radiographic examinations. Imaging Sci Dent 2016; 46: 239–44. doi: 10.5624/isd.2016.46.4.239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Abesi F, Mirshekar A, Moudi E, Seyedmajidi M, Haghanifar S, Haghighat N, et al. . Diagnostic accuracy of digital and conventional radiography in the detection of non-cavitated approximal dental caries. Iran J Radiol 2012; 9: 17–21. doi: 10.5812/iranjradiol.6747 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Haiter-Neto F, Wenzel A, Gotfredsen E. Diagnostic accuracy of cone beam computed tomography scans compared with intraoral image modalities for detection of caries lesions. Dentomaxillofac Radiol 2008; 37: 18–22. doi: 10.1259/dmfr/87103878 [DOI] [PubMed] [Google Scholar]
- 13.Krzyżostaniak J, Kulczyk T, Czarnecka B, Surdacka A. A comparative study of the diagnostic accuracy of cone beam computed tomography and intraoral radiographic modalities for the detection of noncavitated caries. Clin Oral Investig 2015; 19: 667–72. doi: 10.1007/s00784-014-1282-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sousa Melo SL, Belem MDF, Prieto LT, Tabchoury CPM, Haiter-Neto F. Comparison of cone beam computed tomography and digital intraoral radiography performance in the detection of artificially induced recurrent caries-like lesions. Oral Surg Oral Med Oral Pathol Oral Radiol 2017; 124: 306–14. doi: 10.1016/j.oooo.2017.05.469 [DOI] [PubMed] [Google Scholar]
- 15.Tyndall DA, Ludlow JB, Platin E, Nair M. A comparison of kodak ektaspeed plus film and the siemens sidexis digital imaging system for caries detection using receiver operating characteristic analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1998; 85: 113–8. doi: 10.1016/S1079-2104(98)90408-5 [DOI] [PubMed] [Google Scholar]
- 16.Pontual AA, de Melo DP, de Almeida SM, Bóscolo FN, Haiter Neto F. Comparison of digital systems and conventional dental film for the detection of approximal enamel caries. Dentomaxillofac Radiol 2010; 39: 431–6. doi: 10.1259/dmfr/94985823 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Belém MD, Ambrosano GM, Tabchoury CP, Ferreira-Santos RI, Haiter-Neto F. Performance of digital radiography with enhancement filters for the diagnosis of proximal caries. Braz Oral Res 2013; 27: 245–51. doi: 10.1590/S1806-83242013000300004 [DOI] [PubMed] [Google Scholar]
- 18.Lane EJ, Proto AV, Phillips TW. Mach bands and density perception. Radiology 1976; 121: 9–17. doi: 10.1148/121.1.9 [DOI] [PubMed] [Google Scholar]
- 19.Berry HM. Cervical burnout and Mach band: two shadows of doubt in radiologic interpretation of carious lesions. J Am Dent Assoc 1983; 106: 622–5. doi: 10.14219/jada.archive.1983.0109 [DOI] [PubMed] [Google Scholar]
- 20.Bottenberg P, Jacquet W, Stachniss V, Wellnitz J, Schulte AG. Detection of cavitated or non-cavitated approximal enamel caries lesions using CMOS and CCD digital X-ray sensors and conventional D and F-speed films at different exposure conditions. Am J Dent 2011; 24: 74–8. [PubMed] [Google Scholar]
- 21.Dehghani M, Barzegari R, Tabatabai H, Ghanea S. Diagnostic value of conventional and digital radiography for detection of cavitated and non-cavitated proximal caries. J Dent 2017; 14: 21–30. [PMC free article] [PubMed] [Google Scholar]
- 22.Pakkala T, Kuusela L, Ekholm M, Wenzel A, Haiter-Neto F, Kortesniemi M. Effect of varying displays and room illuminance on caries diagnostic accuracy in digital dental radiographs. Caries Res 2012; 46: 568–74. doi: 10.1159/000341218 [DOI] [PubMed] [Google Scholar]
- 23.Hellén-Halme K, Lith A. Carious lesions: diagnostic accuracy using pre-calibrated monitor in various ambient light levels: an in vitro study. Dentomaxillofac Radiol 2013; 42: 20130071. doi: 10.1259/dmfr.20130071 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kutcher MJ, Kalathingal S, Ludlow JB, Abreu M, Platin E. The effect of lighting conditions on caries interpretation with a laptop computer in a clinical setting. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006; 102: 537–43. doi: 10.1016/j.tripleo.2005.11.004 [DOI] [PubMed] [Google Scholar]
- 25.Hellén-Halme K, Petersson A, Warfvinge G, Nilsson M. Effect of ambient light and monitor brightness and contrast settings on the detection of approximal caries in digital radiographs: an in vitro study. Dentomaxillofac Radiol 2008; 37: 380–4. doi: 10.1259/dmfr/26038913 [DOI] [PubMed] [Google Scholar]
- 26.Zhang ZL, Qu XM, Li G, Zhang ZY, Ma XC. The detection accuracies for proximal caries by cone-beam computerized tomography, film, and phosphor plates. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011; 111: 103–8. doi: 10.1016/j.tripleo.2010.06.025 [DOI] [PubMed] [Google Scholar]
- 27.Schwendicke F, Tzschoppe M, Paris S. Radiographic caries detection: a systematic review and meta-analysis. J Dent 2015; 43: 924–33. doi: 10.1016/j.jdent.2015.02.009 [DOI] [PubMed] [Google Scholar]
- 28.Zayet MK, Helaly YR, Eiid SB. Effect of changing the kilovoltage peak on radiographic caries assessment in digital and conventional radiography. Imaging Sci Dent 2014; 44: 199–205. doi: 10.5624/isd.2014.44.3.199 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Miri S, Mehralizadeh S, Sadri D, Motamedi MR, Soltani P. The efficacy of the reverse contrast mode in digital radiography for the detection of proximal dentinal caries. Imaging Sci Dent 2015; 45: 141–5. doi: 10.5624/isd.2015.45.3.141 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Seneadza V, Koob A, Kaltschmitt J, Staehle HJ, Duwenhoegger J, Eickholz P. Digital enhancement of radiographs for assessment of interproximal dental caries. Dentomaxillofac Radiol 2008; 37: 142–8. doi: 10.1259/dmfr/51572889 [DOI] [PubMed] [Google Scholar]